When most people in our community say “neuropathy,” they mean their feet. Sometimes their hands. The slow, length-dependent kind that creeps up the body from the toes. So it can come as a real shock when a different kind of nerve damage shows up — one that changes the face overnight, makes one eye stop tracking, or sets off electric-shock pain in a cheek that hasn't been touched. That's a cranial neuropathy, and it's a very different animal from what most of us know.
I'm writing about this because two members of my support group have had cranial neuropathies in the last few years — one with Bell's palsy after a stressful winter, one with trigeminal neuralgia that took two years to diagnose properly. In both cases, what they wished they'd known earlier could have saved them weeks of fear, ER visits that didn't help, and treatments that didn't fit. So this is the conversation I wish someone had handed them on day one.
What Cranial Neuropathies Are, In Plain English
Your brain has twelve pairs of nerves that come directly out of the base of the skull rather than running through the spinal cord. They're called cranial nerves, and they handle most of the things your face, eyes, mouth, and throat do — seeing, hearing, smelling, tasting, smiling, chewing, swallowing, balance, and the autonomic functions like tearing and salivation.
Key Takeaway
Cranial neuropathies affect the 12 nerves coming directly out of the brainstem, not the long peripheral nerves. They appear suddenly, affect single nerves, and often resolve more completely than peripheral neuropathy. But some presentations are time-sensitive emergencies — sudden double vision with pupil involvement, multiple cranial nerves at once, sudden vision loss.
A cranial neuropathy is damage to one or more of those twelve nerves. It produces symptoms in the head, face, eyes, mouth, throat, or neck — not in the hands or feet. The cause might be similar to the causes of peripheral neuropathy in some cases (diabetes, autoimmune disease, infection, trauma), or completely different (a brain tumor pressing on a nerve, a viral infection of the nerve itself, an aneurysm).
The two cranial neuropathies people are most likely to have heard of are Bell's palsy, which affects the seventh cranial nerve and causes one-sided facial droop, and trigeminal neuralgia, which affects the fifth cranial nerve and causes severe, electric-shock face pain. Those two together account for the majority of cases people end up reading about.
The Twelve Cranial Nerves and What They Do
You don't need to memorize this list, but knowing roughly which nerve does what helps make sense of cranial neuropathy symptoms when they appear.
The 12 Cranial Nerves — Quick Reference
Olfactory — smell
Optic — vision
Oculomotor — most eye movements, eyelid lift, pupil
Trochlear — downward and inward eye movement
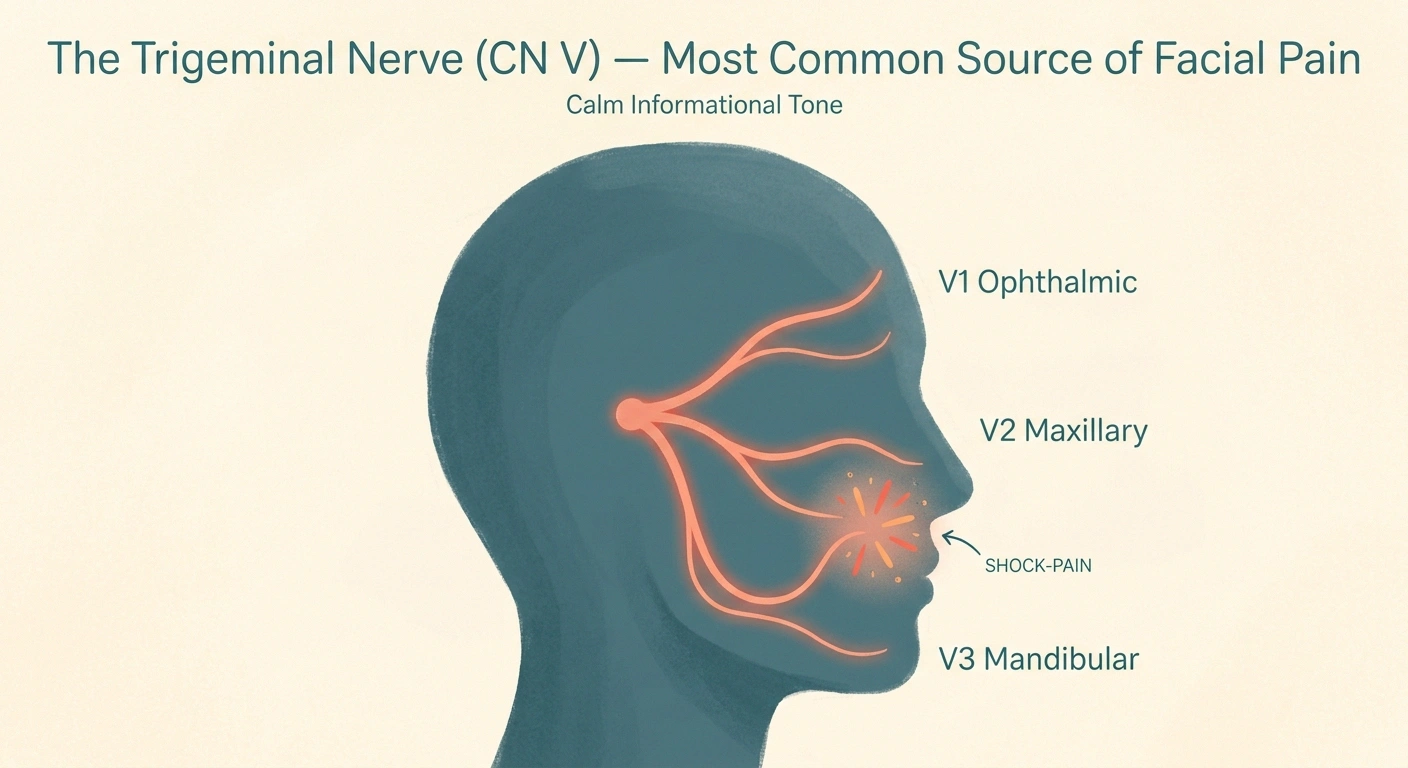
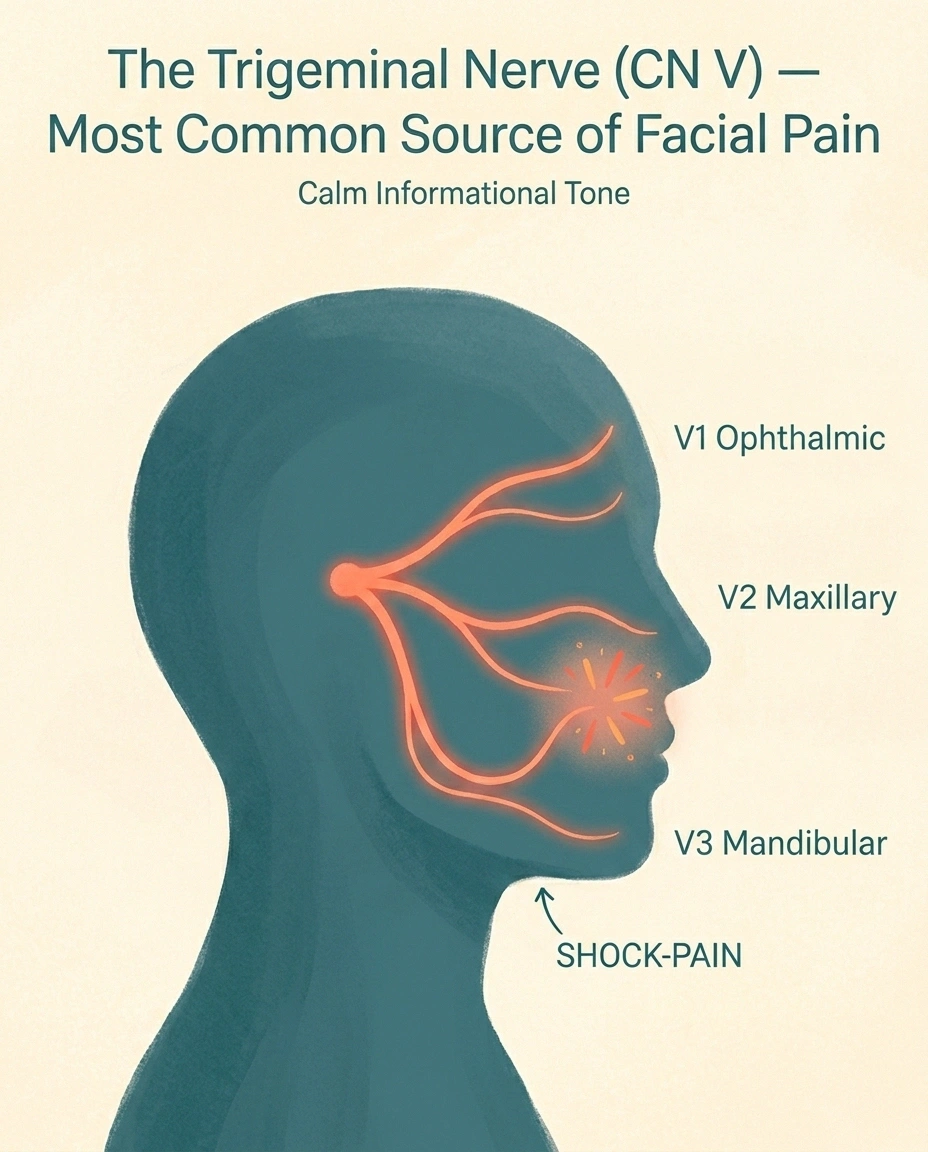
Trigeminal — face sensation, chewing — trigeminal neuralgia
Abducens — outward eye movement
Facial — facial expression, taste, tearing — Bell's palsy
Vestibulocochlear — hearing and balance
Glossopharyngeal — throat sensation, taste, gag reflex
Vagus — voice, swallowing, autonomic functions
Accessory — shoulder shrug, head turn
Hypoglossal — tongue movement
- I — Olfactory: sense of smell.
- II — Optic: vision.
- III — Oculomotor: most eye movements, eyelid lift, pupil constriction.
- IV — Trochlear: downward and inward eye movement.
- V — Trigeminal: sensation of the face; chewing muscles. The big one for face pain.
- VI — Abducens: outward eye movement.
- VII — Facial: facial expression, taste in the front two-thirds of the tongue, tearing, salivation. The Bell's palsy nerve.
- VIII — Vestibulocochlear: hearing and balance.
- IX — Glossopharyngeal: sensation in the back of the throat, taste in the back of the tongue, gag reflex.
- X — Vagus: voice, swallowing, autonomic functions throughout the chest and abdomen.
- XI — Accessory: shoulder shrug and head turn muscles.
- XII — Hypoglossal: tongue movement.
When one of these nerves is damaged, the symptoms map directly onto its job. A damaged optic nerve causes vision problems. A damaged facial nerve causes facial droop. A damaged trigeminal nerve causes facial pain or numbness. Knowing which nerve is involved is the first step in figuring out why.
The Most Common Cranial Neuropathies
Of the twelve nerves, a small handful account for most of what neurologists actually see. Here's what each looks like in real life.
Bell's palsy (CN VII). Usually comes on over hours to a day or two — sometimes you wake up with it. One side of the face droops. The eye on that side may not close fully. A smile is crooked. Drinking water dribbles. Some people lose taste on the front of the tongue or experience hyperacusis (sounds seem painfully loud) on the affected side. The cause is often viral, particularly herpes simplex reactivation, though many cases are technically called “idiopathic.” About 70 to 85 percent of cases recover fully, especially if treated with prednisone within 72 hours of onset. Treatment within that window genuinely matters.
Trigeminal neuralgia (CN V). Brief, intense, electric-shock pain in the cheek, jaw, gums, lip, or forehead — usually on one side. Triggered by light touch, brushing teeth, eating, or even cold air on the face. Episodes last seconds, but a flare can include hundreds of episodes a day for weeks. The cause is often a small artery pressing on the nerve where it exits the brainstem; less commonly, it's multiple sclerosis or a tumor. Trigeminal neuralgia is its own deep topic and worth reading separately if you suspect it. Carbamazepine and oxcarbazepine are first-line; microvascular decompression surgery and gamma knife radiosurgery are options for refractory cases.
Microvascular cranial nerve palsies (often CN III, IV, or VI). Sudden onset of double vision or eye-movement problems, typically in someone with diabetes or hypertension. The mechanism is small-vessel ischemia of the nerve, similar to what causes the foot-and-hand neuropathy of diabetes. Most resolve in three to six months once the underlying condition is controlled. The crucial caveat: a CN III palsy that involves the pupil (a dilated pupil that doesn't react to light) is a red flag for an aneurysm and needs emergency imaging.
Vestibular neuritis (CN VIII). Sudden, severe vertigo lasting days, often after a viral illness. No hearing loss in pure vestibular neuritis; if hearing is lost too, it's called labyrinthitis. Recovery is usually complete but can take weeks.
Glossopharyngeal neuralgia (CN IX). Brief shock-like pain at the back of the throat, ear, or tongue base, triggered by swallowing or talking. Less common than trigeminal neuralgia, treated with similar medications.
Multiple cranial neuropathies. When more than one cranial nerve is affected at the same time, the differential narrows quickly: skull-base tumors, leptomeningeal disease, Guillain-Barré variants like Miller Fisher syndrome, sarcoidosis, or certain infections. Guillain-Barré syndrome can include cranial nerve involvement, especially in its facial-onset variants.
Why Cranial Neuropathies Happen
The causes of cranial neuropathy fall into several categories, and a thorough workup will usually run through most of them.
Vascular. Diabetes and hypertension can damage the small blood vessels supplying cranial nerves. Stroke can affect cranial nerve nuclei in the brainstem. Aneurysms can compress nerves directly.
Infectious. Lyme disease commonly affects the seventh nerve, sometimes on both sides. Herpes simplex and varicella-zoster (shingles) can produce facial palsies and post-herpetic neuralgia. Bacterial meningitis can inflame multiple cranial nerves at once. Otitis media (middle ear infection) can spread to nearby nerves.
Autoimmune and inflammatory. Sarcoidosis is famous among neurologists for affecting cranial nerves, especially CN VII, often on both sides. Multiple sclerosis frequently involves the optic nerve and can cause trigeminal neuralgia. Sjögren's syndrome can produce trigeminal sensory neuropathy. Guillain-Barré variants can affect cranial nerves alongside or before the limb weakness.
Compressive. Tumors near the cranial nerves — vestibular schwannomas (acoustic neuromas), meningiomas, pituitary tumors — can press on a nerve and produce gradually progressive symptoms. New-onset cranial neuropathy that develops over weeks to months, rather than suddenly, deserves brain imaging.
Traumatic. Skull-base fractures, facial trauma, and surgical injury can damage cranial nerves directly.
Increased intracranial pressure. Anything that raises pressure inside the skull — tumors, hemorrhage, idiopathic intracranial hypertension — can stretch or compress cranial nerves, especially CN VI.
Idiopathic. A meaningful share of Bell's palsy cases have no clearly identified cause, though many are now thought to be viral. The label “idiopathic” is honest, not lazy — it means we don't know exactly why this nerve, this person, this week.
Symptoms That Warrant the Emergency Room
Not every cranial neuropathy is an emergency. Most Bell's palsy cases, microvascular palsies in well-controlled diabetics, and stable trigeminal neuralgia can wait for a regular appointment. But some presentations are red flags that mean go now, not later.
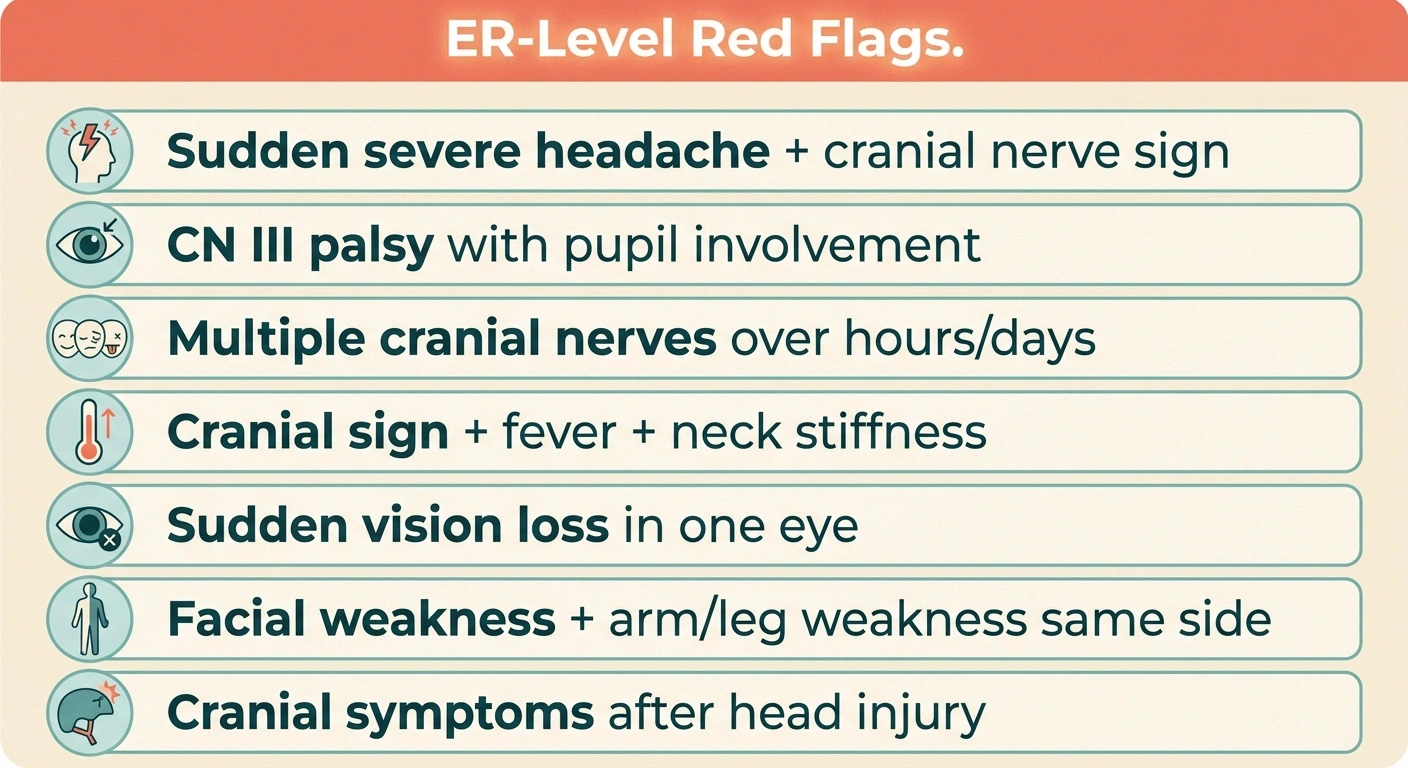
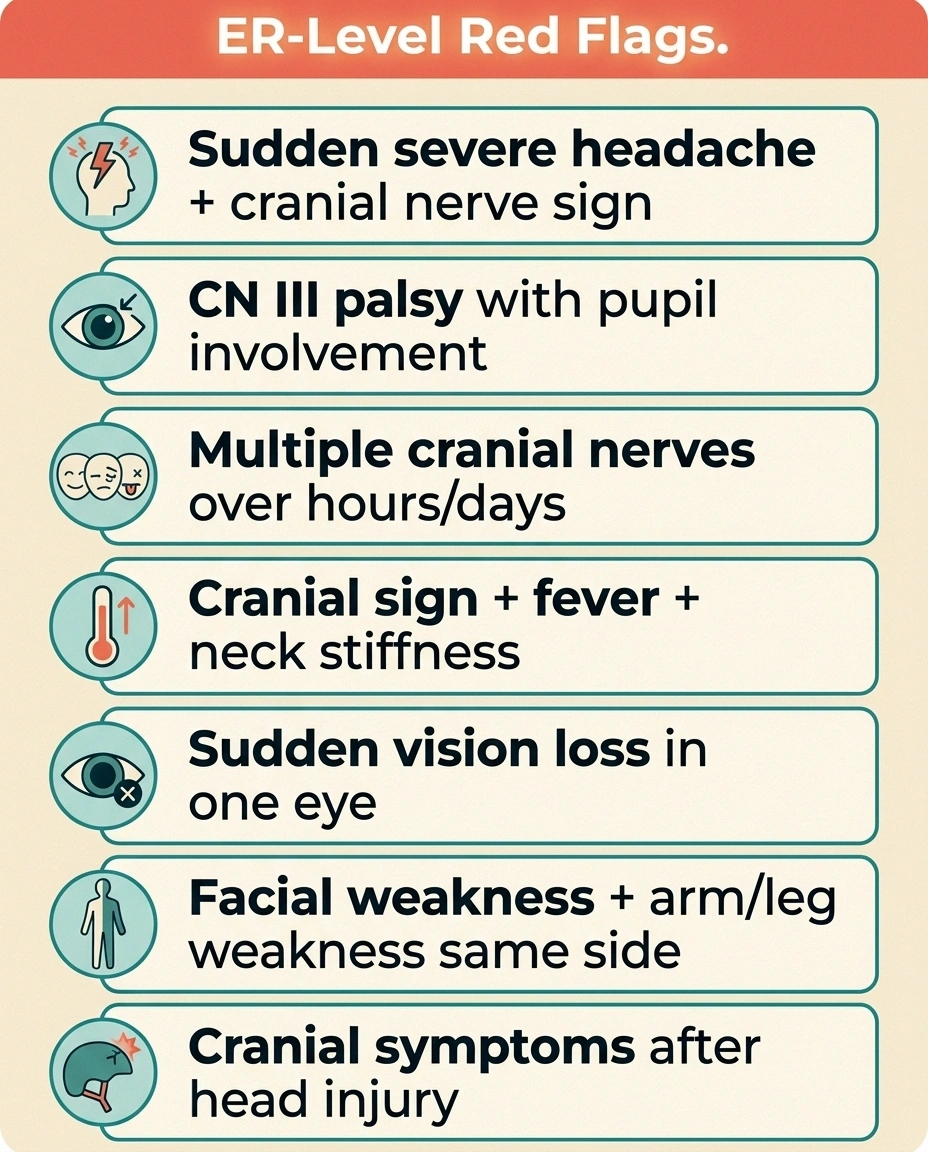
ER-Level Red Flags
- Sudden severe headache + any cranial nerve sign
- CN III palsy with pupil involvement (dilated pupil that doesn't react)
- Multiple cranial nerves affected over hours/days
- Cranial nerve symptom + fever + neck stiffness
- Sudden vision loss in one eye
- Facial weakness + arm/leg weakness on the same side
- Cranial symptoms after any head injury
These presentations need imaging within hours, not days.
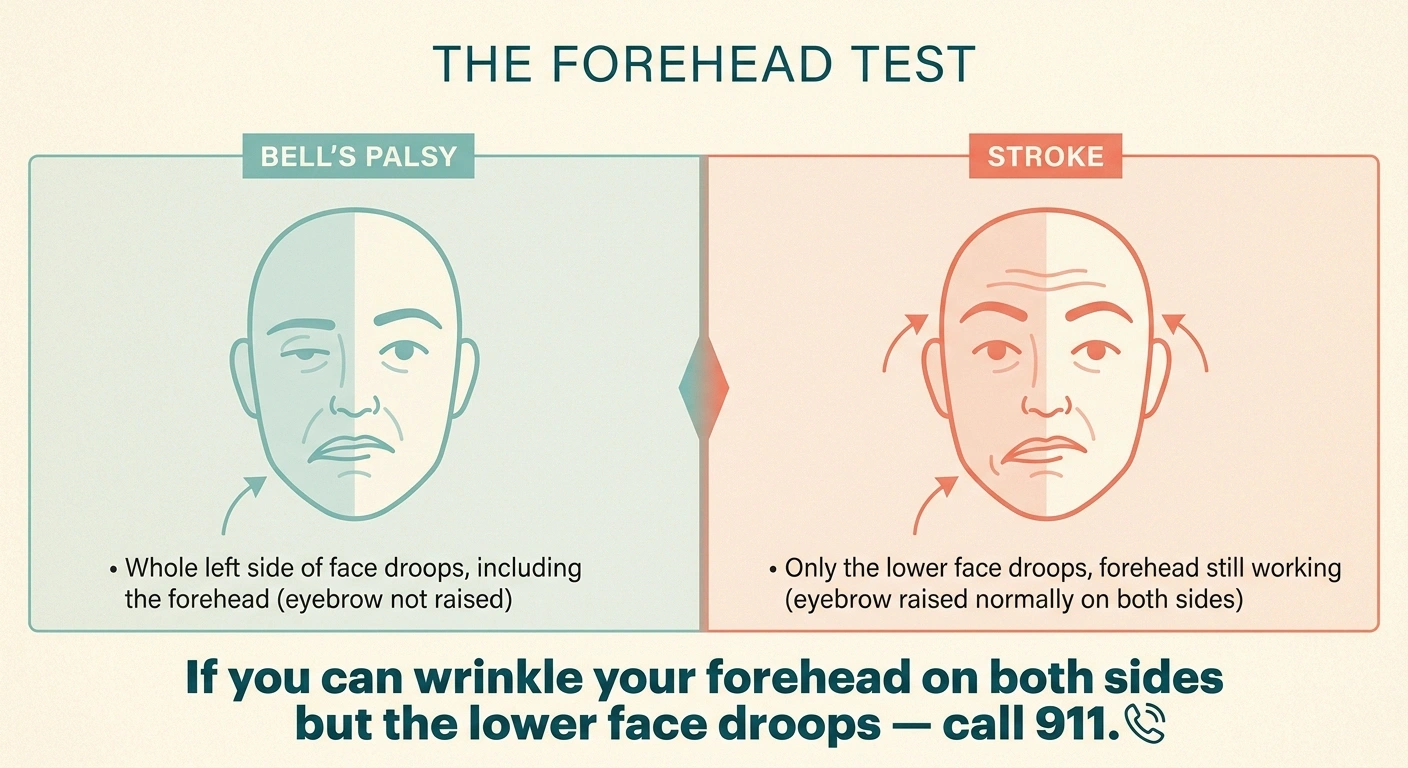
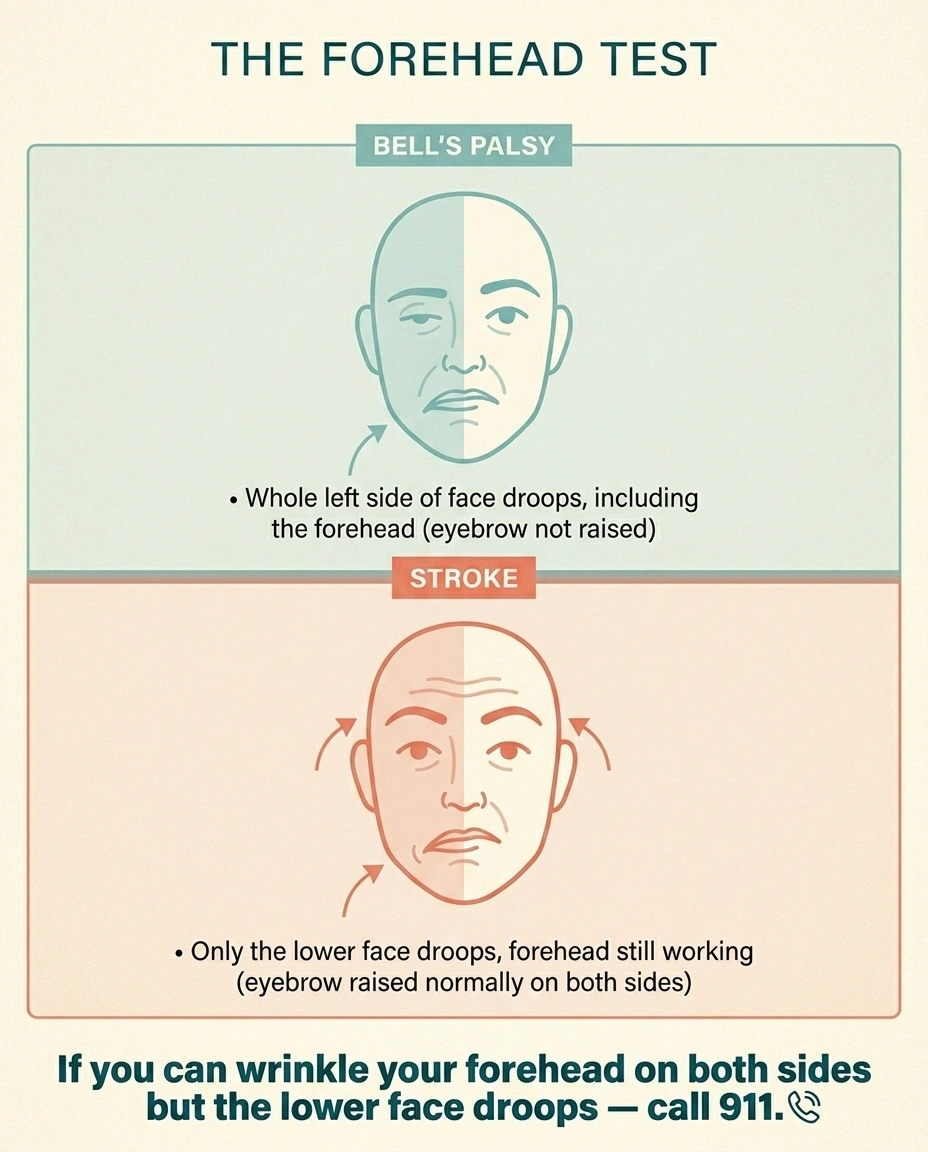
Bell's Palsy vs. Stroke — The Forehead Test
Bell's Palsy (CN VII)
Whole side of face affected, including the forehead. Cannot raise eyebrow on affected side.
Stroke
Forehead usually spared. Can wrinkle forehead on both sides. Lower face droops. Often arm/leg weakness too.
If you can wrinkle your forehead on both sides but the lower face is drooping, get evaluated for stroke immediately.
- Sudden severe headache plus any cranial nerve sign (especially CN III with pupil involvement) — possible aneurysm or bleed.
- Multiple cranial nerves becoming affected over hours or days — possible serious infection, inflammation, or tumor.
- Cranial nerve symptoms with fever and neck stiffness — possible meningitis.
- Sudden vision loss in one eye — possible optic neuritis or vascular event.
- Facial weakness with weakness in the arm or leg on the same side — possible stroke. (Bell's palsy alone affects only the face, including the forehead. A stroke usually spares the forehead.)
- Cranial nerve symptoms following a head injury, even a minor one — needs evaluation.
Bell's palsy versus stroke is the distinction that trips up the most people. The shorthand: Bell's affects the whole side of the face including the forehead (you can't raise that eyebrow). A stroke usually leaves the forehead working because of how the upper face is wired. If you can wrinkle your forehead on both sides but the lower face is drooping, get evaluated for stroke immediately.
Getting Diagnosed
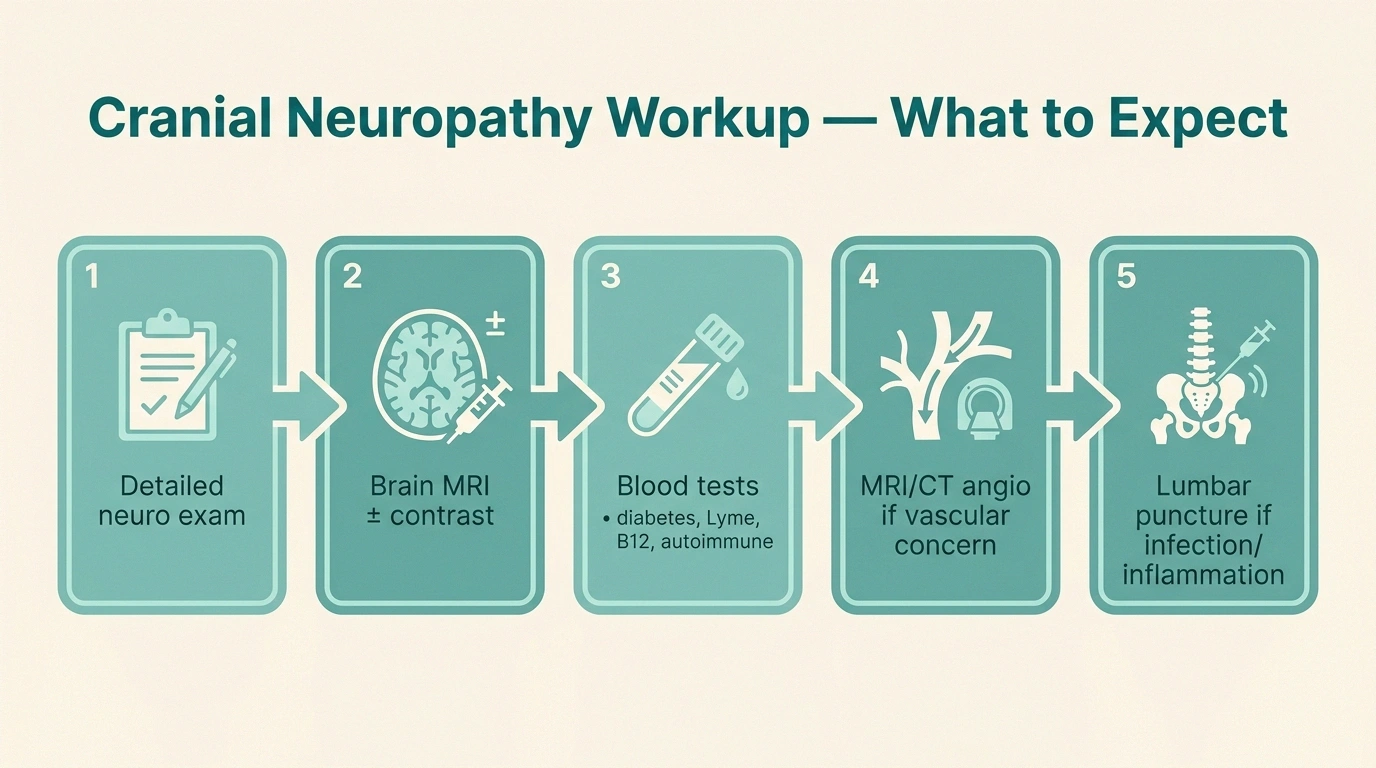
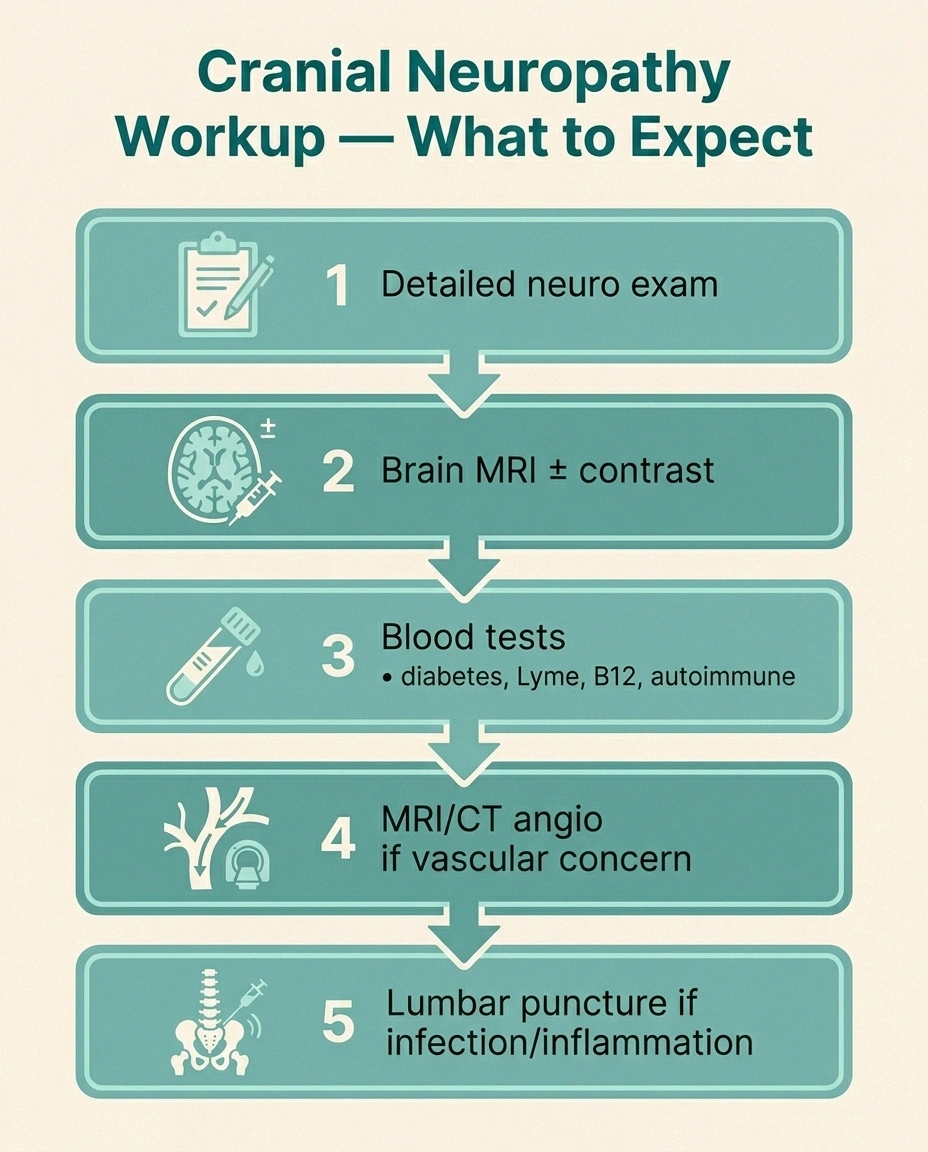
The diagnostic workup for a cranial neuropathy depends heavily on which nerve is involved and how it presented. A typical evaluation might include:
- Detailed neurological exam. Testing each cranial nerve specifically — eye movements, facial sensation and movement, hearing, balance, taste, swallow, tongue movement, neck strength.
- Brain MRI with and without contrast. The single most useful test for most cranial neuropathies, especially if anything looks atypical or progressive.
- MRI angiography or CT angiography. If aneurysm or vascular cause is suspected.
- Lumbar puncture. If infection, inflammation, or leptomeningeal disease is on the differential.
- Blood tests. Diabetes screening, Lyme titer, ACE level (sarcoidosis), B12 level, thyroid function, autoimmune panels — depending on the clinical picture. A standard neuropathy diagnostic workup is a useful starting point and shares many of the same labs.
- EMG and nerve conduction studies. Less commonly needed for cranial neuropathies than for peripheral ones, but specific tests like blink reflex studies can help characterize trigeminal or facial nerve damage.
The most useful first step is usually a neurologist, not a primary care doctor — the exam findings are subtle, the differential is wide, and the imaging needs to be ordered correctly. If your primary care physician is willing to refer quickly, that's a real gift. If you're stuck waiting weeks, the urgent care or ER route is reasonable for any rapidly progressive or red-flag presentation.
Treatment by Nerve

Treatment depends on which nerve is involved and what's causing the damage. Some quick orientation:
72 hrs
window for prednisone in Bell's palsy
Steroids started within 72 hours of onset substantially improve recovery rates. The clock starts at first symptom — don't wait.
Bell's palsy. Oral prednisone (corticosteroids) within 72 hours of onset is the gold standard and substantially improves recovery rates. Antiviral drugs are sometimes added in severe cases. Eye protection — artificial tears during the day, lubricating ointment and a patch or taping the eye shut at night — is critical when the eye doesn't close fully, because corneal damage is the main avoidable complication. Facial physical therapy, sometimes called neuromuscular retraining, helps a subset of patients with prolonged or incomplete recovery.
Trigeminal neuralgia. Carbamazepine or oxcarbazepine first; gabapentin, baclofen, or other agents added or substituted as needed. For pain refractory to medication, microvascular decompression surgery (separating the offending blood vessel from the nerve) has the best long-term success rate. Gamma knife radiosurgery and percutaneous procedures are non-surgical alternatives.
Microvascular cranial nerve palsies. The treatment is largely not the nerve — it's the underlying condition. Tighter blood sugar control, blood pressure management, lipid control. Most resolve in three to six months. If they don't, the diagnosis usually needs to be revisited.
Infection-related cranial neuropathies. Treat the infection. Lyme disease responds to appropriate antibiotics, especially if treated early. Bacterial meningitis is an emergency requiring immediate IV antibiotics. Viral causes are often self-limited but can be treated with antivirals when identified.
Compressive lesions. Surgery, radiation, or watchful waiting depending on the lesion type, location, growth rate, and the patient's overall health.
How Cranial Neuropathies Differ From Peripheral Neuropathy
If you're already living with peripheral neuropathy in your feet or hands, you may wonder whether a new cranial neuropathy is “the same disease moving up.” Usually it isn't. The two patterns of nerve damage tend to have different causes, different timelines, and different treatments.
Cranial vs. Peripheral Neuropathy
Cranial
- Sudden onset
- Single-nerve focal
- Often unilateral
- Vascular, infectious, autoimmune, compressive
- Usually recovers fully
Peripheral
- Slow, gradual onset
- Length-dependent (toes first)
- Bilateral, symmetric
- Metabolic, toxic causes
- Often persists long-term
Peripheral neuropathy is typically length-dependent — it starts at the longest nerves (toes, fingers) and progresses slowly. The mechanism is often metabolic (diabetes, alcohol, B12 deficiency) or toxic (chemotherapy, certain medications). It's usually bilateral and symmetric.
Cranial neuropathy is typically focal — it affects a single nerve or a small set of nerves, often suddenly. The mechanism is more likely to be vascular, infectious, compressive, or autoimmune. It's often unilateral.
There are exceptions. Diabetes can produce both, and sarcoidosis or Sjögren's can affect both peripheral and cranial nerves. Guillain-Barré variants can involve both. So the appearance of a new cranial neuropathy in someone with established peripheral neuropathy isn't automatically unrelated — but it usually deserves its own workup, not just an assumption that “the diabetes is acting up.”
Living With a Cranial Neuropathy
Recovery from cranial neuropathy looks different from recovery from peripheral neuropathy. Many cranial neuropathies resolve completely or nearly so in months, which is more hope than a lot of us with peripheral neuropathy are used to. But the period during which they're active can be very disorienting — your face, your vision, or your voice is the part of your body most central to your identity, and damage there hits differently than damage to a foot.
Some practical guidance for the active period of a cranial neuropathy:
- Protect what isn't working. If your eye won't close, tape it shut at night and use lubricating drops during the day. If your face droops, watch for food and drink leaks. If your throat doesn't swallow well, eat slowly and sit upright.
- Don't isolate. Bell's palsy especially can make people withdraw out of self-consciousness. The withdrawal hurts more than the temporary appearance does. Tell the people in your life what's happening; most will rise to it.
- Track your recovery. Photos every few days for facial symptoms. Notes for pain frequency for trigeminal neuralgia. The “feeling” of progress is unreliable; the data is more honest.
- Ask about physical therapy. Facial neuromuscular retraining is a real specialty for Bell's palsy that hasn't fully recovered, and it isn't always offered without asking.
- Treat the mood piece. Cranial neuropathies, especially facial ones, often produce a meaningful emotional impact during recovery. Mental health support is part of the treatment, not separate from it.
Frequently Asked Questions
What's the difference between a cranial neuropathy and a stroke?
A cranial neuropathy is damage to a single nerve at or after it leaves the brainstem; a stroke is damage to brain tissue itself, often affecting multiple functions. Bell's palsy affects the whole side of the face including the forehead, while a stroke usually leaves the forehead working. Sudden facial droop with weakness in the arm or leg on the same side, or with slurred speech, suggests stroke and is an emergency.
Can cranial neuropathies be reversed?
Often yes, more reliably than peripheral neuropathies. Most Bell's palsy cases recover fully or near-fully within months, especially with prompt prednisone. Microvascular cranial nerve palsies in diabetics typically resolve in three to six months. Trigeminal neuralgia is usually managed rather than cured but is highly treatable. Compressive and progressive causes have variable outcomes depending on the underlying lesion.
Does diabetes cause cranial neuropathy?
Yes. Diabetes is a leading cause of microvascular cranial nerve palsies, especially affecting eye-movement nerves (CN III, IV, VI) and producing sudden double vision. These typically improve in three to six months with good blood sugar control. Diabetic cranial neuropathies follow the same general pattern as other diabetic nerve damage but are usually more focal and faster to recover.
Is Bell's palsy the same as a cranial neuropathy?
Bell's palsy is a specific cranial neuropathy — damage to the seventh cranial nerve (the facial nerve), usually idiopathic or viral. So Bell's palsy is one type of cranial neuropathy, but not all cranial neuropathies are Bell's palsy.
How long does a cranial neuropathy take to heal?
It depends on the nerve and the cause. Bell's palsy: most improvement happens in the first three months, with full recovery typically within six to nine months. Microvascular palsies: usually three to six months. Trigeminal neuralgia: medication-managed long-term rather than healed in the usual sense. Tumor- or compression-related cranial neuropathies depend on whether and how the lesion is treated.
Can stress cause a cranial neuropathy?
Stress is not usually a direct cause but can be a trigger for some viral reactivations, including the herpes simplex reactivation associated with many Bell's palsy cases. Stress also worsens trigeminal neuralgia flares. Managing stress is unlikely to prevent cranial neuropathy on its own, but it's a reasonable supporting strategy.
Should I see a neurologist for a cranial neuropathy?
Yes, in almost all cases. The diagnostic workup is more nuanced than a primary care office is set up to do quickly, and the right imaging and lab tests depend on which nerve is involved. A neurologist with expertise in neuro-ophthalmology, neuro-otology, or peripheral nerve disease — depending on the symptom — is the right specialist. Your primary care doctor can refer.
The Bottom Line
Cranial neuropathies are a different family of conditions from the foot-and-hand neuropathy most of us live with. They appear suddenly, affect single nerves, and often resolve more completely than peripheral neuropathies do. They also include some genuinely time-sensitive presentations — a CN III palsy with pupil involvement, multiple cranial nerves at once, sudden vision loss — where a few hours can matter.
If something new and strange happens to your face, your eyes, your hearing, or your voice, take it seriously. Get to a doctor who can examine the cranial nerves properly and order the right imaging. Most stories end with recovery. The ones that don't are usually the ones that waited too long to start.


