The first time my friend Marie's husband almost crumpled in their kitchen, she thought he'd had a stroke. He stood up from the table to refill his coffee, took two steps, said “I need to sit,” and dropped onto the chair like the floor had moved. His blood pressure, taken five minutes later, was a fine 124 over 78. Standing? It had been 76 over 50. He had something most people have never heard of: neurogenic orthostatic hypotension — the kind of standing dizziness that comes from autonomic nerve damage, not a heart problem or a stiff neck.
His neurologist prescribed a drug called droxidopa — brand name Northera. I'd never heard of it either. Marie called me the next day with a stack of questions, and we spent an evening going through them together. This article is the conversation I wish more patients and their families could have before the appointment, so they walk in knowing the right questions to ask.
I'm Janet — a patient advocate, not a doctor — and as always I'll point you back to your prescribing neurologist for anything that touches your own care. The aim here is to demystify the medication, not replace your medical team.
The Problem Droxidopa Is Built to Solve
When you stand up, gravity wants to pool about a half-liter of blood in your legs. A healthy nervous system catches that drop instantly — it constricts blood vessels in the lower body and signals the heart to beat a little harder, so your brain keeps its supply for the second or two it takes to settle into a standing posture.
Key Takeaway
Droxidopa treats neurogenic orthostatic hypotension — the standing-dizzy, blood-pressure-crashes-on-rising problem common in autonomic neuropathy. It supplies the raw material your nervous system uses to constrict blood vessels when you stand, and it carries a serious supine-hypertension warning that shapes how you take it.
In autonomic neuropathy, that reflex is broken. The signal to constrict either doesn't get sent or doesn't get there in time. So when you stand, your blood pressure drops, the brain dips below its happy zone, and you feel:
- Lightheaded, foggy, or like you're about to fade out
- Visually gray or “tunnel-y” for a few seconds
- Wobbly in the knees
- Sometimes nauseated
- And, in the worst cases, all the way to a faint or a fall
This is called neurogenic orthostatic hypotension, often shortened to nOH. The “neurogenic” part is important — it means the cause is nerve, not pump (heart) or pipe (blood vessel). It's a common complication of diabetic neuropathy, Parkinson's disease, multiple system atrophy, pure autonomic failure, and a few other rarer conditions. It's also a leading reason that older adults with these diagnoses end up in the emergency room after a fall.
What Droxidopa Actually Is
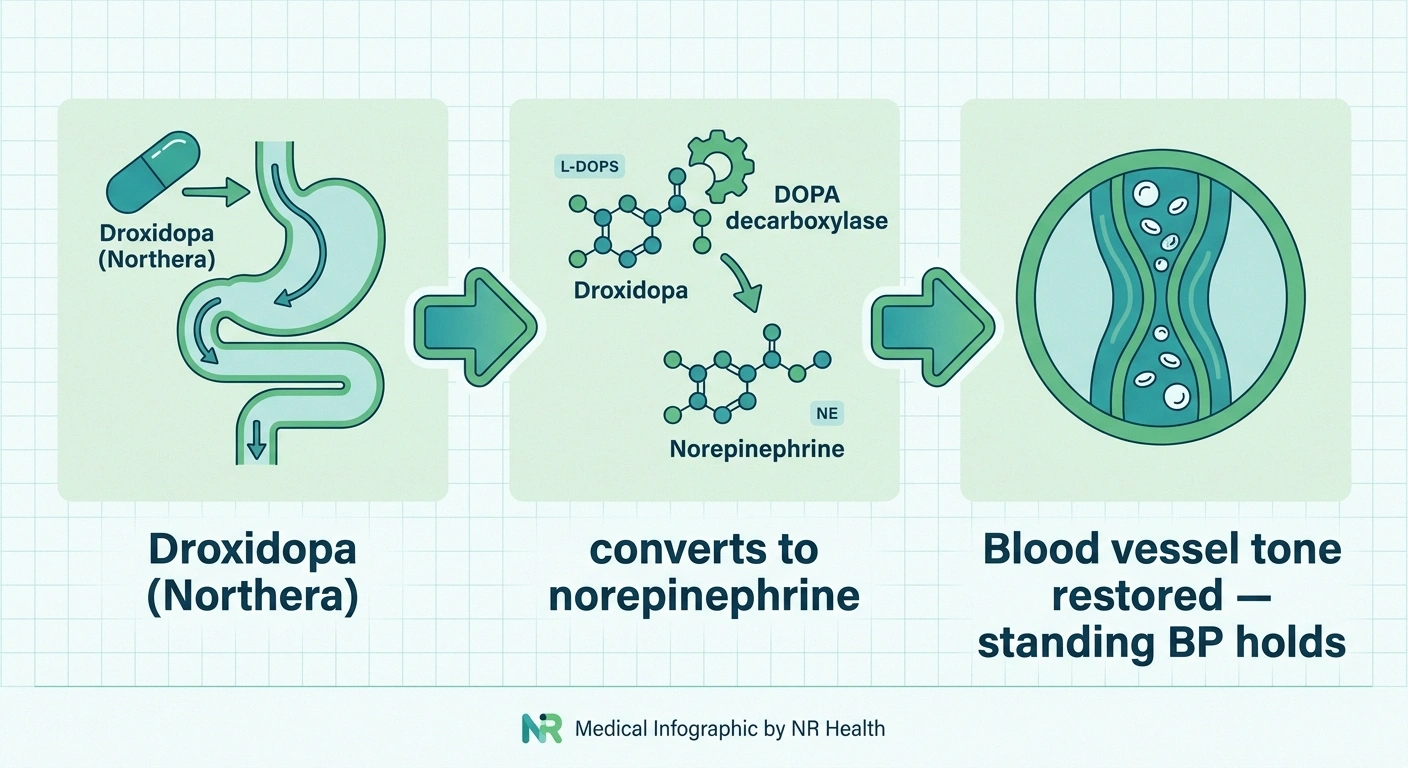
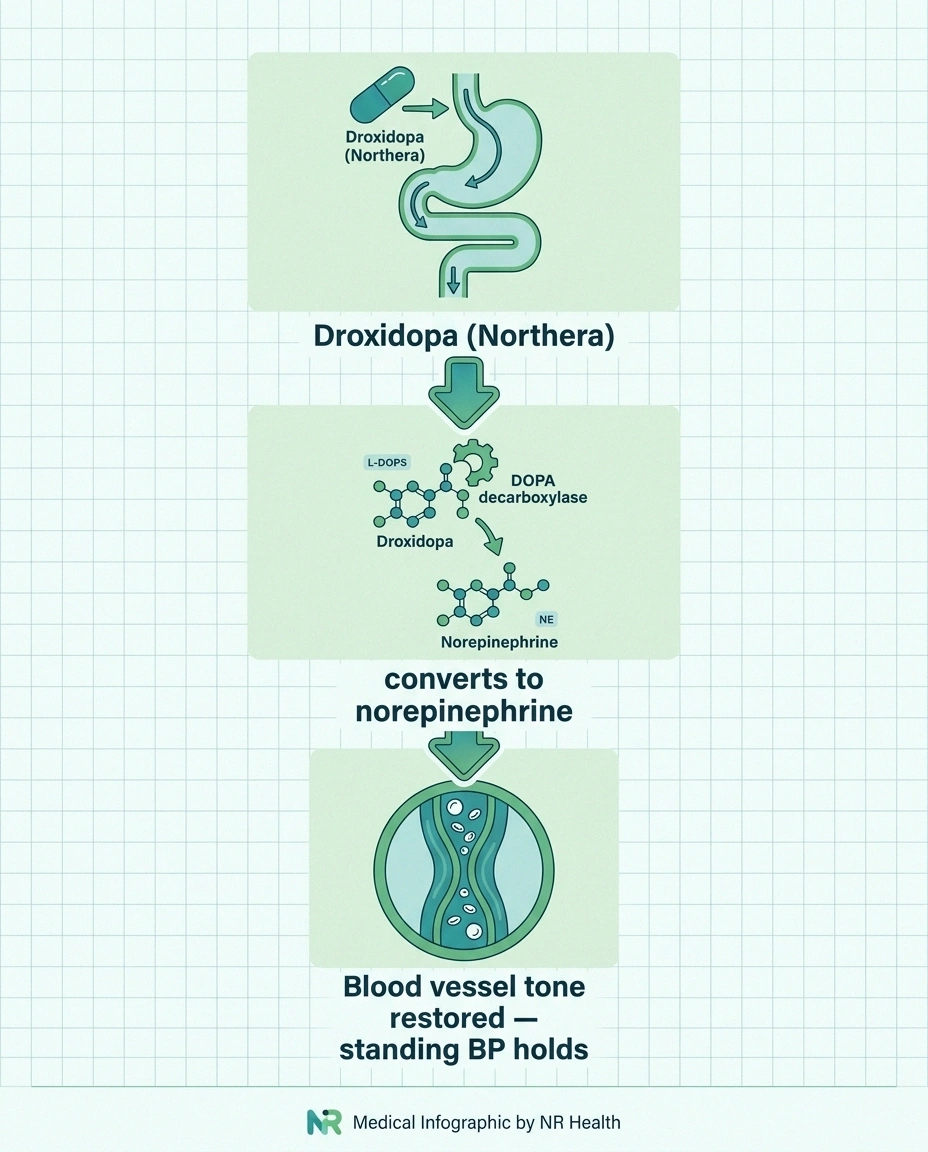
Droxidopa is a synthetic version of a molecule your body almost makes naturally. The full name is L-threo-3,4-dihydroxyphenylserine — but no one says that. Inside the body, an enzyme called DOPA decarboxylase converts droxidopa into norepinephrine. Norepinephrine is the chemical your sympathetic nervous system uses to tell blood vessels to constrict.
From Pill to Blood-Vessel Tone
So the medication doesn't force blood pressure up like a stimulant. It supplies the raw material your nervous system was supposed to make and dispatch on its own, and lets the conversion happen wherever the enzyme is sitting. The end result, when it works, is that when you stand up your blood vessels get the chemical signal they need to tighten — and the dizzy spell either fades or never starts.
It's been FDA-approved since 2014 specifically for symptomatic nOH. That's important: it's not approved for ordinary low blood pressure, not for fatigue, not for general dizziness. It's a narrow tool for a specific problem.
How a Typical Day on Droxidopa Looks
Dosing matters with this drug more than with most. Here's the rhythm a neurologist will usually walk you through.
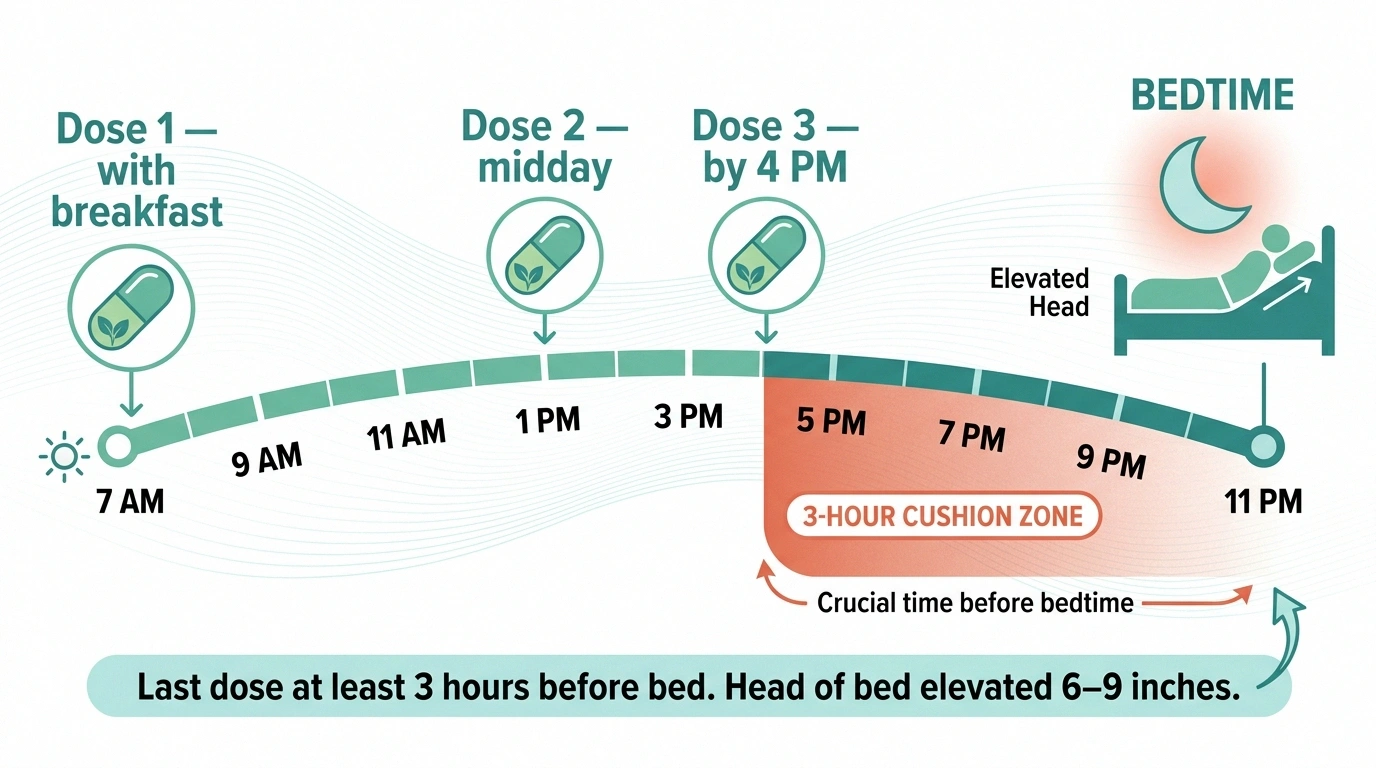
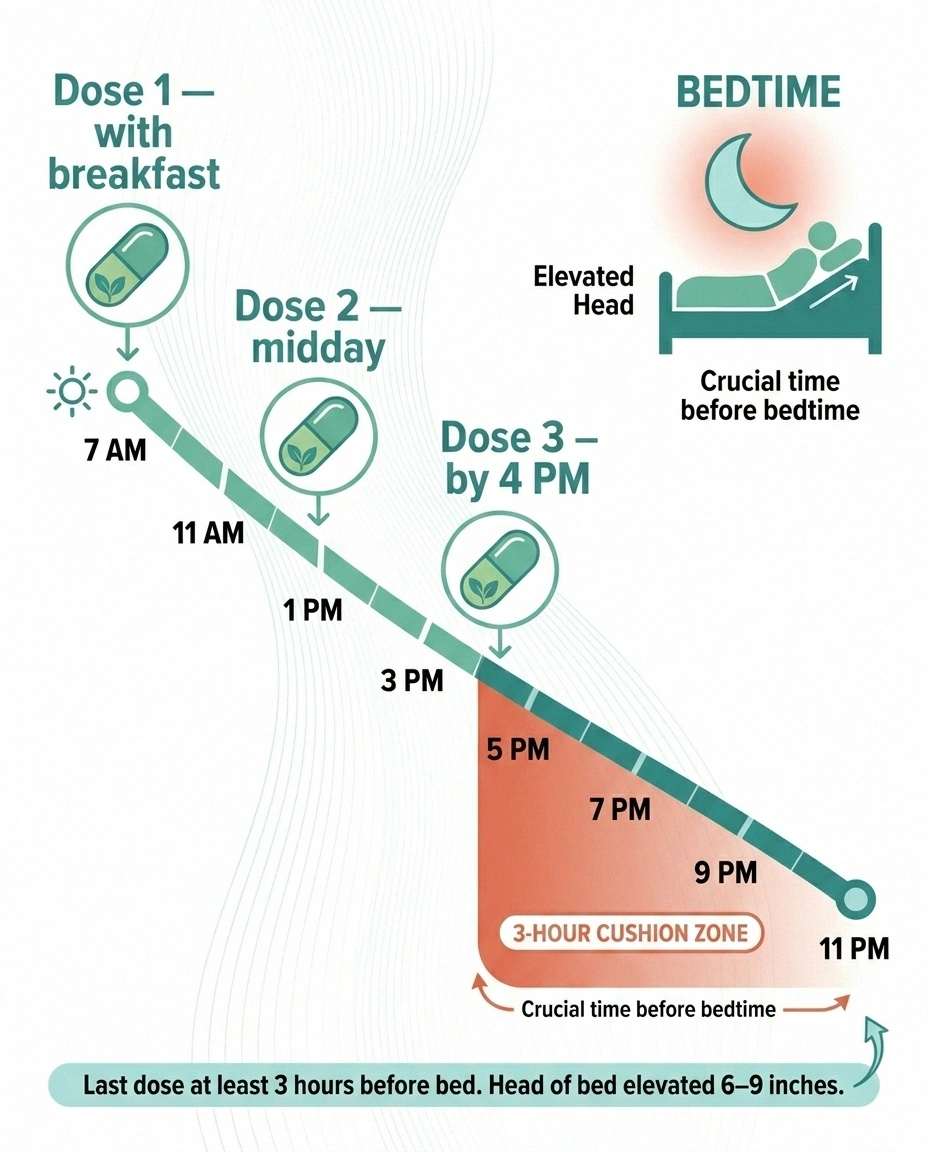
- Three times a day, only while you're awake. Starting dose is typically 100 mg in the morning, 100 mg at midday, and 100 mg in the afternoon.
- Last dose at least 3 hours before bedtime. This is the rule that prevents the most common serious problem — supine hypertension, which we'll cover in detail below.
- Slow titration up. Every day or two, the doctor may add 100 mg to each dose if symptoms aren't controlled and supine blood pressure stays acceptable. Maximum is 600 mg three times a day, or 1,800 mg total per day.
- Take with or without food. Either is fine, but consistency helps you track effect.
- Pair with non-drug strategies. Compression stockings, slow standing, salt and fluid liberalization, head-of-bed elevation. The pill is part of the picture, not the whole picture.
The Boxed Warning Every Patient Has to Hear
Droxidopa carries the FDA's most serious warning category — a boxed warning — for one specific risk: supine hypertension. That's blood pressure that gets dangerously high when you lie down.
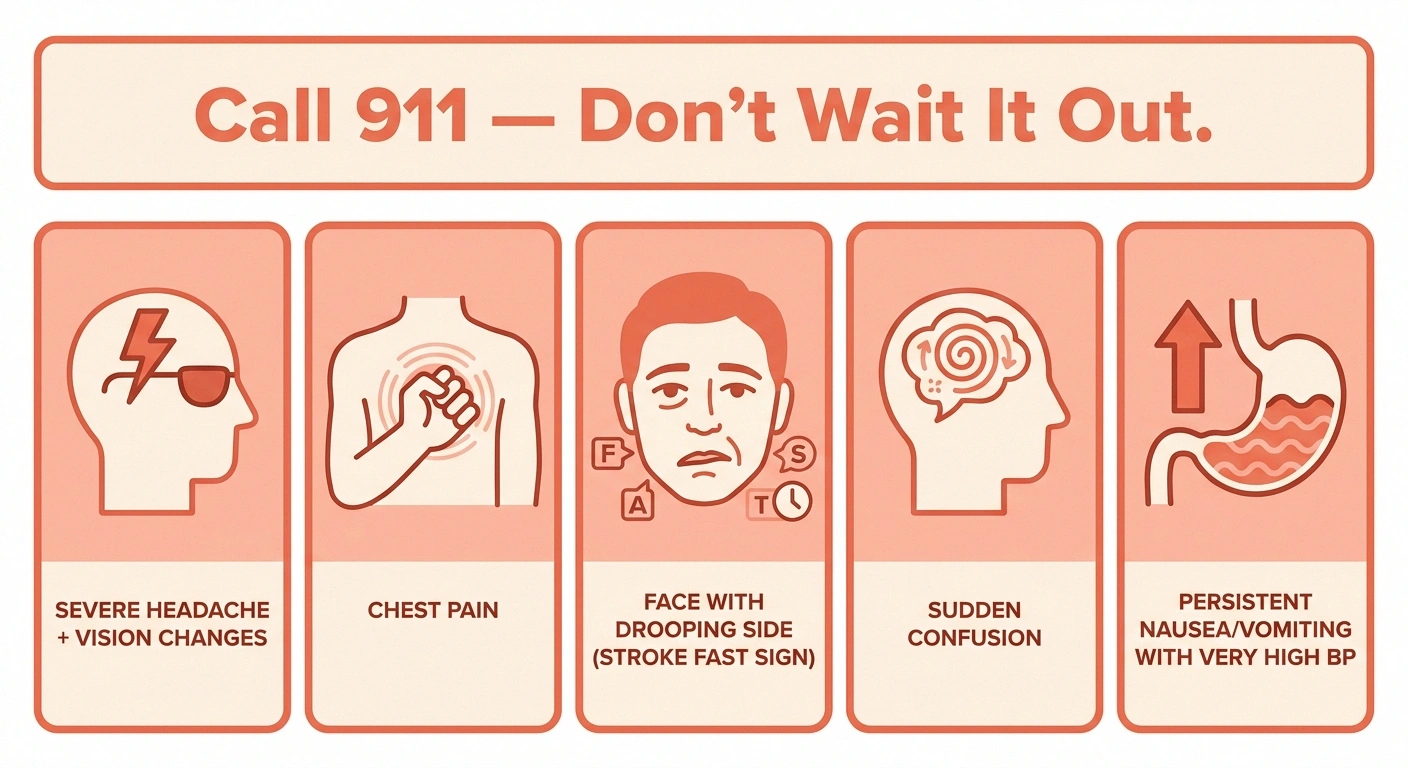
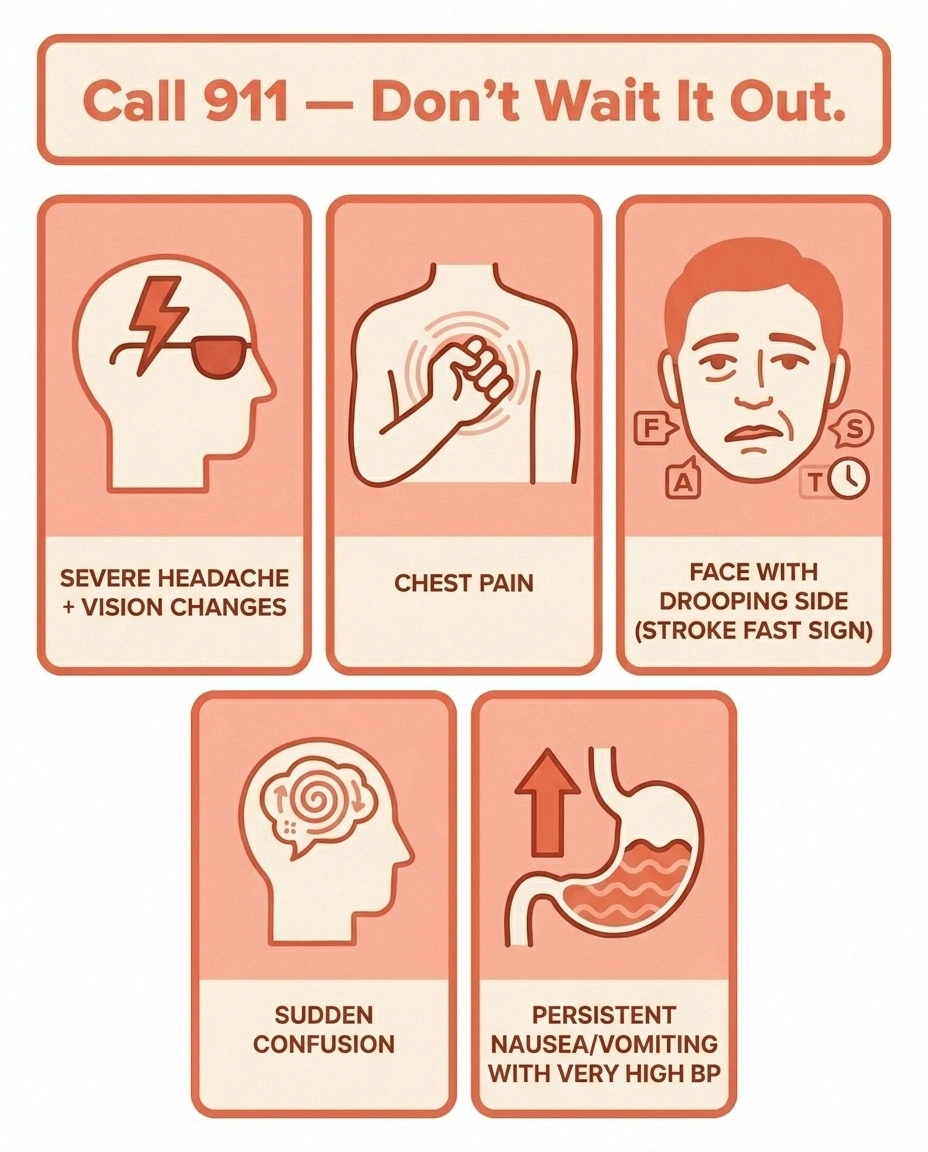
911 If You Notice…
Supine hypertension can spike into a true hypertensive emergency. Don't wait it out — call 911 for any of these while lying down or shortly after:
- Severe pounding headache, especially with vision changes
- Chest pain or pressure
- One-sided weakness or sudden trouble speaking (stroke signs)
- Sudden confusion or significant mental status change
- Persistent nausea or vomiting with a very high BP reading
It's the same property that makes the drug useful. When the medication is in your system and you're upright, it holds your pressure where it should be. When the same medication is in your system and you're flat in bed, the gravitational drain on the lower body disappears, and pressure can climb to numbers that increase your stroke and heart-attack risk.
This is why the protocol almost always includes:
- Sleep with the head of the bed elevated — typically 6 to 9 inches under the head end of the bed frame, not just stacked pillows. Specially made wedge pillows are an alternative.
- Avoid the late-evening dose. Three hours before bed is the minimum cushion.
- Take supine BP readings at home regularly, especially during titration. Your doctor will give a target. Many cardiologists worry once supine systolic crosses 180 mmHg.
- Know the danger signs. Pounding headache with vision changes, chest pressure, sudden confusion, or one-sided weakness while lying down or shortly after is a 911 situation, not a “wait and see.”
I want to be very direct here: if any of those symptoms appear, call emergency services. Don't try to ride it out. Hypertensive emergencies are treatable, but they don't wait politely for a morning appointment.
Side Effects You're Most Likely to Encounter
Beyond the supine-pressure issue, the side effects most commonly reported on droxidopa are usually manageable:
- Headache — the most common complaint, especially in the first couple of weeks. Often dose-related.
- Dizziness — yes, the same symptom you're trying to fix. The body needs to recalibrate. Usually improves after the first two weeks.
- Nausea — taking with a small snack can help.
- Fatigue — varies considerably.
- In Parkinson's disease patients, very occasionally an increase in hallucinations or worsening of pre-existing motor symptoms.
None of these are reasons to white-knuckle through — call the prescriber's office if they persist past two weeks. There are dose adjustments, timing adjustments, or alternative medications that may suit you better.
Does It Keep Working?
This is the question I'd want every patient asking, because the answer matters for how you plan your year.
Titrated upward in 100 mg-per-dose increments every 24–48 hours by your prescriber, only if symptoms aren't controlled AND supine blood pressure remains acceptable.
The initial trials that earned droxidopa its approval showed clear short-term benefit — usually within the first week or two. Longer-term studies have been less consistent. Some patients sustain benefit for months and years. Others find the symptomatic improvement quietly fades after the first one to two weeks, even as their standing blood pressure numbers stay better than baseline.
FDA labeling now reflects this: prescribers are expected to periodically reassess whether the medication is still doing useful work, not just continue it indefinitely. That's a conversation to have at every neurology visit. If symptoms are creeping back, ask whether a brief “drug holiday” might restore responsiveness, or whether a switch or add-on is appropriate.
Droxidopa vs. Midodrine: The Most Common Comparison

Most patients with nOH have heard of midodrine first — it's been around longer and is much cheaper. Both drugs raise standing blood pressure. Both can cause supine hypertension. They take different routes to get there.
Droxidopa vs. Midodrine at a Glance
| Feature | Droxidopa (Northera) | Midodrine |
|---|---|---|
| Mechanism | Norepinephrine precursor (needs enzyme) | Direct alpha-1 receptor agonist |
| Onset | ~1–2 hours | 30–60 minutes |
| Duration | ~4–6 hours | ~3–4 hours |
| Dose schedule | 3× daily, last dose 3+ hrs before bed | 3× daily, last dose 3+ hrs before bed |
| Supine HTN risk | Yes — boxed warning | Yes — boxed warning |
| Common AEs | Headache, dizziness, nausea | Scalp tingling, urinary urgency |
| Typical cost | Brand only — thousands/mo without insurance | Generic — often under $25/mo |
- Midodrine is a direct stimulator of the alpha-1 receptors on blood vessels — it skips the “convert to norepinephrine” step and just pushes the constriction button directly. It works fast (30 to 60 minutes), peaks in about an hour, and wears off in about four. Cheap as generics go. Side effects: scalp tingling, “goosebump” sensation, urinary urgency.
- Droxidopa goes through the natural enzyme pathway and produces norepinephrine that the nervous system then uses. Onset is similar, duration is similar, but it may work in patients who don't respond to midodrine because the underlying problem is norepinephrine availability rather than receptor function.
Cost is the elephant in the room. Midodrine generic is usually under $25 a month with insurance. Droxidopa is brand-only, and the retail price runs in the thousands of dollars per month — almost always requiring insurance prior authorization and often a patient assistance program from the manufacturer.
Most neurologists try midodrine first. Patients who don't respond, who can't tolerate it, or whose insurer approves droxidopa for a specific clinical reason may end up on the newer drug. Some patients benefit from a combination, with careful monitoring.
The Lifestyle Side That Makes the Medication Work Better
Almost every neurologist I've heard from on this topic says the same thing: the pill works best when the daily habits around it are dialed in. None of these are optional add-ons. They're part of the treatment.
A Day That Helps Your Medication Work
- Slow position changes. Sit on the edge of the bed for 30 seconds before standing. Stand still for another 30 seconds before walking.
- Compression stockings. Knee-high or thigh-high medical-grade (20–30 mmHg or as prescribed). Put them on before getting out of bed in the morning.
- Salt and fluid. Unless contraindicated by heart failure or kidney disease, most nOH patients are advised to increase salt intake and target around 2 liters of fluid a day.
- Crossing the legs and tensing leg muscles when standing — a small physical-counterpressure trick that buys time during pressure dips.
- Avoid hot showers, hot weather, large meals, and alcohol when possible — all worsen the standing drop.
- Plan for the fall risk regardless. Read up on fall-prevention strategies and grab-bar placement; even a well-controlled patient can have a bad day.
When Droxidopa Isn't the Right Choice
This medication is not for everyone. The prescriber should pause and reconsider if you have:
- Severe heart disease, especially recent heart attack or unstable angina
- Uncontrolled high blood pressure at baseline
- Severe kidney disease, especially on dialysis
- A history of stroke or transient ischemic attack
- A previous serious allergic reaction to droxidopa or any of its components
It also has documented interactions with several other medication classes, most notably MAO inhibitors (some Parkinson's drugs and older antidepressants), certain triptan migraine drugs, and other vasopressor agents. Your pharmacist's drug-interaction review at the time of filling is a real safety check — don't wave it off.
Some patients also discover their dizziness isn't purely autonomic. It can be made worse by dehydration, by certain other medications (some of which are themselves listed in medications that can cause neuropathy), or by an undiagnosed cardiac issue. A thorough neurologic and cardiac workup before starting droxidopa is standard for a reason.
What This Looks Like When It's Going Well

Marie's husband, the one whose story opened this article, has been on droxidopa for almost a year now. Three doses a day, last one by 4 p.m. Head of the bed up six inches. He wears thigh-high stockings every day, drinks more water than he'd like, and salts his food cheerfully. His standing pressure is now mostly in the 110s systolic instead of the 70s. He hasn't fallen since the second month. His supine evening readings, which his cardiologist watches like a hawk, stay under 160.
It is, in his words, “annoying as hell to manage, but I'm not crashing into the furniture anymore.” That tradeoff is most of what this drug is — a real symptom relief that demands real day-in, day-out attention to the warning signals. For the right patient with the right team, that's a fair trade.
If your prescriber is bringing it up, ask them three questions: What supine blood pressure number should make me call? When do we reassess whether it's still working? What's my plan B if I can't tolerate it? Those three questions launch the right conversation, every time.
Frequently Asked Questions
Is droxidopa the same as Northera?
Yes. Droxidopa is the generic name of the active medication, and Northera is the brand name under which it is sold in the United States. Both refer to the same drug. As of 2026, there is no FDA-approved generic version available in the US, so all prescriptions in the United States are dispensed as Northera.
How fast does droxidopa start working?
Most patients feel some symptomatic improvement within one to two hours of the first dose. The maximal short-term benefit is usually evident in the first one to two weeks of consistent dosing. Whether that benefit sustains long-term varies significantly from patient to patient, which is why the prescribing label recommends periodic reassessment.
Can I take droxidopa if I have diabetes-related autonomic neuropathy?
Yes — diabetic autonomic neuropathy with symptomatic neurogenic orthostatic hypotension is one of the conditions droxidopa is approved to treat. The same boxed warning about supine hypertension applies, and patients with longstanding diabetes often need extra coordination between their endocrinologist, neurologist, and cardiologist because of overlapping cardiovascular risk.
What time should I take my doses?
A common schedule is the first dose with breakfast, the second around midday, and the third in mid-afternoon — never within three hours of bedtime. Your prescriber will personalize this based on when your standing dizziness is most bothersome and how your supine pressure responds.
Does droxidopa interact with my Parkinson's medications?
It can. Carbidopa, which is part of carbidopa-levodopa (Sinemet), inhibits the enzyme that converts droxidopa to norepinephrine — so the two drugs together require careful timing and dose adjustment. MAO-B inhibitors used in Parkinson's (rasagiline, selegiline) can amplify droxidopa's effect on blood pressure. Always confirm timing with the neurologist managing your Parkinson's care.
What if I miss a dose?
Skip the missed dose if it's close to the next scheduled one or close to bedtime. Don't double up — the supine hypertension risk goes up sharply if you take two doses too close together. Resume your normal schedule with the next dose.
How will I know if my supine blood pressure is too high?
You won't always feel it, which is why home monitoring matters. Take a reading after you've been lying down for five minutes, especially in the evening before your bedtime cushion. A persistent supine systolic reading above the number your doctor specified (often 160 to 180 mmHg) is a reason to call. A reading paired with severe headache, chest pain, vision changes, confusion, or weakness is a 911 call.
Is droxidopa covered by insurance?
Most US insurers cover it with a prior authorization that documents the diagnosis of symptomatic neurogenic orthostatic hypotension and, in many cases, a trial of cheaper alternatives like midodrine first. Out-of-pocket without coverage runs into the thousands of dollars per month. The manufacturer offers a patient assistance program that's worth asking your prescriber's office about.


