
The first time my neighbor Marlene mentioned the tingling in her hands, she blamed it on her rheumatoid arthritis. “It's just the RA,” she said. “Everything is the RA.” I nodded, because for ten years, just about everything had been the RA. The swollen knuckles, the stiff mornings, the bone-deep fatigue. Why would tingling be any different?
It turned out to be different. After her rheumatologist sent her for nerve testing, the diagnosis came back as carpal tunnel syndrome on top of her RA, made worse by the chronic swelling around her wrists. A small change to her splints and a steroid injection later, and the tingling was mostly gone. But the question stuck with me: how often is nerve damage hiding inside an RA diagnosis, getting written off as “just the arthritis”?
The answer, it turns out, is more often than most people realize. Rheumatoid arthritis can damage your peripheral nerves in several distinct ways, and recognizing which one you have changes everything about how it gets treated. This is the patient's-eye view of how RA and neuropathy connect, the warning signs to watch for, and what the treatment options look like in 2026.
How Common Is Neuropathy in Rheumatoid Arthritis?
Studies put the rate of peripheral neuropathy in RA patients anywhere from less than 1% to as high as 85%, depending on what you count and how hard you look. The wide range comes from different definitions — some studies only count clinically obvious cases (the patient is symptomatic and their doctor noticed); others use sensitive nerve conduction studies that pick up subtle changes in people who don't feel anything yet.
Key Takeaway
RA causes nerve damage in three main ways: compression (carpal tunnel from joint swelling), inflammatory polyneuropathy (cytokines damaging nerves over years), and vasculitic neuropathy (immune attack on nerve blood supply — rare but emergency). Tingling and numbness aren't “just the RA” — they deserve their own evaluation, and modern biologic treatment can prevent or improve most forms.
The most realistic working numbers, from clinical practice:
- Roughly 30 to 40 percent of RA patients show some objective nerve abnormality on testing, even if mild
- About 18 percent develop carpal tunnel syndrome (median nerve compression at the wrist) — often one of the first signs
- Around 10 to 15 percent develop symptomatic distal sensory polyneuropathy (the burning, tingling, numbness in feet and hands you might think of as “classic” neuropathy)
- About 1 percent develop the most serious form, vasculitic mononeuritis multiplex — rare but a true emergency
What this means in practical terms: if you have RA, you're not unusual for noticing nerve symptoms. If you've had RA for more than ten years, especially if your disease has been hard to control, the odds go up further. It's not “just the arthritis.” It deserves its own evaluation.
The Three Main Ways RA Damages Nerves
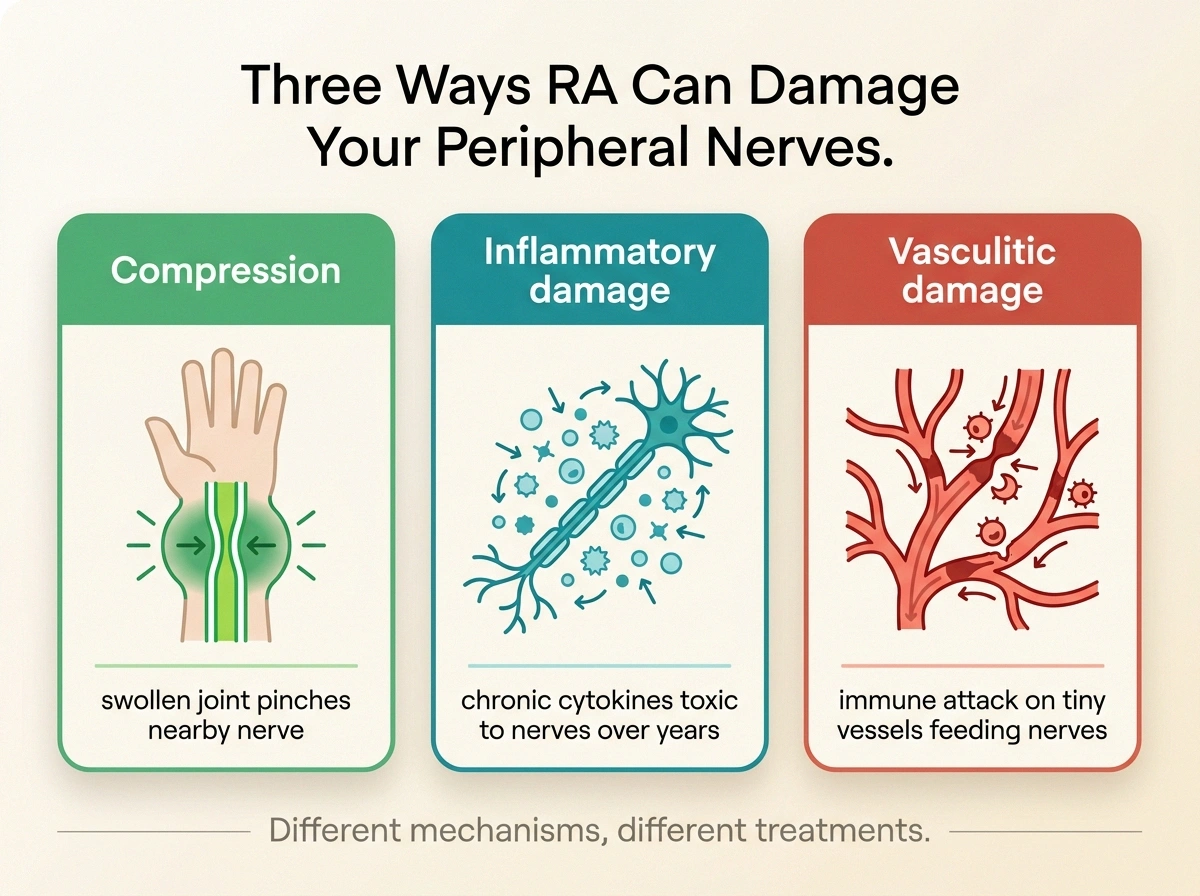
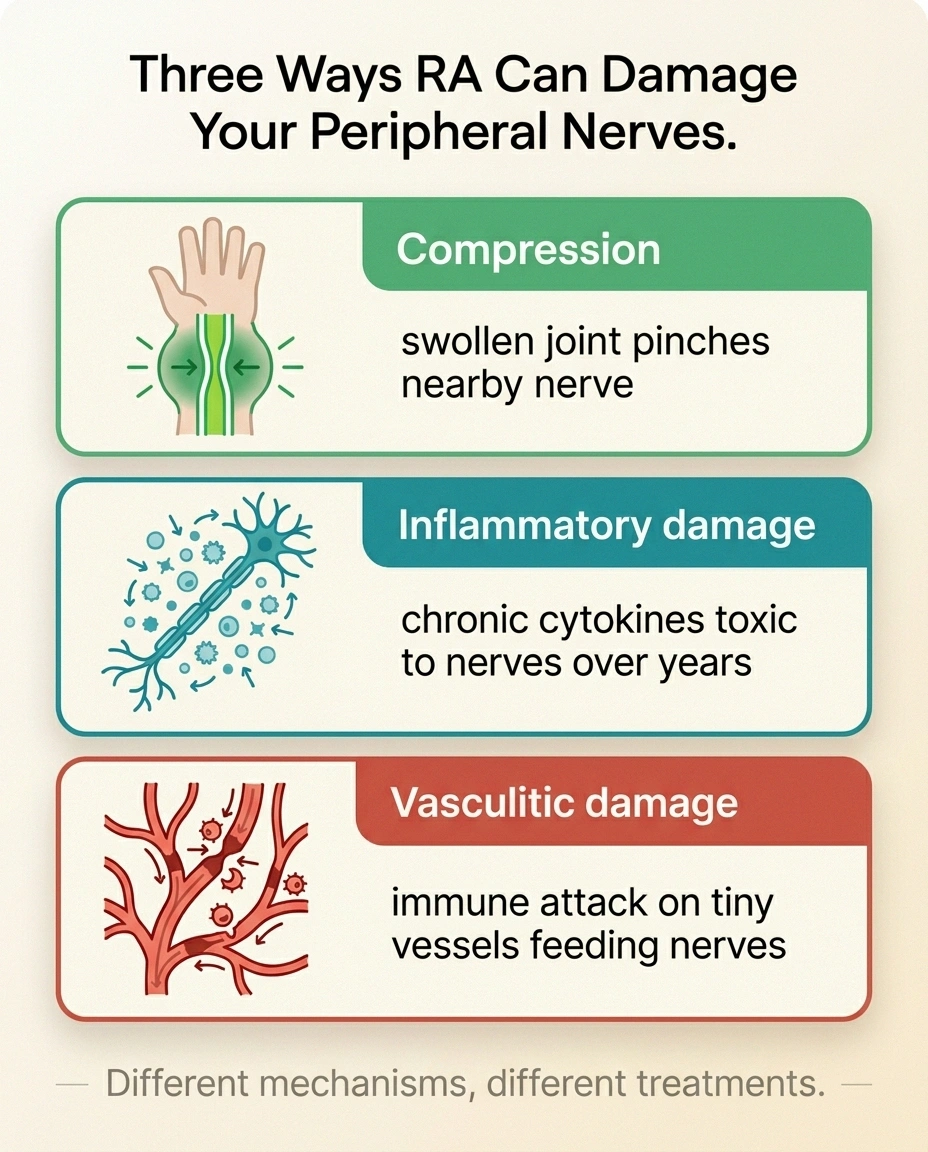
Understanding which mechanism is at work matters because the treatment paths look very different. RA causes neuropathy through three main routes.
RA Neuropathy — By the Numbers
Of RA patients show some nerve abnormality on objective testing
Develop carpal tunnel syndrome from compression
Develop symptomatic distal sensory polyneuropathy
Develop vasculitic mononeuritis multiplex (rare emergency)
1. Compression — Swollen Joints Pressing on Nearby Nerves
This is the most common and the most fixable. The same chronic synovial swelling that damages joints can squeeze nerves passing nearby. The classic examples:
- Carpal tunnel syndrome — the median nerve at the wrist, swollen from RA inflammation in the surrounding tissues. Symptoms: night-time tingling, burning, or numbness in the thumb, index finger, and middle finger. Often wakes people up; shaking the hand helps briefly. Affects about 18% of RA patients.
- Cubital tunnel syndrome — the ulnar nerve at the elbow. Symptoms: tingling along the ring finger and pinky, weakness gripping objects, sometimes a “funny bone” sensation that lingers.
- Tarsal tunnel syndrome — the posterior tibial nerve at the inner ankle. Symptoms: burning or tingling in the sole and toes, often worse with walking or standing.
The good news with compression neuropathy: it usually responds to splints, anti-inflammatory treatment, steroid injections into the joint or tunnel, and in some cases, a relatively small surgical release procedure. Hand neuropathy from compression often improves dramatically with the right intervention.
2. Inflammatory Polyneuropathy — The Cytokines Themselves Damage Nerves
Chronic inflammation isn't kind to nerves. The same pro-inflammatory chemicals that drive joint damage in RA — particularly TNF-alpha and interleukin-6 — are directly toxic to peripheral nerves over years of exposure. This produces a slow, symmetric, “stocking-glove” distal sensory polyneuropathy that looks a lot like diabetic neuropathy.
Symptoms develop gradually:
- Burning, tingling, or numbness in both feet, then later both hands
- Symmetric (both sides at once, not just one foot)
- Sensation of walking on cotton or pebbles
- Sometimes allodynia — light touch becoming painful
- May affect small nerve fibers first, before showing up on standard nerve tests
This type tends to track with how active your RA has been and for how long. Patients with long-standing seropositive RA (positive rheumatoid factor and anti-CCP antibodies) and high disease activity scores are at the highest risk.
3. Vasculitic Neuropathy — The Most Serious Form
This is the one that scares rheumatologists and the one I want you to know about by name even though it's rare. In rheumatoid vasculitis, the immune system attacks the small blood vessels that feed peripheral nerves (called the vasa nervorum). When those tiny vessels get blocked by immune complexes, the nerves they supply suffer ischemic damage — essentially small strokes inside the nerve.
The presentation is dramatic compared to the slow polyneuropathy:
- Sudden onset — over days to a week or two
- Asymmetric — one foot, one hand, one side dramatically worse than the other
- Painful — often severe, burning, deep
- Often motor — sudden weakness, foot drop, wrist drop
- This pattern is called mononeuritis multiplex — multiple individual nerves affected randomly, not the symmetric stocking-glove pattern
Vasculitic neuropathy is the medical emergency of the RA-and-nerve world. Untreated, the nerve damage becomes permanent. Treated quickly with high-dose steroids and immunosuppressants like cyclophosphamide or rituximab, much of the function can be preserved.
Risk factors for rheumatoid vasculitis: long-standing severe seropositive RA (often 10+ years), presence of subcutaneous rheumatoid nodules, smoking history, high disease activity scores. The good news is that aggressive modern RA treatment with biologics has made rheumatoid vasculitis significantly rarer than it was a generation ago.
The Other Types Worth Knowing About

A few less common patterns:
RA Compression Neuropathies — Where to Watch
- Carpal tunnel (median nerve at wrist) — night-time tingling in thumb, index, middle finger; shaking helps
- Cubital tunnel (ulnar nerve at elbow) — tingling along ring finger and pinky; weakness gripping
- Tarsal tunnel (posterior tibial nerve at ankle) — burning in sole and toes, worse with walking
All three respond to splints, steroid injections, and aggressive RA control — often with surgical release as a backup.
Drug-induced neuropathy. Some RA medications can cause neuropathy as a side effect. Methotrexate rarely; leflunomide occasionally; the older gold therapy and penicillamine more notably (though these are seldom used now). TNF inhibitors like infliximab and adalimumab have been associated with rare cases of demyelinating neuropathy. If new neuropathy starts within months of a new RA medication, the timing is worth flagging to your doctor.
Cervical myelopathy that mimics neuropathy. Long-standing severe RA can cause instability in the upper cervical spine (atlanto-axial subluxation), which can compress the spinal cord. Symptoms — hand weakness, balance problems, bladder issues — can look like neuropathy but require completely different evaluation and treatment. Any RA patient with new weakness or balance trouble should have their neck imaged.
Autonomic neuropathy. RA can affect the autonomic nervous system that controls heart rate, blood pressure, sweating, and digestion. Symptoms include lightheadedness on standing, dry mouth and dry eyes (especially if secondary Sjögren's syndrome coexists), and constipation or diarrhea. Less common but worth knowing about.
How RA Neuropathy Is Diagnosed

If you're noticing nerve symptoms, your rheumatologist will typically do (or refer you for):
RA Neuropathy Diagnostic Workup
- EMG and nerve conduction studies. The gold standard for confirming neuropathy and identifying the pattern (symmetric vs asymmetric, sensory vs motor, axonal vs demyelinating).
- Skin punch biopsy if small fiber neuropathy is suspected (small fibers don't show up on standard EMG).
- Bloodwork looking at inflammation markers (ESR, CRP), RA serology (RF, anti-CCP), antibodies suggesting overlap autoimmunity (ANA, complement), cryoglobulins, and the basics that contribute to any neuropathy (HbA1c, B12, TSH, kidney and liver function).
- Nerve biopsy if vasculitis is suspected — usually a sural nerve biopsy. This is invasive and reserved for cases where the diagnosis would change treatment dramatically.
- Cervical spine MRI if myelopathy is on the differential.
This workup matters because the treatment differs sharply by mechanism. A compression neuropathy doesn't need cyclophosphamide; vasculitis can't be fixed with a wrist splint.
Treatment: Disease Control First

The single most important intervention for RA neuropathy is good control of the underlying RA. When the joint inflammation is suppressed, the systemic inflammation that's punishing your nerves drops too.
What the Evidence Says
Aggressive modern RA control reduces neuropathy. Biologics (TNF inhibitors, IL-6 blockers, JAK inhibitors, B-cell depleters) have made rheumatoid vasculitis significantly rarer than a generation ago.
A 2026 Frontiers in Immunology case report documented refractory peripheral neuropathy improving on the IL-6 blocker tocilizumab — a result that wouldn't have been possible 20 years ago.
This is one of the quiet wins of the modern biologic era. Aggressive treatment with DMARDs (methotrexate, hydroxychloroquine, sulfasalazine) and biologics (TNF inhibitors, IL-6 inhibitors, JAK inhibitors, B-cell depleters) has not only made RA much more manageable joint-wise — it's reduced the rate of severe complications including vasculitic neuropathy.
Specific treatment approaches by mechanism:
For compression neuropathies: Splints (especially nighttime wrist splints for carpal tunnel), corticosteroid injections into the affected joint or tunnel, addressing the underlying joint synovitis aggressively, and surgical release if conservative measures fail. Carpal tunnel release is one of the most successful surgeries in medicine.
For inflammatory polyneuropathy: Better RA control over time often improves symptoms slowly. Symptom control with the same medications used for any neuropathy — gabapentin, pregabalin, duloxetine, topical lidocaine, and lifestyle measures (sleep, blood sugar, B-vitamin status, gentle movement).
For vasculitic neuropathy: This is rheumatology emergency-territory. Treatment usually involves high-dose corticosteroids initially, followed by an immunosuppressant — historically cyclophosphamide, increasingly rituximab in modern practice. The goal is to halt the immune attack on the vasa nervorum before more nerves are infarcted. IVIG is occasionally used in selected cases. Recovery depends on how quickly treatment starts and how much nerve damage occurred before then.
Red Flags: When to Call Your Rheumatologist Today
Most RA neuropathy is slow and chronic. But some patterns mean call now, not at your next scheduled appointment:
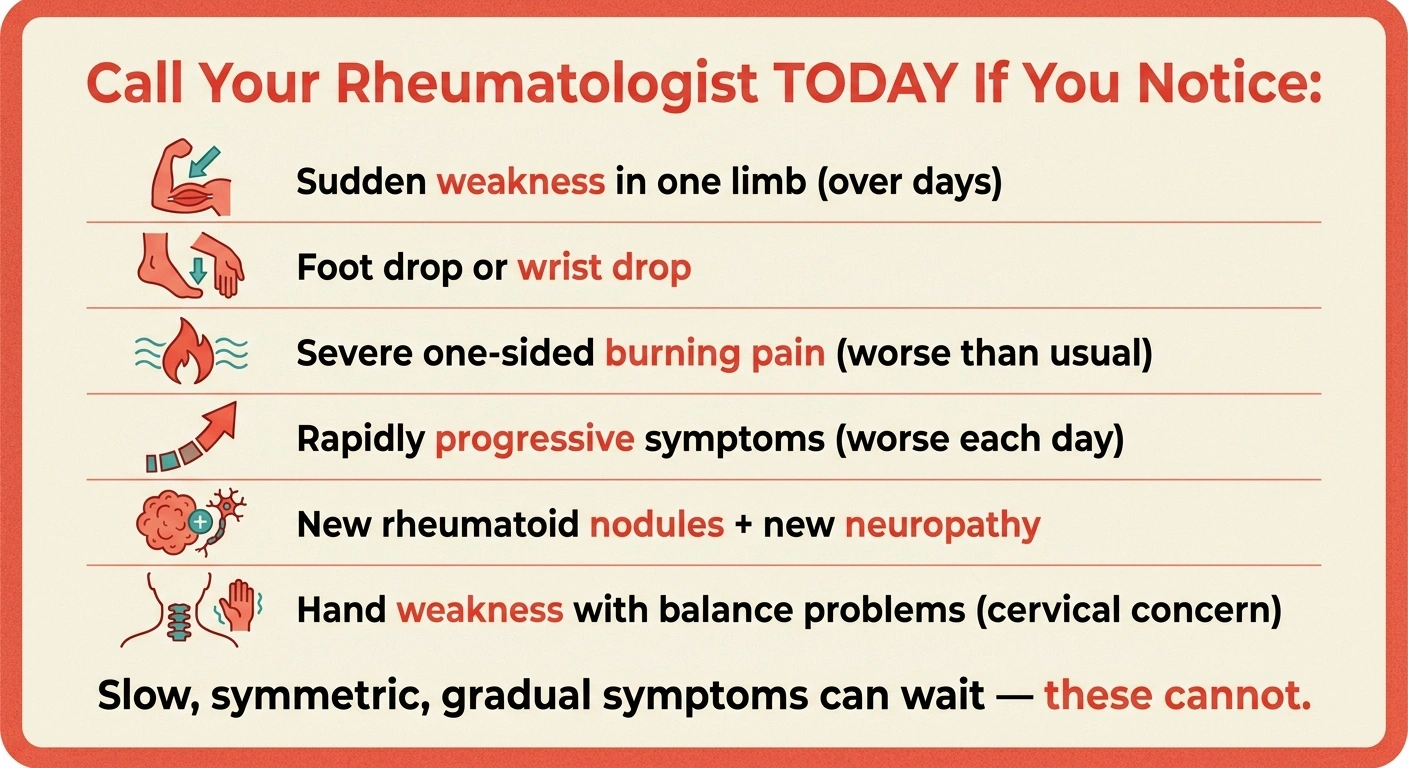
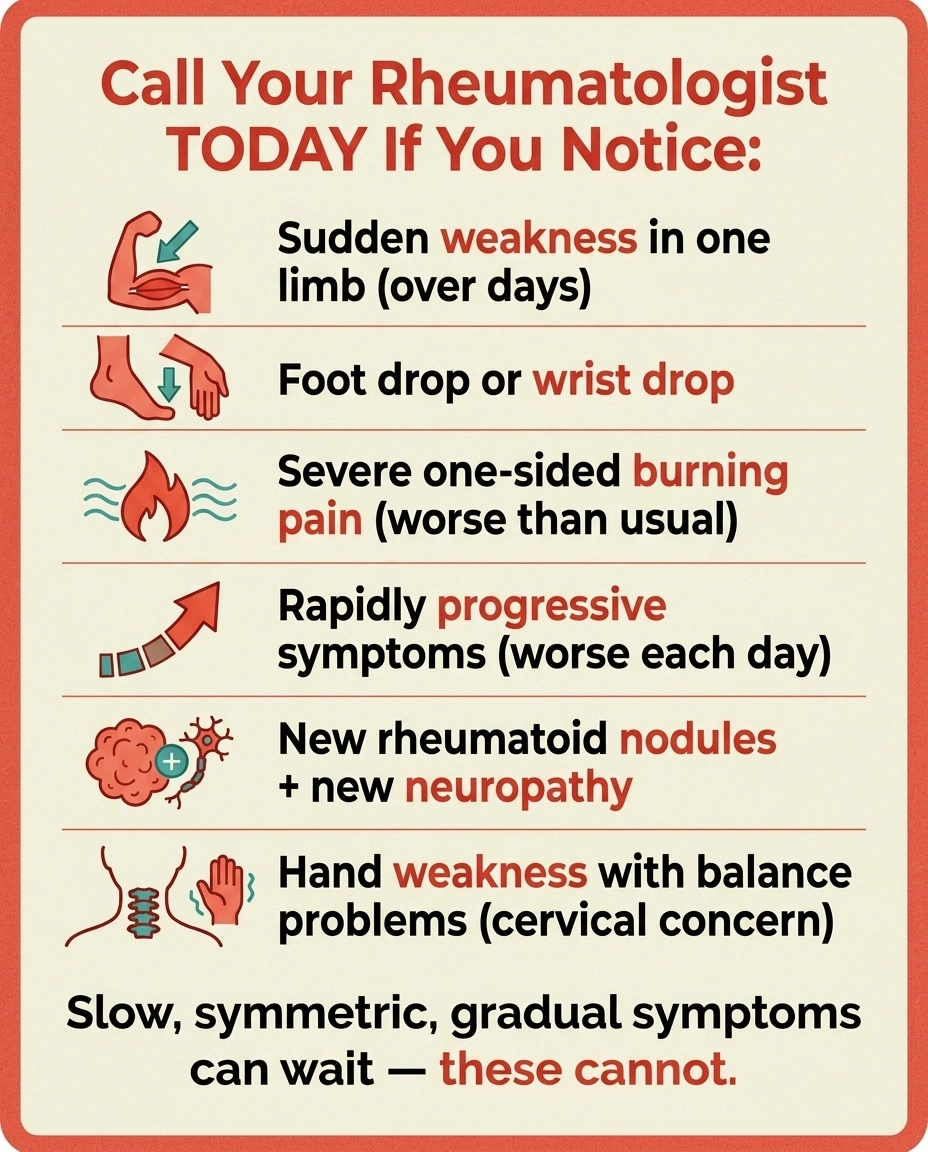
Call Your Rheumatologist TODAY If You Notice:
- Sudden weakness in one limb developing over days
- Foot drop or wrist drop — can't lift the foot or extend the wrist normally
- Severe asymmetric burning pain worse than anything you've had before
- Rapidly progressive symptoms — noticeably worse each day or week
- New rheumatoid nodules + new neuropathy in active disease
- Hand weakness with balance problems (possible cervical myelopathy)
Slow, gradual, symmetric symptoms can wait for your scheduled appointment. These cannot.
- Sudden weakness in one limb developing over days, especially if asymmetric (one foot drops, one hand weakens)
- Foot drop or wrist drop — inability to lift your foot or extend your wrist normally
- Severe asymmetric burning pain in one limb that's much worse than anything you've had before
- Rapidly progressive symptoms — getting noticeably worse each day or week
- New neuropathy symptoms alongside an active RA flare with new rheumatoid nodules
- Hand weakness, balance problems, or bladder changes in someone with long-standing RA — possible cervical myelopathy
Call. Don't wait. These patterns can represent vasculitis or cervical cord compression, both of which do better the sooner treatment starts.
Living With Both
If you're managing both RA and neuropathy, you're carrying a heavier load than people give credit for. The fatigue, joint pain, stiffness, and burning nerve pain stack on each other. Days can feel impossibly long. The mental weight of two chronic conditions is real.
Some practical things that help:
- One unified care team. Your rheumatologist and your primary care should be talking. If you have a neurologist for the neuropathy too, make sure each has the others' notes and current medication lists. Bring printouts to appointments.
- Foot care matters more than ever. RA can change the shape of your feet (bunions, hammer toes, fallen arches), and neuropathy reduces the protective sensation that warns you when something fits wrong. Properly fitted shoes and a once-a-month foot inspection (yourself or a podiatrist) prevent the small wounds that can become big problems.
- Energy is finite. Pacing yourself across the day, building in rest periods, and saying yes to help are not weakness. They're strategy.
- Watch your mental health. Two chronic painful conditions plus the medications used to treat them puts you at significantly higher risk for depression and anxiety. Address it directly with your doctor.
- Connect with others. RA support communities and neuropathy support communities both exist and overlap more than you might think.
The Hopeful Part

Modern RA treatment is dramatically better than it was twenty years ago. Biologics and targeted therapies have changed not only joint outcomes but the rate of serious complications including neuropathy. New molecules continue to enter the pipeline. Recent case reports have even shown refractory peripheral neuropathy in long-standing RA improving with IL-6 blockers like tocilizumab — a result that wouldn't have been possible a generation ago.
Marlene, the friend I started with, is doing well. Her carpal tunnel cleared up with splints and a steroid injection. Her RA is in remission on her current biologic. The tingling she dismissed as “just the RA” turned out to be an entirely separate, fixable problem. Most RA neuropathy stories are like that — they have moves on the board, options that work, and a path back to function. The first move is naming the problem clearly enough to treat it.
Frequently Asked Questions
Can rheumatoid arthritis cause neuropathy?
Yes. RA causes peripheral neuropathy through three main mechanisms: compression of nerves by swollen joints (most commonly carpal tunnel at the wrist), inflammatory damage to nerves from chronic exposure to inflammatory cytokines like TNF-alpha and IL-6, and rare but serious vasculitic damage where the immune system attacks the small blood vessels feeding nerves. Studies estimate that 30 to 40 percent of RA patients show some objective nerve abnormality on testing, with about 18 percent developing carpal tunnel syndrome and 10 to 15 percent developing symptomatic polyneuropathy.
What does RA neuropathy feel like?
It depends on the type. Compression neuropathy at the wrist (carpal tunnel) typically causes tingling, burning, or numbness in the thumb, index, and middle fingers, often worse at night and improved by shaking the hand. Distal symmetric polyneuropathy from chronic inflammation feels like burning, tingling, or numbness in both feet (and later both hands), symmetric and slowly progressive. Vasculitic neuropathy is dramatically different: sudden, asymmetric, painful, often with weakness in one limb developing over days. The differences matter because treatment approaches are quite different.
What is rheumatoid vasculitis and how does it affect nerves?
Rheumatoid vasculitis is a rare but serious complication where the immune system attacks small blood vessels throughout the body, including the tiny vessels that supply blood to peripheral nerves (vasa nervorum). When those vessels are blocked by immune complexes, the nerves they supply suffer ischemic damage — essentially small strokes inside the nerves. This causes mononeuritis multiplex: sudden, asymmetric, painful weakness in one or more limbs, often with foot drop or wrist drop. It's a medical emergency that requires high-dose immunosuppression, usually including corticosteroids and either cyclophosphamide or rituximab. Modern biologic treatment has made it much rarer than it was a generation ago.
Can RA medications cause neuropathy?
Some RA medications can rarely cause neuropathy. Methotrexate rarely causes peripheral neuropathy; leflunomide occasionally causes it; the older medications gold and penicillamine were more notable causes (though seldom used now). TNF inhibitors like infliximab and adalimumab have been associated with rare cases of demyelinating neuropathy, which is part of why your rheumatologist screens for any neurologic history before starting them. If new neuropathy symptoms appear within weeks to months of starting a new RA medication, the timing is worth raising with your doctor — sometimes the medication needs to be changed.
Will treating my RA help the neuropathy?
Often yes, especially for inflammatory polyneuropathy and for compression neuropathy from joint swelling. When systemic inflammation drops, the cytokines damaging your nerves drop too, and over time symptoms can improve or stabilize. There are even case reports of refractory peripheral neuropathy improving on IL-6 blockers like tocilizumab. For compression neuropathies, controlling the synovial swelling can reduce pressure on the nerve. Vasculitic neuropathy specifically requires aggressive immunosuppression aimed at the vasculitis itself, not just standard RA control.
What's the difference between RA neuropathy and diabetic neuropathy?
The clinical picture can look similar — burning, tingling, numbness in feet then hands — but the underlying mechanisms are different. Diabetic neuropathy is driven by chronic high blood sugar damaging nerves over years, often with vascular contributions. RA-related polyneuropathy is driven by chronic inflammation and pro-inflammatory cytokines. Many people unfortunately have both at once (RA increases insulin resistance and diabetes risk). Treatment overlaps significantly for symptom control but differs in the upstream cause: tight blood sugar control matters most for diabetes, while controlling RA disease activity matters most for RA-driven nerve damage.
When should I worry about my RA-related nerve symptoms?
Call your rheumatologist promptly if you develop any of these red flags: sudden weakness in one limb over days, asymmetric foot drop or wrist drop, severe one-sided burning pain that's worse than anything you've had before, rapidly progressive symptoms, or new neuropathy alongside an active RA flare with new rheumatoid nodules. Slowly progressive bilateral tingling and numbness can usually wait for a regular appointment, but anything sudden, asymmetric, or accompanied by weakness needs urgent evaluation. Long-standing RA patients with new hand weakness or balance trouble should also have their cervical spine imaged to rule out atlanto-axial subluxation.
Can carpal tunnel syndrome be caused by rheumatoid arthritis?
Yes, very commonly. About 18 percent of RA patients develop carpal tunnel syndrome — the synovial inflammation around the wrist tendons can compress the median nerve as it passes through the carpal tunnel. RA-related carpal tunnel often responds well to night-time wrist splints, corticosteroid injections, and aggressive control of the underlying RA. Surgical release is highly effective when conservative treatment isn't enough. It's actually one of the most fixable forms of RA-related neuropathy, which is why noticing the early signs (night-time tingling in the first three fingers) and naming them out loud to your rheumatologist matters.


