
Tingling in Hands: Neuropathy vs. Carpal Tunnel vs. MS vs. Vitamin Deficiency
You're lying in bed and your hand starts tingling. You shake it out, but it comes back. Or maybe it's been there for weeks — a persistent pins-and-needles sensation that won't go away. Your mind goes to dark places. Is this neuropathy? Could it be multiple sclerosis? Carpal tunnel from too much time at a keyboard?
The truth is, tingling in your hands can come from several completely different conditions — some serious, some easily fixed. The challenge is figuring out which one you're dealing with, because the treatment for each is radically different. Taking gabapentin for what's actually carpal tunnel won't help. Wearing a wrist brace for what's actually B12 deficiency won't either.
This guide breaks down the four most common causes of tingling hands — peripheral neuropathy, carpal tunnel syndrome, multiple sclerosis, and vitamin deficiency — with the specific patterns that distinguish each one. I'm not going to diagnose you (only your doctor can do that), but I am going to arm you with the right questions and the knowledge to advocate for yourself.
Understanding Why Hands Tingle
Tingling happens when something disrupts normal nerve signaling. But where that disruption occurs — and why — is completely different for each condition:
The Key Difference
Neuropathy = damaged nerve fibers. Carpal tunnel = healthy nerve being squeezed. MS = central nervous system demyelination. Vitamin deficiency = metabolic nerve damage. Same symptom — completely different mechanisms and treatments.
Peripheral neuropathy involves damage to the peripheral nerves themselves — the long nerve fibers that run from your spinal cord to your fingertips. The damage typically starts at the ends of the longest nerves (feet first, then hands) and progresses inward. This is why neuropathy usually causes symptoms in both hands in a “glove” distribution.
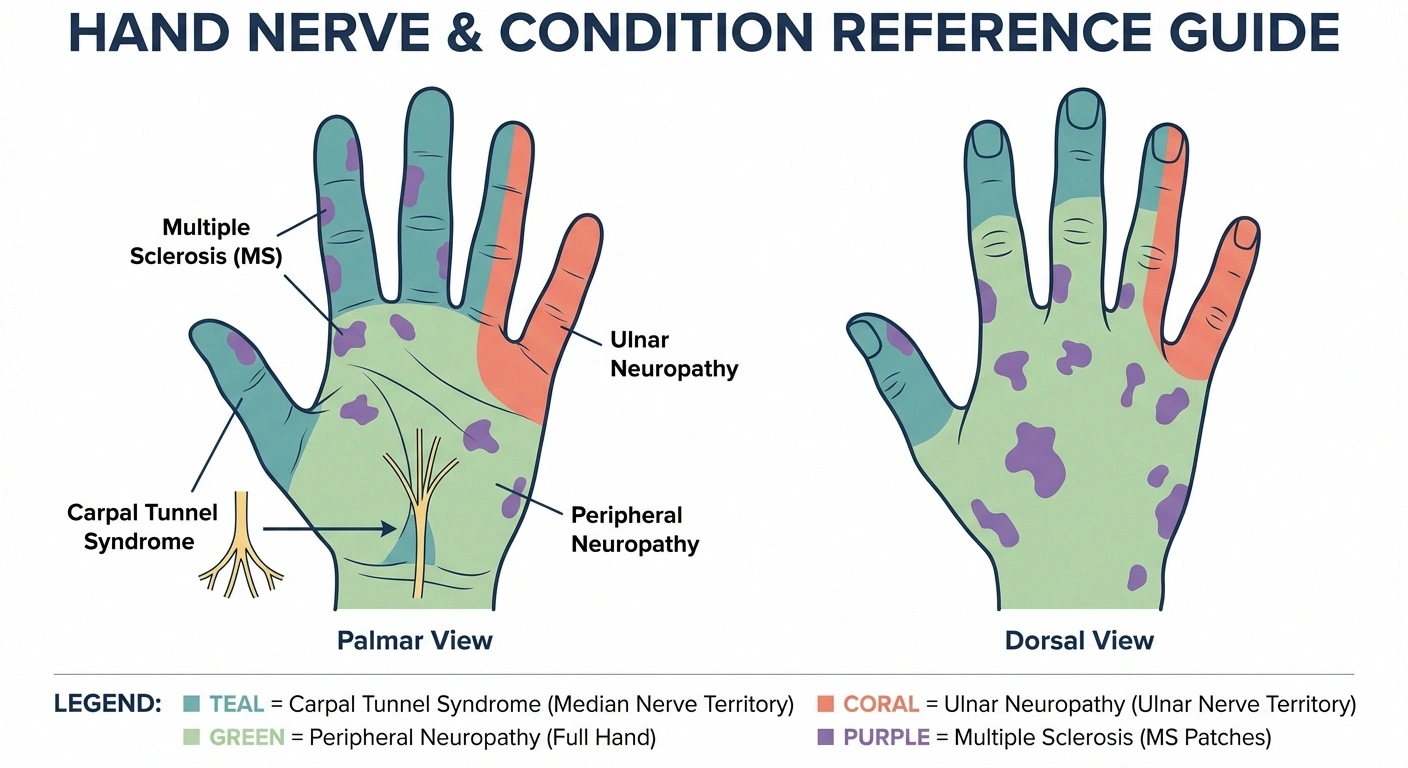
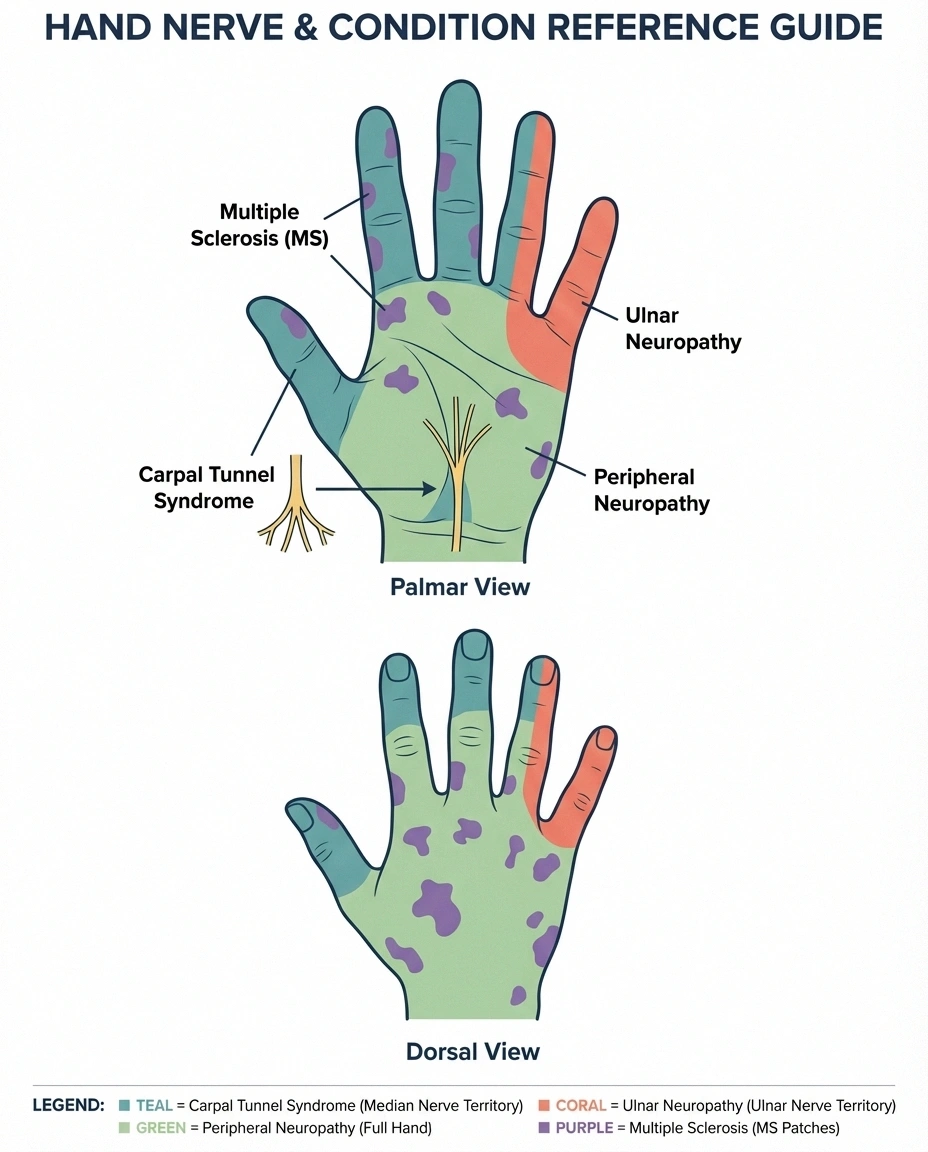
Carpal tunnel syndrome is a compression problem. The median nerve gets squeezed as it passes through a narrow passage (the carpal tunnel) at the wrist. The nerve itself may be healthy — it's just being pinched. This is why symptoms follow the median nerve's territory: the thumb, index, middle, and half the ring finger. Your pinky is spared because it's served by a different nerve (the ulnar nerve).
Multiple sclerosis (MS) damages the myelin sheath in the central nervous system — the brain and spinal cord. Unlike neuropathy, which affects the peripheral nerves, MS disrupts nerve signaling at the source. This means tingling from MS can appear anywhere and may be accompanied by symptoms you'd never see with carpal tunnel or peripheral neuropathy, like vision changes or cognitive problems.
Vitamin deficiency — particularly B12, B6, and sometimes E — damages nerves by disrupting the metabolic processes they need to function. B12 deficiency specifically attacks the myelin sheath (similar to MS), but it affects both the central and peripheral nervous systems. The good news: it's often entirely reversible when caught early.
Which Fingers Are Affected? The Key Diagnostic Clue
This is the single most helpful piece of information for narrowing down the cause of hand tingling. Pay close attention to exactly which fingers are involved:
🖐️ Quick Finger Check: Which Pattern Matches Yours?
Thumb + index + middle finger → Carpal tunnel syndrome (median nerve)
Ring finger + pinky → Ulnar neuropathy (cubital tunnel)
All five fingers, both hands → Peripheral neuropathy or vitamin deficiency
Random patches, one hand, changing locations → More consistent with MS
Thumb, index, and middle finger (+ half of ring finger): Strongly suggests carpal tunnel syndrome. According to the Mayo Clinic, this pattern follows the median nerve's distribution and is the hallmark of carpal tunnel. If your pinky is not tingling while these fingers are, carpal tunnel is the leading suspect.
Ring finger and pinky: Suggests ulnar neuropathy (cubital tunnel syndrome) — compression of the ulnar nerve, typically at the elbow. This is sometimes confused with carpal tunnel but has a distinctly different finger pattern. See our complete guide to ulnar neuropathy.
All five fingers, both hands: Suggests peripheral neuropathy or vitamin deficiency — both cause a symmetric “glove” pattern affecting the entire hand.
Random patches, one hand only, or changing locations: More consistent with MS, where demyelination can affect unpredictable areas. MS tingling may move around, affecting different areas at different times.
Detailed Symptom Comparison
Onset and Progression
Peripheral neuropathy: Gradual onset over months to years. Typically starts in the feet first, then progresses to the hands once foot symptoms are well-established. If your hand tingling appeared before any foot symptoms, peripheral neuropathy is less likely (with the exception of small fiber neuropathy, which can occasionally present in the hands first).
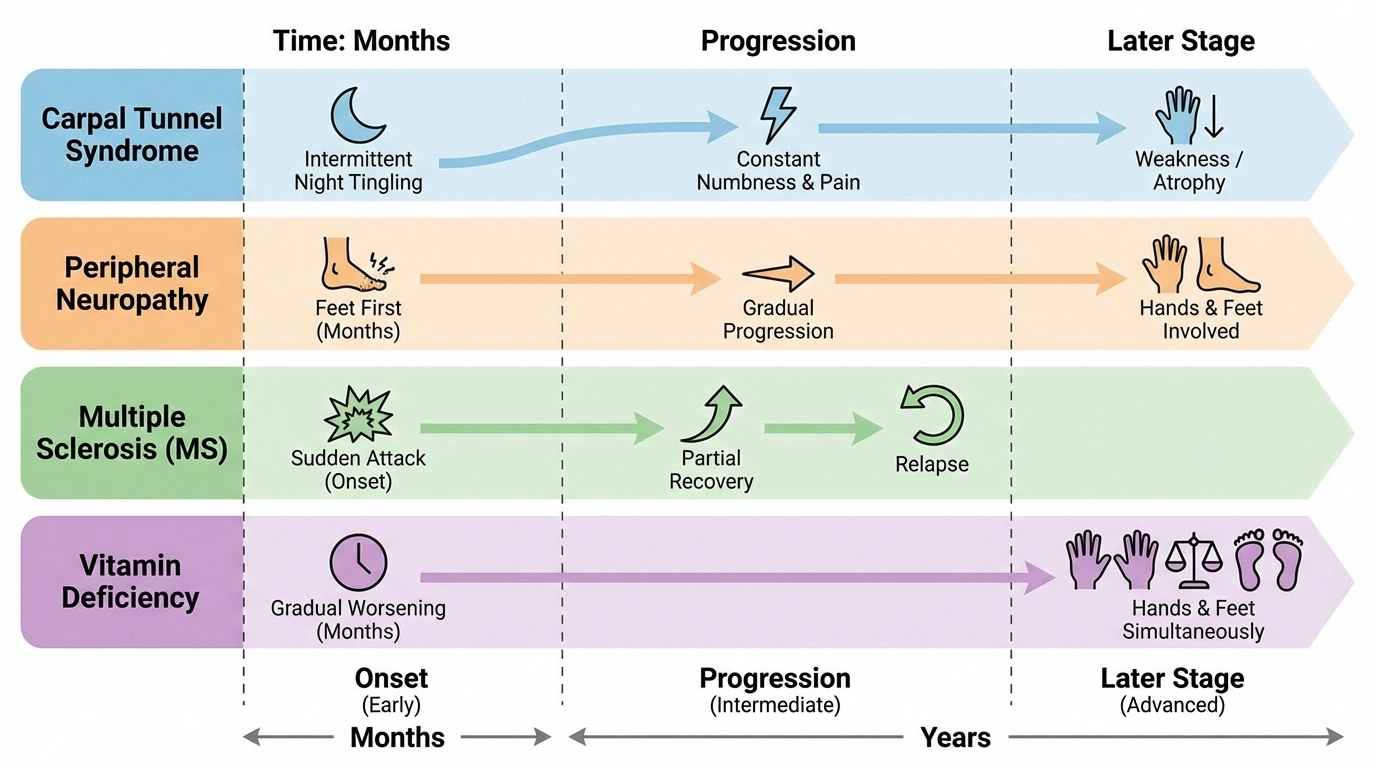
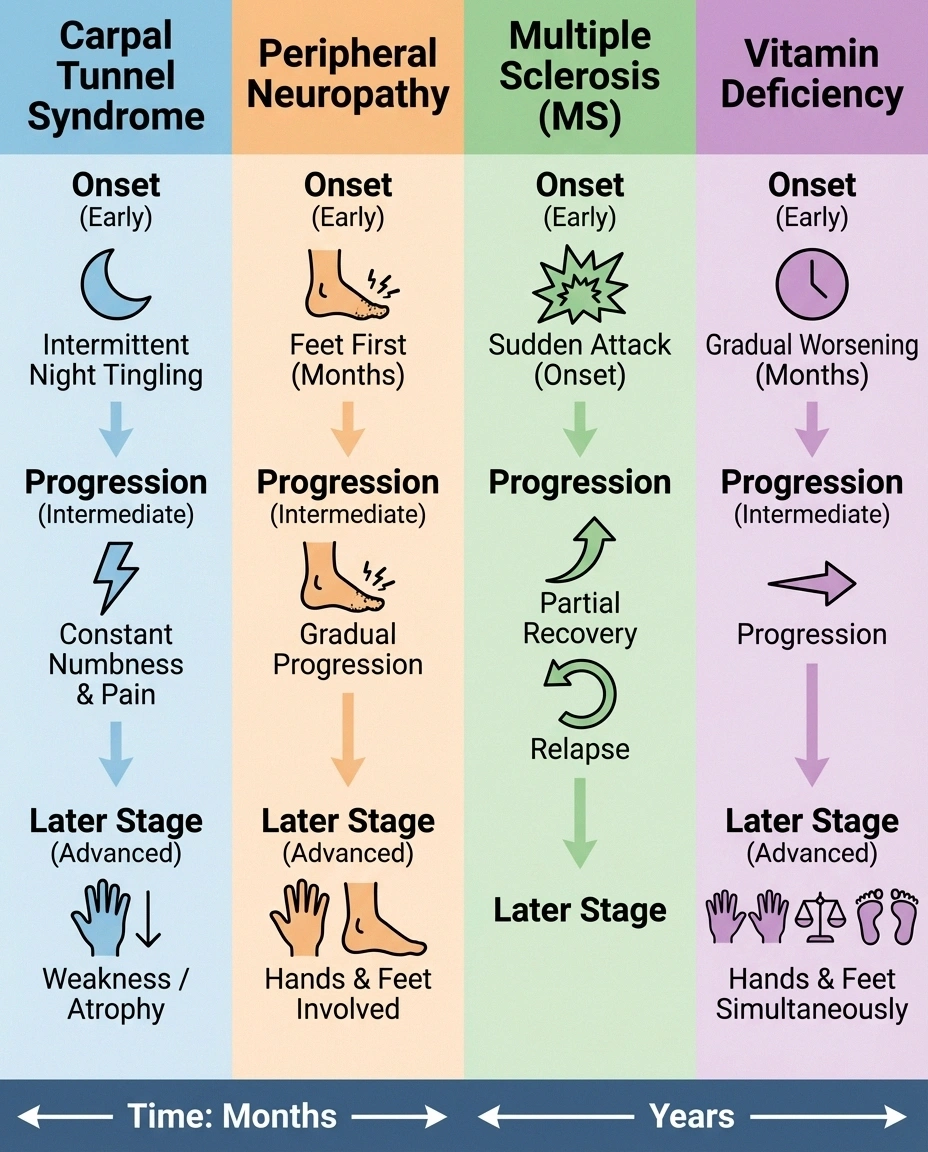
Carpal tunnel syndrome: Gradual onset, often linked to repetitive hand activities. Symptoms frequently start with intermittent tingling that comes and goes, especially at night. Many people notice they wake up with numb or tingling hands and need to shake them out. Over months, the tingling becomes more constant.
Multiple sclerosis: Can be sudden or gradual. MS often presents in “attacks” or “relapses” — symptoms appear over days, last for weeks, then may partially or fully resolve. The first MS symptom is often sensory (tingling, numbness) in one limb. Between relapses, you may feel completely normal.
Vitamin deficiency: Gradual onset over weeks to months, corresponding to the timeline of developing deficiency. B12 deficiency neuropathy can affect hands and feet simultaneously — a pattern that's uncommon in other types of neuropathy and should raise a red flag for your doctor.
What Makes It Better or Worse?
Peripheral neuropathy: Usually worse at night, with activity, and in hot weather. Walking or standing may increase foot symptoms. Symptoms are relatively constant — they don't dramatically change with wrist or hand position.
What Makes Each Condition Worse?
Neuropathy
🌙 Nighttime
🔥 Heat
🚶 Walking/standing
Carpal Tunnel
🛏️ Sleeping
⌨️ Repetitive motions
✊ Gripping objects
MS
🔥 Heat (Uhthoff's)
😰 Fatigue/stress
🛁 Hot baths
Vitamin Deficiency
📈 Gradual worsening
🚫 No positional triggers
⏰ Constant once started
Carpal tunnel: Worse with wrist flexion (bending the wrist forward), gripping objects, and repetitive motions. Notably worse during sleep because many people sleep with flexed wrists. Shaking the hands out typically provides temporary relief — this is so characteristic that doctors call it the “flick sign.” Better when the wrist is in a neutral position.
MS: May worsen with heat (a hot bath, exercise, warm weather) — this is called Uhthoff's phenomenon and is fairly specific to MS. Fatigue and stress can also trigger or worsen symptoms. Rest and cooling typically help.
Vitamin deficiency: Symptoms don't fluctuate much with position or activity. They're relatively constant and gradually worsen until the deficiency is corrected. No specific positional triggers.
Associated Symptoms to Watch For
Peripheral neuropathy: Burning, numbness, balance problems, foot pain, sensitivity to touch. Typically accompanies foot symptoms. May include flare-ups triggered by stress or illness.
Red Flag Symptoms
If hand tingling is accompanied by vision changes, electric shock sensations down your spine, cognitive problems, or episodes of weakness that come and go — see a neurologist promptly. These symptoms go beyond carpal tunnel or neuropathy and may indicate MS or another central nervous system condition that benefits greatly from early treatment.
Carpal tunnel: Weakness in grip strength, dropping objects, difficulty with fine motor tasks (buttoning shirts, turning keys). Pain may radiate up the forearm. No leg or foot symptoms — if you have foot tingling too, it's not carpal tunnel.
MS: This is where the associated symptoms really diverge. MS can cause: vision problems (blurry vision, double vision, optic neuritis), profound fatigue, cognitive changes, muscle spasms, bladder dysfunction, difficulty walking, and Lhermitte's sign (an electric shock sensation down the spine when bending the neck). No other condition on this list produces this range of symptoms.
Vitamin deficiency: Fatigue, pale skin, sore tongue, memory problems, mood changes, weakness, unsteady gait. B6 toxicity (from over-supplementation) can also cause neuropathy — so too much of a vitamin, not just too little, can be the problem.
Diagnostic Tests for Each Condition
Getting the right tests is critical. Here's what to discuss with your doctor for each suspected condition. For a comprehensive overview of neuropathy testing, see our guide to EMG and nerve conduction studies.
Peripheral Neuropathy Tests
- Nerve conduction study (NCS) and EMG — the primary diagnostic test for large fiber neuropathy
- Skin biopsy — measures nerve fiber density for small fiber neuropathy
- Blood work: HbA1c, fasting glucose, B12, MMA, thyroid panel, CBC, comprehensive metabolic panel
- Autonomic testing — if autonomic neuropathy is suspected
Carpal Tunnel Tests
- Phalen's test — bending the wrists forward for 60 seconds to reproduce symptoms. Positive in about 75 percent of carpal tunnel cases.
- Tinel's sign — tapping over the carpal tunnel at the wrist. A tingling sensation radiating into the median nerve fingers suggests compression.
- Nerve conduction study — measures slowing of nerve signals across the wrist. This is the confirmatory test and also grades severity.
- Ultrasound — can visualize swelling of the median nerve at the wrist.
Multiple Sclerosis Tests
- Brain and spinal cord MRI with contrast — the primary diagnostic tool. MS produces characteristic white lesions (plaques) on MRI. This is non-negotiable if MS is suspected.
- Lumbar puncture (spinal tap) — checks cerebrospinal fluid for oligoclonal bands, which are present in about 90 percent of MS patients.
- Evoked potentials — measures electrical signals in the brain in response to stimulation. Slowed responses suggest demyelination.
- Blood tests — primarily to rule out other conditions that mimic MS (lupus, Lyme disease, B12 deficiency, neuromyelitis optica).
Vitamin Deficiency Tests
- Serum B12 — below 400 pg/mL with neurological symptoms warrants further testing, even if technically “normal”
- Methylmalonic acid and homocysteine — functional markers of B12 status that catch early deficiency
- Vitamin B6 level — both deficiency AND excess can cause neuropathy. If you're taking B6 supplements, this test is essential.
- Vitamin E level — less common but can cause sensory neuropathy
- Folate — often deficient alongside B12
Risk Factors: Who Gets What?
Your personal risk factors can help narrow the possibilities:

Higher risk for peripheral neuropathy: Diabetes or prediabetes, heavy alcohol use, chemotherapy history, family history of neuropathy, age over 60, autoimmune conditions. See our stages of neuropathy guide for more on progression.
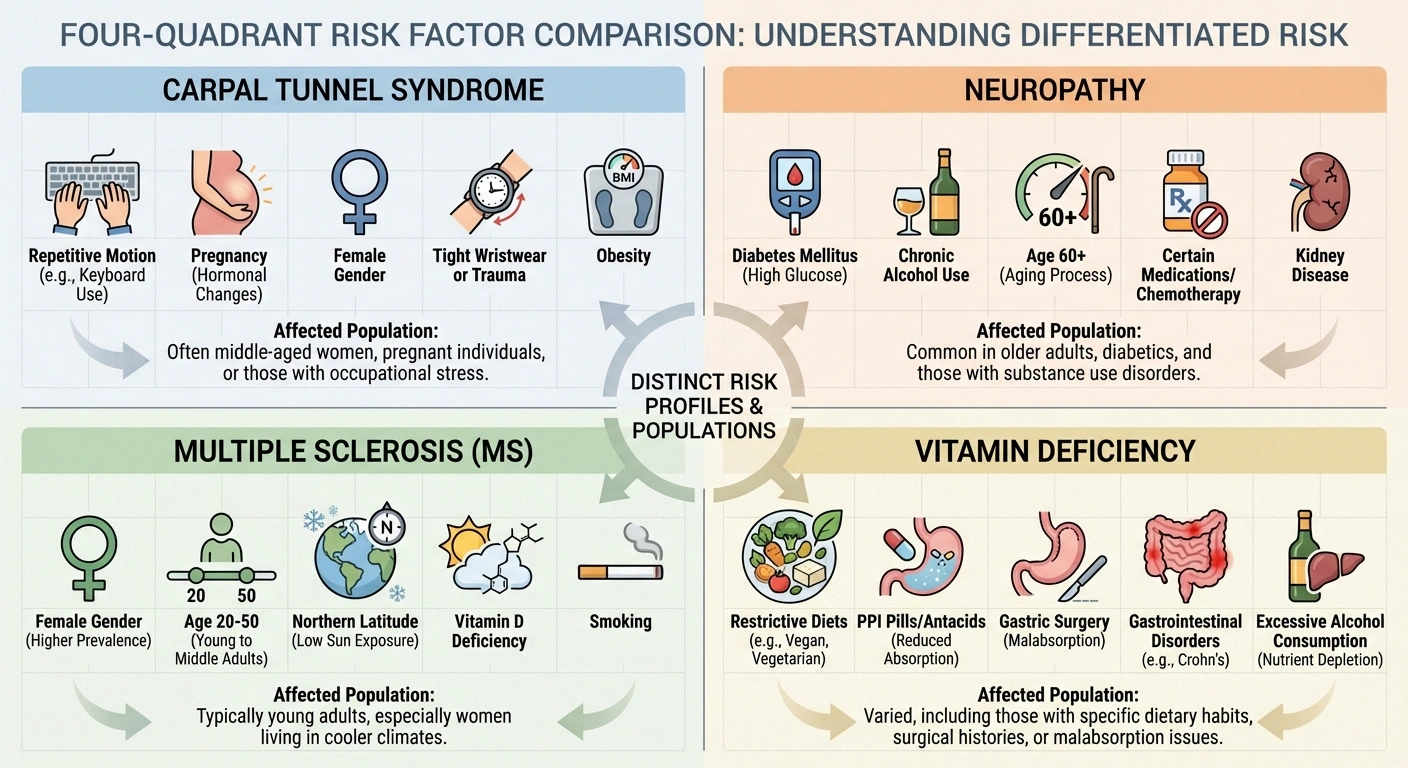
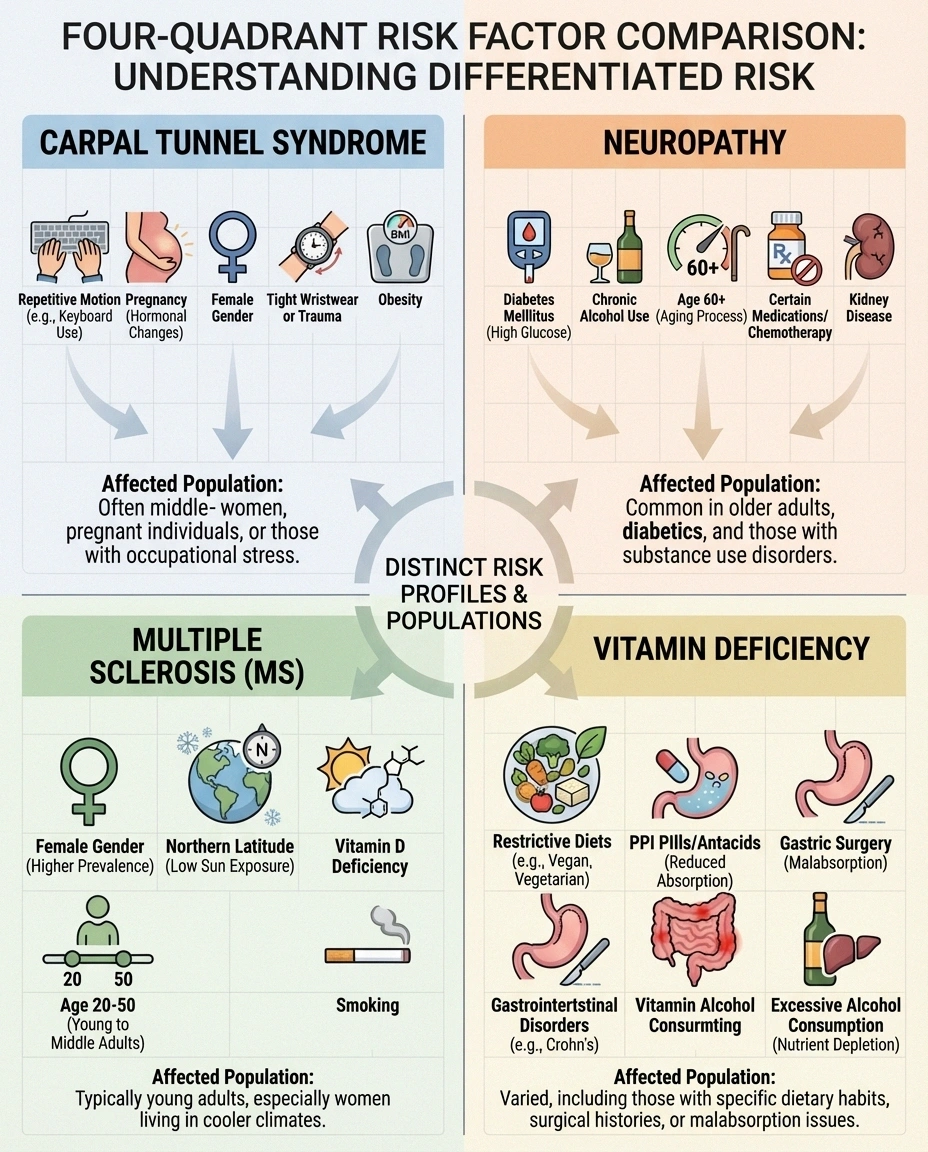
Higher risk for carpal tunnel: Repetitive hand/wrist work (typing, assembly line work, construction), pregnancy, hypothyroidism, rheumatoid arthritis, obesity, female sex (3 times more common in women). Affects working-age adults most commonly.
Higher risk for MS: Female sex (2-3 times more common in women), age 20-50 at onset, northern latitude/low vitamin D, family history of MS, smoking, certain infections (Epstein-Barr virus). MS is relatively rare — about 1 million Americans — but should not be dismissed because early treatment dramatically changes outcomes.
Higher risk for vitamin deficiency: Vegan or vegetarian diet (B12), older adults (reduced absorption), gastric bypass surgery, chronic acid reflux medication (PPIs reduce B12 absorption), metformin use, heavy alcohol use, restricted diets, malabsorption conditions (Crohn's disease, celiac disease).
The Decision Tree: What to Do Next
Based on the symptom patterns above, here's a practical approach to getting the right diagnosis:
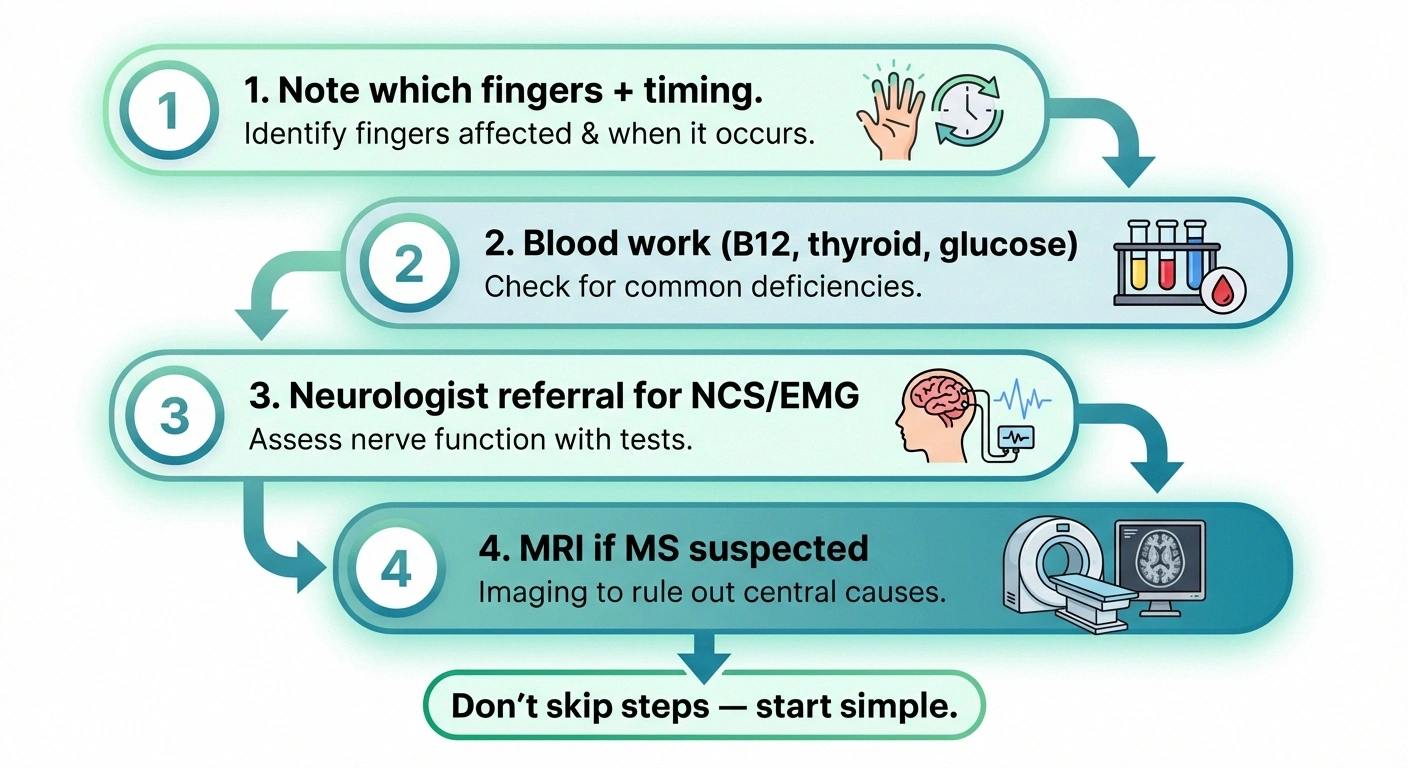
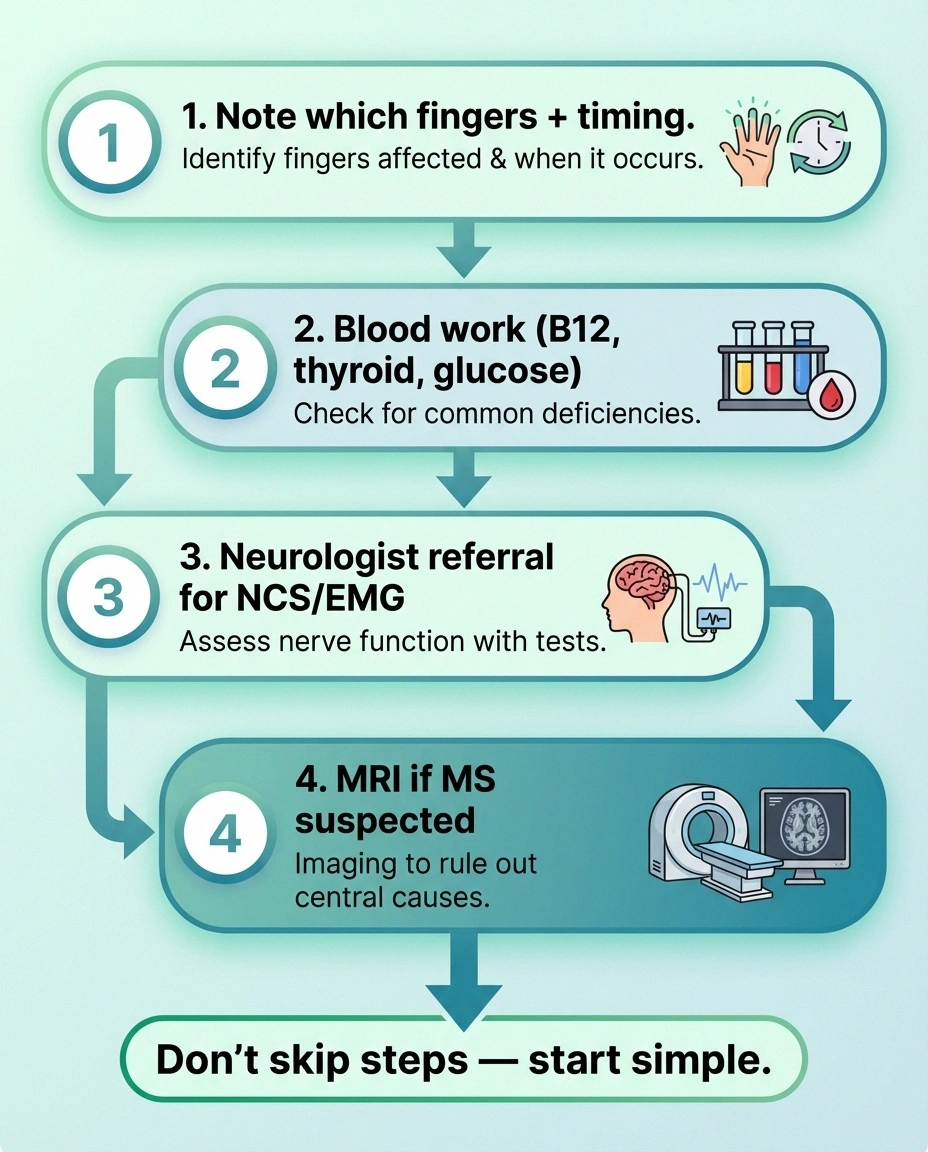
Your Diagnostic Action Plan
Track Your Symptoms
Which fingers? When? What makes it better or worse? Write it down.
Get Blood Work
B12, MMA, CBC, thyroid, HbA1c, fasting glucose. One draw, many answers.
See a Neurologist
Nerve conduction studies distinguish carpal tunnel from peripheral neuropathy.
MRI If Needed
Only if MS or central nervous system involvement is suspected. Don't skip to this step.
Step 1: Note which fingers are affected and when symptoms occur (constant vs. intermittent, night vs. day, at rest vs. with activity).
Step 2: See your primary care doctor. Request baseline blood work: B12, methylmalonic acid, CBC, thyroid panel, HbA1c, fasting glucose, vitamin B6. This one blood draw can confirm or rule out vitamin deficiency and flag diabetes or thyroid problems.
Step 3: If blood work is normal and symptoms persist, get a referral to a neurologist for nerve conduction studies. The NCS can distinguish between carpal tunnel (localized compression at the wrist) and peripheral neuropathy (generalized nerve damage).
Step 4: If the neurologist suspects MS — especially if you have symptoms beyond the hands, visual changes, or a relapsing-remitting pattern — an MRI of the brain and spinal cord is the next step.
Don't skip steps. The most common mistake is jumping straight to expensive imaging when a simple blood test would have found the answer. Conversely, don't let a normal blood test reassure you if symptoms are worsening — some conditions require specialized testing to diagnose.
Frequently Asked Questions
Can carpal tunnel syndrome cause tingling in all five fingers?
Carpal tunnel syndrome should only cause tingling in the thumb, index finger, middle finger, and half of the ring finger — the area served by the median nerve. If your pinky finger is also tingling, the cause is likely not isolated carpal tunnel syndrome. You may have ulnar neuropathy in addition to carpal tunnel, or the underlying cause may be peripheral neuropathy rather than nerve compression at the wrist. Tell your doctor specifically which fingers are affected.
Should I be worried that tingling in my hands is MS?
MS is relatively uncommon, affecting about 1 million Americans compared to the 20 million with peripheral neuropathy. While hand tingling can be an early symptom of MS, it is far more commonly caused by carpal tunnel syndrome, vitamin deficiency, or peripheral neuropathy. MS becomes more likely if you also experience vision changes, severe fatigue, cognitive changes, electric shock sensations in the spine, or if symptoms come and go in distinct episodes lasting days to weeks.
Can you have both carpal tunnel and neuropathy at the same time?
Yes, and this is surprisingly common, especially in people with diabetes. Diabetic neuropathy can make the median nerve more susceptible to compression at the wrist, creating a “double crush” phenomenon. If nerve conduction studies show both slowed conduction at the wrist and generalized neuropathy, both conditions may be contributing to your symptoms. Treatment would address both — a wrist brace or surgery for the carpal tunnel and medical management for the neuropathy.
How quickly does vitamin B12 deficiency cause tingling?
B12 deficiency typically takes months to years to develop because the body stores several years' worth of B12 in the liver. However, once neurological symptoms appear, they can progress relatively quickly. If you have been on a vegan diet without supplementation, are taking proton pump inhibitors (PPIs) for acid reflux, or have had gastric bypass surgery, your timeline to deficiency may be shorter. Early treatment is important because nerve damage from prolonged B12 deficiency may not fully reverse.
Does the Phalen's test at home reliably diagnose carpal tunnel?
The Phalen's test — bending both wrists forward for 60 seconds to see if tingling occurs — has about 75 percent sensitivity for carpal tunnel syndrome. It is a useful screening tool but not definitive. A positive test at home is a good reason to see your doctor, but a negative test does not rule out carpal tunnel, especially in early cases. Nerve conduction studies remain the gold standard for confirming the diagnosis and grading its severity.
What is the most important first test to get for tingling hands?
A basic blood panel including vitamin B12 with methylmalonic acid, complete blood count, fasting blood sugar or HbA1c, and thyroid function tests. This single blood draw can identify or rule out several common treatable causes of hand tingling including vitamin deficiency, diabetes, and thyroid disease. It is inexpensive, widely available, and should be the first step before more specialized testing like nerve conduction studies or MRI.
The Bottom Line
Tingling hands have a cause, and that cause can almost always be identified with the right testing. The pattern of which fingers are affected, when symptoms occur, and what other symptoms accompany the tingling are your most powerful diagnostic clues. Bring this information to your doctor — it dramatically speeds up diagnosis.

The most important thing is to not ignore persistent tingling. Whether it turns out to be carpal tunnel (treatable with a splint or minor surgery), vitamin deficiency (reversible with supplements), neuropathy (manageable with the right approach), or something more serious that benefits from early treatment — getting answers sooner is always better than waiting.
For more on understanding and managing nerve symptoms, explore our guides on what neuropathy feels like, vitamin deficiency and neuropathy, and the complete neuropathy diagnosis process.


