
When medications, lifestyle changes, and other treatments haven't provided enough relief from neuropathy pain, your doctor may bring up a treatment that sounds almost like science fiction: spinal cord stimulation (SCS). A small device implanted near your spine sends mild electrical pulses that interrupt pain signals before they reach your brain. It's been called a “pacemaker for pain” — and for some neuropathy patients, it's been genuinely life-changing.
But spinal cord stimulation isn't right for everyone, and the decision to pursue it deserves honest, unbiased information — not a sales pitch from a device manufacturer or a clinic that profits from the procedure. In this article, I'll walk you through how SCS works, what the research actually shows, what the experience is like from a patient's perspective, and the questions you should ask before making this decision.
How Spinal Cord Stimulation Works
The basic idea behind spinal cord stimulation is surprisingly simple, even if the technology is sophisticated. Here's what happens:
The Gate Control Analogy
Think of your spinal cord as a gate between your body and brain. Pain signals travel through this gate to reach your brain. Spinal cord stimulation sends mild electrical pulses that help close the gate, reducing the number of pain signals that get through. It also boosts GABA — your body's natural braking system for pain signals.
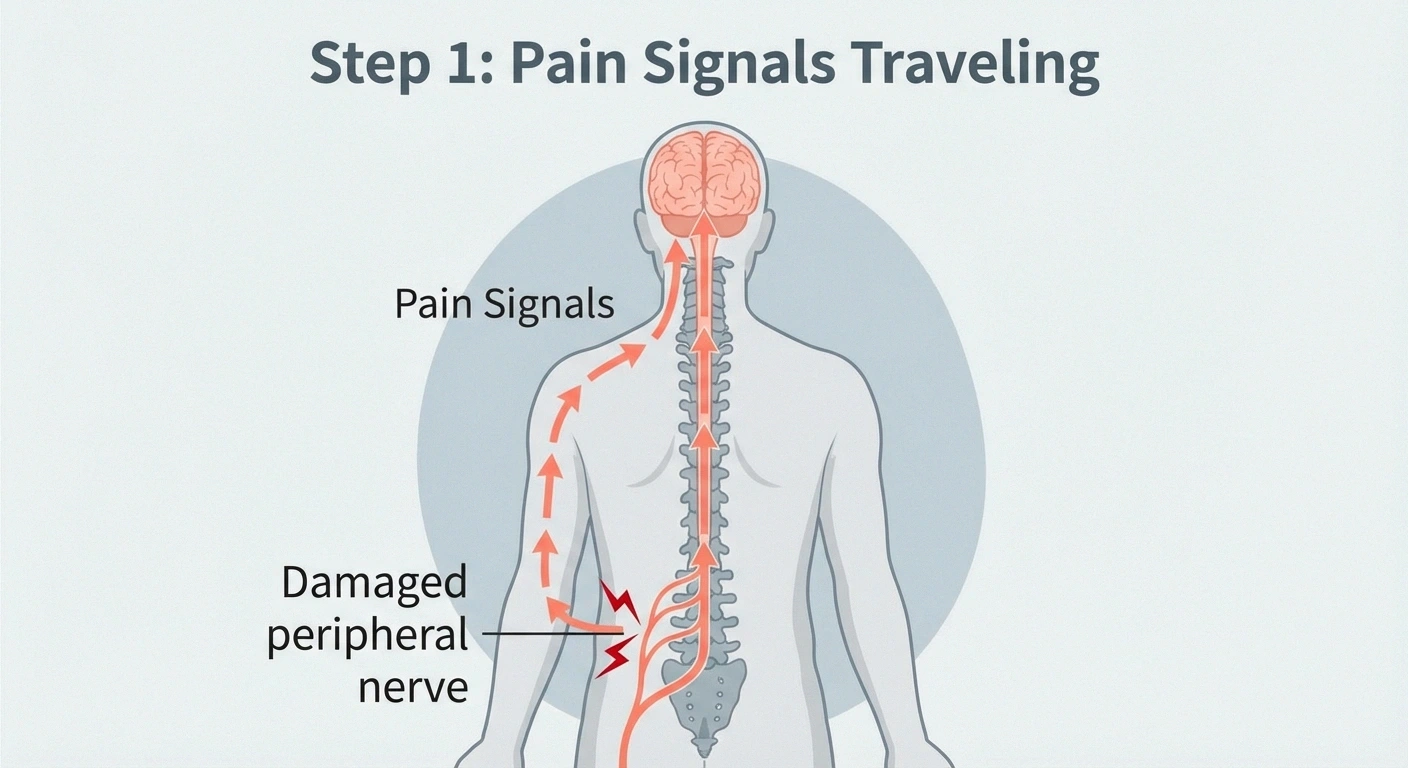
A thin wire with tiny electrodes (called a lead) is placed in the epidural space — the area just outside the protective membrane surrounding your spinal cord. This lead connects to a small pulse generator (about the size of a thick credit card) that's typically implanted under the skin near your hip or buttock.
The device sends controlled electrical pulses to the spinal cord, which modify or override the pain signals traveling from your damaged peripheral nerves to your brain. It doesn't fix the nerve damage itself — it changes how your brain receives and interprets the pain signals.
The science behind this goes back to the gate control theory of pain, first proposed in 1965 and put into clinical practice by Dr. Norman Shealy in 1967. The theory suggests that the spinal cord acts as a “gate” for pain signals. By stimulating certain nerve fibers, you can essentially close that gate, preventing pain signals from passing through to the brain. Modern SCS technology has evolved far beyond the original concept, but the core principle remains.
One important mechanism involves the neurotransmitter GABA — the same inhibitory chemical that gets depleted when neuropathy damages the pain-control circuits. SCS has been shown to boost GABA activity in the spinal cord, helping restore the natural braking system that neuropathic pain disrupts.
Types of Spinal Cord Stimulation
SCS technology has evolved significantly over the past decade. The three main types you should know about:
SCS Stimulation Types Compared
Tonic
40-80 Hz
Traditional Stimulation
Produces a tingling sensation (paresthesia) that replaces or masks pain. Some patients find it pleasant; others prefer paresthesia-free options.
HF10
10,000 Hz
High-Frequency Stimulation
Paresthesia-free — no tingling sensation. Specifically studied for diabetic peripheral neuropathy. Many patients prefer this option.
Burst
Grouped
Burst Stimulation
Mimics natural nerve firing patterns. May target the emotional/suffering component of pain through different brain pathways.
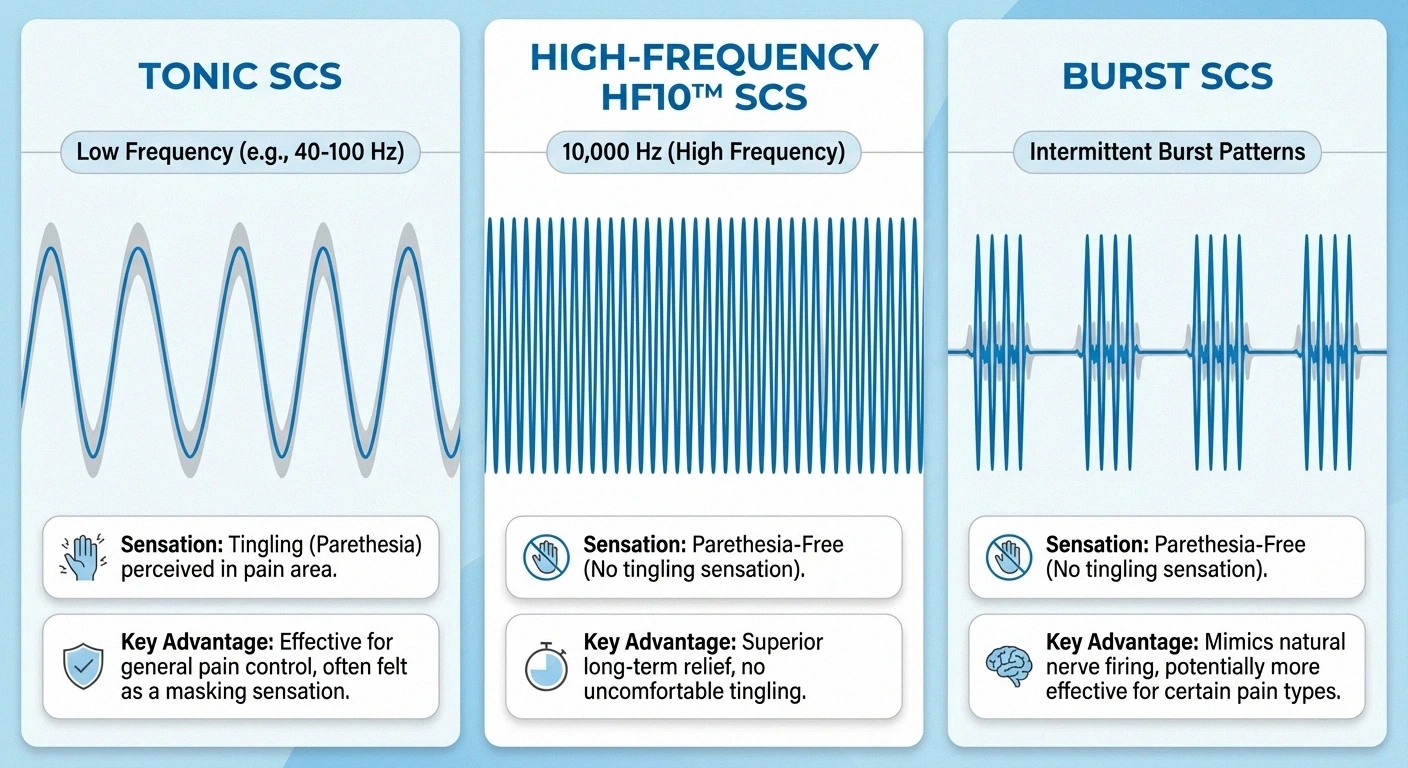
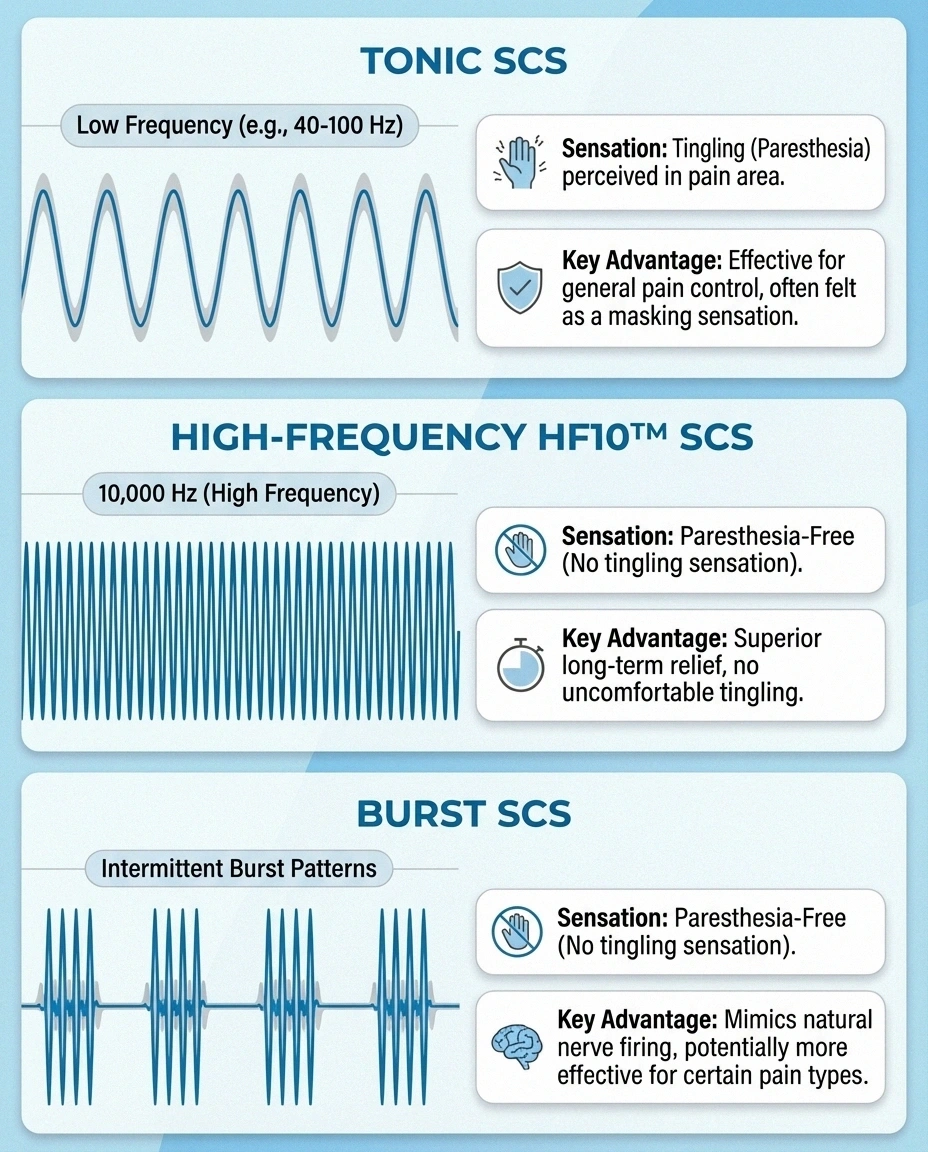
Traditional (tonic) stimulation delivers a constant, rhythmic pulse that produces a tingling sensation (called paresthesia) in the areas where you normally feel pain. The idea is that this tingling replaces or masks the pain signal. Some patients find the tingling pleasant or neutral; others find it bothersome over time.
High-frequency stimulation (HF10) uses a much higher pulse rate — 10,000 Hz compared to the traditional 40-80 Hz — and doesn't produce the tingling sensation. This “paresthesia-free” approach has been popular because many patients prefer pain relief without having to feel continuous tingling. The HF10 system was specifically studied in diabetic peripheral neuropathy.
Burst stimulation delivers electrical pulses in closely spaced groups (bursts) that more closely mimic natural nerve firing patterns. Research suggests burst stimulation may be particularly effective for the emotional component of pain — the suffering aspect — because it targets different brain pathways than tonic stimulation.
Many modern SCS systems can deliver multiple stimulation types, allowing your doctor to adjust the programming to find what works best for you. This adaptability is one of the advantages of newer systems.
What the Research Shows for Neuropathy
SCS was originally developed for conditions like failed back surgery syndrome and complex regional pain syndrome. Its application specifically for peripheral neuropathy — particularly diabetic peripheral neuropathy (DPN) — is more recent, and the evidence is growing.
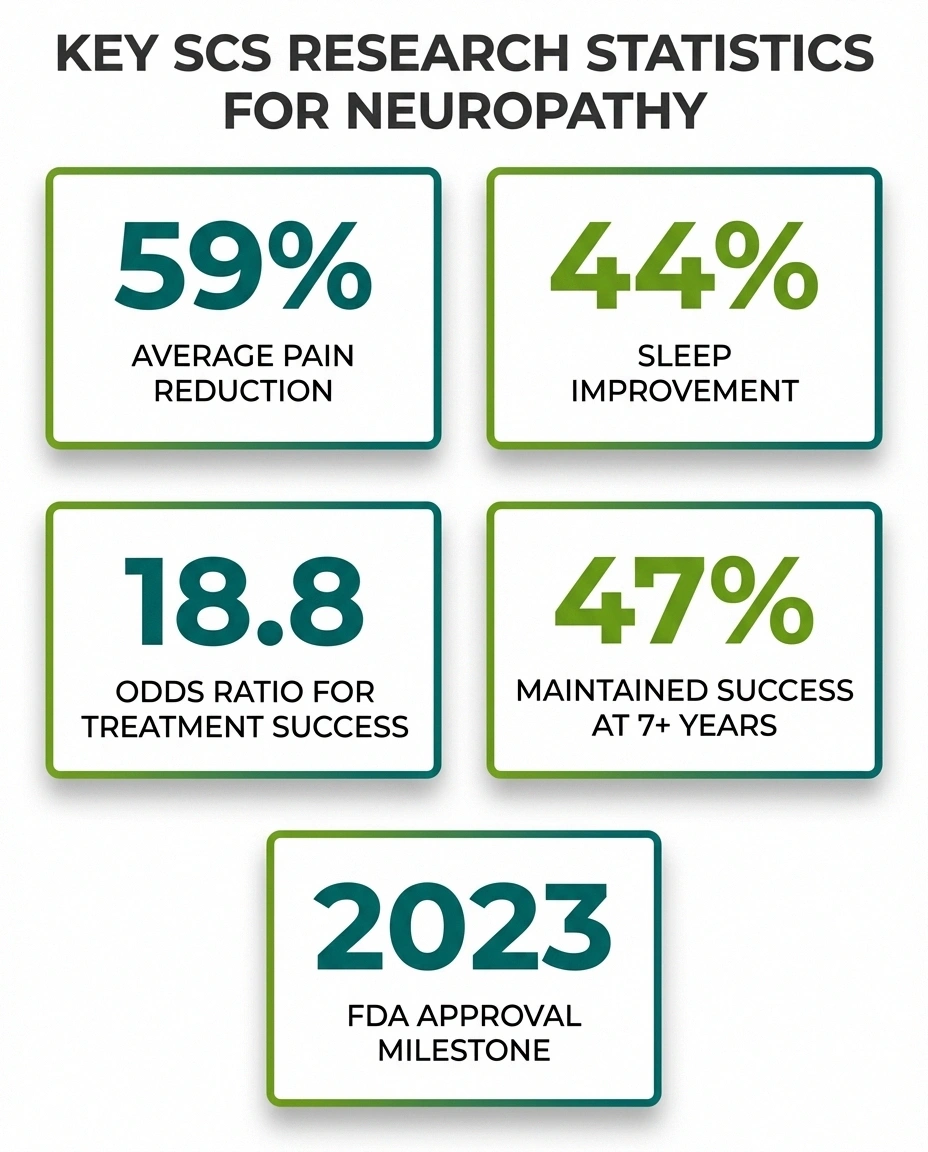
Key Research Results for SCS in Neuropathy
59%
Average Pain Reduction
44%
Sleep Quality Improvement
47%
Success at 7+ Years
2023
First FDA Approval for DPN
Results from randomized controlled trials. Individual outcomes vary. The mandatory trial period helps predict your personal response.
Here are the key research findings:
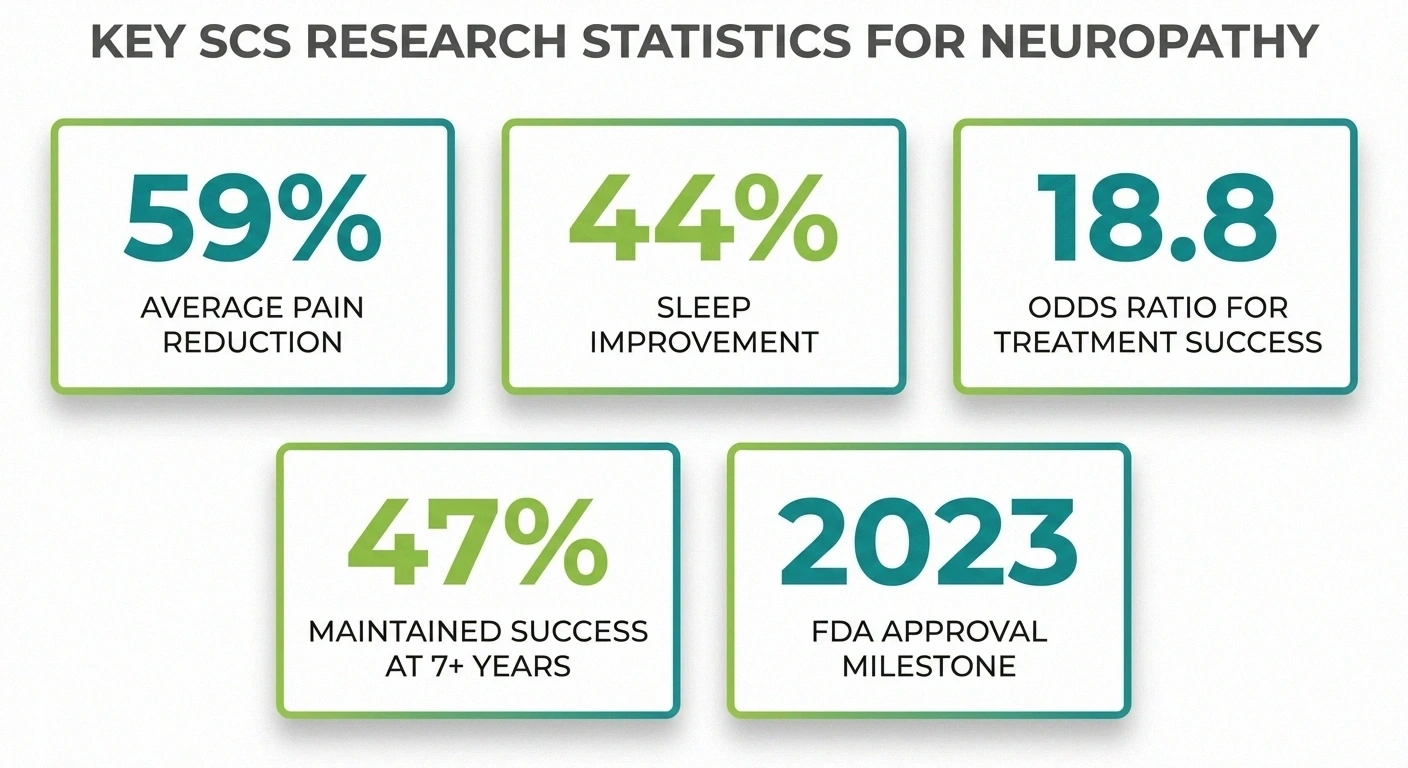
The landmark 2014 Diabetes Care study was a randomized controlled trial that compared SCS plus best medical treatment against best medical treatment alone for painful diabetic neuropathy. The results were striking: the odds ratio for treatment success with SCS was 18.8, meaning patients receiving SCS were nearly 19 times more likely to achieve significant pain relief. Patients reported an average 59% reduction in pain and 44% improvement in sleep quality.
Long-term follow-up data from the same research group showed that 47% of patients maintained successful outcomes at 87 months (over 7 years) of follow-up. This is significant because many pain treatments lose effectiveness over time, and maintaining nearly half of patients at success thresholds for over 7 years suggests real durability.
The 2023 FDA approval of Abbott's Proclaim XR system specifically for painful diabetic peripheral neuropathy was a milestone. This was the first SCS system to receive a specific FDA indication for DPN, marking a shift from off-label use to an officially recognized treatment for neuropathy.
A 2026 review in Neurosurgical Review found that patients with neuropathic pain of peripheral nerve origin (like diabetic neuropathy) had significantly better outcomes with SCS than patients with spinal cord lesion pain, with an odds ratio of 9.60 for favorable outcomes. This suggests that SCS may be particularly well-suited for the type of nerve pain that neuropathy patients experience.
These numbers are encouraging, but context matters. Research studies often involve carefully selected patients in specialized centers. Real-world results may vary, and not every patient will achieve the same degree of relief.
The Trial Period: What to Actually Expect
One of the most important aspects of SCS — and one that sets it apart from many other treatments — is the mandatory trial period. Before getting a permanent implant, you undergo a trial lasting approximately 5 to 10 days to determine if SCS provides meaningful relief for your specific pain.
The SCS Trial-to-Decision Journey
Evaluation & approval — medical assessment, insurance authorization, psychological evaluation
Trial lead placement — minimally invasive, local anesthesia, outpatient procedure
Living with the trial — 5-10 days at home, evaluating pain relief during normal activities
Decision point — based on your trial results:
✓ 50%+ pain relief? → Schedule permanent implant (2-4 weeks later)
✗ Not enough relief? → Leads removed, no commitment, valuable information gained
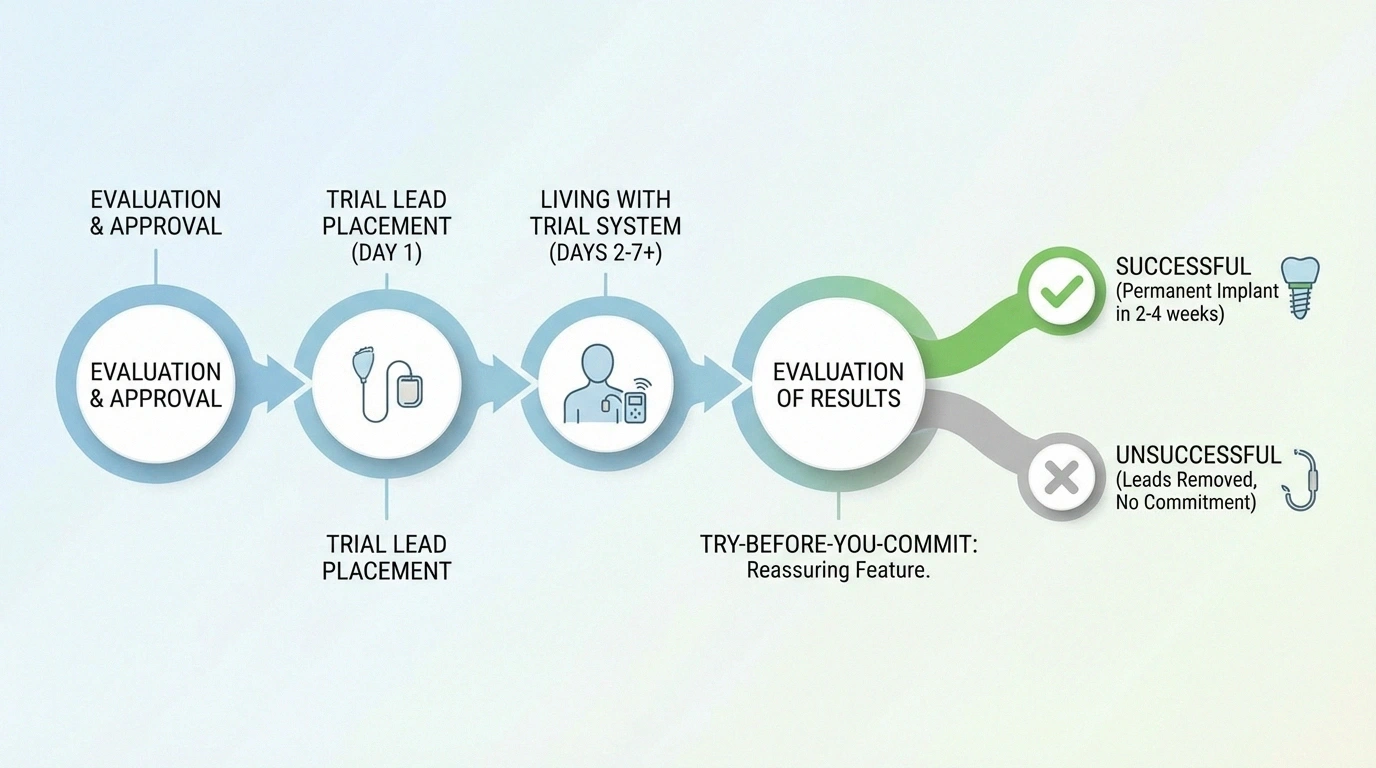
During the trial: Temporary leads are placed through a needle (no major surgery) into the epidural space, usually under local anesthesia and sedation. The leads extend outside your body and connect to an external pulse generator that you wear on a belt. You go home with the temporary system and live your normal life while evaluating the results.
What you're evaluating: The standard benchmark for a “successful” trial is typically a 50% or greater reduction in pain. But beyond the numbers, you're assessing whether the relief meaningfully improves your daily life — your ability to sleep, walk, participate in activities, and reduce pain medications. Keep a detailed pain diary during the trial.
What many patients experience: The trial period can feel strange. Having wires emerging from your back for a week requires care to prevent infection. You'll need to avoid showering (sponge baths instead) and limit certain movements. Some people feel the trial is inconvenient but manageable; others find it uncomfortable. Your medical team will provide specific instructions for care during this period.
If the trial succeeds: You'll be scheduled for permanent implant surgery, typically 2 to 4 weeks after the trial. The permanent system has no external wires — everything is implanted under the skin.
If the trial doesn't work: The temporary leads are simply removed. You've lost nothing except a week of your time, and you have definitive information that SCS isn't the right approach for your pain. This try-before-you-commit feature is genuinely valuable.
Who May Be a Good Candidate
SCS tends to work best for patients who meet certain criteria:
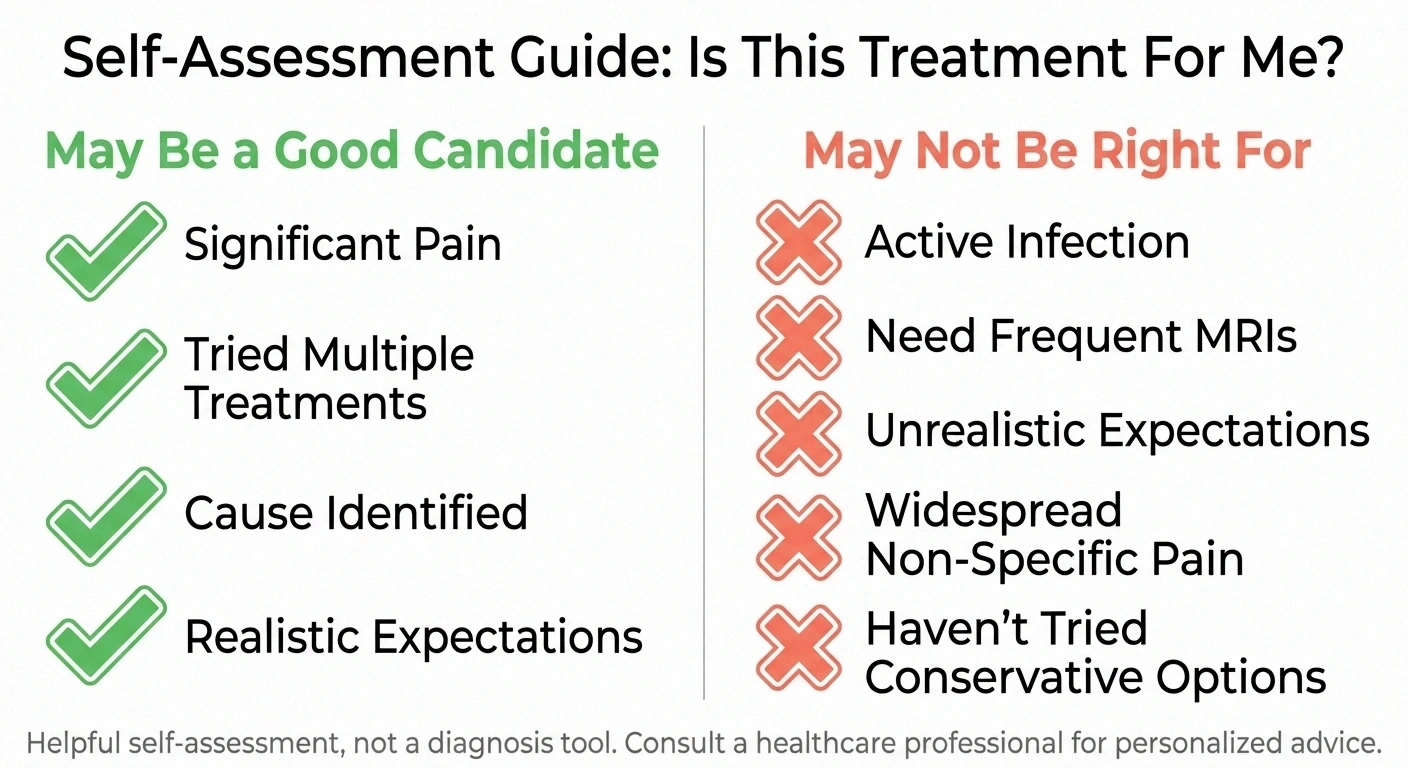
— You have significant neuropathic pain (typically rated 5 or higher on a 10-point scale) that substantially impacts your quality of life
— You've tried multiple conservative treatments — medications like gabapentin, pregabalin, or duloxetine, physical therapy, and possibly other approaches — without adequate relief
— You don't have untreated psychological conditions that might affect your ability to evaluate the treatment
— You're willing to commit to the trial process and ongoing follow-up appointments
— The underlying cause of your neuropathy has been identified and is being managed (for diabetic neuropathy, this means blood sugar is under reasonable control)
Who May NOT Be a Good Candidate
Honest patient education means discussing who SCS is not right for — something many promotional materials skip:
— Patients with active infections — implanting a device near the spine carries infection risk, and existing infections must be resolved first
— Patients on blood thinners who cannot safely pause them for the procedure
— Patients who need frequent MRIs — while many newer SCS systems are MRI-conditional, there are still significant limitations on what types of MRIs you can have
— Patients with unrealistic expectations — SCS rarely eliminates pain completely. The goal is meaningful reduction, not zero pain
— Patients with widespread, non-specific pain — SCS works best for pain in defined areas that can be targeted by lead placement
— Patients who haven't adequately tried conservative options — insurance companies typically require documentation of failed conservative treatments before approving SCS
If you're being told you're a “perfect candidate” by a clinic without thorough evaluation and a frank discussion of limitations, consider getting a second opinion.
Risks and Potential Complications
Like any surgical procedure, SCS carries risks that you should understand before making a decision:
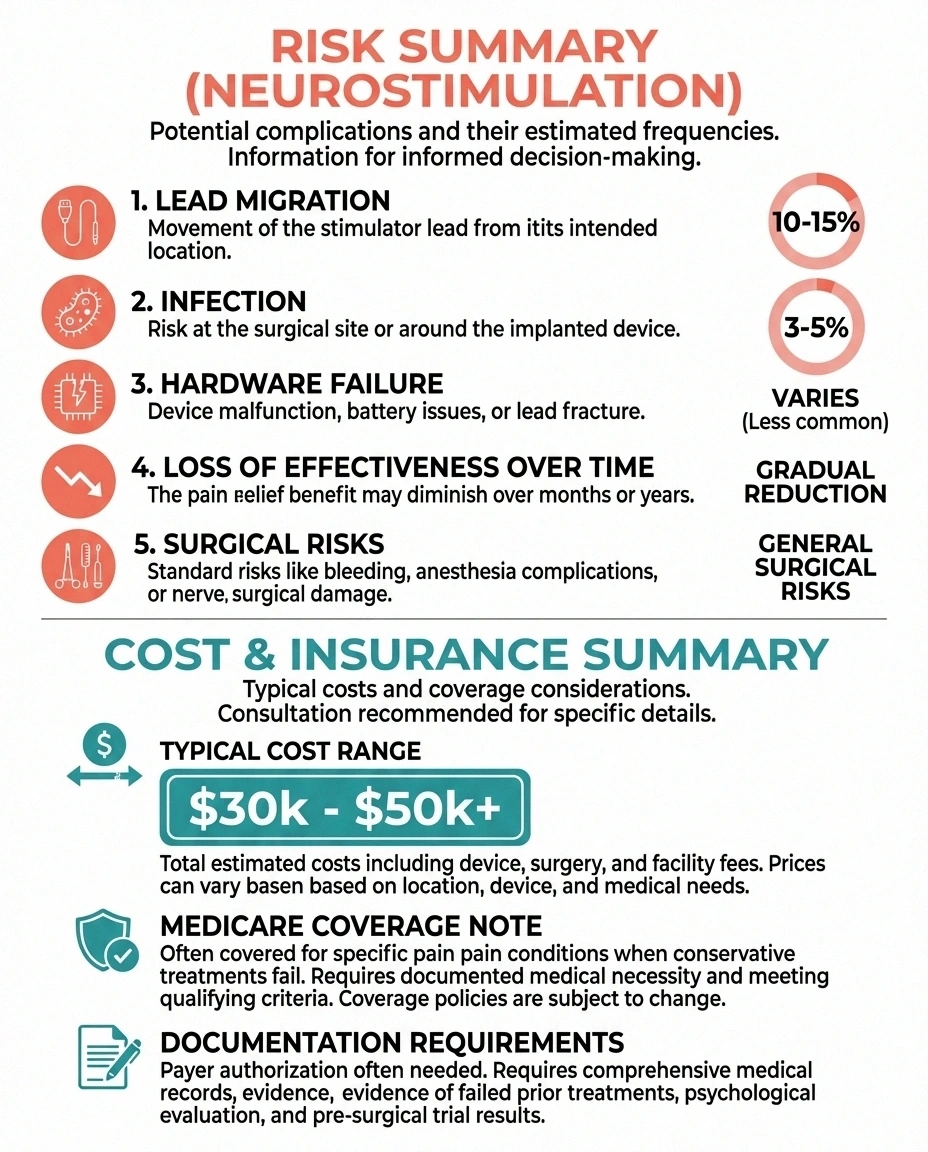
Know the Risks
Lead migration: ~10-15% of cases (usually correctable with minor revision)
Infection: ~3-5% of cases (most treatable, severe cases may need device removal)
Diminished effectiveness: Over half of initial responders see reduced benefit over 7+ years. Reprogramming can sometimes help.
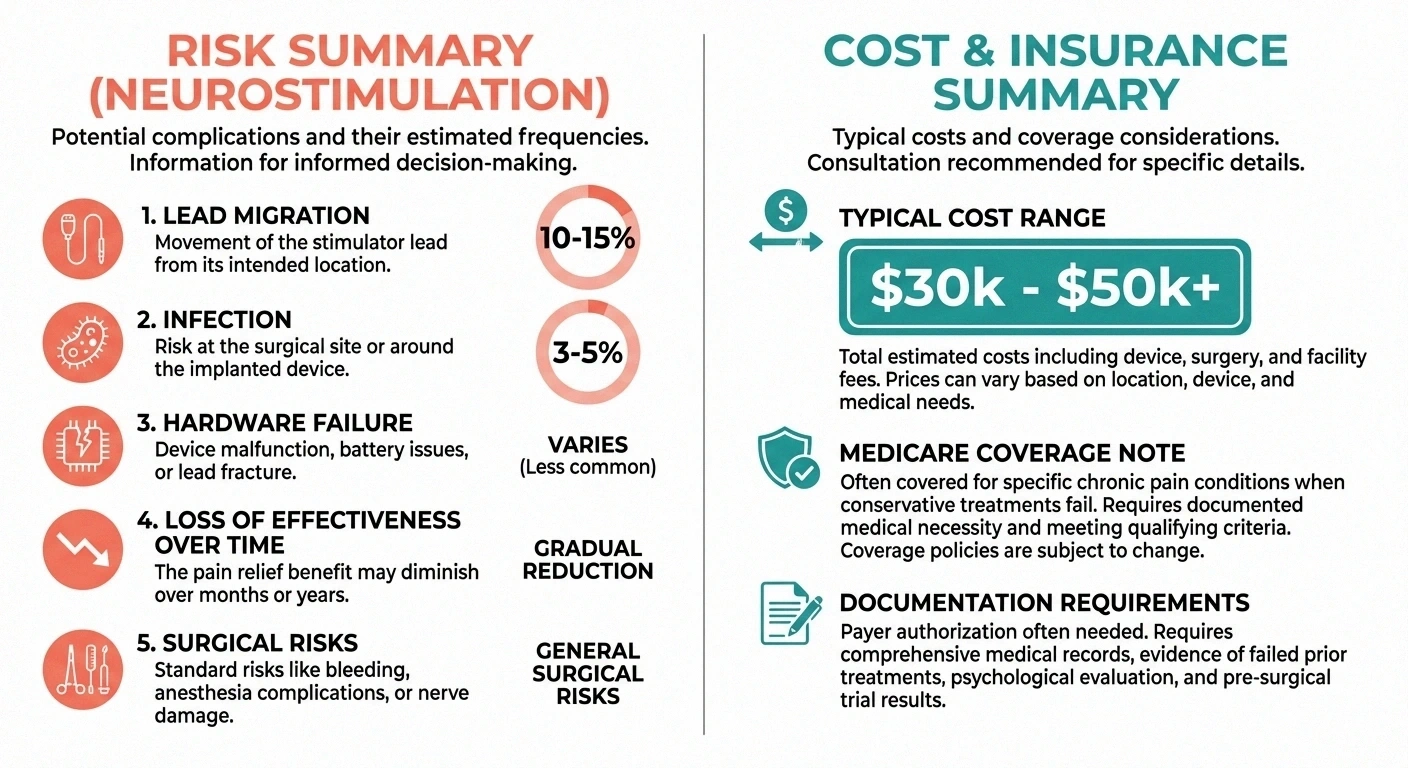
Lead migration is the most common complication. The thin electrode leads can shift from their optimal position, which changes the stimulation pattern and may reduce effectiveness. This occurs in roughly 10-15% of cases and typically requires a minor revision procedure to reposition the leads.
Infection at the implant site occurs in approximately 3-5% of cases. While most infections are superficial and treatable with antibiotics, severe infections may require device removal.
Hardware failure — leads can break, connectors can loosen, or batteries can fail earlier than expected. Modern rechargeable systems have reduced battery-related issues, but hardware problems still occur.
Loss of effectiveness over time is reported by some patients. While the long-term data shows 47% success at 7+ years, the flip side is that over half of initial responders eventually see diminished benefits. Reprogramming the device can sometimes restore effectiveness.
Surgical risks include bleeding, nerve damage from lead placement (rare), and reactions to anesthesia. Epidural hematoma and spinal cord injury are extremely rare but serious potential complications.
These risks are real but manageable, and they should be weighed against the impact that uncontrolled neuropathic pain has on your quality of life. Talk to your doctor about your specific risk factors.
Cost, Insurance, and Practical Considerations
Let's talk about the practical reality that many medical articles avoid:
Cost & Practical Reality
$30K–$50K+
Total cost (device + surgery)
7–10+ yrs
Rechargeable battery life
Most major insurance plans and Medicare cover SCS when medical necessity documentation requirements are met.
Cost: The total cost of SCS — including the trial, permanent implant surgery, device, and initial programming — typically ranges from $30,000 to $50,000 or more. The device itself is the most expensive component. This is one of the most expensive pain management interventions available.
Insurance coverage: Most major insurance plans, including Medicare, do cover SCS when medical necessity criteria are met. However, getting approval typically requires documentation of failed conservative treatments (usually 3-6 months of medication trials), a psychological evaluation, and a successful trial period. The approval process can take weeks to months. Understanding your insurance coverage before starting the process saves significant frustration.
Ongoing maintenance: After implantation, you'll need follow-up visits for programming adjustments, especially in the first year. Rechargeable batteries last 7-10+ years but eventually need surgical replacement. Non-rechargeable batteries last 3-5 years. Factor these ongoing costs and time commitments into your decision.
Lifestyle adjustments: With an SCS implant, you'll need to carry a patient identification card (for airport security and MRI facilities), avoid certain activities that could damage the leads, and charge your device regularly if you have a rechargeable system. Most patients adapt to these adjustments quickly, but they're worth knowing about in advance.
How SCS Compares to Other Advanced Treatments
SCS is one of several neuromodulation options available. Understanding where it fits helps frame your decision:
Peripheral nerve stimulation (PNS) places electrodes directly near specific peripheral nerves rather than in the spinal cord. PNS is less invasive than SCS and may be appropriate for patients with more localized pain patterns. Some newer PNS systems don't require a permanently implanted pulse generator.
TENS (Transcutaneous Electrical Nerve Stimulation) is a non-invasive, external device that uses the same gate control principle as SCS but without surgery. TENS is often tried first and can provide meaningful relief for milder pain, though it's generally less powerful than SCS for severe neuropathic pain.
Intrathecal drug delivery (pain pumps) delivers medication directly to the spinal fluid, bypassing the blood-brain barrier. This is typically reserved for patients who haven't responded to both medication and SCS.
Your pain management specialist can help you understand which approach — or combination — makes the most sense for your specific situation.
Questions to Ask Your Doctor About SCS
If you're considering spinal cord stimulation, bring these questions to your appointment:
Top Questions for Your Doctor
☐ How many SCS procedures have you performed for neuropathy?
☐ Which system do you recommend, and why this one?
☐ What's your personal complication rate?
☐ Will my insurance cover this, and what do we need?
☐ Can I still get MRIs? What kind and under what conditions?
☐ What should I realistically expect from the trial period?
☐ What lifestyle restrictions come with a permanent implant?
Print this list and bring it to your appointment. A confident doctor will welcome these questions.
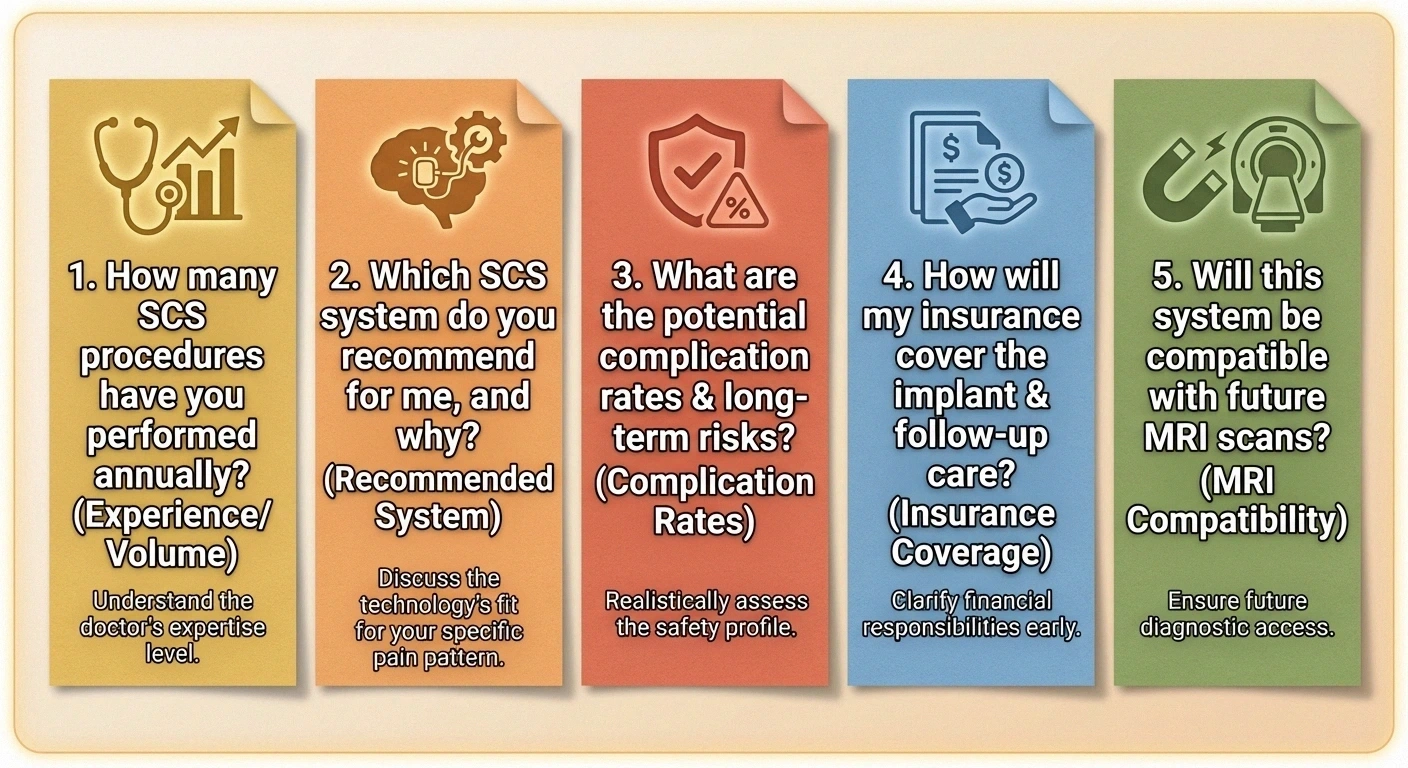
1. Based on my specific type of neuropathy, what success rate do you typically see with SCS?
2. How many SCS procedures have you personally performed for neuropathy patients?
3. Which SCS system do you recommend for my situation, and why?
4. What stimulation types (tonic, high-frequency, burst) does the recommended system support?
5. What's your complication rate, and how do you handle lead migration or infection?
6. Will my insurance cover this, and what documentation do we need?
7. What should I expect during the trial period — pain level, restrictions, daily routine?
8. If the trial is successful, how long until permanent implant?
9. What lifestyle restrictions will I have with a permanent implant?
10. Can I still have MRIs? What kind, and under what conditions?
A doctor who is confident in their recommendation will welcome these questions. If anyone seems uncomfortable with your due diligence, that itself is information worth having.
Making the Decision
Spinal cord stimulation is a significant decision, and there's no universal right answer. What I can tell you from connecting with patients over the years is this:

The patients who are most satisfied with SCS are those who went in with realistic expectations — understanding that the goal is meaningful pain reduction, not elimination — and who had truly exhausted other options first. They evaluated the trial honestly, worked with experienced specialists, and viewed SCS as one piece of a comprehensive pain management strategy rather than a standalone cure.
The patients who are least satisfied tend to be those who expected SCS to eliminate their pain entirely, or who were rushed into the decision by providers without adequate discussion of limitations and alternatives.
Take the time to research, ask questions, seek second opinions, and make this decision from a place of informed confidence rather than desperation. Your pain deserves serious intervention — and you deserve honest information to guide that choice.
Frequently Asked Questions
Does spinal cord stimulation actually work for neuropathy?
Clinical research shows that SCS can provide significant pain relief for neuropathy patients, particularly those with diabetic peripheral neuropathy. A randomized controlled trial found that SCS patients were nearly 19 times more likely to achieve treatment success compared to medication alone. However, results vary between individuals, and the mandatory trial period helps determine whether SCS will work for your specific pain before committing to a permanent implant.
What does the spinal cord stimulation trial involve?
The trial lasts approximately 5 to 10 days. Temporary electrode leads are placed through a needle near your spinal cord under local anesthesia and sedation. The leads connect to an external pulse generator you wear on a belt. You go home and evaluate pain relief during normal daily activities. A successful trial typically means 50 percent or greater pain reduction. If the trial is unsuccessful, the temporary leads are simply removed.
How much does spinal cord stimulation cost?
The total cost including trial, permanent implant surgery, device, and initial programming typically ranges from $30,000 to $50,000 or more. Most major insurance plans and Medicare cover SCS when medical necessity criteria are documented, including evidence of failed conservative treatments. Ongoing costs include follow-up programming visits and eventual battery replacement surgery every 7 to 10 years for rechargeable systems.
What are the risks of spinal cord stimulation?
The most common complication is lead migration, occurring in roughly 10 to 15 percent of cases and usually requiring a minor revision. Infection at the implant site occurs in approximately 3 to 5 percent of cases. Hardware failure, loss of effectiveness over time, and standard surgical risks like bleeding are also possible. Serious complications like spinal cord injury are extremely rare. These risks should be weighed against the quality of life impact of uncontrolled neuropathic pain.
Can I get MRIs with a spinal cord stimulator implant?
Many newer SCS systems are labeled as MRI-conditional, meaning MRIs are possible under specific conditions such as limited body regions, specific MRI machine settings, and particular patient positions. However, there are still significant restrictions compared to patients without implants. Discuss MRI compatibility with your doctor before choosing a system, especially if you have conditions that may require regular MRI monitoring.
How long does a spinal cord stimulator last?
Modern rechargeable SCS systems have batteries that last approximately 7 to 10 or more years before needing surgical replacement. Non-rechargeable systems typically last 3 to 5 years. The leads and other hardware can last much longer if they remain properly positioned. Long-term studies show that approximately 47 percent of patients maintain successful pain relief at 7 or more years, though effectiveness may decrease over time for some individuals.
Is spinal cord stimulation covered by Medicare?
Yes, Medicare generally covers spinal cord stimulation when medical necessity criteria are met. This typically requires documentation of chronic neuropathic pain, evidence that conservative treatments like medications and physical therapy have been tried for 3 to 6 months without adequate relief, a psychological evaluation, and a successful trial period. Work with your doctor's office and insurance coordinator to ensure all documentation requirements are met before scheduling the procedure.


