When most people hear “Botox,” they picture cosmetic procedures — smoothing wrinkles, lifting brows. What doesn't come to mind is neuropathy pain relief. And yet, neurologists have been quietly using botulinum toxin injections for neuropathic pain for more than two decades, with a growing body of clinical evidence to back it up.
I want to be upfront: Botox for neuropathy pain is not a mainstream first-line treatment, and it's not right for everyone. It requires a specialist, repeated injections, and careful patient selection. But for people with certain types of severe or treatment-resistant nerve pain, it represents a genuinely promising option that many patients and even some doctors don't know exists.
Let me walk you through what botulinum toxin actually does in the context of nerve pain, which conditions it may help, what the treatment experience is like, and what the research actually shows.
What Is Botulinum Toxin — and Why Would It Help Pain?
Botulinum toxin is a protein produced by the bacterium Clostridium botulinum. In large amounts, it causes botulism — a serious illness. In precisely controlled, tiny doses, it has remarkable therapeutic properties.
Botox relieves neuropathy pain through mechanisms completely separate from its muscle-relaxing effect. Research has confirmed that pain relief lasts far longer than muscle effect — meaning the toxin directly targets sensory nerves, not just muscles.
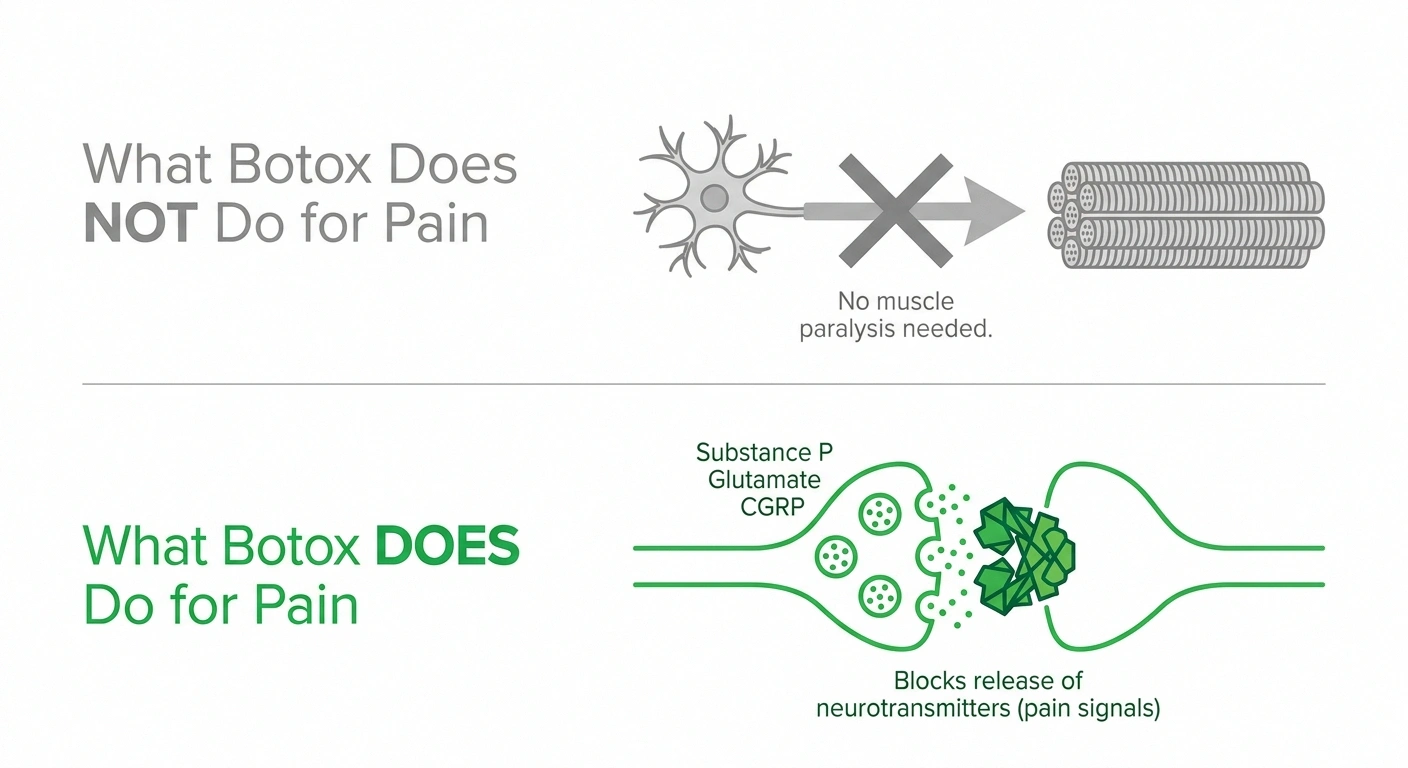
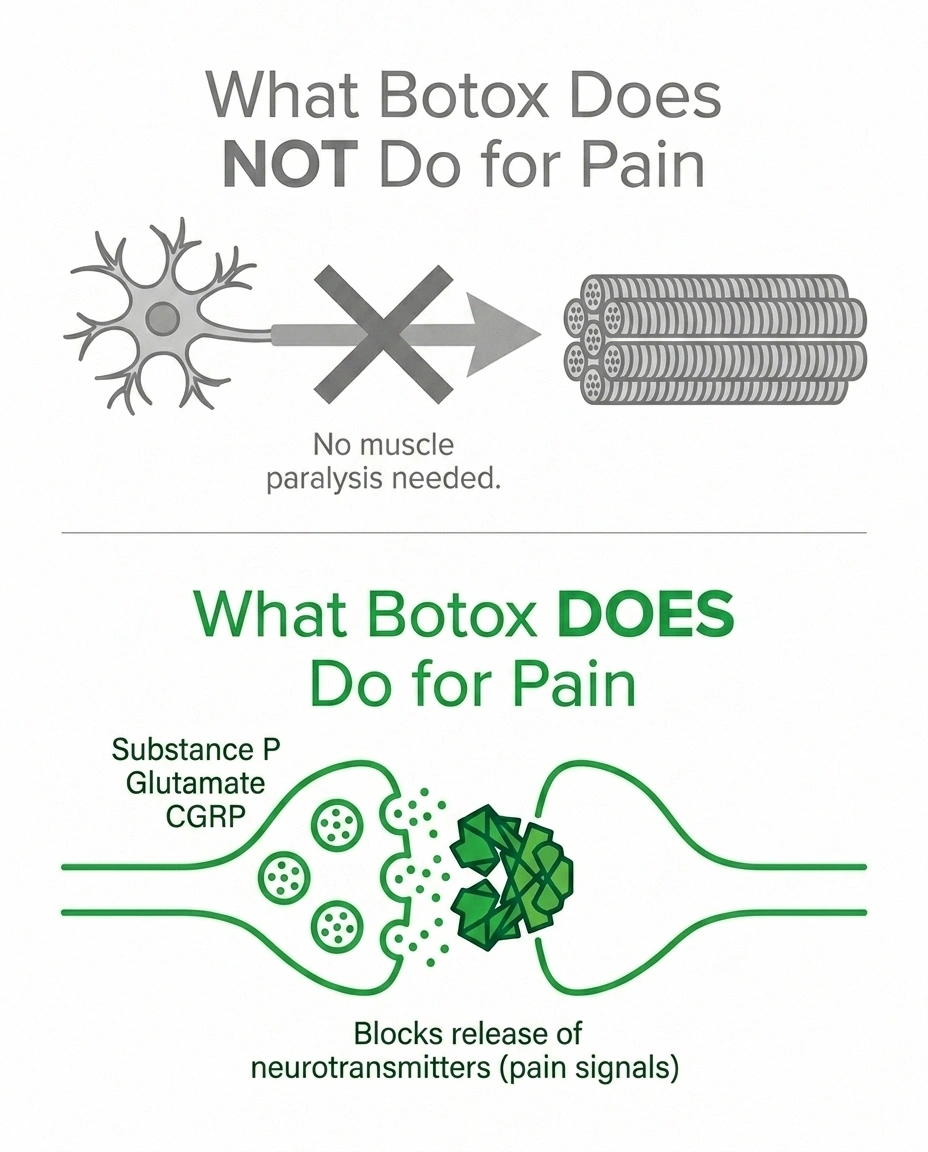
Most people know botulinum toxin for its muscle-relaxing effect: it blocks the release of acetylcholine at neuromuscular junctions, causing temporary, localized muscle paralysis. This is the mechanism behind both its cosmetic uses (relaxing facial muscles to reduce wrinkles) and its well-established medical uses (treating cervical dystonia, spasticity, chronic migraine, excessive sweating, and overactive bladder).
But when it comes to pain, the mechanism is different — and this distinction is critical. The analgesic (pain-relieving) effects of botulinum toxin in neuropathic pain are independent of muscle relaxation. Research has clearly demonstrated that the duration of pain relief extends well beyond the duration of muscle effect. In other words, you don't need to paralyze muscles to get pain relief — the toxin has direct actions on sensory nerves that are separate from its muscle effects.
How Botulinum Toxin Works on Nerve Pain
The mechanisms by which botulinum toxin reduces neuropathic pain are multiple and still being refined, but here's what the research has established:
The landmark BOTNEP trial (The Lancet Neurology, 2016) — a randomized, double-blind, placebo-controlled study — found that two rounds of botulinum toxin A injections produced sustained analgesic effects against peripheral neuropathic pain beyond what the toxin's direct tissue duration would predict, suggesting possible longer-term recalibration of pain processing.
Blocking pain mediator release. Botulinum toxin inhibits the release of several key pain-signaling molecules from sensory nerve endings:
- Substance P — a neuropeptide that transmits pain signals and promotes inflammation
- Glutamate — a major excitatory neurotransmitter involved in pain sensitization
- Calcitonin gene-related peptide (CGRP) — involved in neurogenic inflammation and sensitization
Reducing neurogenic inflammation. By blocking the release of these mediators, botulinum toxin reduces the local inflammatory response around nerve endings — the kind of inflammation that amplifies pain signals and perpetuates the cycle of chronic neuropathic pain.
Central effects via axonal transport. Botulinum toxin can travel up nerve fibers (axonal transport) to exert effects in the dorsal root ganglia and spinal cord — not just at the injection site. This helps explain why a relatively small injection can have more widespread pain-relieving effects and why the relief can last much longer than the local muscle effect.
Sodium channel deactivation. There is evidence that botulinum toxin affects sodium channels on sensory neurons, reducing their excitability and the generation of ectopic (abnormal, spontaneous) nerve signals — which are a key driver of neuropathic pain symptoms like burning, electric shocks, and spontaneous pain.
Together, these mechanisms help explain why botulinum toxin can interrupt the cycle of neuropathic pain at multiple points — and why it's particularly interesting for conditions involving both peripheral sensitization and central sensitization. Understanding central sensitization helps explain why some neuropathy pain is so difficult to treat with standard approaches, and why drugs or techniques that interrupt sensitization can be so valuable.
Which Types of Neuropathy Pain Has Botox Been Used For?
Botulinum toxin has been studied in several specific neuropathic pain conditions. The evidence varies in strength, but here's where the research is most promising:
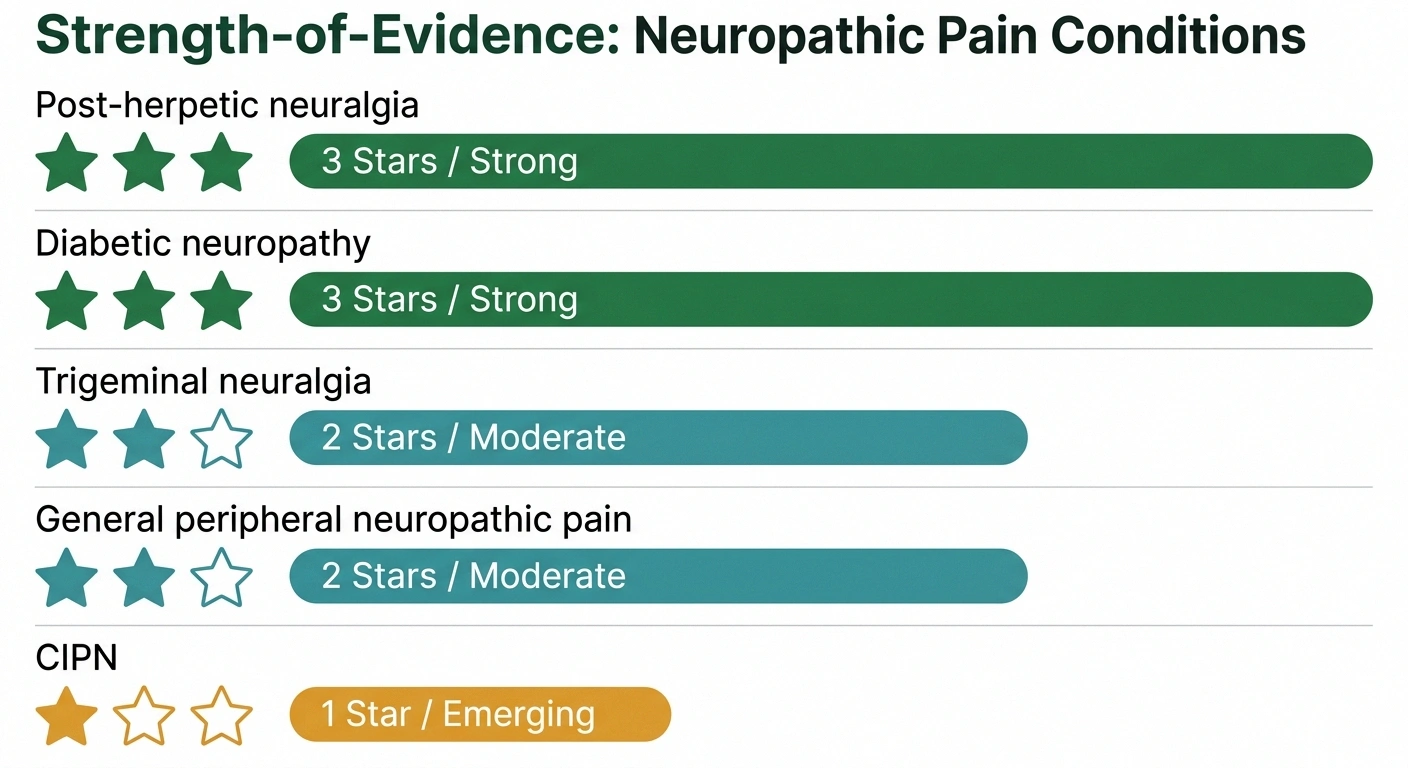
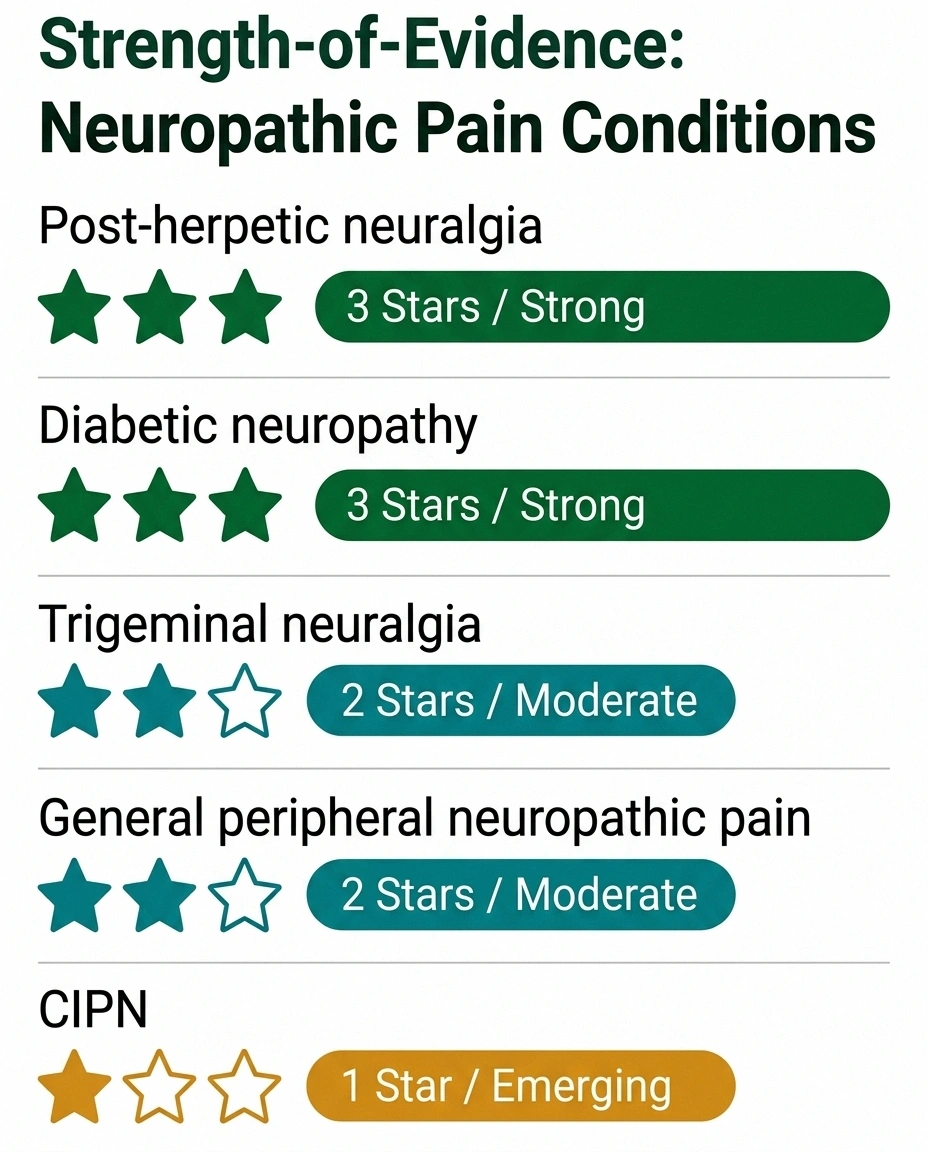
| Condition | Evidence Level |
|---|---|
| Post-herpetic neuralgia (shingles pain) | Strong ✓✓✓ |
| Diabetic peripheral neuropathy | Strong ✓✓✓ |
| Trigeminal neuralgia | Moderate ✓✓ |
| Peripheral neuropathic pain (mixed causes) | Moderate ✓✓ |
| Chemotherapy-induced neuropathy (CIPN) | Emerging ✓ |
Post-herpetic neuralgia (PHN). This is arguably where the evidence is strongest. PHN — the persistent nerve pain that follows a shingles outbreak — is notoriously difficult to treat, and many patients find limited relief from conventional medications. Multiple clinical trials have shown that intradermal injections of botulinum toxin A provide significant, sustained pain reduction in PHN. The relief typically lasts 3–4 months, corresponding to the duration of the toxin's effects. This is one of the best-supported applications.
Diabetic peripheral neuropathy. Several studies have examined botulinum toxin injections in the feet for diabetic neuropathy pain. Results have been generally positive, showing reductions in burning and pain scores. A notable 2016 Lancet Neurology trial (BOTNEP) — a randomized, double-blind, placebo-controlled study — demonstrated that two administrations of botulinum toxin A produced a sustained analgesic effect against peripheral neuropathic pain that lasted beyond the treatment period.
Trigeminal neuralgia. For the severe, electric-shock facial pain of trigeminal neuralgia, botulinum toxin injections have shown meaningful benefit in multiple trials, including patients who had not responded adequately to carbamazepine or other medications.
Peripheral neuropathy from various causes. Case series and smaller studies suggest benefit across different types of peripheral neuropathic pain, including chemotherapy-induced peripheral neuropathy (CIPN) and painful neuropathy from other causes. The evidence here is less robust than for PHN and diabetic neuropathy but growing.
Allodynia (pain from non-painful touch). For patients with allodynia — where even light touch, clothing, or bedsheets cause pain — botulinum toxin injections into the affected skin area have shown particularly interesting results, possibly because of its direct action on the peripheral sensory nerve endings responsible for triggering allodynic responses.
The BOTNEP Trial: A Landmark Study
The BOTNEP trial, published in The Lancet Neurology in 2016, is worth understanding in some detail because it represents one of the most rigorous evaluations of botulinum toxin for neuropathic pain.
The trial enrolled patients with peripheral neuropathic pain from various causes. Participants received two rounds of botulinum toxin A injections or placebo injections, administered months apart. Key findings:
- Both administrations produced significant analgesic effects compared to placebo
- Pain relief was sustained — lasting well beyond what would be expected from the toxin's direct tissue effects alone
- The treatment was well-tolerated with no major safety concerns
- Patients who received botulinum toxin reported improvements in sleep quality and daily function, not just pain scores
What's particularly notable is that the sustained analgesic effect suggests that botulinum toxin may do more than temporarily block pain signals — it may actually reset or recalibrate abnormal pain processing, at least temporarily.
What the Treatment Experience Is Like
If you and your neurologist decide to try botulinum toxin for neuropathic pain, here's what to expect:

Consultation and mapping. Your neurologist will carefully map the area of pain — often marking the skin or identifying specific regions based on where symptoms are most intense. For conditions like diabetic foot neuropathy, the pain distribution is fairly predictable. For post-herpetic neuralgia, it follows the dermatome (skin area) affected by the original shingles rash.
The injection procedure. Botulinum toxin for neuropathic pain is typically injected intradermally (into the skin) or subcutaneously (just below the skin) rather than into muscle. Multiple small injections are given in a grid pattern across the painful area. A typical treatment session might involve 20–50 small injections into the skin of the foot, or across a PHN-affected dermatome on the trunk or face.
The injections use very fine needles, and topical numbing cream is often applied beforehand. Most patients describe the discomfort as mild to moderate — similar to multiple small insect stings. The procedure itself typically takes 15–30 minutes.
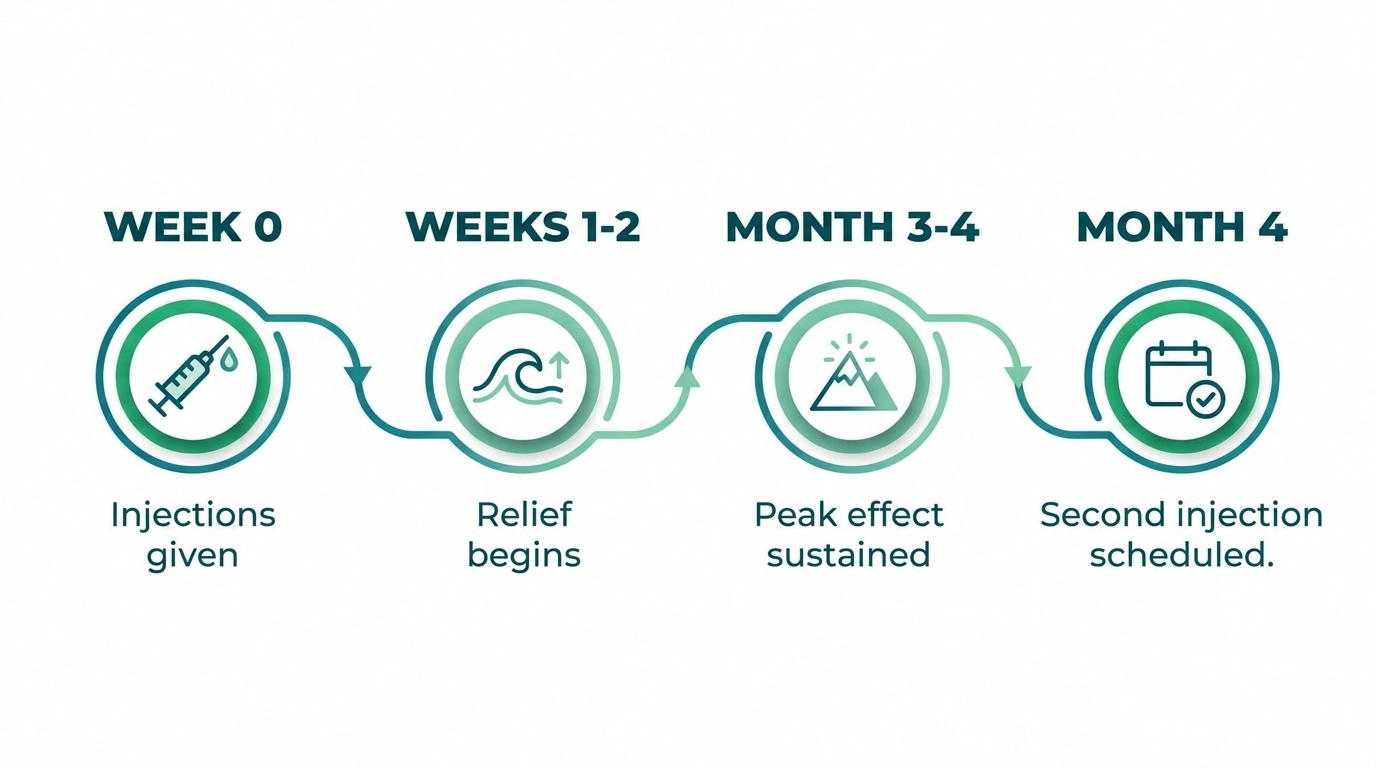
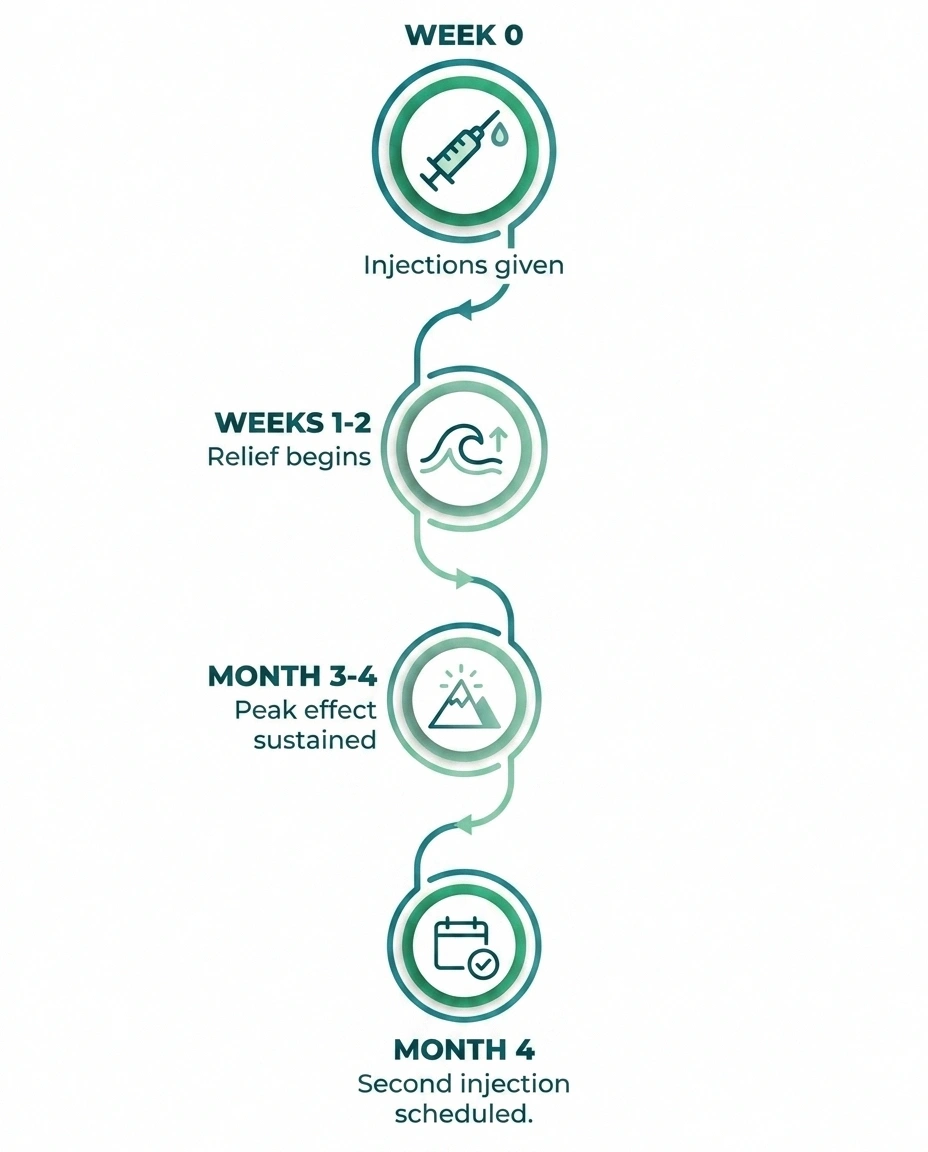
Onset and duration. Pain relief usually begins within 1–2 weeks after injection, as the toxin's effects on sensory nerve terminals develop. Relief typically lasts 3–4 months. Most treatment protocols involve repeat injections every 3–4 months to maintain benefit.
What about muscle weakness? When botulinum toxin is injected intradermally for pain (as opposed to intramuscularly for spasticity or cosmetic purposes), significant muscle weakness is not expected and is generally not observed. The doses used and the injection technique are specifically designed to target sensory nerves without major motor nerve effects.
Who Is a Good Candidate for Botulinum Toxin Treatment?
Botulinum toxin for neuropathic pain is typically considered for patients who:

- Have significant ongoing pain despite adequate trials of conventional medications (gabapentin, pregabalin, duloxetine, amitriptyline, etc.)
- Have a well-defined, localized area of pain that can be specifically targeted with injections
- Have certain specific diagnoses with the strongest evidence base (PHN, diabetic neuropathy, trigeminal neuralgia)
- Cannot tolerate or have contraindications to systemic medications
- Are willing to commit to a series of injections every 3–4 months
It is generally not appropriate for patients with:
- Known allergy or sensitivity to botulinum toxin
- Neuromuscular junction disorders (myasthenia gravis, Lambert-Eaton syndrome)
- Infection at the proposed injection site
- Bleeding disorders or anticoagulant use (relative contraindication)
- Diffuse, widespread, poorly localized neuropathic pain (harder to target)
A conversation with a neurologist experienced in pain management and botulinum toxin therapy is essential to determine candidacy. This is not a treatment you'll receive from your primary care doctor in most cases.
How Does Botox Compare to Other Neuropathy Treatments?
Botulinum toxin occupies a specific niche in the neuropathy treatment landscape. It's not a first-line therapy — standard first-line options include medications like gabapentin, pregabalin, and duloxetine. But it has a place as a specialized option for specific situations.
Compared to other interventional approaches:
- vs. TENS: Botulinum toxin requires a medical procedure but may provide longer-lasting relief than TENS stimulation
- vs. nerve blocks: More sustained effect than most nerve blocks; targets sensory mechanisms rather than just temporarily blocking nerve conduction
- vs. spinal cord stimulation: Less invasive and less expensive than spinal cord stimulation; appropriate for more localized pain
- vs. topical treatments (capsaicin, lidocaine patches): Similar localized approach but potentially longer-lasting effects; different mechanism
One of botulinum toxin's advantages is that it avoids the systemic side effects of oral medications — sedation, cognitive effects, weight gain, and others that many neuropathy patients find burdensome. For older patients who are particularly sensitive to these effects, the targeted, localized nature of the treatment is a real practical advantage.
Insurance Coverage and Practical Considerations
Here's the practical reality: botulinum toxin for neuropathic pain is generally considered off-label use in the United States. The FDA has approved botulinum toxin for many indications (migraine, cervical dystonia, spasticity, etc.), but peripheral neuropathic pain is not among the specific approved indications.
Botulinum toxin for peripheral neuropathic pain is off-label in the US. Insurance coverage is inconsistent — expect to need prior authorization and documentation of failed standard treatments. Discuss costs upfront with your neurologist's office before scheduling. Academic medical centers and pain clinics are most likely to have experienced practitioners.
This creates several practical challenges:
- Insurance coverage is inconsistent and often requires prior authorization and documentation of failed trials of standard therapies
- Not all neurologists offer this treatment; finding one with experience in botulinum toxin for pain specifically (rather than just for cosmetic or dystonia uses) matters
- Out-of-pocket costs can be significant if insurance doesn't cover the treatment
If you're interested in exploring this option, ask your neurologist specifically about their experience with botulinum toxin for neuropathic pain — not just Botox for cosmetic or migraine purposes. Academic medical centers with pain clinics or neurology departments often have more experience with off-label pain applications.
The Research Horizon
Research into botulinum toxin for pain continues to expand. Current areas of investigation include:
- Optimal dosing protocols and injection grid patterns for different pain conditions
- Whether certain subtypes of neuropathic pain (based on sensory profiling — e.g., patients with prominent heat pain vs. cold allodynia) respond better or worse
- Whether botulinum toxin can actually modulate central sensitization in the long term, not just provide temporary relief
- Combination approaches — botulinum toxin plus other interventions
- New formulations designed for better skin penetration or longer duration of effect
Given the current trajectory of neuropathy research, including work on nerve regeneration and novel treatments, the next decade is likely to bring more refined understanding of which patients benefit most from botulinum toxin and how to optimize outcomes.
Frequently Asked Questions
How does Botox help with neuropathy pain?
Botulinum toxin reduces neuropathic pain through several mechanisms independent of its muscle-relaxing effect. It blocks the release of pain-signaling molecules (substance P, glutamate, CGRP) from sensory nerve endings, reduces local neurogenic inflammation, travels up nerve fibers to exert effects in the dorsal root ganglia and spinal cord, and may desensitize overactive sodium channels on pain-sensing nerves. Together, these actions interrupt the peripheral and central sensitization that drives chronic neuropathic pain.
Which types of neuropathy pain respond best to Botox?
Post-herpetic neuralgia (shingles pain) and diabetic peripheral neuropathy have the strongest evidence base. Trigeminal neuralgia and other focal peripheral neuropathic pain conditions also have supporting evidence. Allodynia (pain from light touch) is another condition where botulinum toxin has shown particularly interesting results. Treatment works best when the pain is well-localized and can be specifically targeted with injections.
How long does Botox pain relief last for neuropathy?
Pain relief typically begins within 1-2 weeks after injection and lasts approximately 3-4 months. This corresponds to the duration of the toxin's biological effects on sensory nerve terminals. Most patients require repeat injections every 3-4 months to maintain benefit. Some studies suggest that the pain-relieving effect may actually outlast what would be expected from the toxin's direct tissue effects, suggesting possible longer-term changes in pain processing.
Is Botox for neuropathy FDA-approved?
Botulinum toxin is FDA-approved for many medical conditions including chronic migraine, cervical dystonia, spasticity, and overactive bladder — but not specifically for peripheral neuropathic pain. Its use for neuropathy is considered off-label. This means insurance coverage is inconsistent and requires documentation of need. Off-label use is common in medicine when evidence supports a treatment, and neurologists who specialize in pain management are familiar with this application.
Are the Botox injections for neuropathy painful?
Most patients tolerate the injections well. The procedure involves multiple small intradermal or subcutaneous injections using very fine needles. Topical numbing cream is often applied beforehand. Most people describe the discomfort as mild to moderate — similar to multiple small pin-pricks or insect stings. The procedure typically takes 15-30 minutes. Any local redness or tenderness at injection sites usually resolves within 24-48 hours.
Will Botox cause muscle weakness when used for neuropathy?
When administered by an experienced practitioner using intradermal or subcutaneous injection technique for pain, significant muscle weakness is not expected. The doses and injection depth used for neuropathic pain specifically target sensory nerve endings rather than motor nerve-muscle junctions. This is different from intramuscular injection for spasticity or cosmetic use, which does cause muscle relaxation. Let your practitioner know about any unusual weakness after treatment.
How do I find a doctor who offers Botox for neuropathy pain?
Ask your neurologist specifically about their experience with botulinum toxin for neuropathic pain management (not just for cosmetic or migraine uses). Academic medical centers with neurology departments or dedicated pain clinics are the most likely to offer this. Pain medicine specialists who work with neurologists are another avenue. Be specific when asking — experience with using botulinum toxin for peripheral neuropathy is a distinct subspecialty skill.