
About two years into my neuropathy I had a moment I still think about. I was at the kitchen window watching my husband walk out to the mailbox, and I caught my reflection in the glass and didn't recognize the woman looking back. Not the way she looked. The way she stood. The way she carried herself, careful and small, like she was waiting for the next thing to hurt. I remember saying out loud, “When did I become her?”
If you've been living with neuropathy for any real length of time, you may know the moment I'm describing. It isn't the pain that does it, exactly. It's the slow accumulation of small surrenders — the things you stopped doing, the invitations you stopped accepting, the version of yourself you used to introduce to people. One day you look up and that person is gone, and someone else is standing there in your kitchen.
This is the part of neuropathy nobody warns you about. The doctors talk about nerve damage, the supplement bottles talk about tingling, the support groups talk about pain. Almost nobody talks about the quiet identity grief — the loss of who you used to be. So that's what I want to talk about today, because I think the silence around this is one of the loneliest parts of this disease.
Why Neuropathy Is Different From a Broken Leg
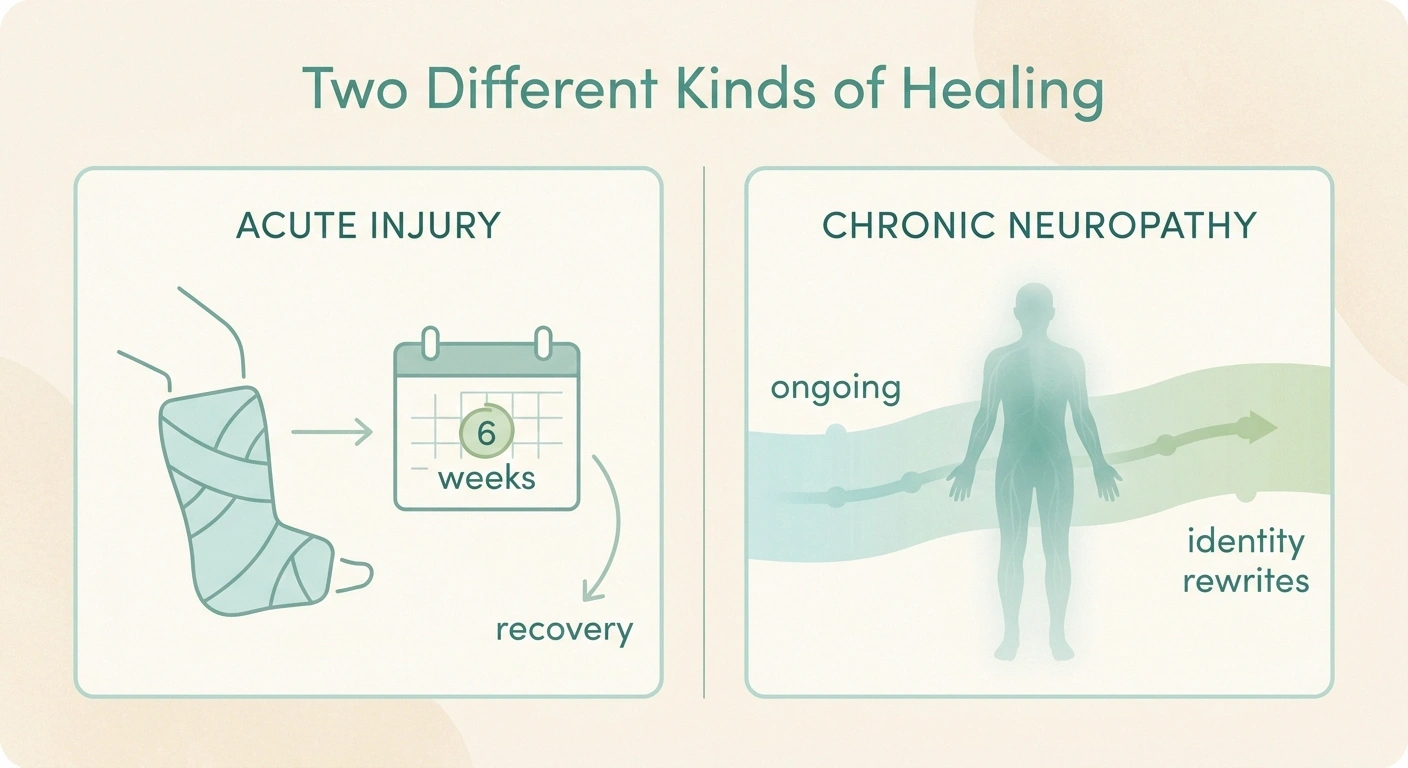
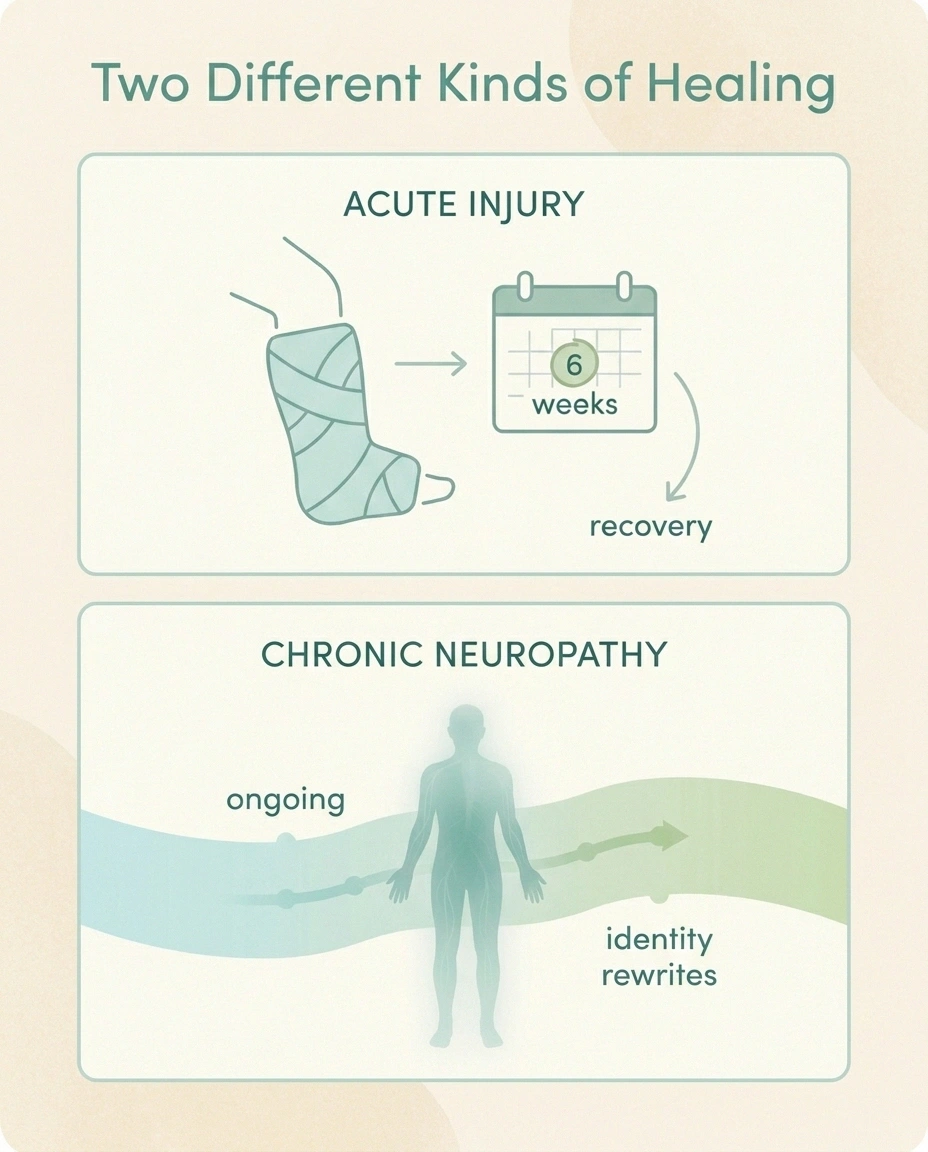
When you break your leg, you and everyone around you understand the deal. There's an injury, there's a recovery, and one day you'll be back to yourself. The “self” doesn't change. Only the leg does, and only for a while.
Key Takeaway
Chronic neuropathy reshapes more than the body. Long-standing neuropathic pain causes measurable changes in the brain's body map, and confiscates roles, hobbies, and routines you didn't agree to give up. The grief is real. Naming it — instead of around it — is one of the most important steps toward rebuilding.
Chronic pain doesn't work like that. Researchers have documented that long-standing neuropathic pain causes real, measurable changes in the somatosensory cortex — the part of the brain that maps your body. Studies on altered bodily perception in chronic pain show that people who live with this for years often report their feet feel “not their own,” or that their hands feel disconnected, or that the painful part of their body has lost its place in the map of who they are. That isn't your imagination. The brain is rewriting itself in response to constant input it can't turn off.
And it isn't just the brain. It's the whole life that grew up around the body that used to work differently. Jobs. Hobbies. Roles. Relationships. The volunteer slot you used to fill. The grandkid you used to chase around the yard. The friend who used to be the one who organized everyone for lunch. When the body changes, all of that gets renegotiated, and the renegotiation isn't quick, and it isn't optional.
The Hidden Grief of “What I Used To Do”
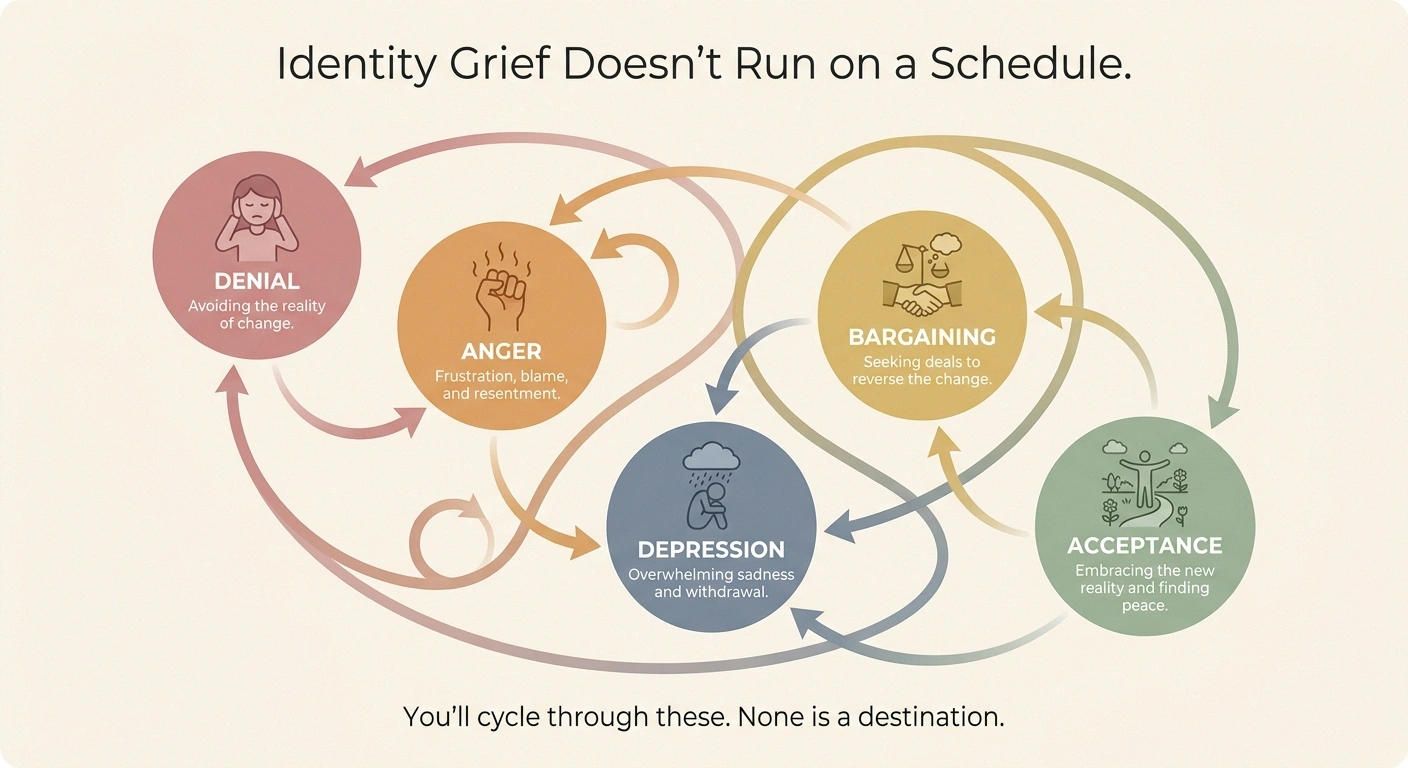
Most of us know about the five stages of grief — denial, anger, bargaining, depression, acceptance — from books or shows. They were originally written about death. But anyone who has lost a piece of themselves to a chronic condition will tell you the stages apply just as well to the death of a former self.
Identity Grief Doesn't Run On a Schedule
Denial
“This isn't permanent. I'll bounce back.”
Anger
“Why me? Why now? Why this body?”
Bargaining
“If I just take the right supplement… if I exercise more…”
Depression
“This is going to be the rest of my life.”
Acceptance
“This is real. Now what kind of life can I build?”
You'll cycle through these. That's normal. None is a destination.
What's strange about chronic-illness grief is that there's no funeral. Nobody sends a casserole. There's no weekend off work. The loss happens in pieces, over months or years, and most of those pieces aren't visible to anyone but you. The day you realized you couldn't garden anymore. The day you stopped wearing the heels. The morning you stood at the bottom of the stairs and decided to take the elevator from now on. Each of those moments is a small grief, and they accumulate into something much bigger.
Pain psychologists who specialize in chronic illness will tell you that naming this grief — actually saying out loud, “I am grieving the person I used to be” — is one of the most important steps in moving forward. As long as the loss is unnamed, it sits underneath everything as a low hum of something wrong. Once it has a name, you can finally turn toward it instead of around it.
The Difference Between Roles and Identity
One of the most useful distinctions I learned, late, is the difference between your roles and your identity. They are not the same thing, even though we often confuse them.
Roles vs. Identity
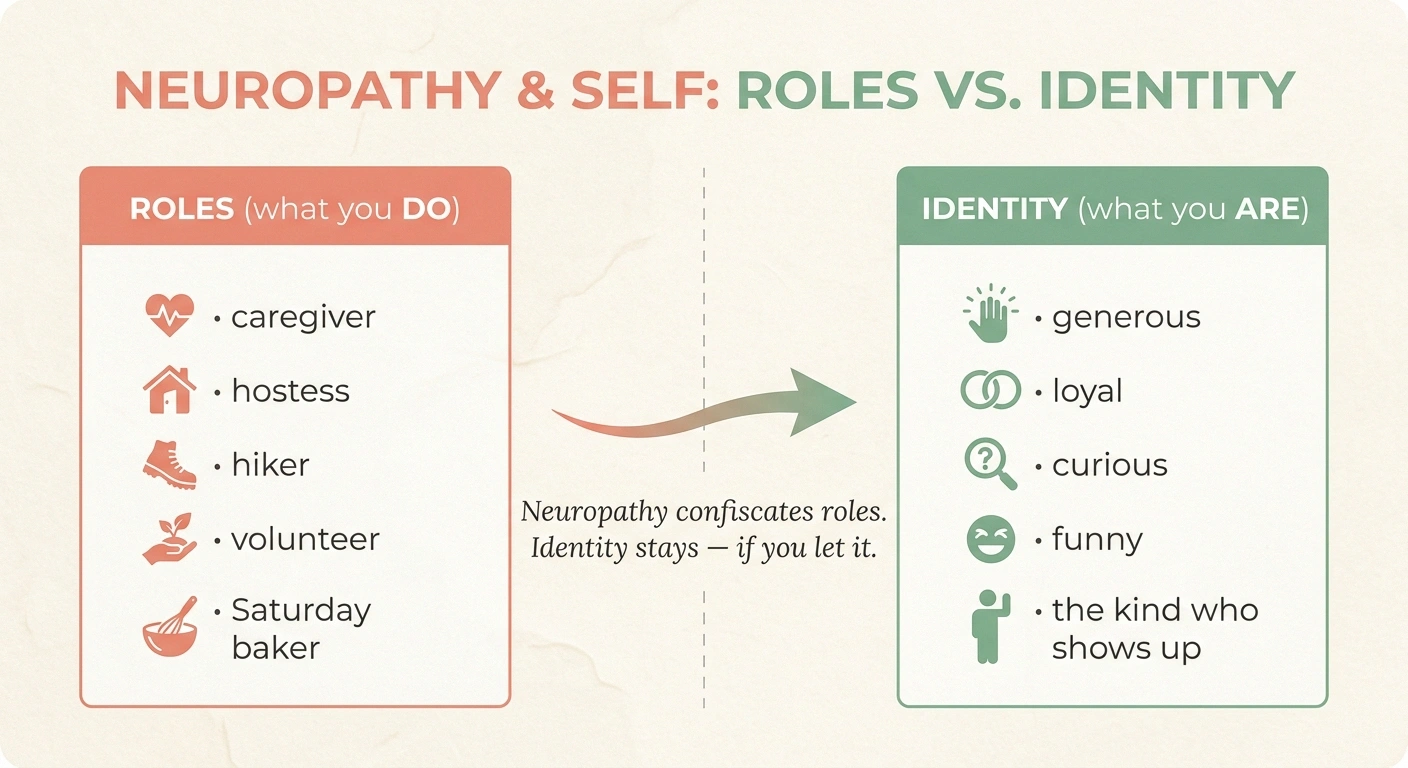
A ROLE is what you DO
Caregiver. Hostess. Hiker. Volunteer. Saturday-morning baker. The one who organizes everyone.
IDENTITY is what you ARE
Generous. Loyal. Curious. Funny. The kind who shows up for people. The one who notices.
Neuropathy confiscates roles. It leaves identity intact — if you let it.
A role is something you do. Caregiver. Hostess. Volunteer. Hiker. Marathon runner. Saturday-morning baker. The person who always organizes the family reunion.
An identity is something you are. Generous. Loyal. Curious. Funny. The kind of person who shows up for people. The kind of person who notices what others miss.
Here's what neuropathy does: it confiscates roles. Sometimes a lot of them. But it leaves your identity intact, if you let it. The hostess who can't host a sit-down dinner anymore is still generous — she shows generosity differently now, with phone calls and notes and the half-hour visit instead of the four-hour party. The hiker who can't hike is still curious about the natural world; she just expresses that curiosity through bird-feeders on the porch and books from the library now.
The trap is when we confuse the role with the identity, and we think that because the role is gone, the identity is gone too. It isn't. It's still in there, looking for a new way out.
Why Other People's Reactions Hurt So Much

One of the hardest parts of identity shift in chronic pain is that other people get to keep the old version of you in their heads, and they don't always update it gracefully.
Research Says
Chronic neuropathic pain produces measurable structural and functional changes in the somatosensory cortex. Patients commonly report that the painful body part feels “not their own” — a phenomenon called altered bodily perception.
Social withdrawal, employment loss, and altered self-concept are documented as some of the most common, and most under-discussed, consequences of chronic neuropathic pain.
The friend who keeps inviting you to things you can no longer do, and gets a little hurt every time you say no. The relative who remembers when you were “the energetic one” and still expects that person to show up. The stranger at the doctor's office who looks at you and decides you don't look sick enough. None of them are usually trying to be cruel. They just haven't had the slow, internal experience of becoming the new version of you, and so the new version reads to them like a disappointment, or an excuse, or a problem.
The cost of this on identity is real. Research on neuropathic pain as an interdisciplinary problem shows that social withdrawal is one of the most common, and most under-discussed, consequences of chronic pain. People stop reaching out because they're tired of explaining. They stop accepting invitations because the post-event flare isn't worth it. And in the silence that follows, the version of themselves that other people remember slowly stops being maintained — until even they start to feel like a stranger.
The Anger Stage Is Normal
If you're in the part of this process where you're furious — at your body, at your doctors, at the people who don't understand, at the universe for rolling these particular dice — that's a real and valid stage of identity grief. The anger and frustration of chronic neuropathy is one of the most under-recognized parts of this disease.
The anger isn't a personality flaw. It's a normal response to losing things you didn't agree to lose. It usually shows up loudest about the time you've finished denying that anything is really wrong, and it tends to be embarrassing and exhausting and lonely all at once. Most people I know who eventually built a peaceful life with neuropathy went through a hot, ugly anger stage first.
If you're in it now, the worst thing you can do is shame yourself for it. The best thing you can do is pour the energy into something that won't be hurt by it — journaling, walking, talking to a therapist, smashing old plates in the driveway, anything physical and productive. The anger is real information about a real loss. It deserves to be respected, processed, and eventually allowed to soften into something quieter.
Acceptance Is Not Giving Up

Of all the words used in chronic pain, “acceptance” is the one most likely to make people angry. It sounds like surrender. It sounds like the doctors and the books and the well-meaning relatives are asking you to stop fighting. That isn't what the word actually means in pain medicine.
Acceptance, as it's used in pain psychology, means accepting reality — not accepting defeat. It means turning toward the truth that this is the body you have, this is the life you're living, and the energy that used to go into pretending otherwise can now be redirected toward making this life as good as possible.
The opposite of acceptance isn't fighting. The opposite of acceptance is exhausting yourself in a war with reality, which leaves you with no resources for the actual life you're trying to live. Acceptance is what frees up the energy to garden differently, work differently, love differently, show up differently — and to discover that “differently” can still be very full.
I'd say it took me about four years to really arrive at acceptance, and I still slide out of it on the bad weeks. It isn't a destination. It's a practice. But the first time you really stand in it, you can feel something heavy you've been carrying set down, and the relief is hard to describe.
Practical Steps for Rebuilding Identity

If you're reading this in the part of the journey where the old version of yourself is gone and the new version hasn't shown up yet, here are some things that have helped me and the people in my support group find our footing again.
Five Steps Toward Rebuilding
- Name what you've lost. Out loud or on paper. Not to dwell — to acknowledge.
- Inventory what's left. Traits, skills, knowledge, relationships. Almost always longer than expected.
- Look for the through-line. Generosity, curiosity, family, beauty — how do you express the value in this body, today?
- Pick one new thing. Not a replacement — something that belongs only to this version of you.
- Update the people who love you. A direct conversation does more than a year of trying to be the old version.
Name what you've lost. Out loud, or on paper. Make a list of the roles, activities, and parts of yourself you've had to set aside. Not to dwell — to acknowledge. Things that aren't named have a way of haunting us. Things we name lose some of their grip.
Inventory what's left. Make a second list. The traits, skills, knowledge, relationships, and parts of yourself that neuropathy has not touched. This list is almost always longer than people expect. The fact that you're still curious enough to read this article is on it.
Look for the through-line. Most people have one or two core things they value above all else — generosity, learning, beauty, justice, humor, family. Those don't change. Ask yourself: how can I express that core value in this body, in this life, today? The expression will be different. The value is the same.
Pick one new thing. Not a replacement for what you lost — those are usually disappointing. Something new, that didn't exist in your old life. A craft you never tried. A subject you never studied. A new friend made through a support group. Something that belongs to this version of you, not the old one.
Update the people who love you. Most of the friction with people who knew the old you is that they have outdated information. A simple, honest conversation — “I've changed, here's how, and here's what I still want from our friendship” — sometimes does more than a year of trying to be the old version for them.
When to Get Professional Support
There's no shame in needing help with this. Pain psychologists, chronic-illness counselors, and therapists who specialize in adjustment to disability are real specialties for a reason. If any of the following are true for you, please consider it.
When to Reach for Professional Help
Crying most days for more than two weeks. Withdrawing from things you used to enjoy. Using more alcohol or pills than you used to. Thoughts that the people in your life would be better off without you.
If any of those resonate, a therapist who works with chronic illness or chronic pain can change the trajectory. This is not weakness. This is medicine.
988 Suicide and Crisis Lifeline — call or text, 24/7. You don't need to be in active crisis. You can call because the day was too heavy.
- You've been crying most days for more than two weeks.
- You've had thoughts that the people in your life would be better off without you.
- You've stopped doing things you used to enjoy and aren't replacing them with anything.
- You're using more alcohol, food, or pills than you used to in order to get through the day.
- You haven't been honest with anyone, including yourself, about how hard this is.
If any of those resonate, you are in the territory where professional help can change the trajectory. The kind of grief work this calls for is different from regular talk therapy — find someone who explicitly works with chronic illness or chronic pain. The link between neuropathy and mental health is well established, and it deserves the same medical respect as the physical symptoms.
If you've had thoughts of suicide, the 988 Suicide and Crisis Lifeline is available 24/7 in the United States. You can call or text 988. You don't have to be in active crisis to call. You can call because the day was too heavy and you don't want to carry it alone.
What I Wish Someone Had Told Me Five Years Ago
You are not who you used to be. That's true. It's also not the tragedy it feels like in the early years.
The version of you that existed before neuropathy was beautiful, and she's worth grieving. But she was also unfinished, like all of us are unfinished. The version of you that's emerging on the other side of this — the one who's had to learn what really matters, who's had to slow down enough to see things she never saw before, who's had to ask for help and learn how to receive it — that version is also beautiful. She's just newer, and she's still figuring herself out, which is uncomfortable in the way that anything new is uncomfortable.
Give her time. Give her grace. The first version of you didn't show up overnight either. She took decades to become herself. This new one will take a while too.
You're still in there. The pain didn't take you. It just rearranged the room.
Frequently Asked Questions
Is it normal to grieve who I was before neuropathy?
Yes. Pain psychologists consistently identify grief as a core experience of chronic illness, not a sign of weakness or failure to cope. The grief is for real losses — roles, capacities, identities — that you didn't choose to give up. Naming it usually helps more than ignoring it.
How long does the identity-shift period last?
It varies enormously. Some people move through it in a year or two, others take longer or move through it in waves. Most people I know who've reached a settled place describe it as a years-long process, not a months-long one, with periodic setbacks during flares or major life events. There is no schedule, and going slowly is not the same as failing.
Why do I feel like a stranger to myself?
Two things are usually happening at once. First, your roles and routines have changed, and our sense of self is built on those things more than we realize. Second, chronic pain produces measurable changes in the brain's body map, which can make even your physical self feel less familiar. Both effects are real, both are documented, and both can ease with time and the right support.
What if my family and friends don't understand?
Many won't, fully — they haven't lived inside it. The most useful response is usually a direct, calm, non-defensive conversation about what's changed and what you still want from the relationship. Some relationships will adapt; some will not. Investing more in the ones that adapt and less in the ones that don't is not selfish, it's wise spoon management.
Is acceptance the same as giving up on getting better?
No. Acceptance in pain psychology means accepting reality so you can act effectively within it. It doesn't mean stopping treatment, stopping advocacy, or stopping hope. It means refusing to spend the energy of every day fighting the existence of the disease, so that you have energy left to live a life worth fighting for.
Can therapy actually help with chronic-pain identity issues?
Yes, particularly therapy that specializes in chronic illness, chronic pain, or adjustment to disability. Acceptance and Commitment Therapy (ACT), Cognitive Behavioral Therapy for chronic pain (CBT-CP), and trauma-informed therapy are among the modalities with research support for this population. Your primary care doctor or neurologist can usually refer.
How do I rebuild a sense of purpose when so much has changed?
Start with values, not activities. Identify the two or three things that have always mattered most to you — generosity, curiosity, family, justice, beauty — and ask how you can express those values inside the life and body you have now. The expression will look different. The values will not.
The Last Thing
If you take only one thing away from this article, let it be this: the woman or man you see in the kitchen-window reflection is not a stranger. She's just a chapter you haven't read yet.
You're allowed to grieve. You're allowed to be angry. You're allowed to take years to figure this out. And you're allowed to discover, eventually, that the new version of you has things to teach you that the old version never could.
That's not a consolation prize. That's a real life. It's just a different one than you ordered.


