
This is one of the most uncomfortable conversations I have in our support group, because it happens to people who were doing everything they thought was right. They added a B-complex because someone told them it was good for nerves. They picked up a “stress relief” multivitamin that promised more energy. Maybe their doctor mentioned B6 in passing. And then, over months, the same tingling and numbness they were trying to fix actually got worse — and nobody connected the dots until it had been going on for a year.
I'm Janet Ellis. I am a community advocate who has lived with neuropathy for years; I am not a doctor or a pharmacist. What I can do is translate what the medical and regulatory literature actually says about pyridoxine (vitamin B6) and the kind of nerve damage that a “helpful vitamin” can quietly cause when the dose is too high or the use is too long. If you are reading this because you suspect this is you, please do not panic. There is a lot of nuance to this story, and most people who catch it early recover.
The Counterintuitive Problem
B6 is one of those vitamins that gets recommended for nerve health, and there are real reasons for that. The active form of B6 (pyridoxal-5-phosphate, or PLP) is a coenzyme for over 100 enzymatic reactions, including several that nerves depend on for normal function. A genuine B6 deficiency can absolutely cause neuropathy, and correcting that deficiency does help.
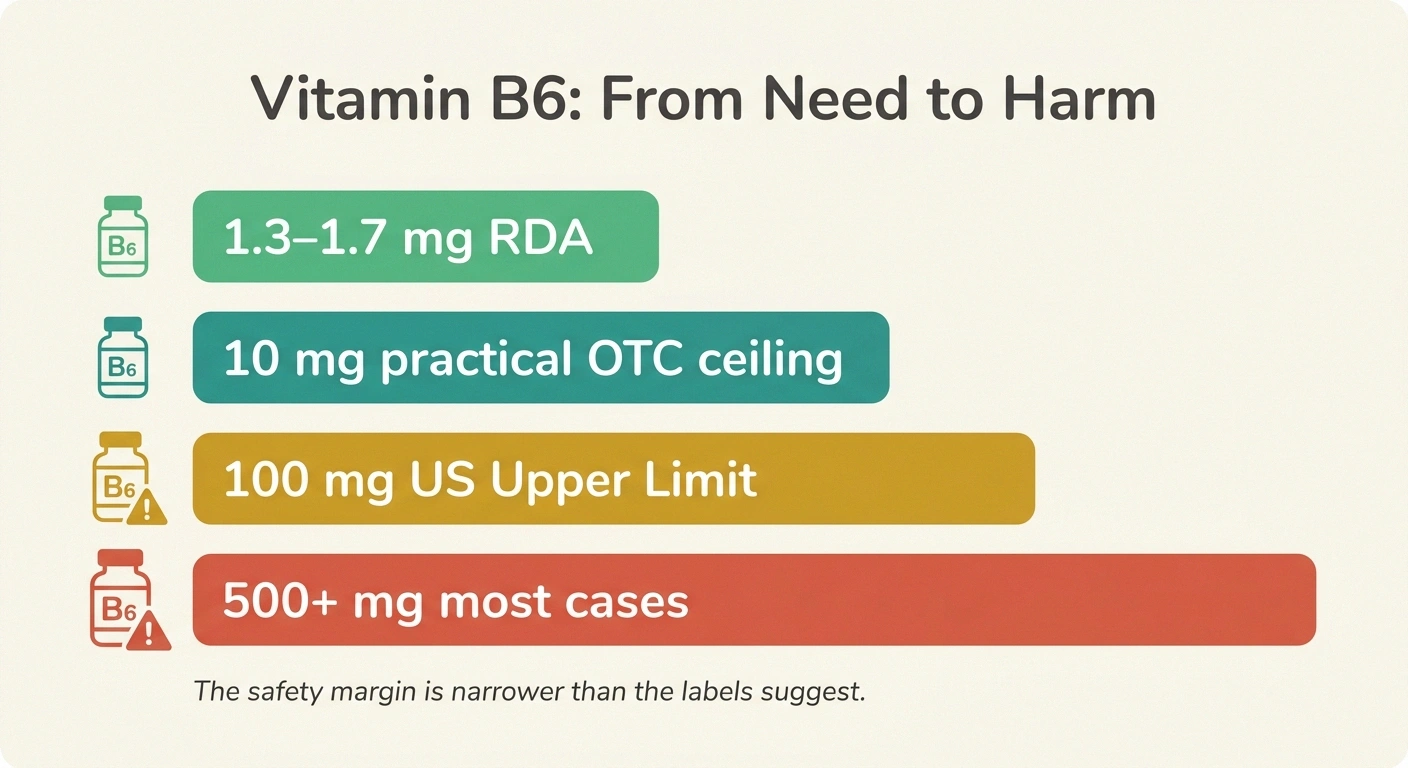
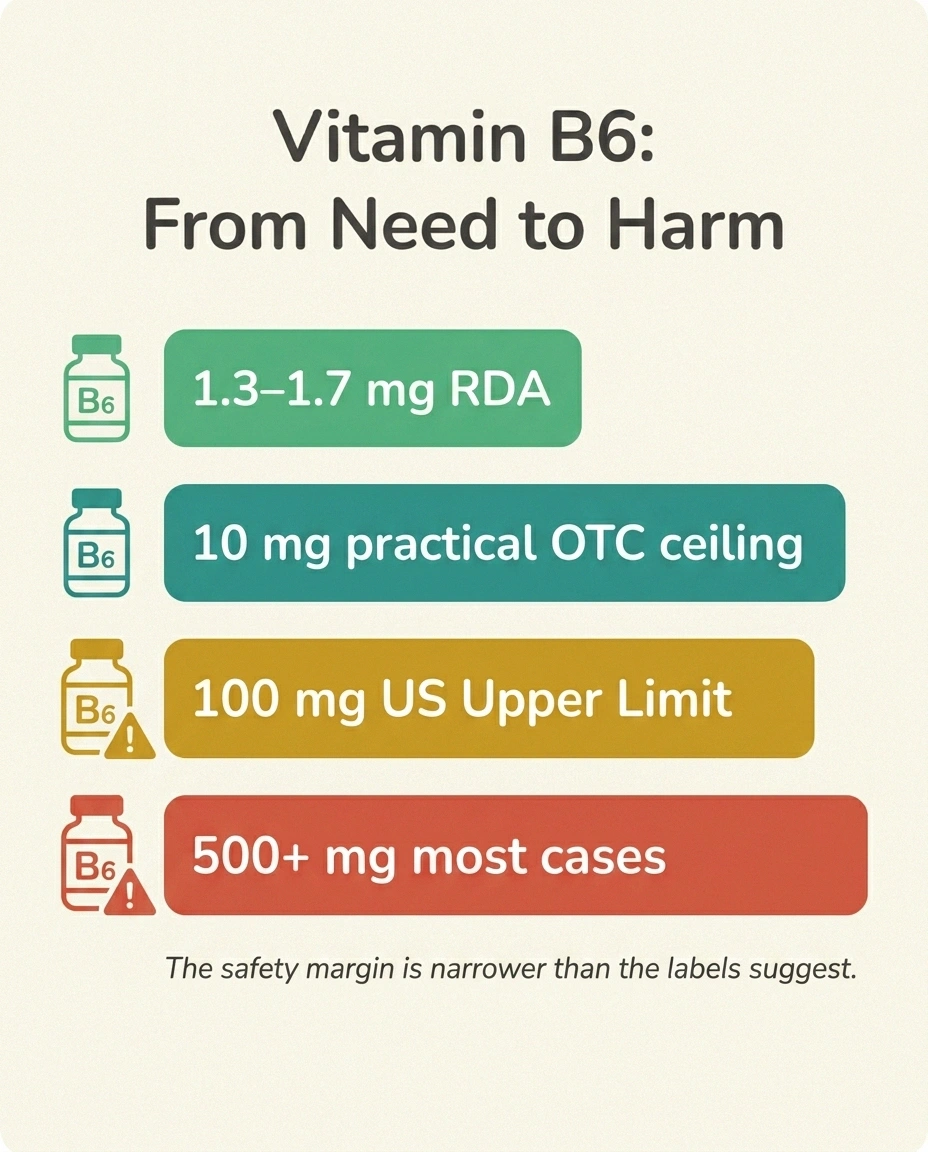
Vitamin B6 is one of the few vitamins where too much causes the same nerve damage it is supposed to prevent. The practical safe ceiling for long-term over-the-counter use is closer to 10 mg per day than the 100 mg upper limit most product labels reference — especially for anyone already living with neuropathy.
But here is the counterintuitive part: B6 is one of the few vitamins where too much can cause the same nerve damage it is supposed to prevent. The dose-response curve is not flat at the top. There is a window where B6 supports nerves, and there is a window above it where B6 quietly poisons the sensory ganglia where nerve signals originate. Almost no other water-soluble vitamin behaves this way. It is what makes B6 toxicity easy to miss — and why even thoughtful people can stumble into it.
What B6 Toxicity Neuropathy Actually Looks Like

The clinical picture of pyridoxine-induced neuropathy is fairly specific, and recognizing the pattern is the first step toward catching it. The condition is technically called a “sensory neuronopathy” or “sensory ganglionopathy,” because the damage is to the cell bodies of sensory nerves (the dorsal root ganglia, just outside the spinal cord), not to the long peripheral axons themselves. This matters for two reasons. First, it produces a particular set of symptoms. Second, it is a different kind of damage from most other neuropathies, and the recovery pattern reflects that.
The Pyridoxine Toxicity Pattern
Typical symptoms:
- Tingling, numbness, or burning sensations, usually starting in the feet but sometimes also in the hands
- A sense of unsteadiness, especially in the dark or with eyes closed — this is “sensory ataxia,” and it happens because you have lost some of the position sense your brain normally uses to know where your feet are. Our guide to proprioception loss in neuropathy covers this specific kind of balance problem in more depth.
- Difficulty with fine motor tasks like buttoning shirts, when sensory feedback from fingertips is impaired
- Loss of the Achilles reflex on neurological examination
- Pain that has a “deep” or “shooting” quality in some people
- Motor strength is usually preserved — this is a clue, because most other neuropathies eventually affect motor function too
The symptoms often creep in slowly enough that people attribute them to “getting older,” to their existing neuropathy worsening, or to a new condition altogether. The fact that they coincided with starting a supplement does not always register.
The Dose Question Everyone Asks
“How much B6 is too much” is the question I get most. The honest answer is that the threshold is variable, and the regulatory recommendations have been tightening as more cases get reported. Here is what we know:
B6 Dose Thresholds at a Glance
- The US Recommended Dietary Allowance is 1.3 to 1.7 mg per day. You can get this from food without supplementing at all.
- The Institute of Medicine's Tolerable Upper Intake Level is 100 mg per day. This was set in 1998 as a level below which sensory neuropathy was not expected. It is the number most product labels still reference.
- Case literature documents neuropathy at doses well below 100 mg per day, particularly with prolonged use. Reports exist of symptomatic toxicity at 50 mg, at 25 mg, even at 10 mg per day in some individuals. There are isolated case reports describing toxicity at as little as 6 mg per day from chronic multivitamin use in genetically susceptible people.
- Most clear-cut cases occur at doses above 500 mg per day taken for months, but the safety margin is much narrower than the 100 mg upper limit suggests.
- Regulators have responded. Australia's Therapeutic Goods Administration in 2022 required warning labels on any product containing more than 10 mg per day of B6. New Zealand and Singapore followed with similar guidance. The UK MHRA tightened recommendations in 2024. The trend is unmistakable: the practical safe ceiling for over-the-counter B6 is much closer to 10 mg per day than to 100 mg per day, especially with daily long-term use.
The variation between individuals is real. Some people take 200 mg daily for years and have no symptoms. Others take 50 mg for six months and develop them. We do not yet have a reliable way to predict who falls where, which is why “stay near the bottom of the dose range” is the right default for anyone supplementing without a specific medical reason.
Where the B6 Is Hiding

This is the part that catches people. They look at their “neuropathy supplement” bottle and see 25 mg of B6, which sounds modest. What they do not realize is that they are also taking:
A single “B6 supplement” is rarely the whole picture. Add up every source:
- B-complex (often 25-100 mg per dose)
- Multivitamins and “energy” formulas
- “Nerve support” supplements (often the highest)
- Hair-skin-nails products
- Magnesium-plus-B blends
- Pre-workout drinks and fortified shakes
- Some prenatal vitamins
- A B-complex with 50 mg
- An “energy” multivitamin with 20 mg
- A “nerve support” formula with 100 mg (this category often runs very high)
- A magnesium-plus-B formula with 10 mg
- A hair-skin-nails product with 15 mg
- A pre-workout drink with 5 mg per serving
- A fortified breakfast drink or shake with 2-3 mg
Add those up and a person can easily be taking 200 mg per day without ever opening a “B6 supplement” bottle. This is the most common pattern I see in my reading and in our group: the toxicity comes not from one big dose but from many small overlapping doses.
Particularly worth flagging: many products marketed for “nerve support” or “energy and stamina” contain high-dose B6 — sometimes 100 to 200 mg per dose. The supplements industry has known about the neuropathy risk for decades, and many manufacturers have voluntarily lowered their doses, but the regulatory ceiling in the US is still loose enough that high-dose products remain on shelves. Read every label. If you have ever been told that you have neuropathy or that you are at risk for it, the hidden B6 in your supplement drawer deserves an honest audit. Our guide to the best supplements for nerve health is built around this exact safety principle — useful doses, not heroic ones.
Why This Specific Vitamin and Not the Others
You might wonder why B6 is the troublemaker when B1 (thiamine), B12 (cobalamin), and folate are happily prescribed in doses many times the RDA for various nerve conditions. The current best understanding is that pyridoxine — the most common supplemental form of B6 — accumulates in the dorsal root ganglion cells when intake outpaces the body's ability to convert it to the active PLP form. The unphosphorylated pyridoxine appears to displace the active form at the same enzymatic sites, disrupting the very metabolic pathways B6 is supposed to support. The sensory neurons of the dorsal root ganglion are unusually exposed to circulating compounds because the blood-nerve barrier is weak in that location — and that is exactly where the damage shows up. Our guide to the blood-nerve barrier in neuropathy explains why certain neurons are more vulnerable to circulating toxins than others.
Australia's TGA (2022), New Zealand's Medsafe (2025), and Singapore's HSA have all issued safety guidance requiring warnings or limits on supplements above 10 mg per day of B6. The regulatory direction is unmistakable: the practical safe ceiling for over-the-counter B6 is much closer to 10 mg per day than to the older 100 mg upper limit.
This dorsal-root-ganglion specificity is also why the damage pattern is “sensory only” — motor neurons are protected differently. It is why classic pyridoxine neuropathy looks the same regardless of the underlying reason for over-supplementation.
Active Forms vs Pyridoxine
A reasonable next question: is the active form (pyridoxal-5-phosphate, or PLP, also sold as P-5-P) safer than plain pyridoxine? The short, honest answer is that there is less case literature on P-5-P toxicity, but the absence of evidence is not the same as evidence of safety. Most experts treat P-5-P with the same caution as pyridoxine at the same milligram dose, in part because no one has done the careful comparison studies that would justify higher dosing. Until that data exists, “active form” should not be treated as a free pass to higher amounts.
If you have a specific medical condition that requires a particular B6 form — certain inborn errors of metabolism, for example — that decision belongs with a specialist who can weigh the trade-offs in your specific case. For garden-variety supplement use, the dose ceiling is essentially the same whether you choose pyridoxine or P-5-P.
Who Is Most at Risk
Anyone can develop B6 toxicity at high enough doses, but a few groups appear to be more vulnerable:
Existing neuropathy (any cause) · older adults · reduced kidney function · long-duration daily use · medications affecting B6 metabolism (isoniazid, penicillamine, certain anti-epileptics) · genetic differences in vitamin metabolism.
For anyone in these groups: conservative ceiling ~10 mg/day from all supplemental sources combined.
- People who already have neuropathy from another cause. A nerve that is already stressed is more vulnerable to additional insults. This is the same “double crush” idea that comes up in many other contexts. If you already have diabetic, chemotherapy-related, idiopathic, or any other neuropathy, the B6 ceiling for you is lower than for the general population.
- Older adults. Kidney clearance of pyridoxine decreases with age, so the same dose produces higher and longer-lasting blood levels.
- People with reduced kidney function for the same reason.
- People on long-term supplementation regardless of dose. Time at exposure matters as much as the daily amount. A modest dose taken every day for ten years is not the same as the same modest dose taken occasionally.
- People taking medications that affect B6 metabolism, including isoniazid (for tuberculosis), penicillamine, hydralazine, and certain anti-epileptic drugs. These interactions cut in both directions — sometimes increasing risk of deficiency, sometimes affecting how B6 accumulates.
- People with genetic differences in vitamin metabolism that we are only beginning to understand. This is why some case reports describe toxicity at startlingly low doses.
How the Diagnosis Gets Made
If your clinician suspects pyridoxine toxicity, the workup is fairly straightforward, but it requires that someone raise the question in the first place — which is the hard part. The basic elements:
- A careful supplement and medication history covering every bottle you take and have taken, going back at least a year or two. Bring everything to the appointment. This is the single most important step, because the diagnosis hinges on the exposure history matching the clinical pattern.
- Blood pyridoxal-5-phosphate (PLP) level. An elevated PLP supports the diagnosis but a normal level does not rule it out, because levels can normalize after a supplement is stopped while symptoms persist. The test is most useful when drawn while the person is still actively supplementing.
- EMG and nerve conduction study (electromyography). The classic pattern is reduced or absent sensory nerve action potentials with preserved motor function. Our guide to reading EMG and nerve conduction results walks through what these reports actually say.
- Skin biopsy for small-fiber assessment in some cases, particularly when the symptoms are predominantly burning rather than numbness.
- Exclusion of other causes, because pyridoxine toxicity sits within the broader differential of sensory neuropathies — diabetes, B12 deficiency, paraneoplastic syndromes, toxic exposures, and autoimmune conditions among them. Our guide to how neuropathy gets diagnosed covers this broader workup.
The diagnosis is ultimately a clinical one. It requires a clinician who has heard of this entity, a patient who has brought the supplement bottles in, and the conviction to take a B6 history seriously even when nothing looks dramatic.
What Happens When You Stop

The first thing to do, if pyridoxine toxicity is suspected, is to stop all supplemental B6 entirely. Not “cut back” — stop. This includes the obvious B-complex and B6 single supplements, but also the multivitamins, the energy formulas, the prenatal vitamins, the “nerve support” products, and the fortified shakes that are quietly contributing. You may need to live with food-only B6 (which is more than adequate for normal nutrition) for many months while the body clears the excess and the affected neurons recover.
After You Stop — What Recovery Usually Looks Like
What to expect from recovery:
- Most cases improve over weeks to many months after the supplement is stopped. Some symptoms may continue to worsen for the first few weeks even after stopping (a phenomenon called “coasting”) before stabilizing and then improving. This is dispiriting if you are not expecting it, but it is documented.
- Recovery is often incomplete. Many people are left with some residual sensory loss or imbalance, particularly if exposure was prolonged or severe. The body can repair the dorsal root ganglion cells to a degree, but very damaged neurons can be permanently lost.
- Severity matters. Cases caught early with shorter exposure tend to recover more completely. Cases caught after years of high-dose supplementation tend to leave more residual symptoms.
- The full recovery timeline can be six to twelve months or longer. Patience is genuinely required here. If you are improving at three months, the trajectory is good even if you are not “back to normal” yet.
During recovery, the same supportive care that helps any sensory neuropathy is reasonable: gentle exercise (especially balance work to compensate for sensory loss), supportive footwear, fall prevention, and symptomatic medications for pain if needed. None of these speed up nerve healing, but they help you live with the symptoms while it happens. Our guide to neuropathy balance and fall prevention is particularly relevant when sensory ataxia is part of the picture.
The Specific Case of “I Was Taking This for My Neuropathy”

The bitter irony of this condition is that many people develop it from products marketed to help nerve pain. They have neuropathy from some other cause — diabetes, chemotherapy, an autoimmune condition, idiopathic — they want something that might help, they pick up a “nerve support” supplement at the pharmacy or online, and the supplement is loaded with B6 well above safe daily intake.
If you have an underlying neuropathy and you are taking a nerve-support supplement, please do this:
- Look at the label. Find the B6 (pyridoxine, pyridoxine HCl, P-5-P, or pyridoxal-5-phosphate) line.
- Add up all your other sources of B6 from every other supplement and fortified food you take.
- If your total is more than 10 to 25 mg per day, talk with your clinician about whether your symptoms could be made worse by what you are taking, not better.
- Consider whether the supplements with evidence behind them for nerve health — alpha-lipoic acid, benfotiamine (a fat-soluble B1 form, different from B6), acetyl-L-carnitine, and properly-dosed B12 — might serve you better than a high-B6 multi-formula.
None of this means B6 is bad. It means the dose discipline matters more for B6 than for almost any other water-soluble vitamin.
What “Safe” Looks Like in Practice

For most adults with no specific medical reason to take high-dose B6, the safe practical guidance is:
- Get most of your B6 from food. Poultry, fish, chickpeas, potatoes, bananas, fortified cereals — a regular diet easily exceeds the 1.3-1.7 mg RDA.
- If you take a multivitamin, look for one with B6 in the range of 1 to 5 mg, not 25 mg or 50 mg.
- If you take a B-complex, prefer one in the 5 to 10 mg range; the very-high-dose B-complexes (50 or 100 mg of each B vitamin) are mostly marketing.
- If you take a “nerve support” or “energy” formula, audit the B6 content; if it is over 25 mg per day and you are taking it daily, ask whether the dose is justified.
- If you have any clinical neuropathy or are at risk for one (diabetes, chemo, autoimmune disease, family history), set your personal ceiling at 10 mg per day from all supplemental sources combined, unless a clinician has a specific reason to prescribe more.
These are not regulatory thresholds — they are practical floors-and-ceilings drawn from the patient-safety literature. Reasonable clinicians will disagree on exact numbers. The principle is what matters: B6 has a narrower therapeutic window than the bottle labels suggest, and the responsible default is to keep daily total intake conservative.
The Conversation to Have With Your Doctor
If you suspect B6 is contributing to your symptoms, the conversation is more productive when you bring specifics:
- A list of every supplement, multivitamin, fortified drink, and protein powder you take, with the B6 milligrams from each label
- The total daily B6 intake added up
- A timeline of when each supplement started relative to when symptoms began
- A clear description of the symptoms — particularly any sensory ataxia, balance problems in the dark, or the burning/tingling pattern
This is one of those medical situations where the diagnosis often hinges on the patient noticing the connection first and bringing it to the clinician's attention. Not because clinicians are inattentive — but because B6 is so quietly woven into so many products that the supplement history is genuinely hard to take in a brief visit unless the patient has done the inventory at home.
Frequently Asked Questions
How much vitamin B6 is too much in a day?
The US Tolerable Upper Intake Level is 100 mg per day, but case literature documents neuropathy below that ceiling, particularly with prolonged daily use. Several international regulators have tightened guidance toward a 10 mg per day practical ceiling for over-the-counter products. For someone who already has neuropathy or is at risk for one, keeping total daily supplemental B6 under 10 mg is the conservative position. The body's daily need from food is only 1.3 to 1.7 mg.
Is vitamin B6 toxicity reversible?
Partially or fully reversible in many cases if the supplement is stopped early, but recovery often takes six to twelve months and may be incomplete. Symptoms can briefly worsen in the first weeks after stopping (called “coasting”) before stabilizing and improving. Severe or long-duration toxicity can leave permanent residual sensory loss, which is why catching it early matters.
Can B6 from food cause neuropathy?
No. Food sources of B6 cannot deliver doses high enough to cause toxicity. A normal mixed diet provides several milligrams per day, well within safe range. Toxicity is essentially always a supplement or fortification phenomenon, not a food phenomenon.
What does B6 toxicity feel like?
Most commonly: tingling, burning, or numbness in the feet and sometimes hands; unsteadiness or balance trouble, especially in the dark or with eyes closed; difficulty with fine motor tasks like buttoning shirts; loss of the ankle reflex on examination. Motor strength is typically preserved. The pattern is “sensory only,” and it usually develops gradually over weeks to months.
Is pyridoxal-5-phosphate (P-5-P) safer than regular B6?
There is less case literature on P-5-P toxicity, but the absence of reports is not strong evidence of safety. Most clinicians treat P-5-P with the same caution as pyridoxine at the same milligram dose. Until comparative safety data exists, the active form should not be assumed to allow higher dosing.
Should I stop my B-complex right now?
If you have neuropathy symptoms and you are taking a B-complex containing more than 10 mg of B6 (or you are stacking multiple supplements that add up to that), it is reasonable to stop the B6-containing products and discuss with your clinician. If you have no symptoms and your daily total is conservative, you can continue. Bring all your supplement bottles to your next appointment for a real audit.
How long after stopping B6 will my symptoms improve?
Improvement usually begins within weeks to a few months of stopping, but the full recovery can take six to twelve months or longer. Some people experience a brief worsening in the first few weeks before stabilizing — this is called “coasting” and is documented in the literature. Patience is genuinely required.
What B6 dose is safe for someone with diabetic neuropathy?
For someone who already has any clinical neuropathy, the conservative ceiling is about 10 mg per day of total supplemental B6 unless a clinician has a specific reason to prescribe more. The principle is that a nerve already damaged by one cause is more vulnerable to a second insult — and pyridoxine, paradoxically, can be the second insult.


