When I first heard about IVIG therapy for neuropathy, I'll be honest — the name alone felt overwhelming. Intravenous immunoglobulin. Three hours sitting in an infusion chair. A treatment pulled from pooled human blood donations. It sounded more like something from a medical drama than a real option for people like us navigating nerve damage.
But over the years, I've spoken with dozens of people in our community who have gone through IVIG treatment — some of whom describe it as genuinely life-changing. Others found it wasn't the right fit. The difference, almost always, came down to why their neuropathy started in the first place.
That's the most important thing to understand about IVIG: it's not a blanket treatment for all neuropathy. It's a targeted therapy for neuropathies driven by immune system malfunction. If that describes your situation, IVIG may be one of the most powerful tools available to you. If it doesn't, it may do very little at all.
Let me walk you through what IVIG actually is, who it helps, what the process involves, and the questions you'll want answered before your next neurology appointment.
What Is IVIG, and Why Would It Help Neuropathy?
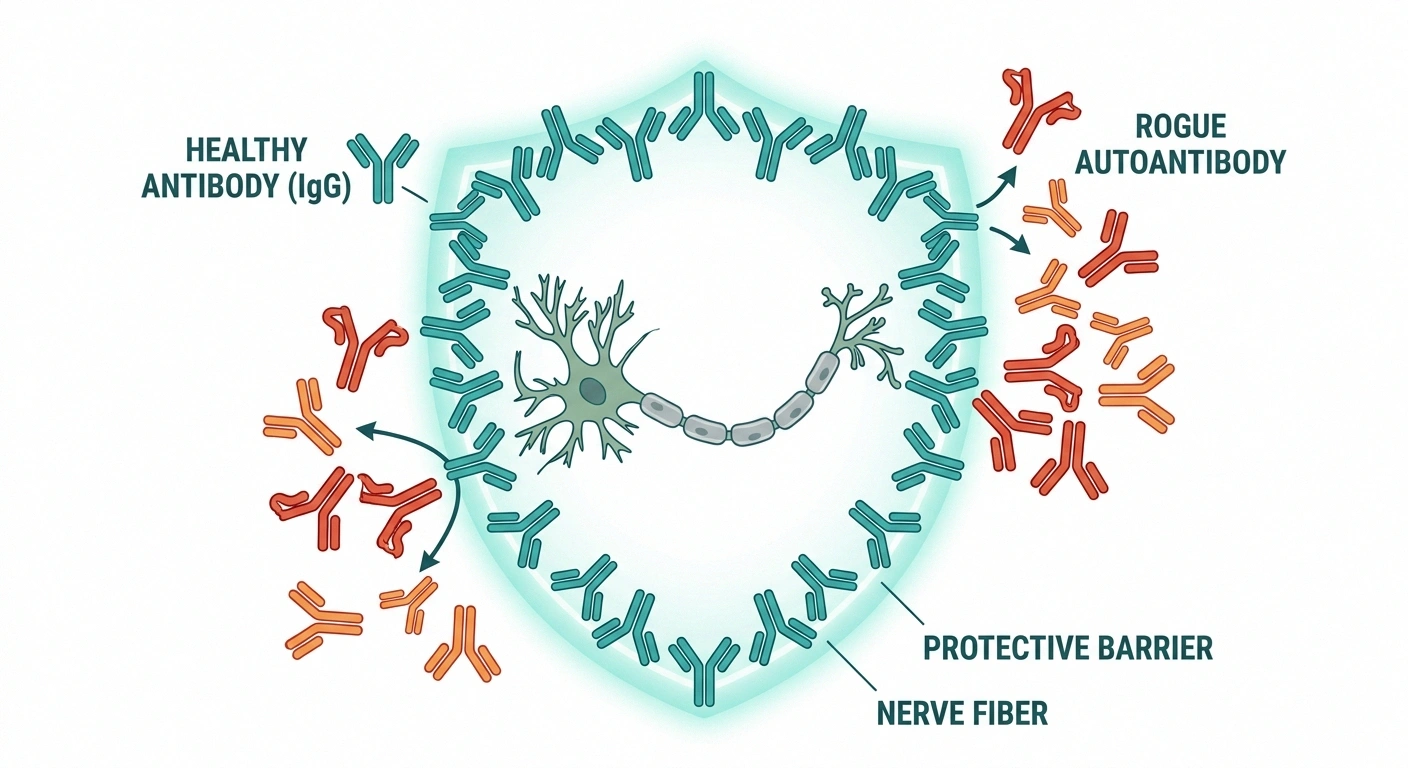
IVIG stands for intravenous immunoglobulin. The “immunoglobulin” part refers to antibodies — specifically, the IgG class of antibodies that your immune system normally uses to fight infections and coordinate immune responses.
Key Takeaway
IVIG works by supplying healthy antibodies that interrupt the immune system's attack on your nerves. It's highly effective for immune-mediated neuropathies like CIDP, Guillain-Barré, and MMN — but not for neuropathies caused by diabetes, toxins, or nutritional deficiencies.
IVIG is made by collecting blood plasma from thousands of healthy donors and extracting the IgG antibodies from that pool. The result is a concentrated preparation containing an enormous diversity of antibodies — antibodies that collectively represent the immune experience of thousands of people.
When someone with an autoimmune neuropathy receives IVIG, those healthy donated antibodies do something remarkable: they essentially interrupt the misdirected immune attack on the nerves. They do this through several mechanisms — competing for receptors that normally amplify immune activity, binding to the antibodies that are attacking nerve tissue, and modulating inflammatory signals throughout the nervous system.
In practical terms: when your immune system is damaging your nerves, flooding it with a massive dose of healthy antibodies can put the brakes on that process. The result, in many patients, is reduced inflammation, slowing of nerve damage, and — when treatment begins early enough — actual recovery of nerve function over time.
This is fundamentally different from how most neuropathy medications work. Drugs like gabapentin or pregabalin manage the symptoms of nerve pain. IVIG addresses the underlying immune process that's causing the damage.
The Neuropathies IVIG Is Proven to Treat
IVIG has strong evidence behind it for a specific group of immune-mediated neuropathies. These are the conditions where neurologists regularly recommend it.
Who IVIG Helps vs. Who It Doesn't
| IVIG Is Indicated | IVIG Is NOT Indicated |
|---|---|
| CIDP (chronic inflammatory demyelinating polyneuropathy) | Diabetic peripheral neuropathy |
| Guillain-Barré syndrome (GBS) | Idiopathic small fiber neuropathy (I-SFN) |
| Multifocal motor neuropathy (MMN) | Toxic or alcohol-related neuropathy |
| Some vasculitic and autoimmune neuropathies | Hereditary neuropathies (e.g., CMT) |
Chronic Inflammatory Demyelinating Polyneuropathy (CIDP)
CIDP is arguably where IVIG has its strongest evidence base. In CIDP, the immune system attacks the myelin sheath — the protective coating around nerve fibers — leading to progressive weakness and sensory loss that often affects both legs and arms.
IVIG is an FDA-approved treatment for CIDP and is considered one of three first-line options (alongside corticosteroids and plasma exchange). Many CIDP patients receive IVIG infusions every three to four weeks on an ongoing basis to keep the condition from progressing. Clinical trials have consistently shown it slows disease progression and can improve strength and function.
Guillain-Barré Syndrome (GBS)
Guillain-Barré syndrome is an acute autoimmune neuropathy, often triggered by an infection, where the immune system attacks peripheral nerves in a rapid ascending pattern. GBS can be terrifying — weakness may progress to paralysis within days. IVIG is one of two treatments proven to shorten recovery time (the other being plasma exchange). A five-day course of IVIG is typically given as soon as GBS is diagnosed, and it can significantly reduce the severity and duration of the illness.
Multifocal Motor Neuropathy (MMN)
MMN is a rarer autoimmune neuropathy affecting mainly motor nerves, causing progressive weakness that often starts in the hands and arms. IVIG is the treatment of choice for MMN — corticosteroids, interestingly, can actually worsen MMN, making IVIG particularly important for this diagnosis. Regular maintenance infusions are usually required.
Other Autoimmune Neuropathies
IVIG may also be considered for other immune-mediated neuropathies, including vasculitic neuropathy, some cases of small fiber neuropathy with confirmed autoimmune markers, paraproteinemic neuropathies, and certain nerve complications from conditions like Sjögren's syndrome or lupus. In these cases, the decision is more individualized and depends heavily on the specific immunological findings from your workup.
When IVIG Is Not the Answer
This is where I want to be very direct with you, because I've seen people pursue IVIG with high hopes only to feel let down when it didn't help — not because IVIG failed, but because it was never the right treatment for their type of neuropathy.
Important
IVIG for neuropathy should only be initiated by a neurologist after a thorough diagnostic workup. Using it for neuropathies without an immune component is unlikely to help and exposes you to unnecessary cost and risk. Getting the correct underlying diagnosis is the essential first step.
IVIG does not work for neuropathies that are not immune-mediated. This includes:
- Diabetic peripheral neuropathy — caused by metabolic damage from blood sugar, not immune attack
- Idiopathic small fiber neuropathy (I-SFN) — studies have specifically shown IVIG has no significant effect on pain in this group
- Toxic neuropathy — caused by medications, alcohol, or chemical exposure
- Nutritional deficiency neuropathy — caused by vitamin B12, B1, or other deficiencies
- Hereditary neuropathies — genetic conditions affecting nerve structure
If your neuropathy falls into one of these categories, your neurologist should be directing you toward other evidence-based approaches. Getting a thorough neuropathy diagnosis that identifies the underlying cause is absolutely essential before IVIG is even considered.
The IVIG Infusion Process: What to Expect
If you've been told IVIG is appropriate for your neuropathy, here's what the process actually looks like.

What Happens on Infusion Day
Before Your First Infusion
Your neurologist will order blood work before starting IVIG. This typically includes kidney and liver function tests (because IVIG is processed by these organs), IgA levels (some people have IgA deficiency that can cause severe reactions to IVIG), a complete blood count, and any specific immune markers relevant to your diagnosis.
You'll also need prior authorization from your insurance company. Because IVIG is expensive — a single infusion cycle can run $5,000 to $25,000 or more — insurance requires documented medical necessity. Your neurologist's office typically handles this, but it can take time, so don't be surprised if there's a waiting period before your first infusion is approved.
During the Infusion
IVIG is given through an IV, typically placed in a vein in your arm. The infusion takes anywhere from two to five hours per session, depending on the dose and how well you tolerate it. Most people start with a slow infusion rate, and the nurse may increase the speed gradually as your body adjusts.
Infusions are usually done at a hospital outpatient infusion center, a specialty infusion clinic, or sometimes at home with a nurse present. Home infusion is increasingly common for patients who have established that they tolerate IVIG well.
Bring something to do — a book, headphones, a laptop. Many people watch movies or catch up on podcasts. You may feel fine throughout, or you may feel tired. A lot of people say they feel a mild headache building toward the end of the infusion, which is one of the more common side effects.
Dosing Schedules
Dosing varies by condition:
- GBS (acute): High-dose IVIG given over 5 consecutive days, then treatment is complete
- CIDP (induction): Loading doses over several days, followed by maintenance infusions every 3–4 weeks
- MMN: Initial response induction, then ongoing maintenance every 2–6 weeks
The maintenance schedule for chronic conditions like CIDP is ongoing — IVIG doesn't cure these conditions, it keeps them controlled. Some patients, once their condition has been stable for an extended period, may be able to try tapering the frequency or switching to subcutaneous immunoglobulin (SCIG), a home-based alternative discussed below.
Side Effects and How to Manage Them
Most people tolerate IVIG reasonably well. The side effects are usually mild and manageable. Here's what to expect and what helps:

Common Side Effects
- Headache — the most frequent complaint; often described as a dull, building pressure; premedication with acetaminophen or ibuprofen before the infusion helps many people. Staying well hydrated before and during infusion is also important.
- Fatigue — many people feel wiped out for a day or two after infusion. Plan rest time accordingly.
- Nausea or light-headedness — usually mild; slowing the infusion rate often resolves this
- Infusion site reactions — redness, soreness, or bruising at the IV site; normal and temporary
- Low-grade fever or chills — more common in first few infusions; may improve with subsequent treatments
- Flu-like aching — muscle soreness or joint achiness for a day or two post-infusion
Rare but Serious Risks
Serious adverse events are uncommon but worth knowing about:
- Anaphylaxis — very rare; more likely in patients with IgA deficiency (which is why that blood test is important beforehand)
- Aseptic meningitis — rare; severe headache, neck stiffness, light sensitivity after infusion; requires medical attention
- Thromboembolism — IVIG can thicken blood; people at higher risk for clots (older patients, cardiovascular history) should discuss this with their doctor
- Kidney injury — rare; certain formulations are more nephrotoxic; people with existing kidney issues should discuss formulation choice with their doctor
- Hemolysis — rare destruction of red blood cells; more common with certain blood types
These risks are why IVIG is given in a monitored clinical setting, especially for the first several infusions.
How Long Does IVIG Take to Work?
This is one of the hardest things to wait through. The honest answer is: it varies considerably, and patience is genuinely required.
Research Says
Multiple randomized controlled trials confirm IVIG's effectiveness for CIDP, with response rates of 50–70% in treated patients. For Guillain-Barré syndrome, a 5-day IVIG course has equivalent effectiveness to plasma exchange and can significantly shorten the recovery timeline.
Some people — particularly GBS patients and some CIDP patients — notice meaningful improvement within days to weeks of their first infusion cycle. Strength may begin returning. Numbness may ease. For others, particularly those with more longstanding damage, improvements come over months.
What neurologists typically look for when assessing whether IVIG is working:
- Stopping of disease progression (this alone is a meaningful outcome)
- Gradual improvement in strength or sensation
- Reduction in nerve pain
- Improved scores on standardized disability scales
- Nerve conduction studies showing stabilization or improvement
If IVIG is going to work, you typically see some signal within 3–6 months. If there's no response after a trial period, your neurologist may reconsider whether your diagnosis is correct, or whether a different treatment approach is warranted.
One thing I've heard from several people in our community: the first infusion often brings a temporary period of feeling worse before feeling better. The sudden influx of immune activity can stir things up. If that happens to you, don't interpret it as failure — talk to your neurologist and hang in there for a few weeks.
SCIG: The Home-Based Alternative
For patients who require ongoing maintenance therapy — particularly those with CIDP or MMN — subcutaneous immunoglobulin (SCIG) has become an increasingly attractive alternative to intravenous IVIG.

50–70%
of CIDP patients respond to IVIG with stabilization or improvement in nerve function
SCIG is the same immunoglobulin product but delivered into the fatty tissue just under the skin using a small needle and a pump or syringe. It's given at home, typically once per week, in smaller doses that maintain more stable blood levels than the every-3-to-4-week IVIG cycle.
Benefits of SCIG:
- No IV access required
- No infusion center visits
- More consistent immunoglobulin levels (less “peak and trough” effect)
- Many patients report fewer systemic side effects (less headache, less post-infusion fatigue)
- Easier to incorporate into daily life
The main drawback is that it requires learning to self-inject and managing the logistics of home delivery and storage. It also isn't appropriate for everyone — your neurologist will help determine if SCIG is a reasonable transition once you're stable on IVIG.
Insurance Coverage and Cost
IVIG is one of the more expensive treatments in medicine. A single infusion cycle — depending on the dose, formulation, and whether it's given at a hospital or specialty infusion center — can cost anywhere from $5,000 to over $25,000. For ongoing monthly maintenance, annual costs can reach into six figures before insurance.
The good news: for FDA-approved indications like CIDP, GBS, and MMN, major insurance plans including Medicare typically cover IVIG when medical necessity is well-documented. Your neurologist should submit detailed clinical notes, test results, and treatment justification with the prior authorization request.
If your insurance denies coverage, you have the right to appeal. Many denials are overturned on appeal, especially when your neurologist provides additional documentation. Patient advocacy organizations for specific conditions like CIDP often have resources to help navigate insurance disputes.
Manufacturer patient assistance programs can also help with copays or provide medication at reduced cost for patients who qualify. Ask your neurologist's office or the infusion center about what assistance programs may be available.
If you're thinking about the bigger picture of what neuropathy treatment coverage looks like, our guide to neuropathy insurance coverage breaks down Medicare and private insurance in more detail.
Questions to Ask Your Neurologist About IVIG
If IVIG has come up in your conversations with your doctor, or if you're wondering whether it might be right for you, these are the questions worth asking at your next appointment. Knowing how to talk to your doctor about neuropathy treatment can make a real difference in the quality of conversation you have.

- “Do you believe my neuropathy has an autoimmune or immune-mediated component? What testing supports that conclusion?”
- “Am I a candidate for IVIG based on my diagnosis? Why or why not?”
- “What would a trial of IVIG look like for me — dose, frequency, duration?”
- “How will we measure whether it's working?”
- “What happens if I don't respond after a few cycles?”
- “Is SCIG an option I should consider at some point?”
- “What are the risks most relevant to my situation specifically?”
- “Will you help me get insurance authorization, and what should I expect from that process?”
If you don't feel like your neurologist is engaging fully with your questions, it may be worth considering a second opinion from a neuromuscular specialist — a neurologist who subspecializes specifically in nerve and muscle disorders. These physicians typically have deeper expertise in immune-mediated neuropathies and IVIG management.
IVIG Alongside Other Treatments
IVIG isn't usually a standalone treatment. Most people on IVIG also work with a broader management plan that may include:
- Physical therapy — to rebuild strength and function that was lost during the active phase of the disease
- Occupational therapy — to adapt daily tasks to current functional capacity
- Symptom medications — nerve pain doesn't always resolve immediately even when the immune attack is controlled; medications like duloxetine may continue alongside IVIG
- Fall prevention strategies — particularly important for CIDP patients with balance and gait involvement; our guide to neuropathy and balance is worth reviewing
- Monitoring — regular neurological assessments, nerve conduction studies at intervals, and blood work to track both effectiveness and safety
The goal is not just to stop the damage — it's to help you regain as much function as possible. IVIG gives the nerves a chance to stabilize and, in favorable cases, begin recovering. But recovery still requires active participation in rehabilitation and self-care.
Frequently Asked Questions
How do I know if my neuropathy is autoimmune?
Autoimmune neuropathy is typically identified through a combination of your symptoms, the pattern and progression of nerve involvement, nerve conduction studies and EMG, and blood tests looking for specific antibodies (anti-ganglioside antibodies, anti-MAG antibodies, paraproteins, and others). A neuromuscular specialist is best positioned to interpret these findings and determine if an immune mechanism is driving your neuropathy.
Can IVIG cure neuropathy?
IVIG doesn't cure the underlying autoimmune condition, but it can control it effectively enough that nerve damage stops progressing and some recovery occurs. For conditions like CIDP and MMN, it's generally a long-term management strategy, not a one-time cure. For GBS, a course of IVIG can significantly shorten and reduce the severity of the acute episode, after which many patients have good recoveries without ongoing treatment.
Is IVIG safe for older adults?
IVIG is used in older adults, but with some additional considerations. The risk of blood thickening and potential clots is higher in older patients or those with cardiovascular conditions, so neurologists often use lower infusion rates and monitor more closely. Kidney function should be checked regularly. Overall, IVIG is manageable for most older adults with appropriate precautions.
What's the difference between IVIG and plasma exchange for neuropathy?
Both are used for autoimmune neuropathies like CIDP and GBS. Plasma exchange (plasmapheresis) physically removes the harmful antibodies from your blood by filtering it through a machine. IVIG floods the system with healthy antibodies that neutralize the harmful ones. They have similar effectiveness for many conditions. The choice often comes down to availability, patient tolerance, and individual medical factors. Some patients who don't respond to one are tried on the other.
Does IVIG help with pain specifically?
For immune-mediated neuropathies, IVIG can reduce pain by controlling the underlying immune process causing nerve irritation and damage. However, it's not primarily a pain medication and may not eliminate pain immediately even when working well. Studies specifically looking at idiopathic small fiber neuropathy found IVIG did not significantly reduce pain in that population. Pain management alongside IVIG often involves additional medications and therapies.
Can I travel while on IVIG maintenance therapy?
Yes, many people successfully travel while on IVIG. The main consideration is coordinating infusions with infusion centers at your destination, or transitioning to home SCIG therapy if you travel frequently. Your neurologist's office can help with referrals or prior authorizations needed for infusions in other states or countries.
What if IVIG stops working over time?
Some patients find that IVIG becomes less effective over time — this can happen with CIDP and other chronic conditions. If you notice worsening symptoms between infusions or your condition seems to be progressing again, that's important information to bring to your neurologist promptly. Dose adjustment, more frequent infusions, or transitioning to an alternative treatment like rituximab or mycophenolate may be considered.