The word “surgery” tends to stop people cold. For many of us managing neuropathy, it's not something we've ever seriously entertained — we're focused on medications, supplements, lifestyle changes. Surgery feels like a last resort, something drastic, something to avoid.
But for a specific group of neuropathy patients, nerve decompression surgery isn't a last resort. It's the most direct path to real relief. And for some, it's the only thing that has actually worked.
The key word in that sentence is “specific.” Nerve decompression surgery doesn't help all types of neuropathy — not even close. It's designed to address a particular problem: a nerve that is being physically compressed, entrapped, or pinched by surrounding tissue. When that's what's happening, releasing that pressure can be remarkably effective. When it's not, surgery has nothing to offer.
This guide will walk you through exactly what nerve decompression surgery is, which conditions it's designed for, what the research shows, and — most importantly — how to figure out whether you're a candidate.
What Is Nerve Decompression Surgery?
Nerve decompression surgery is a procedure that releases a nerve that's being compressed, pinched, or constricted by surrounding structures — bone, muscle, tendon, fibrous tissue, or scar tissue. By releasing that constriction, the surgery removes the mechanical source of nerve damage and allows the nerve the space it needs to function normally and, ideally, begin recovering.
Key Takeaway
Nerve decompression surgery works best for entrapment neuropathies — conditions where a nerve is physically pinched at a specific location. It is not a treatment for diffuse polyneuropathy. Getting the correct diagnosis first is the essential first step.
The surgery itself varies in complexity depending on which nerve is involved and where the compression is happening. At the simpler end, carpal tunnel release is a common outpatient procedure that takes 15–30 minutes. More complex procedures — like triple-nerve decompression in the leg for diabetic neuropathy patients — involve multiple sites and longer operating time.
What these surgeries share is their underlying mechanism: they're removing physical obstruction to give a nerve room to breathe.
Conditions That Respond Well to Decompression
The clearest candidates for nerve decompression surgery are the classic entrapment neuropathies — conditions where a nerve is physically trapped at a specific anatomical location.
Common Nerve Entrapments and Their Surgical Procedures
| Condition | Nerve Affected | Procedure | Evidence |
|---|---|---|---|
| Carpal tunnel syndrome | Median nerve (wrist) | Carpal tunnel release | Strong |
| Cubital tunnel syndrome | Ulnar nerve (elbow) | Cubital tunnel release / transposition | Strong |
| Tarsal tunnel syndrome | Posterior tibial nerve (ankle) | Tarsal tunnel release | Moderate |
| Peroneal nerve compression | Peroneal nerve (knee) | Peroneal nerve decompression | Moderate |
| Meralgia paresthetica | Lateral femoral cutaneous (groin) | Inguinal ligament release | Moderate |
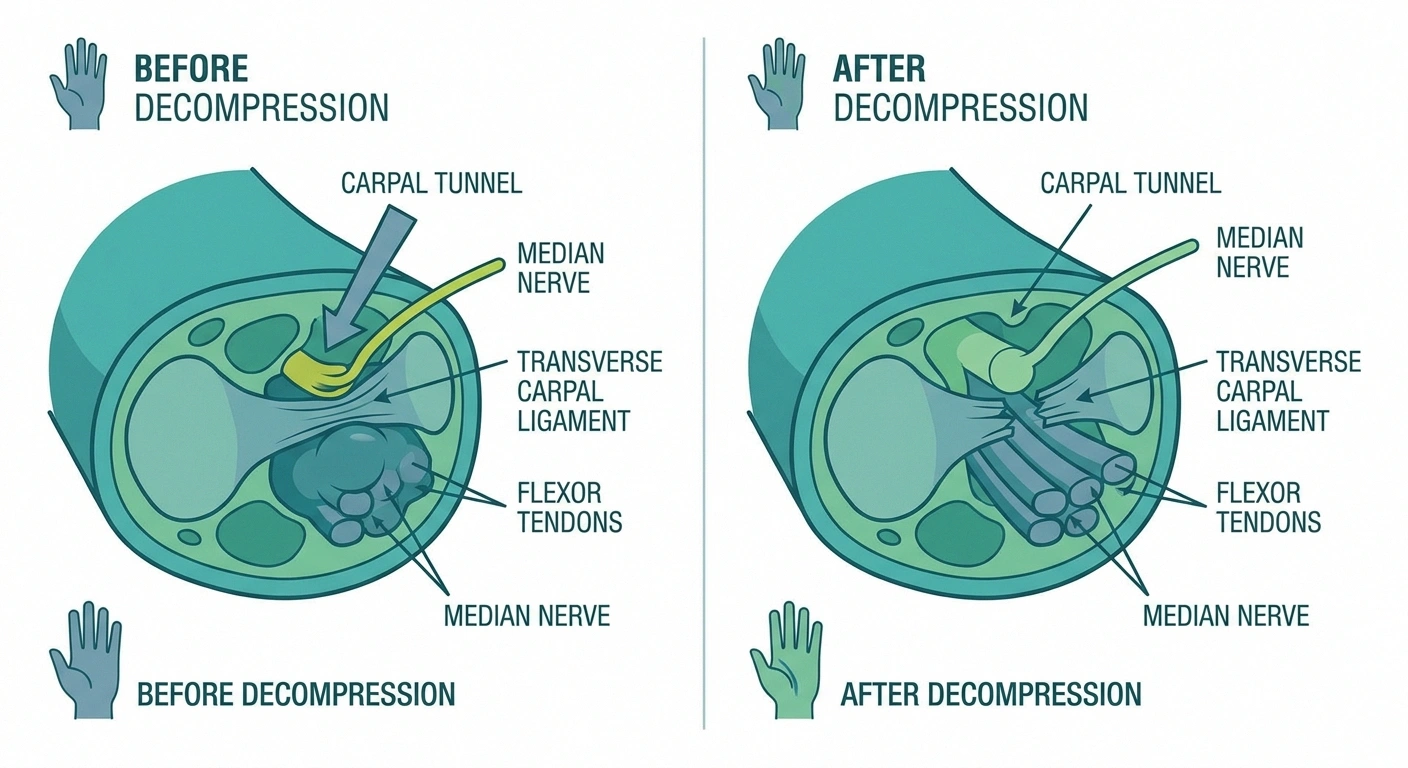
Carpal Tunnel Syndrome
The most widely performed nerve decompression procedure in the world. In carpal tunnel syndrome, the median nerve becomes compressed as it passes through the narrow carpal tunnel in the wrist. Symptoms include tingling, numbness, and pain in the thumb, index, and middle fingers — often worse at night. Carpal tunnel release surgery cuts the transverse carpal ligament to open the tunnel and relieve pressure on the nerve. Success rates are very high, and most patients experience significant relief within weeks.
Cubital Tunnel Syndrome (Ulnar Nerve Compression)
The ulnar nerve — the one responsible for the sharp jolt when you hit your “funny bone” — passes through a narrow channel on the inside of the elbow. When it becomes chronically compressed there, it causes numbness and tingling in the ring and little fingers, weakness in the hand, and difficulty with fine motor tasks. Our article on ulnar neuropathy covers the symptoms in detail. Surgery can release or reposition the nerve with good outcomes in most cases.
Tarsal Tunnel Syndrome
Less well-known but significant for neuropathy patients: the posterior tibial nerve passes through a narrow channel behind the inner ankle (the tarsal tunnel). Compression here causes burning, tingling, and pain in the sole of the foot — symptoms that can closely mimic peripheral neuropathy. Tarsal tunnel release surgery opens that channel and often produces dramatic improvement in foot pain, particularly in patients where conservative treatment has failed.
Peroneal Nerve Compression
The peroneal nerve wraps around the outside of the knee and is vulnerable to compression there. Compression can cause foot drop — difficulty lifting the front of the foot — along with weakness and numbness along the outside of the lower leg and the top of the foot. As we explored in our guide to peroneal neuropathy and foot drop, decompression surgery can restore significant function when performed before permanent nerve damage has occurred.
Meralgia Paresthetica
This condition involves compression of the lateral femoral cutaneous nerve where it passes under or through the inguinal ligament in the groin. It causes burning, tingling, and numbness on the outer thigh. While often managed conservatively, decompression surgery is an effective option when symptoms are severe or persistent.
The Controversial Case: Diabetic Peripheral Neuropathy
Here is where the conversation gets complicated — and where you need to hear both sides.
A subset of surgeons — primarily peripheral nerve surgeons and plastic surgeons with nerve expertise — argue that many patients with diabetic neuropathy also have superimposed nerve entrapments at common anatomical choke points in the leg and foot. They propose that releasing these entrapments can significantly reduce pain and improve sensation, even in patients with established diabetic neuropathy.
The procedure most associated with this argument is the “Dellon triple decompression” — simultaneous release of three nerves in the lower leg (the common peroneal, the deep peroneal, and the posterior tibial nerve at the tarsal tunnel). Proponents report significant pain reduction and improved sensation in selected patients.
However, mainstream neurology is skeptical. The American Academy of Neurology has noted that the evidence base for this procedure in diabetic neuropathy remains insufficient for broad recommendation. Critics point out that the randomized controlled trial data is limited, and that patient selection is critical — not all diabetic neuropathy patients have meaningful entrapment components.
What does this mean practically? If you have diabetic neuropathy and are considering this type of surgery, you need a careful evaluation by a qualified peripheral nerve surgeon, a thorough discussion of the evidence, and ideally a second opinion from a neurologist. It's not that the surgery is wrong for everyone — it's that identifying the right candidates requires expertise and honest assessment.
How Is Entrapment Diagnosed?
The most important test for identifying nerve entrapment is an EMG and nerve conduction study (NCS). This test measures how quickly and effectively nerve signals travel through specific segments of the nerve. A significant slowing at a particular anatomical location — like the wrist, the elbow, or the ankle — is strong evidence of entrapment at that site.

If you've had a nerve conduction study that showed normal results throughout, pure entrapment is less likely. If the study showed localized slowing at a specific site, that's meaningful information pointing toward a potential surgical target.
Additional diagnostic tools may include:
- MRI or ultrasound — can visualize structural compression, scar tissue, or anatomical abnormalities at the entrapment site
- Diagnostic nerve block — injecting local anesthetic at the suspected entrapment site; if it temporarily relieves your symptoms, it supports entrapment as the cause
- Physical examination — a Tinel's sign (tapping on the nerve produces tingling in the distribution) at a specific site suggests entrapment
Getting a thorough neuropathy diagnosis that identifies where and how the nerve is being affected is absolutely foundational before surgery is considered.
Who Is — and Isn't — a Good Surgical Candidate?
Good candidates for nerve decompression surgery typically share these characteristics:
Am I a Good Surgical Candidate? A Quick Self-Check
- Confirmed nerve entrapment at a specific anatomical site on EMG/NCS
- Symptoms consistent with the known distribution of that nerve
- Some remaining nerve function (not complete nerve death at the site)
- Failure of conservative treatment (rest, splinting, physical therapy, anti-inflammatory medications)
- Symptoms that meaningfully limit daily function or quality of life
Surgery is generally not indicated for:
- Diffuse polyneuropathy with no evidence of focal entrapment
- Cases where the nerve has been completely non-functional for too long (nerve tissue has atrophied beyond recovery)
- Patients whose symptoms are primarily from the underlying disease process rather than mechanical compression
- Patients who haven't yet tried appropriate conservative management
The Critical Role of Timing
One of the most important things peripheral nerve surgeons emphasize: timing matters enormously.
⚠ Time-Sensitive
For motor nerve compression causing weakness, the window for successful surgery is typically 9–12 months from onset. After that, motor nerve fibers may have degenerated beyond recovery. If you have progressive weakness that could be entrapment-related, do not wait — get evaluated now.
When nerve compression causes motor weakness — difficulty moving a muscle — the window for surgical success is typically within 9 to 12 months of onset. Beyond that, the nerve's motor axons may have degenerated to a point where even releasing the compression cannot restore function. The nerve cells that control muscle movement have a much more limited capacity for long-distance regeneration than sensory fibers.
For sensory symptoms — numbness, tingling, pain — the timeline is generally more forgiving, because sensory nerve regeneration is somewhat more robust. But waiting years is still not in your favor.
If you have progressive weakness that might be related to nerve entrapment, don't sit on it. Get evaluated. The difference between acting quickly and waiting could be the difference between recovering function and losing it permanently.
What the Recovery Process Looks Like
After nerve decompression surgery, recovery is not immediate — and understanding why helps set realistic expectations.

1 inch/month
The rate at which peripheral nerves regenerate after decompression — expect months, not weeks, for full recovery
Nerves regenerate slowly. The peripheral nervous system is capable of regeneration (unlike the central nervous system), but nerves grow back at approximately one inch per month. So a nerve that was compressed at the wrist and needs to regenerate back down into the fingers is going to take months, not weeks, to fully recover.
Typical recovery milestones:
- Days 1–2: Incision soreness, swelling; the procedure is typically outpatient for simple releases
- Weeks 2–6: Wound healing; light activity resumes; some people notice early improvement in pain or sensation
- Months 2–4: Nerve function gradually improving; tingling may increase temporarily as nerves “wake up”
- Months 4–12: Continued gradual recovery; strength and sensation improvements continue
- Year 1+: Final outcome assessment; nerve regeneration largely complete by 12–18 months
Physical therapy is often recommended post-surgery to help restore strength and function as nerve recovery progresses. Don't skip it — the surgery removes the obstacle, but therapy helps you rebuild what was lost.
Finding the Right Surgeon
This is genuinely important. Not all surgeons who operate on nerves have the same depth of expertise. For peripheral nerve decompression, the most qualified specialists are typically:

Research Says
Carpal tunnel release has one of the highest success rates in elective surgery — approximately 80–90% of properly selected patients experience significant symptom relief. Patient selection quality is the single biggest predictor of outcome.
- Peripheral nerve surgeons — a subspecialty that may be based in plastic surgery, orthopedic surgery, or neurosurgery. These surgeons focus specifically on nerves and have the most experience with decompression procedures across multiple sites.
- Hand surgeons — for upper extremity entrapments (carpal tunnel, cubital tunnel), an experienced hand surgeon is highly qualified.
- Orthopedic or neurosurgeons — for specific procedures; expertise varies widely.
When evaluating a surgeon, ask specifically about their experience with your particular procedure, their complication rates, and what percentage of their patients achieve meaningful improvement. A surgeon who gives you confident numbers and specific data inspires more confidence than one who speaks in vague generalities.
If you're uncertain, knowing when to see a specialist and getting a second opinion before committing to surgery is always a reasonable step.
Frequently Asked Questions

Will insurance cover nerve decompression surgery?
For established entrapment neuropathies like carpal tunnel syndrome with documented EMG evidence, insurance coverage is generally straightforward. For less common procedures or for off-label indications like the Dellon triple decompression for diabetic neuropathy, coverage may require prior authorization and thorough documentation of medical necessity. Check with your insurer and surgeon's billing office before proceeding.
What is the success rate of nerve decompression surgery?
Success rates vary considerably by procedure, patient selection, and how “success” is defined. Carpal tunnel release has excellent outcomes — most studies report 80–90% of patients experiencing significant symptom improvement. Less common procedures have more variable data. The quality of patient selection (i.e., how well the surgeon identifies appropriate candidates) is one of the biggest determinants of outcome.
Can nerve decompression surgery make neuropathy worse?
Any surgery carries risk. Nerve surgery risks include incomplete relief, infection, scar tissue formation, and in rare cases, worsening symptoms from surgical trauma. These risks are reduced when surgery is performed by an experienced peripheral nerve surgeon and when the candidate selection is appropriate. Poorly selected candidates — people whose symptoms aren't actually from entrapment — are unlikely to benefit and may experience frustration rather than improvement.
My EMG was normal. Does that rule out surgery?
Not necessarily, but it shifts the picture significantly. A normal nerve conduction study makes classic entrapment neuropathy less likely. However, some forms of nerve compression, particularly early-stage or small-fiber-predominant cases, may not show clearly on standard EMG. This is a nuanced conversation to have with a peripheral nerve specialist who can evaluate your clinical picture comprehensively, not just the test results in isolation.
Is nerve decompression surgery the same as nerve repair?
No. Nerve decompression releases external compression on a structurally intact nerve. Nerve repair involves suturing together a severed or severely damaged nerve. They're related but distinct procedures. Decompression is appropriate when the nerve is being compressed from outside; repair is appropriate when the nerve itself has been physically disrupted.
How do I know if my neuropathy is entrapment versus systemic?
Entrapment neuropathy typically causes symptoms in a specific nerve distribution — for example, tingling in the thumb and first two fingers (median nerve) rather than diffuse tingling in all toes. It often has identifiable triggers (symptoms worsen with specific positions or activities), and nerve conduction studies show localized slowing at the entrapment site. Systemic polyneuropathy tends to be more diffuse, length-dependent (worse in feet than hands), and without a single focal compression site. A neuromuscular specialist can usually distinguish between the two.
Is physical therapy enough, or do I need surgery?
For mild to moderate entrapment, physical therapy, activity modification, and splinting may be sufficient to control symptoms without surgery. Surgery is generally reserved for cases where conservative management has failed, symptoms are severe or significantly impairing function, or there's evidence of progressive nerve damage. The sequence typically goes: conservative treatment first, then reassess, and consider surgery only if indicated and conservative approaches have been given adequate time.