If you've been managing diabetic neuropathy pain for any length of time, you've probably noticed something frustrating: the list of medications doctors prescribe hasn't really changed in a long time. Gabapentin. Pregabalin (Lyrica). Duloxetine (Cymbalta). The occasional opioid as a last resort. Most of these were approved or repurposed for nerve pain more than 20 years ago. For people who don't respond well — or who can't tolerate the side effects — there hasn't been a brand-new oral option in a generation.
That's why an investigational drug called pilavapadin (also known by its development code LX9211) has been showing up in headlines this year. In early 2025, its maker — Lexicon Pharmaceuticals — released the topline results from a Phase 2b trial called PROGRESS. The headline: a once-daily, oral, non-opioid pill significantly reduced diabetic nerve pain compared to placebo. By early 2026, Lexicon announced that the FDA had cleared the path forward, and two Phase 3 registrational trials are now being prepared.
I want to walk you through what pilavapadin actually is, what the research has shown so far, what it might mean for people living with diabetic peripheral neuropathy — and the important caveats every patient should know before getting their hopes up. Investigational means investigational. It is not approved, you can't get a prescription for it today, and there are real unknowns. But it's the most interesting oral neuropathy drug to enter late-stage development in a long time, and that's worth understanding.
What Pilavapadin Is — In Plain Language
Pilavapadin is a small-molecule oral drug being developed by Lexicon Pharmaceuticals for painful diabetic peripheral neuropathy (DPN). Three things about it stand out:
- It's a pill, taken once a day. No injections, no infusions, no implanted device.
- It works on a target no approved drug currently uses. The mechanism is novel — more on that below.
- It is not an opioid. No euphoria, no respiratory depression risk, no expected dependence — at least based on what's been observed in clinical studies so far.
If it makes it through Phase 3 and gets approved, pilavapadin would be the first new oral non-opioid drug class for neuropathic pain in over two decades. That's the genuine reason researchers, patients, and patient advocates are paying attention. Whether it actually crosses that finish line is still an open question. Phase 3 trials sometimes confirm Phase 2 results, and sometimes they don't.
The Mechanism — What “AAK1 Inhibitor” Actually Means
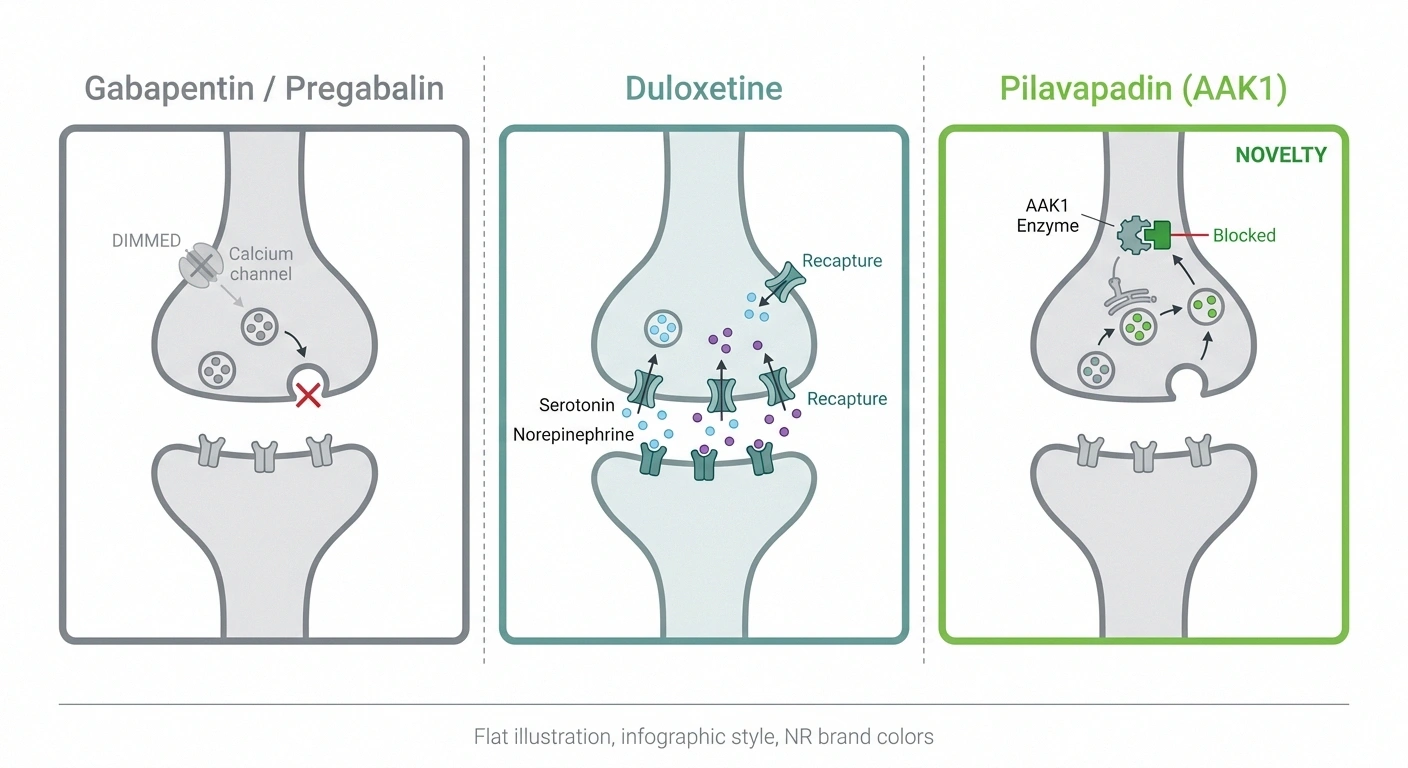
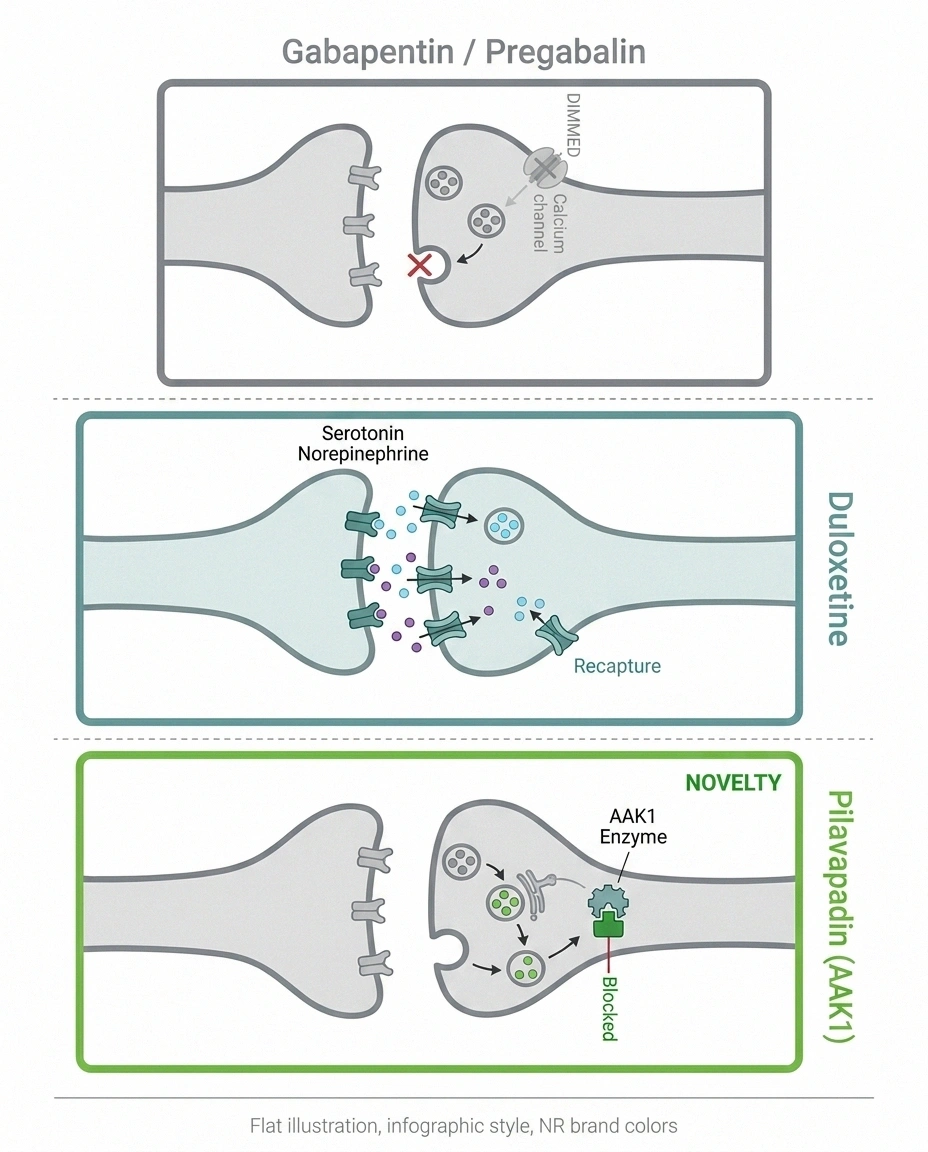
I always try to translate the jargon, so here it is. Pilavapadin blocks an enzyme called AAK1, which stands for “adaptor-associated kinase 1.” AAK1 is found inside nerve cells and helps regulate how pain signals are processed in the central nervous system. Researchers noticed years ago that when AAK1 is reduced or inhibited, animals show less pain-related behavior — without the sedation, addiction, or breathing problems that come with opioids.
Think of it this way: most neuropathic pain medications either dampen overall nerve excitability (gabapentin and pregabalin work this way) or adjust pain-modulating brain chemicals like serotonin and norepinephrine (duloxetine and the older tricyclics). Pilavapadin works through a different doorway entirely — one that hasn't been used by any approved drug.
That's exciting because a different mechanism means it could potentially help people who don't respond to current medications. It also means we genuinely don't know yet how it will perform across diverse patients in larger, longer trials. New mechanisms are double-edged: they're the source of breakthroughs, and they're also where unexpected long-term issues sometimes show up that smaller trials can't catch.
What the Phase 2b PROGRESS Study Actually Showed

This is the trial that brought pilavapadin into the headlines. Here's what happened, in plain numbers.
The PROGRESS study enrolled adults with painful diabetic peripheral neuropathy and randomized them to one of three groups: 10 mg of pilavapadin once daily, 20 mg once daily, or a placebo pill. Patients tracked their pain on a standard 11-point pain scale (0 = no pain, 10 = worst pain imaginable). The primary measure was the change in their average daily pain score over the treatment period.
The 10 mg group saw their pain scores drop by an average of about 1.74 points. The placebo group saw their pain drop by about 1.31 points. That difference — roughly 0.43 points — was statistically significant on the primary endpoint, meaning it was unlikely to be due to chance.
Some readers will look at that and say: “Less than half a point on a 10-point scale? That's it?” It's a fair reaction. Here's the honest context:
- Most approved nerve pain medications show modest effect sizes in trials. Pregabalin, duloxetine, gabapentin — they all show absolute pain reductions of about half a point to a full point above placebo in well-designed studies. Pilavapadin's PROGRESS result sits squarely in that range, which is partly why the FDA accepted the data as a basis for advancing to Phase 3.
- The placebo response in pain trials is large. The PROGRESS placebo group dropped 1.31 points — that's not nothing. Pain is heavily influenced by expectation, attention, and the structure of the trial itself. A drug effect needs to clear that placebo bar.
- Group averages hide individual variation. Within the 10 mg group, some patients had little response, while others reported large reductions. Trials report averages; individuals live their own outcomes.
The 20 mg arm of PROGRESS did not show additional benefit beyond 10 mg and had more side effects, which is why Lexicon chose to take 10 mg forward into Phase 3.
What the Phase 3 Trials Will Test
Phase 3 is where investigational drugs either prove themselves or fail. As of Lexicon's most recent investor update in Q1 2026, here's the plan:
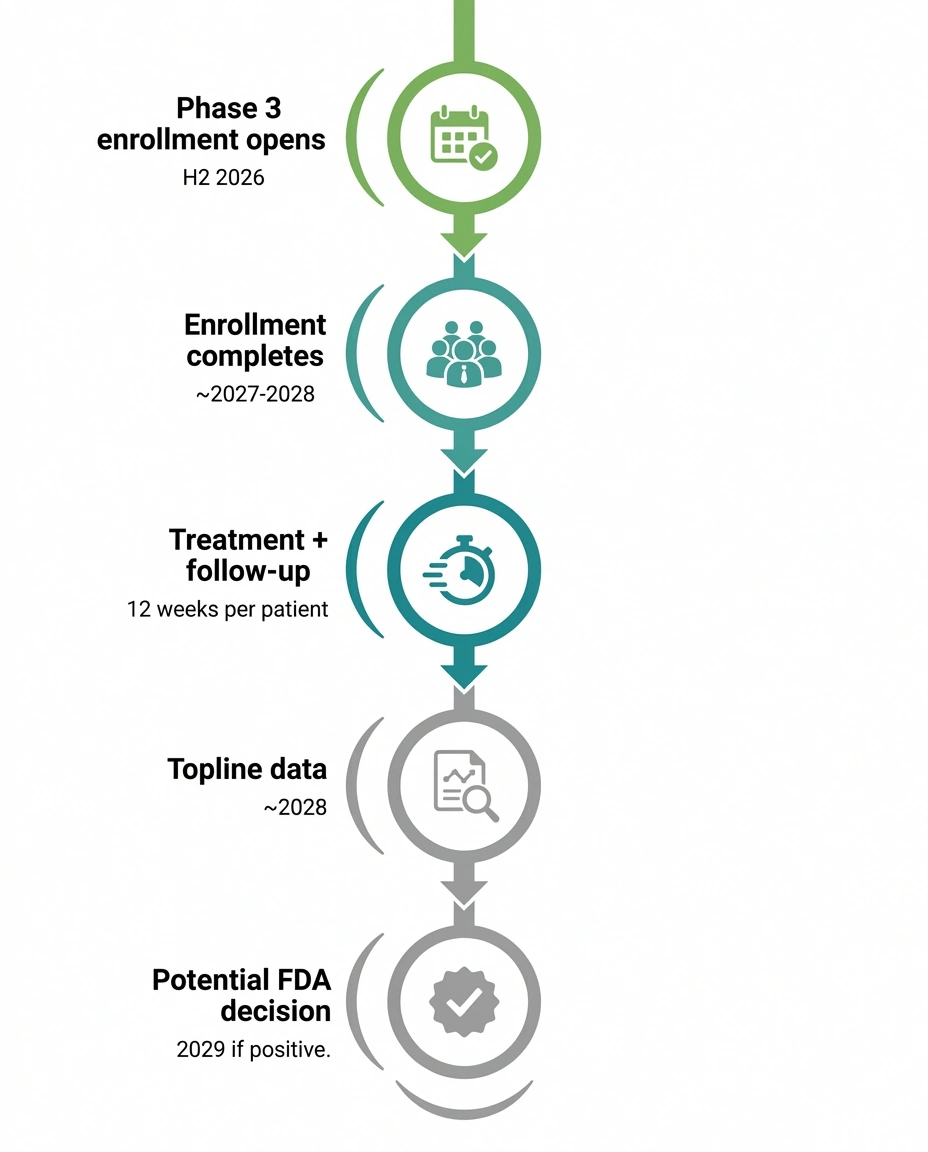
- Two placebo-controlled trials running in parallel, both for painful diabetic peripheral neuropathy.
- Twelve weeks of treatment, with the primary measurement being how much average daily pain scores drop from the baseline to Week 12.
- 10 mg daily versus placebo — only the dose that succeeded in Phase 2b is being tested.
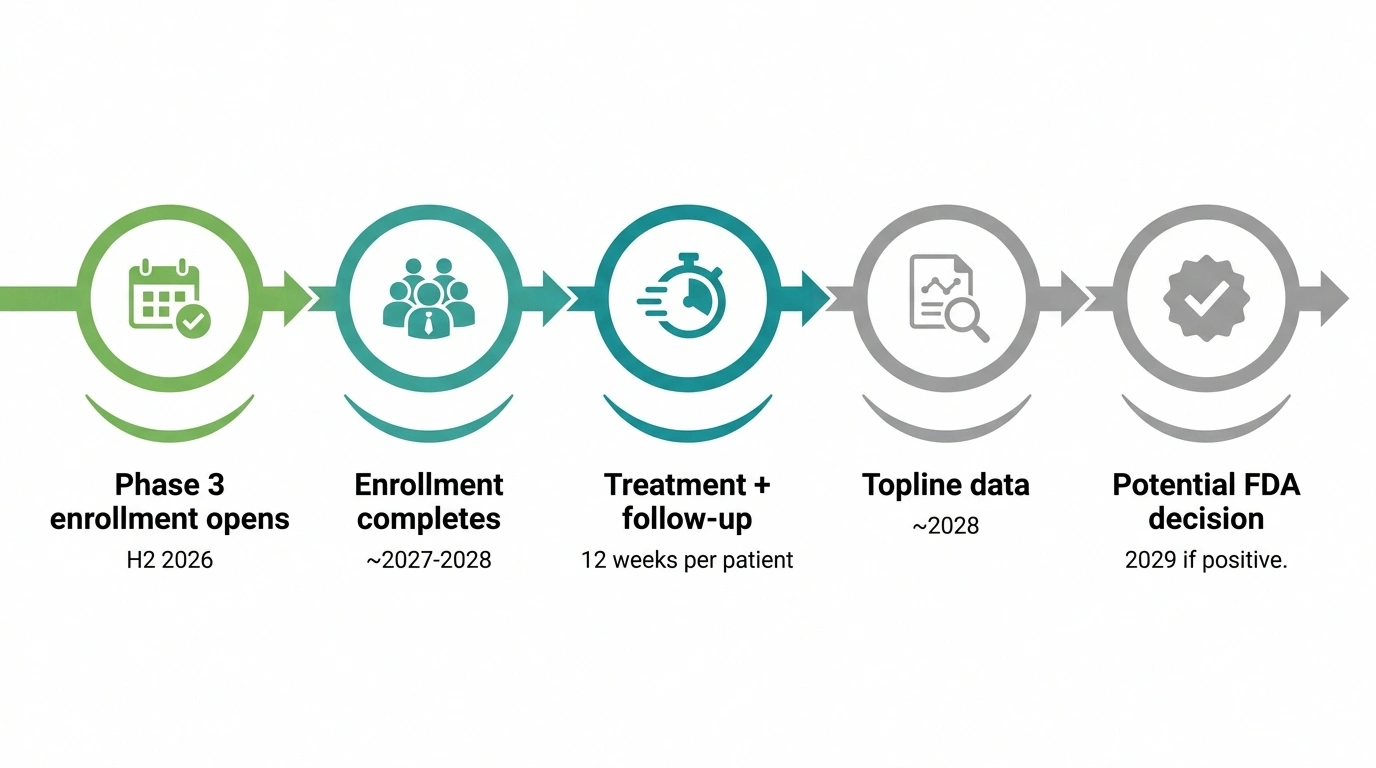
- Patient enrollment expected to begin in the second half of 2026. Phase 3 nerve-pain trials typically take 12 to 24 months to enroll and finish; topline results would then take additional months to analyze.
So even in the best-case scenario where the trials go smoothly and the results are positive, an FDA approval decision is realistically 2 to 3 years away from when enrollment opens. That's how Phase 3 timelines work in this field.
If you're someone who's interested in being part of trials like this — and your DPN is poorly controlled — clinical trial enrollment is one of the few ways to potentially access investigational therapies before approval. We have a separate guide on how to find and join neuropathy clinical trials that walks through the process step by step.
How Pilavapadin Compares to What's Available Now

To make sense of where pilavapadin might fit, it helps to look at the medications doctors currently reach for when treating painful diabetic neuropathy.
Duloxetine (Cymbalta) is FDA-approved for DPN. It's a serotonin-norepinephrine reuptake inhibitor (SNRI) — meaning it adjusts brain chemistry that influences pain perception. It can help mood symptoms as well, which is useful for people whose chronic pain has affected their emotional health. Side effects can include nausea, sleepiness, sweating, and sexual dysfunction. Our deeper article on duloxetine for neuropathy covers what to expect.
Pregabalin (Lyrica) is also FDA-approved for DPN. It calms overactive nerve signaling. Many patients find it effective but weight gain, swelling, drowsiness, and dependence concerns lead some to stop it. Read more about pregabalin for neuropathy.
Gabapentin (Neurontin) is widely prescribed for DPN but technically off-label — it's approved for post-herpetic neuralgia and seizures, not DPN specifically. It's the cheapest of the three and the most familiar to primary care doctors. Our gabapentin guide covers dosing and side effects in detail.
Tapentadol (Nucynta-ER) is approved for DPN but is a controlled opioid-class medication. Most clinicians and patients want to avoid it if possible.
What pilavapadin could offer — if approved — is a fourth option with a completely different mechanism. For people who haven't responded to the SNRI or gabapentinoid pathways, that matters. For people who've struggled with side effects from the current options, that matters too.
What pilavapadin won't be — at least at first — is a cure. None of these medications cure neuropathy. They reduce pain. That's a meaningful difference for daily life, but it's important to set expectations realistically.
Pilavapadin in the Wider Pipeline
Pilavapadin isn't the only investigational neuropathy drug moving through clinical trials right now. It's worth understanding the broader landscape so you can see where this one fits.
| Drug | Target | Status |
|---|---|---|
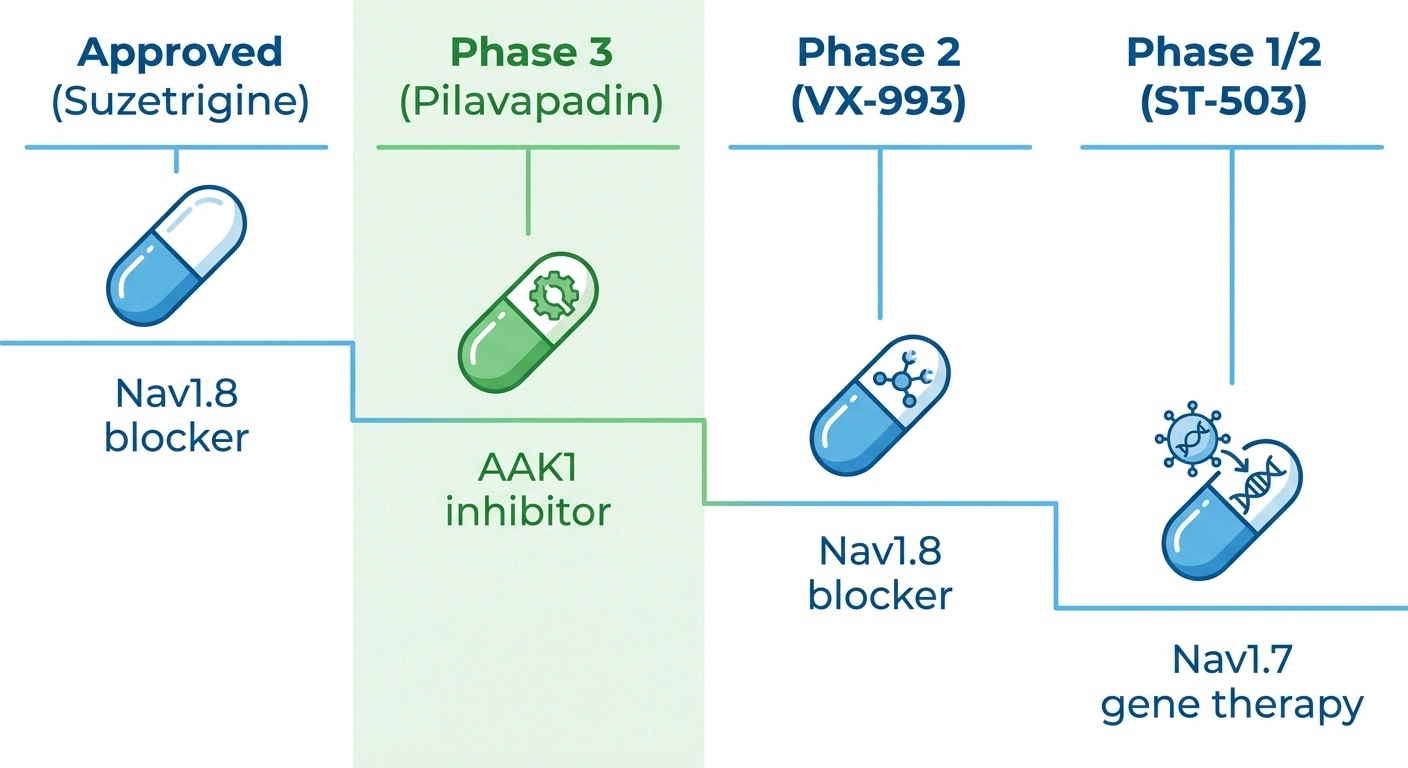
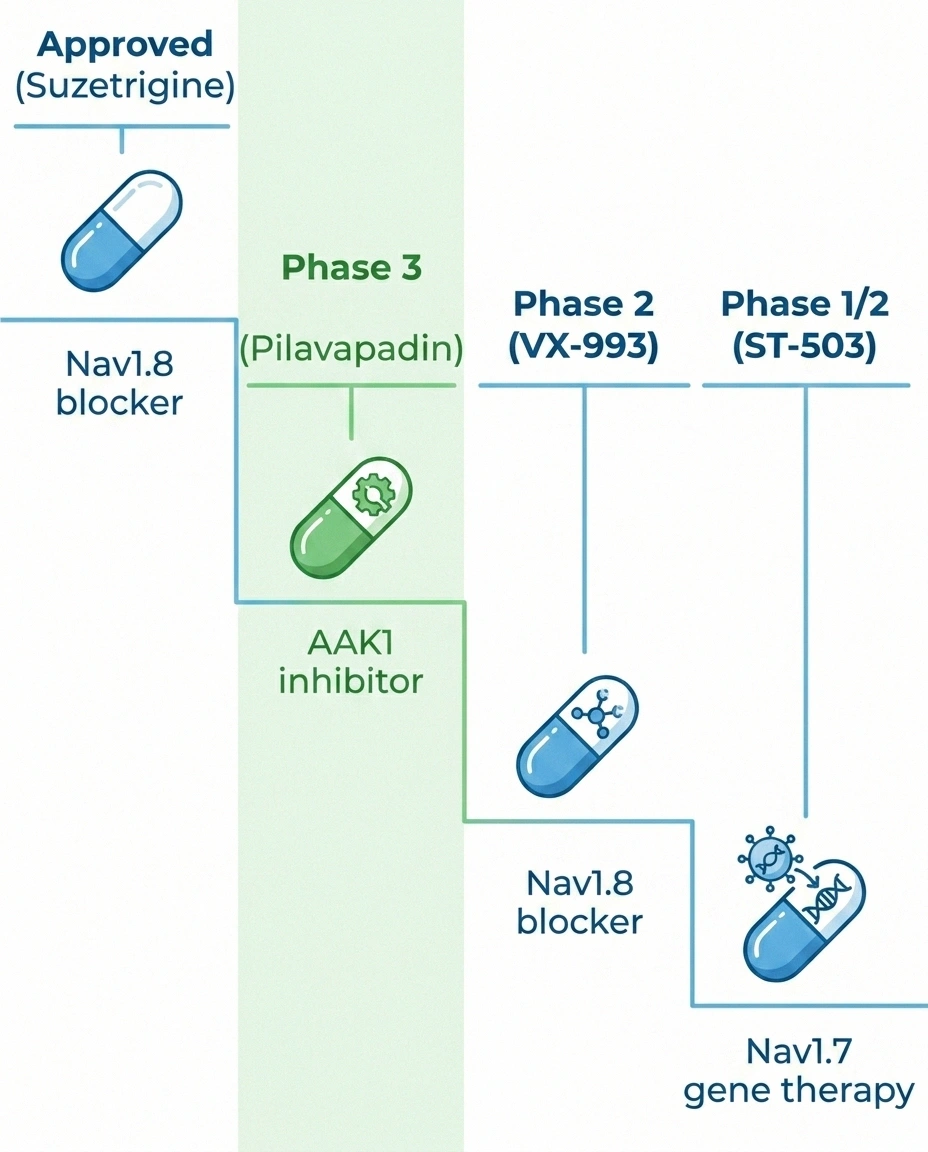
| Suzetrigine (Journavx) | Nav1.8 channel | Approved · acute pain |
| Pilavapadin (LX9211) | AAK1 enzyme | Phase 3 starting · DPN |
| VX-993 | Nav1.8 channel | Phase 2 · DPN enrolling |
| ST-503 | Nav1.7 gene | Phase 1/2 · iSFN |
The biggest recent news was the early-2025 FDA approval of suzetrigine, brand-named Journavx — the first new non-opioid mechanism approved for pain in about 20 years. Suzetrigine blocks the Nav1.8 sodium channel and is currently approved for acute pain. It's being studied for chronic neuropathic pain too. Our Journavx article explains how it works and what it might mean for nerve pain patients.
There are also gene therapies and other novel mechanisms in earlier trials — but those are years further out than pilavapadin. For a wider survey of what's coming, our guide to new neuropathy treatments in 2026 walks through the most credible pipeline candidates.
The honest summary is this: after two decades of stagnation, multiple non-opioid mechanisms are finally maturing in late-stage trials at the same time. Some will succeed and some will fail. Pilavapadin is one of the more advanced of these, but advanced doesn't mean guaranteed.
What Side Effects Have Shown Up So Far
In Phase 2b at the 10 mg dose, the most commonly reported side effects were mild to moderate — typically dizziness, nausea, and headache. Discontinuation rates at the 10 mg dose were similar to placebo, which is a reassuring sign for tolerability. The higher 20 mg dose showed more side effects without more pain relief, which is why it was dropped.
Importantly, the trial did not detect any opioid-like effects — no euphoria signal, no respiratory depression risk, no withdrawal pattern when patients stopped the drug. That's consistent with what the AAK1 mechanism would predict, and it's the central reason pilavapadin is being developed as a non-addictive alternative.
What we don't yet know:
- Long-term safety beyond 12 weeks. Phase 2b trials are relatively short. Issues that take 6, 12, or 18 months to emerge can't be detected in a 12-week study.
- How pilavapadin interacts with other medications. Many people with diabetic neuropathy also take medications for diabetes, blood pressure, cholesterol, and other conditions. Drug-interaction data will accumulate over the Phase 3 program and post-approval studies.
- Who responds and who doesn't. Some people will likely get substantial pain relief; others little or none. We don't yet have biomarkers or clinical features that predict who responds best.
What This Means for You Right Now

Pilavapadin is not available by prescription as of mid-2026. It cannot be obtained, imported, or prescribed off-label — there is no approved version. The only legal way to access it before potential FDA approval is through enrollment in a clinical trial.
- ✓ Confirm your current neuropathy medication is at an effective dose
- ✓ Tighten blood sugar control with your endocrinologist
- ✓ Track daily symptoms for at least 2 weeks to establish a baseline
- ✓ Watch ClinicalTrials.gov for Phase 3 enrollment near you
- ✓ Read about other late-stage pipeline drugs to understand your options
If you're currently managing painful diabetic neuropathy, here's what I'd suggest while pilavapadin works its way through Phase 3:
- Optimize the basics first. Tight blood sugar control is still the single most important factor in slowing the progression of diabetic nerve damage. If you haven't already had a thorough conversation with your endocrinologist about your A1c trajectory and your pain pattern, that conversation matters more than any new drug. Our diabetic neuropathy primer covers this in depth.
- Make sure you've actually tried adequate trials of current options. Many patients are on duloxetine or gabapentin at a dose that's too low to know if the drug works for them. Talk with your prescriber about whether your current treatment has been given a real chance at an effective dose. Our guide to what to do when neuropathy medication stops working walks through the conversation.
- Track your symptoms. Reliable, dated symptom tracking helps you and your doctor see whether anything is changing — and gives you a baseline if you do try a new medication or join a trial later. A simple notebook works; a structured symptom diary works better.
- Stay informed but skeptical. Anything you read about pilavapadin between now and approval — whether positive headlines or skeptical takes — is still based on Phase 2 data and an unfinished Phase 3 program. Treat news the way you'd treat a forecast: useful for planning, not a guarantee.
- Watch for trial sites. If Lexicon's Phase 3 trials open in your region and you meet the criteria, that's a potential pathway. Clinical trial sites get listed on ClinicalTrials.gov when enrollment begins.
What I'm Watching Next
Three milestones will shape whether pilavapadin becomes a real option for patients:
- The Phase 3 enrollment kickoff — expected in the second half of 2026. Once trials open, we'll have firmer dates for when results might come.
- The topline Phase 3 results — likely 12 to 18 months after enrollment completes. This is the moment of truth. Phase 3 results either confirm Phase 2 or don't.
- The FDA's eventual decision — if Phase 3 is positive, an NDA filing and FDA review would typically take 10 to 14 additional months.
I'll update this article as each of those milestones is reached. Bookmark it if you want to follow along. For broader context on what else is in development, our nerve regeneration and cure research article covers the wider landscape, and our complete neuropathy medications guide stays current on what's approved today.
Frequently Asked Questions
Is pilavapadin available by prescription right now?
No. Pilavapadin is investigational and has not been approved by the FDA. The only legal way to access it currently is through enrollment in an approved clinical trial. If a trial opens in your area and you meet the eligibility criteria, your doctor or the trial site can give you information. Do not seek it from non-trial sources online — anything sold as pilavapadin outside of an approved trial is not the real drug.
How is pilavapadin different from gabapentin or pregabalin?
Gabapentin and pregabalin both work by calming overactive nerve cell excitability through the same general pathway. Pilavapadin works on a completely different target called AAK1, which is involved in how pain signals are processed in the central nervous system. Different mechanism means it could potentially help people who don't respond to gabapentin or pregabalin, but that has not been proven yet.
What were the actual pain reduction numbers in the Phase 2b trial?
In the PROGRESS Phase 2b study, patients taking 10 mg of pilavapadin once daily had their average daily pain score drop by about 1.74 points on an 11-point scale. The placebo group dropped about 1.31 points. The roughly 0.43-point difference was statistically significant on the primary endpoint, meaning it was unlikely to be due to chance.
Is pilavapadin an opioid?
No. Pilavapadin is a non-opioid medication. It does not act on opioid receptors. In clinical trials so far, it has not produced euphoria, respiratory depression, or withdrawal symptoms after stopping — none of which are predicted by its AAK1 mechanism. Long-term studies will continue to confirm this profile.
When could pilavapadin be approved by the FDA?
If the Phase 3 trials succeed and are completed on schedule, an FDA approval decision is realistically 2 to 3 years away from when Phase 3 enrollment begins. Lexicon Pharmaceuticals indicated Phase 3 enrollment should begin in the second half of 2026, which would put a potential approval decision somewhere in 2028 or 2029. That timeline assumes everything goes well and is not guaranteed.
Will pilavapadin be expensive if approved?
Pricing has not been announced and will not be set until close to approval. New brand-name non-opioid pain medications have generally launched at significantly higher prices than generic gabapentin. Insurance coverage at launch is typically uneven and improves over time as evidence accumulates. Patient assistance programs from drug makers sometimes help reduce costs early on.
Does pilavapadin treat other kinds of neuropathy beyond diabetic?
The Phase 2 and Phase 3 studies have focused on painful diabetic peripheral neuropathy. Whether pilavapadin would work for chemotherapy-induced neuropathy, post-shingles nerve pain, idiopathic small-fiber neuropathy, or other types has not been studied. If it succeeds in DPN and is approved, additional studies in other neuropathies would likely follow.
What should I do while waiting for pilavapadin?
Optimize what's available now. Confirm your current medications are being used at adequate doses. Tighten blood sugar control if diabetic neuropathy is the cause. Track your symptoms. Stay engaged with your care team. New medications are coming, but the foundation of neuropathy management — the basics of blood sugar, foot care, sleep, movement, and mental health — continues to matter more than any single new drug.