
Most of us who live with neuropathy know the feeling intimately. The tingle in the toes that won't quite go away. The pins and needles that wake you up at 3 a.m. The buzz in your fingertips when you reach for a coffee cup. The strange crawling sensation that has no source you can point to. We feel these things every day, and we describe them with whatever words come to mind — usually some version of “tingling” because that's the closest the English language gets.
The medical word for all of these sensations is paresthesia. It's pronounced pair-es-THEE-zhuh, and it's a useful word to have, because it captures something specific that “tingling” alone doesn't. Paresthesia means an abnormal sensation that arises on its own — without anything from the outside world causing it. Your skin isn't being touched. Nothing is pressing on your nerve. Yet the sensation is there. The signal is coming from inside.
I want to walk you through what paresthesia actually is, what's happening neurologically when you feel it, why some types are harmless and some need urgent attention, and how it relates to the broader picture of neuropathy. This is one of those topics where understanding the mechanism makes the experience less frightening — and helps you tell the difference between “this is my familiar nerve pain” and “this is something I need to call my doctor about right now.”
What Paresthesia Is, in Plain Words
Paresthesia is the medical term for any abnormal sensation that you feel on or just beneath the skin without anything from the outside causing it. The most common forms are tingling, prickling, the classic “pins and needles,” numbness, burning, an itching that has nothing to scratch, or a crawling-skin feeling. Sometimes it's a buzz. Sometimes it's a fizz. Sometimes it's a sensation people describe as “static.”
Paresthesia means “abnormal sensation that arises on its own”
No outside stimulus is causing it — your skin isn't being touched, no pressure is on the nerve, and yet the sensation is there. The signal is coming from inside the nervous system, not from the outside world. That's what makes it different from normal sensation.
What unites all of these is that they originate from the nervous system itself, not from anything happening to your skin. A normal sensation, like the feeling of cool water on your hand, starts when nerve endings in the skin pick up a real stimulus and send a signal to your brain. Paresthesia is what happens when nerves send a signal even though nothing in the outside world has caused it. The wiring is firing on its own.
This can be a one-time, harmless event — like your foot “falling asleep” after sitting cross-legged. Or it can be a daily, persistent companion that comes from genuine nerve damage. The difference between those two situations is what the rest of this article is about.
The Two Big Categories: Transient and Chronic

Paresthesia divides cleanly into two groups, and the distinction matters a lot for what's happening underneath.
Transient vs. Chronic Paresthesia
- Lasts minutes
- From compression or reduced blood flow
- Resolves with movement
- Harmless
- Almost everyone has experienced it
- Persistent or recurring
- From nerve damage or systemic disease
- Doesn't resolve with position changes
- Needs medical evaluation
- Common with neuropathy
Transient paresthesia is the brief, harmless kind almost everyone has experienced. You sit on a leg too long, you lean an elbow on a hard surface, you cross your legs at the wrong angle. Within minutes you have tingling, numbness, or pins and needles in that limb. You shift position, the sensation gets briefly worse as the limb “wakes up,” and then within a few minutes it's gone.
Chronic paresthesia is the kind we who live with neuropathy know too well. It doesn't go away when you change position. It's there whether you've moved or not. It might be worse at certain times of day, or after certain activities, but it's persistent in a way that transient paresthesia isn't. This is the tingling that keeps you up at night, that makes you check your toes for marks, that has you wondering whether something underneath your skin has truly broken.
Chronic paresthesia is almost always a sign that something in the nervous system has gone wrong, somewhere along the chain from peripheral nerves to spinal cord to brain. That “something” is what doctors are trying to identify when they evaluate you, and it ranges from common and treatable causes to rare and serious ones.
What's Actually Happening When You Feel Pins and Needles
This is the part I find genuinely interesting, and it helps to know it.
Three mechanisms that produce paresthesia
1. Compression: Pressure on a nerve interrupts signaling like a kinked hose. When pressure releases, nerves “wake up” with chaotic firing — the classic pins and needles.
2. Ectopic discharge: Damaged nerves develop hyperexcitable membranes and fire spontaneously, without any external stimulus. This drives most chronic neuropathic paresthesia.
3. Central sensitization: Over time, the spinal cord and brain themselves become more reactive, amplifying signals before they reach awareness.
Your nerves communicate using electrical signals that move along their length and chemical signals that pass between them. Under normal conditions, a nerve fires when something appropriate triggers it — a touch, a temperature change, pressure. The signal travels to your brain, which interprets it. Then the nerve goes quiet again.
Several things can disrupt this normal cycle and produce paresthesia.
Compression Paresthesia
When you sit on your leg, you compress the nerves running through it. The pressure interrupts the normal signaling along the nerve fibers — like crimping a garden hose. Some signals stop getting through, which is the “numbness” part. Others get garbled, which can produce strange sensations.
When you release the pressure, the nerves “wake up” with a flood of disorganized firing as normal signaling resumes. That chaotic, rapid firing is what your brain interprets as the classic “pins and needles” — sharp, prickling, almost electrical sensation. It's brief because the nerves quickly settle back into their normal rhythm.
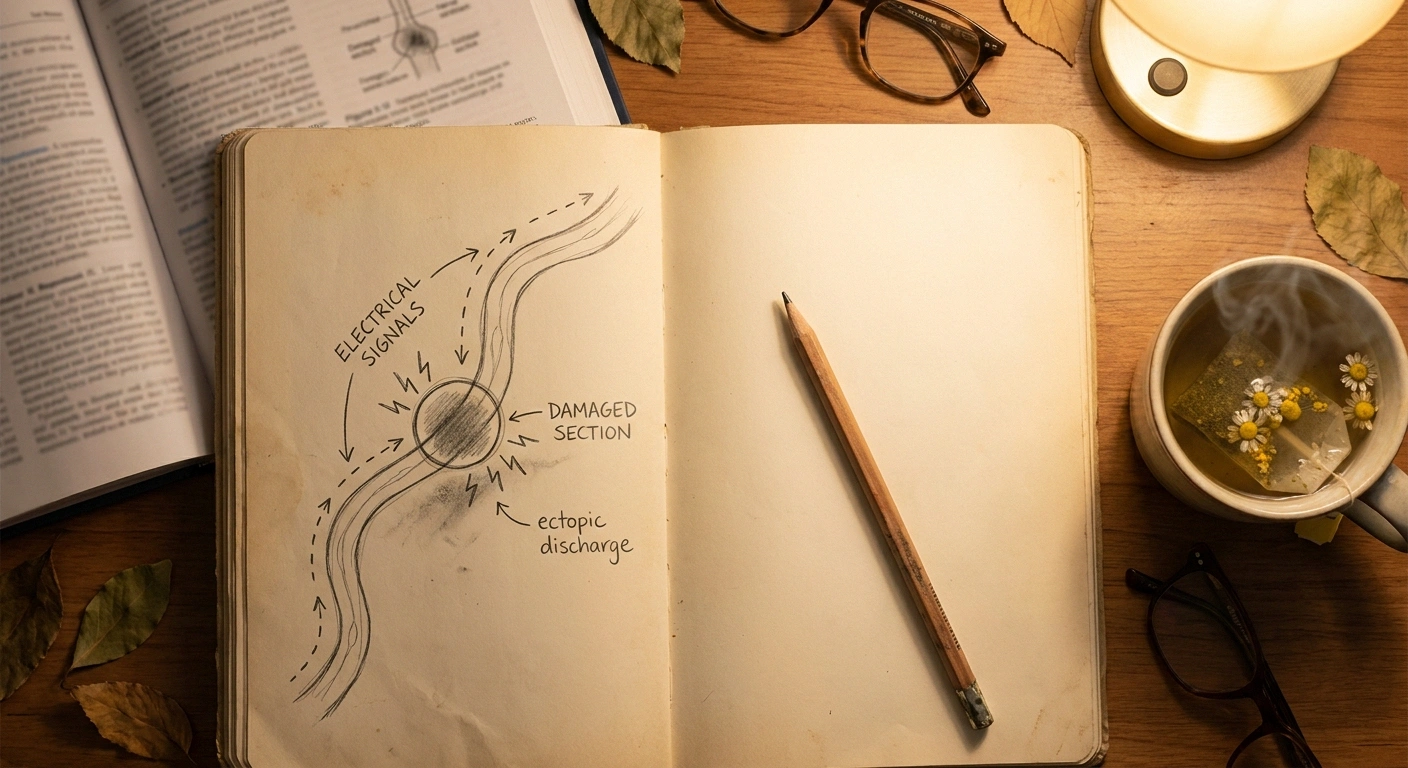
Ectopic Discharge
This is the mechanism behind much of chronic neuropathic paresthesia, and it's why neuropathy can feel like the volume knob on your nerves got stuck on high. When a nerve is damaged — by diabetes, chemotherapy, alcohol, autoimmune attack, or any of the other causes — its membrane often becomes hyperexcitable. Sodium channels, the gateways that let nerves fire, become overrepresented or behave abnormally. The nerve starts firing on its own, without any real stimulus from the outside world.
That spontaneous, abnormal firing is called ectopic discharge — “ectopic” meaning “out of the normal place,” because the signal is coming from a damaged stretch of nerve rather than from a sensory ending picking up a real stimulus. Your brain receives the signal and interprets it as best it can, which is why the sensation is often hard to describe. It doesn't correspond to anything happening on your skin. It's the nerve itself shouting.
This is also why gabapentin and pregabalin (Lyrica) can help neuropathic paresthesia. They quiet down the calcium channel activity that contributes to nerve hyperexcitability. Sodium channel blockers like some anticonvulsants and the topical agent lidocaine work along similar lines.
Central Sensitization
In some chronic cases, the spinal cord and brain themselves become more sensitive over time. The pain and paresthesia signals get amplified before they reach conscious awareness. This is called central sensitization, and it's why some people with neuropathy feel sensations that seem out of proportion to the apparent damage. The nervous system has rewired itself to be more reactive.
What Causes Chronic Paresthesia

The list of causes is long, but a handful account for the majority of cases.
Common Causes of Chronic Paresthesia
Peripheral neuropathy is far and away the most common cause of chronic tingling in hands and feet. Within that, diabetic neuropathy accounts for roughly 30% of all peripheral neuropathy cases. Other major contributors include chemotherapy-induced neuropathy, alcoholic neuropathy, autoimmune neuropathies, and idiopathic neuropathy where no cause is found.
Vitamin deficiencies can produce paresthesia even before they cause overt neuropathy. B12 deficiency is the classic example, but B1 (thiamine), B6, folate, and vitamin E can all be involved. Excess B6, paradoxically, also causes paresthesia.
Nerve entrapment syndromes are localized causes — carpal tunnel syndrome from median nerve compression at the wrist, ulnar neuropathy from elbow compression, peroneal neuropathy from compression at the side of the knee. These tend to produce tingling in specific body areas that match the territory of the trapped nerve.
Systemic diseases can damage nerves throughout the body. Kidney disease, liver disease, hypothyroidism, lupus, and Lyme disease all have neuropathic features in some patients.
Multiple sclerosis can cause paresthesia from demyelination in the brain or spinal cord. The pattern is usually different from peripheral neuropathy — often involving one limb, a band around the trunk, or one side of the face — and other symptoms like vision changes or balance issues commonly accompany it.
Migraine aura can include paresthesia, usually starting in the fingertips and spreading up the arm, often followed by similar sensations around the mouth and tongue. The signs are diagnostic — typically lasting less than an hour and resolving as the migraine itself develops.
Anxiety and hyperventilation can cause paresthesia in the fingertips and around the mouth through a temporary calcium imbalance triggered by overbreathing. This is benign but can be quite alarming for the person experiencing it.
Medications can cause paresthesia as a side effect. Notable culprits include some chemotherapy drugs, certain antibiotics like fluoroquinolones, the tuberculosis drug isoniazid, and the anticonvulsant topiramate. If your tingling started shortly after a new medication, that connection is worth raising with your doctor.
When Paresthesia Is a Red Flag
Most paresthesia is not an emergency. The tingling and numbness of chronic neuropathy, while uncomfortable, isn't a sudden danger. There are, however, specific patterns that need urgent medical evaluation rather than waiting for a routine appointment.
These paresthesia patterns need urgent care
- Sudden one-sided paresthesia, especially with weakness, facial droop, or speech changes (possible stroke)
- Paresthesia ascending from feet upward over days with weakness (possible Guillain-Barré)
- Saddle-area numbness with new bowel or bladder problems (possible cauda equina)
- Paresthesia following a recent head, neck, or spine injury
- Paresthesia with severe new pain or muscle weakness
Don't wait for an appointment — call emergency services or go to the ER for any of these.
- Sudden paresthesia on one side of the body, especially with weakness, facial droop, or speech changes — this is a stroke until proven otherwise. Call emergency services.
- Paresthesia following a recent head, neck, or spine injury — could indicate nerve damage that needs evaluation.
- Progressive paresthesia ascending from feet to legs to trunk over days, especially with weakness — could be Guillain-Barré syndrome, which is a medical emergency.
- Paresthesia with severe new pain or weakness — needs urgent evaluation.
- Paresthesia in the saddle area (inner thighs, genitals, buttocks) with new bowel or bladder problems — could be cauda equina syndrome, a surgical emergency.
If anything in this list matches your experience, don't read further articles, don't wait for your appointment — get medical attention now. The slow, chronic tingling of long-standing neuropathy doesn't have these features, but it's worth knowing them so you can tell the difference if something new and serious starts.
How Doctors Evaluate Chronic Paresthesia

If you've gone in to see a doctor for persistent tingling, you've probably been through some version of the standard workup. Knowing what each test is trying to find can demystify the process.
Standard Workup for Chronic Paresthesia
A careful history is the first and often most useful tool. Where does it tingle? When did it start? Is it on one side or both? Does it come and go, or is it constant? Are there other symptoms? What medications and supplements are you on? What's your medical history?
A focused physical exam follows. Your doctor will check sensation in different parts of your body using touch, vibration, temperature, and a small monofilament tool. They'll check your reflexes and muscle strength. They'll often check your gait and balance.
Blood work commonly includes a complete blood count, glucose and A1C (for diabetes screening), thyroid hormones, B12 and folate levels, sometimes vitamin D, kidney and liver function panels, and inflammatory markers. If a specific autoimmune or infectious cause is suspected, more targeted tests follow.
Nerve conduction studies and electromyography (EMG) directly test whether your nerves are conducting signals normally. They're not always needed, but they're particularly useful when the cause isn't clear or when surgery for nerve entrapment is being considered. Our overview of neuropathy diagnosis walks through what the tests look like and what the results mean.
Living With Chronic Paresthesia

Most chronic paresthesia from neuropathy is something you live with rather than cure. The underlying nerve damage that produces the abnormal sensation often persists even when the original trigger — for example, high blood sugar from diabetes — is brought under control. The goal of treatment becomes reducing the intensity of the sensations and minimizing how much they interfere with your life.
Several types of intervention can help.
Medications targeting nerve hyperexcitability — gabapentin, pregabalin, certain antidepressants like duloxetine and amitriptyline — can dampen ectopic discharge and reduce paresthesia along with pain. They don't fix the underlying nerve damage but can quiet the abnormal signals.
Topical treatments like lidocaine patches and capsaicin cream can locally reduce nerve firing in the skin. They're particularly useful for paresthesia limited to specific areas.
Underlying-cause treatment matters more than any symptom medication. Tight blood sugar control if you have diabetes, B12 supplementation if you're deficient, addressing thyroid problems, treating sleep apnea — these don't always reverse existing damage but they prevent further damage.
Lifestyle approaches that improve overall nerve health include regular gentle exercise, a nutrient-dense diet, adequate sleep, and stress management. These aren't dramatic interventions, but for many people they take the edge off chronic paresthesia in ways that are genuinely meaningful.
Why Naming It Matters

Sometimes people ask me why I bother with the medical word “paresthesia” when “tingling” works fine. The honest answer is that having a precise word for what we feel makes us better partners with our doctors. When you tell a neurologist “I have paresthesia in my feet that worsens at night,” you're using their language. They know exactly what you mean. The conversation moves faster, and the questions they ask back are more targeted.
Naming a thing also has a quieter effect. When the strange tingling that wakes you up at night has a name, it stops being a vague malevolent presence and becomes a known phenomenon with known mechanisms and known interventions. You can read about it. You can ask precise questions about it. You can find others who have it. That doesn't make it go away, but it makes it less frightening, and that's its own kind of relief.
What to Take From This
The chronic tingling, prickling, and pins-and-needles sensations many of us live with are paresthesia. They're not imagined. They're not “just” anything. They're real signals coming from real changes in real nerves — most often nerves that have been damaged by something, sometimes nerves that are temporarily compressed, occasionally nerves that are responding to a deeper systemic problem.
Real signals from real changes in real nerves
Paresthesia isn't imagined or “just” anything. The chronic kind almost always has an identifiable cause and an evidence-based treatment path. Knowing the mechanism, the red flags, and the standard workup turns vague distress into a manageable medical conversation.
The vast majority of chronic paresthesia from neuropathy isn't dangerous in the immediate sense, even though it's distressing. The patterns to take seriously are sudden, one-sided, progressive, or accompanied by weakness, severe pain, or bowel/bladder changes. Everything else, while worth investigating thoroughly with your doctor, is part of the long, manageable journey of living with neuropathy.
And it's a journey we don't have to walk alone. Understanding what's happening inside, having the right words for it, and knowing what to expect is part of how we move forward — one tingle, one tracking entry, one good question to the doctor at a time.
Frequently Asked Questions
What's the difference between paresthesia and neuropathy?
Paresthesia is a symptom — the abnormal sensation itself. Neuropathy is the underlying nerve damage that often causes paresthesia. You can think of paresthesia as what you feel; neuropathy as what's wrong. Not all paresthesia comes from neuropathy (a foot falling asleep is brief paresthesia from compression, not nerve damage), but most chronic paresthesia in the hands and feet is a symptom of an underlying neuropathy.
Why do my hands and feet feel like pins and needles all the time?
Persistent pins-and-needles sensations in the hands and feet usually point to peripheral neuropathy from one of several causes — most commonly diabetes, vitamin deficiencies (especially B12), chemotherapy effects, alcohol-related nerve damage, or autoimmune conditions. A doctor's evaluation can identify the underlying cause, which is the most important step in finding the right treatment.
Is paresthesia always serious?
No. Brief, transient paresthesia from compression — the feeling of a limb falling asleep — is harmless and resolves quickly. Chronic paresthesia is a sign that something is wrong neurologically and deserves medical evaluation, but most of the underlying causes are manageable, not life-threatening. Specific patterns — sudden onset, one-sided, progressive, or with weakness — do need urgent attention.
What causes paresthesia at night?
Several things make paresthesia worse at night. The lack of distractions makes you more aware of sensations you'd ignore during a busy day. Lying down can compress nerves in ways your daytime posture doesn't. Drops in body temperature, blood pressure changes, and natural circadian rhythms all affect how nerves fire. Many people with neuropathy describe their symptoms peaking at night, and there are real physiological reasons.
Can anxiety cause paresthesia?
Yes. Anxiety and hyperventilation can cause tingling, especially in the fingertips, around the mouth, and sometimes in the feet. The mechanism is a temporary calcium imbalance from overbreathing. Anxiety-related paresthesia tends to come on with anxious episodes and resolve as you calm down, which distinguishes it from chronic neuropathic paresthesia. People with neuropathy can have both, of course, and stress can make any nerve symptom feel worse.
How is paresthesia treated?
Treatment depends on the underlying cause. For neuropathic paresthesia, medications like gabapentin, pregabalin, duloxetine, and amitriptyline can quiet abnormal nerve firing. Topical treatments like lidocaine patches and capsaicin cream help with localized symptoms. Treating the underlying condition — diabetes, B12 deficiency, thyroid disease — is equally or more important than treating the symptom directly.
Does paresthesia mean I have nerve damage?
Chronic paresthesia usually does indicate some change in nerve function, though not always permanent damage. Brief paresthesia from compression doesn't reflect damage. Persistent paresthesia warrants evaluation to determine whether reversible or progressive nerve injury is involved, and what's driving it.
What does paresthesia feel like?
Paresthesia is described in many ways: tingling, prickling, pins and needles, numbness, burning, itching with no rash, crawling skin, buzzing, fizzing, or “static.” The specific feeling often varies by what's causing it and where in the nerve pathway the abnormality is. Two people with similar diagnoses can describe their paresthesia very differently. Whatever words you use, the important thing is to describe accurately what you actually feel rather than reaching for clinical language that doesn't quite fit.


