
Complete Guide to Neuropathy Medications
If you have neuropathy, the medication conversation usually starts the same way: someone mentions gabapentin, someone else mentions Lyrica or Cymbalta, and before long it feels like you're drowning in drug names without a clear map.
Here's the clean version: there is no single best medication for neuropathy. The right starting point depends on your symptom pattern, age, other medical conditions, kidney function, fall risk, sleep quality, mood symptoms, and whether your pain is widespread or localized. This guide walks through the main medication classes, what they actually do, what to watch for, and how to decide what conversation to have with your doctor next.
What Neuropathy Medications Can and Cannot Do
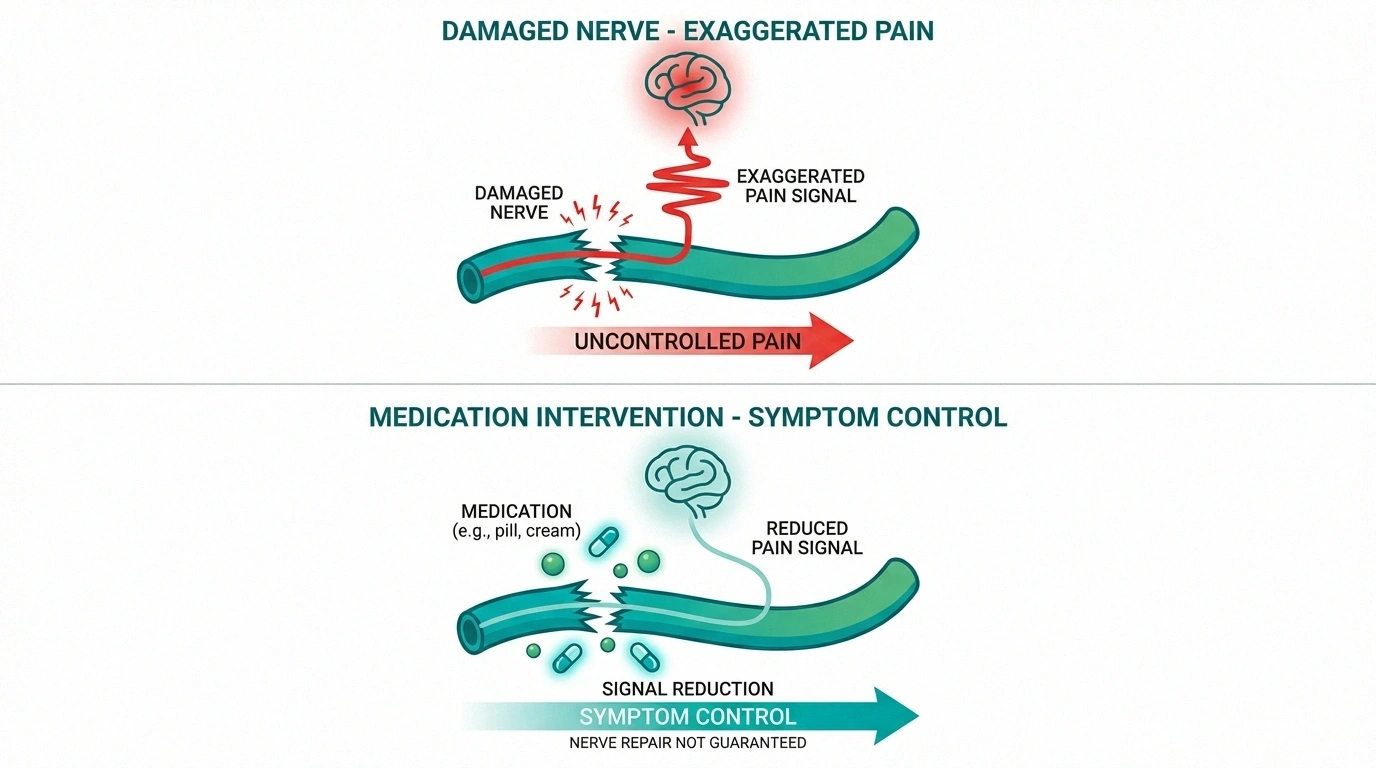
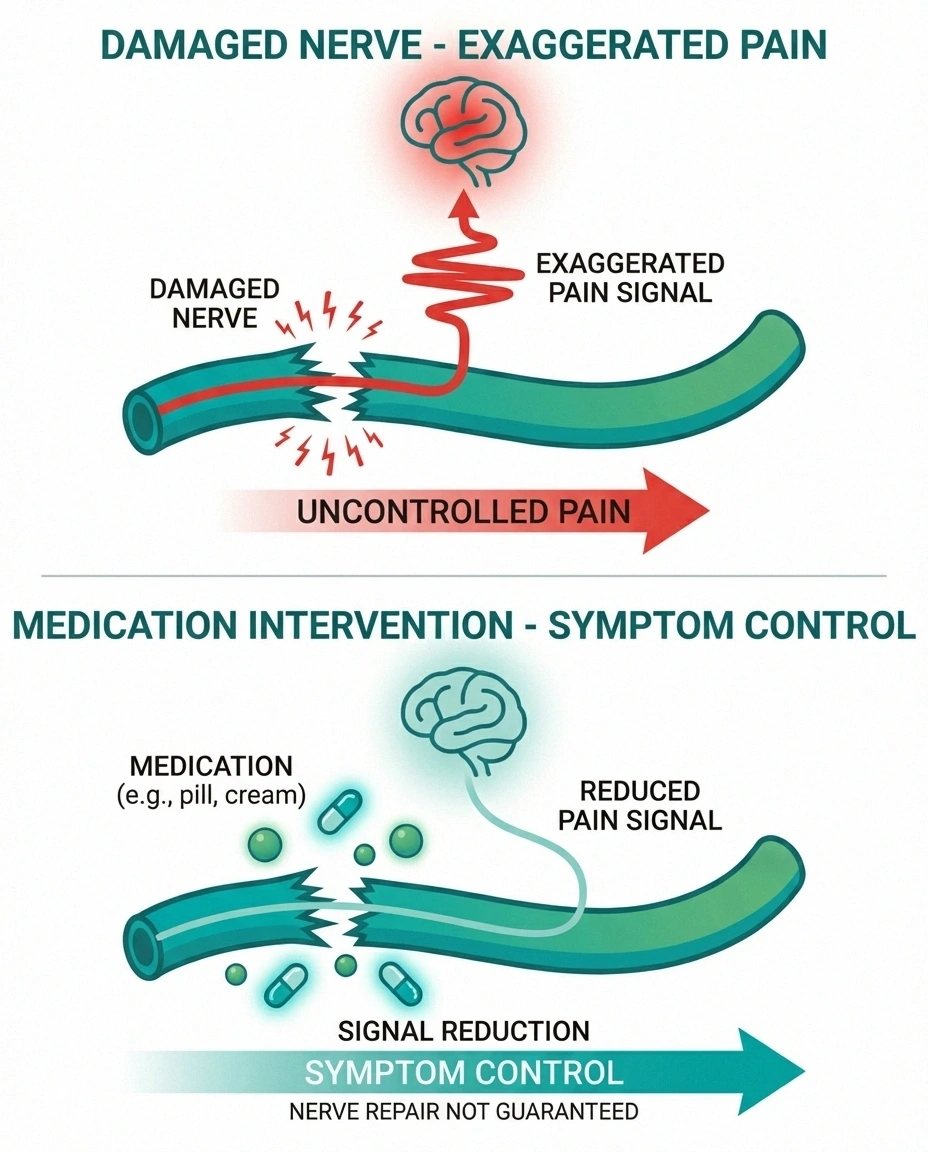
This is the first thing to get straight: most neuropathy medications do not reverse nerve damage. Their main job is to reduce the abnormal pain signaling coming from damaged or irritated nerves so daily life becomes more manageable.
That distinction matters because expectations shape whether people quit too early or keep chasing a “perfect” pill that does not exist. A good medication trial may do any of the following:
- Lower burning, tingling, stabbing, or electric-shock pain
- Make symptoms less constant or less intense
- Help you sleep through the night instead of waking up every time the sheets touch your feet
- Improve walking tolerance, function, and mood because the pain is less dominant
What it usually will not do is make advanced nerve damage disappear overnight. If a medication drops your pain from an eight to a four, that is often a meaningful win. The best outcomes usually come from combining medication with better glucose control when diabetes is involved, physical activity you can tolerate, foot protection, sleep support, and targeted work on the cause of the neuropathy.
First-Line Medications Doctors Usually Start With
Most clinicians start with one of a few well-known classes. They are not identical, but they are the medications most commonly discussed because they have the most real-world use in neuropathic pain.
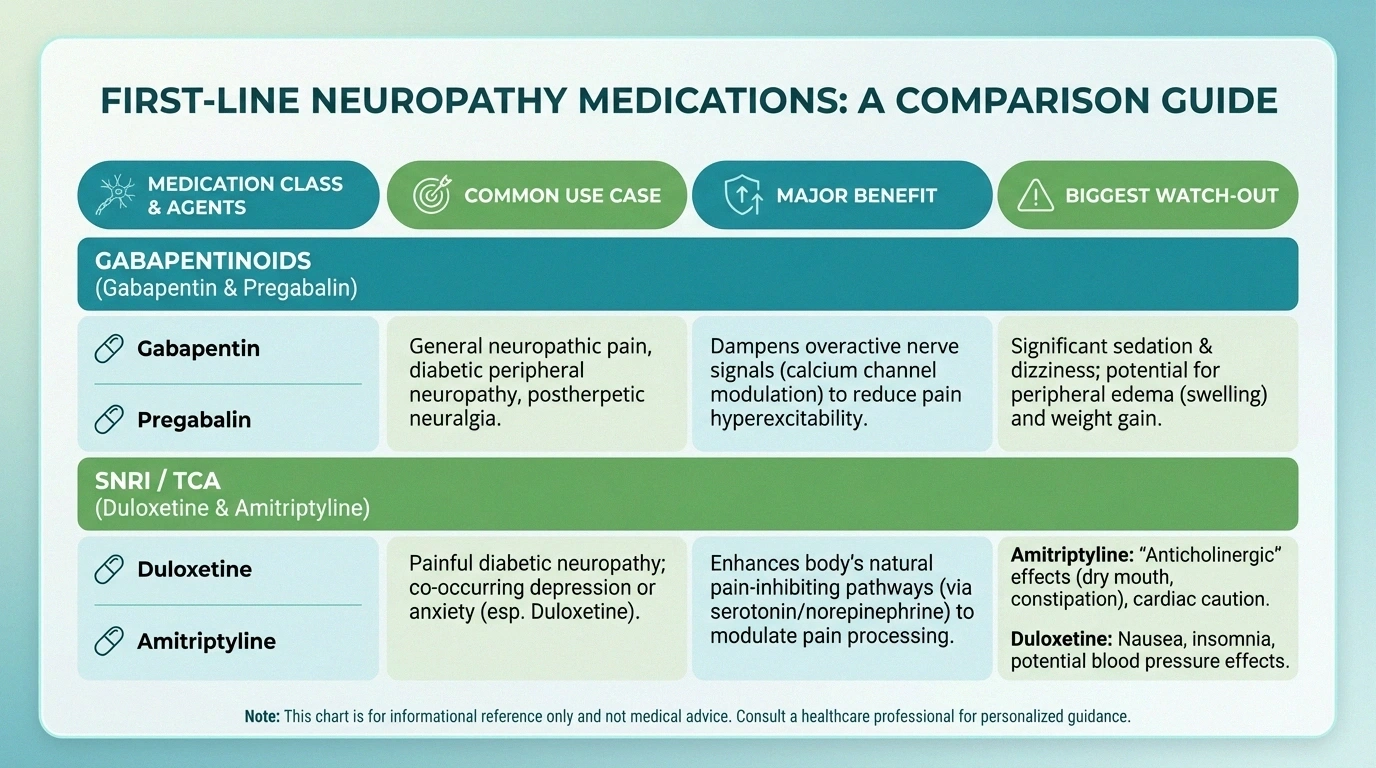
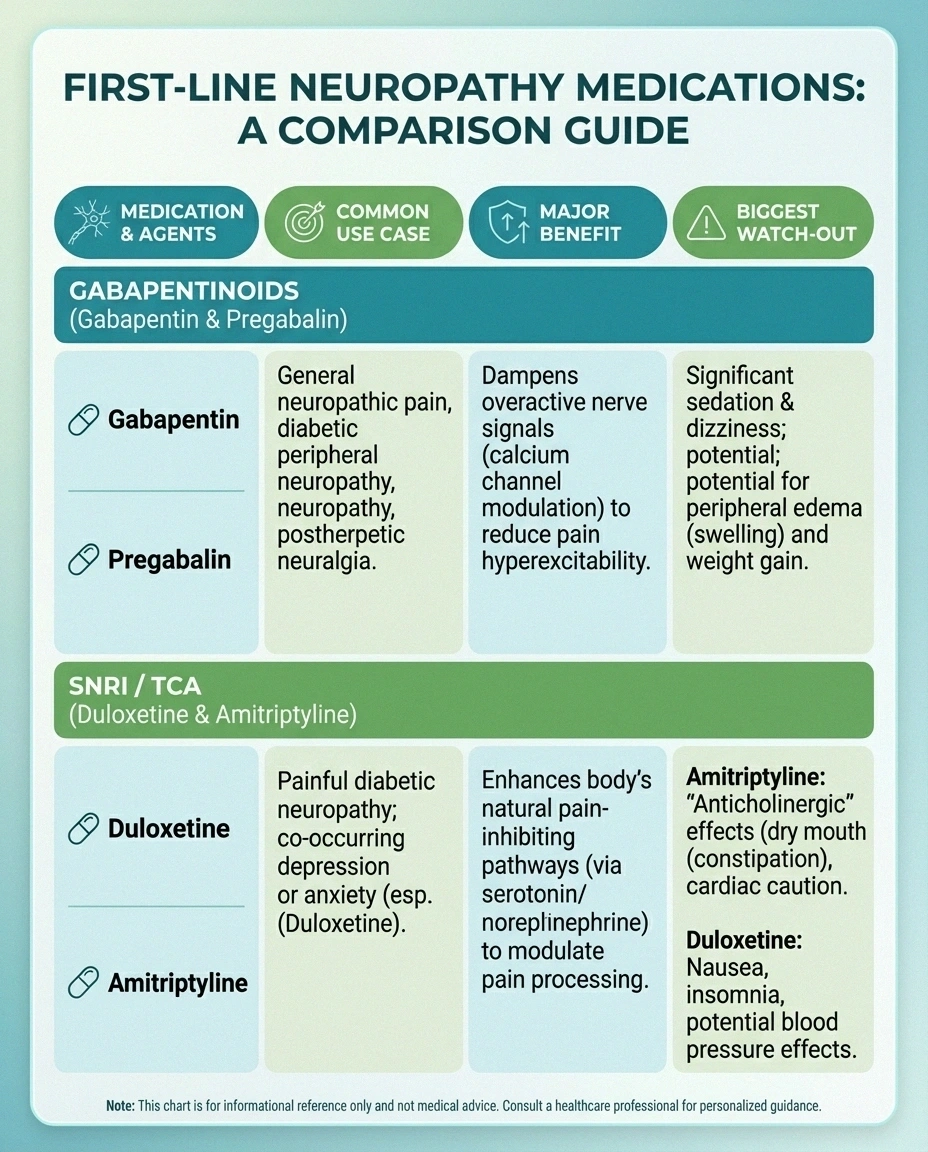
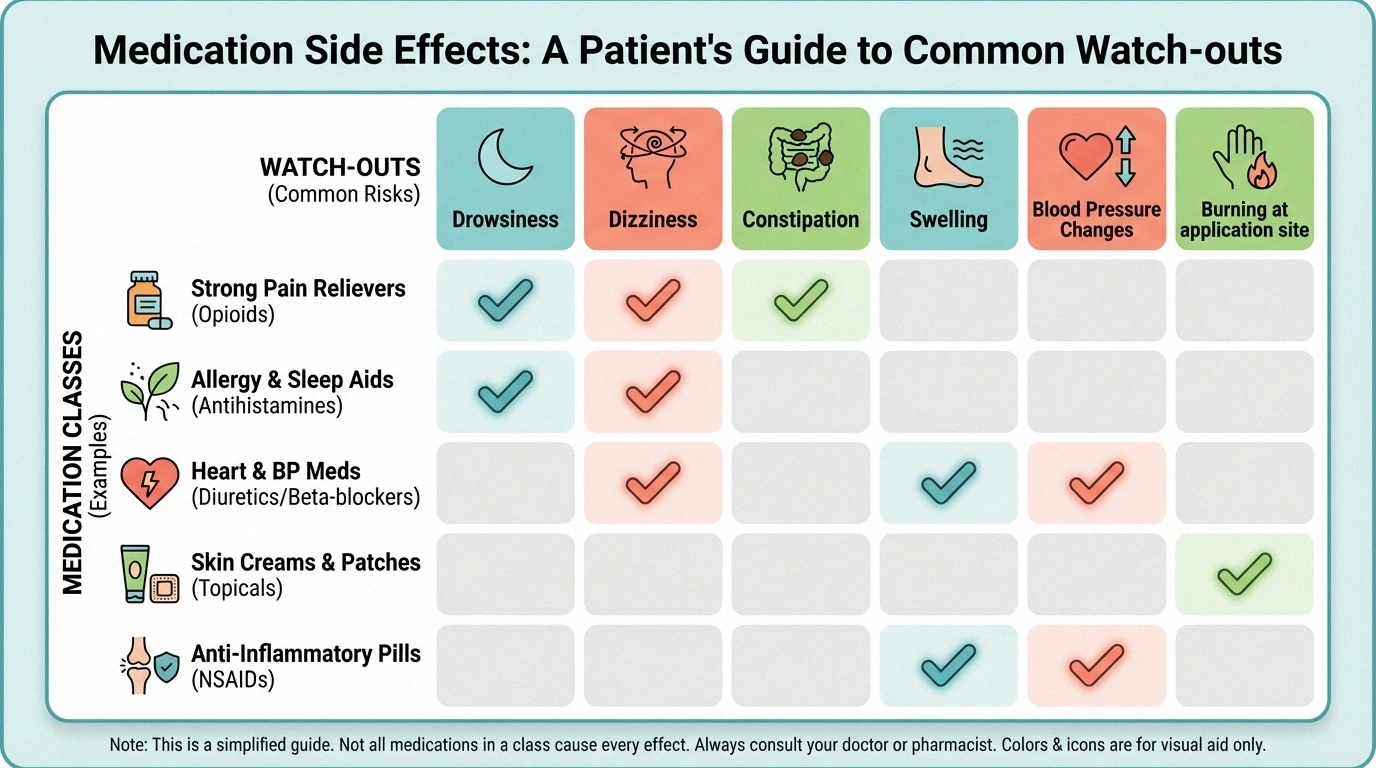
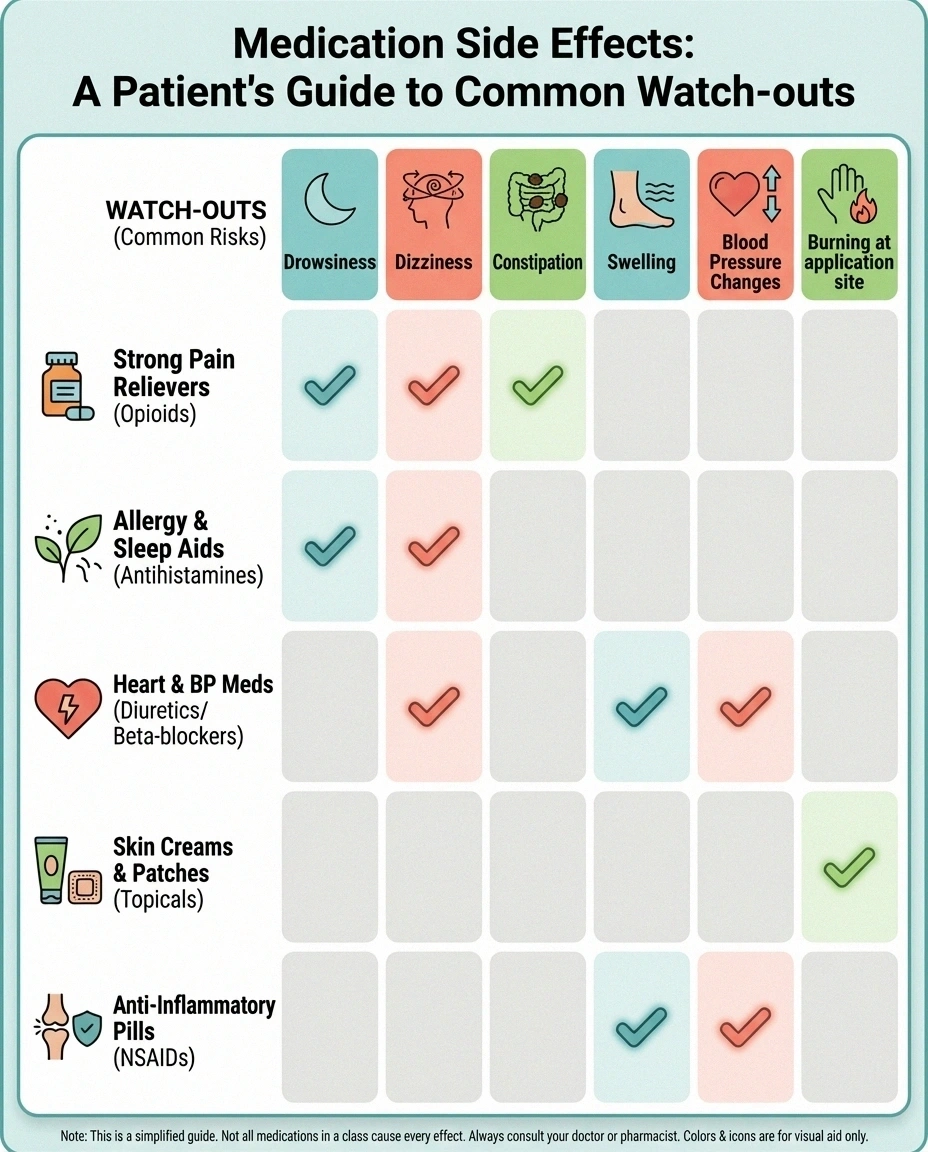
Gabapentin / Pregabalin
Often chosen when burning or shooting pain and night symptoms are dominant. Main tradeoff: drowsiness, dizziness, swelling, and brain fog in some people.
Duloxetine / Amitriptyline
Often useful when pain overlaps with sleep issues, mood symptoms, or a strong stress-pain loop. Main tradeoff: nausea, dry mouth, constipation, dizziness, or next-day grogginess.
Gabapentin and Pregabalin
Gabapentin and pregabalin calm overactive nerve firing. They are often used when neuropathy pain is burning, shooting, restless, or worst at night. They can be especially useful when sleep disruption is a big part of the problem.
Pregabalin is sometimes described as more predictable from a dosing standpoint, while gabapentin is often used first because it is familiar and widely available. Neither one is automatically “stronger” in a way that matters for every patient. The real question is whether you tolerate the dose needed for pain relief.
Common issues include drowsiness, dizziness, swelling in the feet or ankles, brain fog, and weight gain. Those side effects matter a lot if you already struggle with balance, fatigue, or daytime driving alertness. Kidney function also matters because dose adjustment may be needed.
Duloxetine and Other Antidepressants for Nerve Pain
Duloxetine is one of the better-known medication evidence for VA neuropathy claims for painful neuropathy, especially when pain and mood symptoms overlap. It works differently from gabapentin or pregabalin and may be a smart first choice if you also deal with depression, anxiety, or a strong stress-pain loop.
Older tricyclic antidepressants such as amitriptyline or nortriptyline can also help, especially when sleep is poor. But they can come with more baggage in older adults: dry mouth, constipation, blurry vision, dizziness, urinary trouble, and next-day grogginess. That does not make them bad medications. It makes patient selection more important.
If someone has glaucoma, significant heart rhythm concerns, urinary retention, or a history of medication sensitivity, that changes the conversation fast. This is why a medication that works beautifully for one person is a terrible match for someone else.
Topical and Second-Line Options

Not every patient needs a whole-body medication. If your pain is localized — for example, a patch of burning foot pain or a clearly defined area after shingles or surgery — topical treatment can make more sense.
Key Takeaway
If your pain is localized, a topical treatment may be the highest-leverage move because it can reduce pain without adding as much whole-body sedation.
Lidocaine patches and creams can numb a focused area without causing the same level of whole-body sedation as oral suzetrigine. Capsaicin works differently: it gradually reduces pain signaling in the treated area, but it can sting or burn at first. Some people hate that transition period. Others find it worth it because they avoid daytime grogginess.
There are also situations where doctors may consider tramadol or an opioid for a short window, but that is generally not the preferred long-term strategy for chronic neuropathic pain. Dependence, sedation, constipation, falls, and diminishing benefit over time are real concerns. In plain English: if the entire plan revolves around stronger and stronger pain pills, the architecture is probably wrong.
Side Effects That Matter Most in Real Life
People often ask, “Which medication has the fewest side effects?” That is the wrong question. The better question is: which side effects are most dangerous or disruptive for me?
Before You Start a Medication, Check These Risk Areas
Fall risk and balance problems
Kidney function and leg swelling
Constipation, urinary issues, or glaucoma concerns
Need to drive, work, or stay alert early in the day
- If falls are the biggest risk: be extra cautious with sedating medications that worsen dizziness or gait instability.
- If constipation is already a problem: tricyclic antidepressants may be harder to tolerate.
- If your feet and ankles already swell: gabapentin or pregabalin may require closer monitoring.
- If blood pressure, sweating, or multiple serotonin-active medications are in play: duloxetine deserves a more careful review.
- If pain is very localized: topical options may give you relief with fewer system-wide tradeoffs.
Older adults especially need a slower ramp-up. The “start low and go slow” rule is not just a cliché. It is how you avoid turning a reasonable trial into a side-effect disaster in week one.
How Doctors Choose a Starting Medication

A smart prescribing decision is not random. Your clinician is usually balancing four buckets at once:
How a Reasonable Neuropathy Medication Trial Usually Works
Pick the best-fit class
Choose based on symptom pattern, medical history, and side-effect risk.
Start low and give it a fair trial
Many medications fail because the dose was too low, too fast, or stopped before the trial was meaningful.
Reassess and pivot if needed
If the first class is a mismatch, switch strategy instead of assuming nothing will work.
- Symptom pattern: burning pain, allodynia, nighttime flares, sleep disruption, cramping, widespread pain, or localized pain
- Body constraints: kidney function, blood pressure, heart rhythm history, bowel/bladder issues, age, and fall risk
- Life constraints: do you need to drive early, care for grandchildren, work, or stay mentally sharp during the day?
- Overlap benefits: would one medication also help sleep, anxiety, or depression?
That is why one person gets gabapentin, another gets duloxetine, and another gets a lidocaine patch plus a non-drug plan. The “best” medication is usually the one that fits your real-life constraints well enough to stay on it long enough to judge it fairly.
If the first medication fails, that does not mean medications do not work for you. It often just means the first class was the wrong fit, the dose was limited by side effects, or the cause of your neuropathy has not been addressed yet. Sometimes the next best move is a different class. Sometimes it is a better workup with labs, a medication review, or a second opinion.
When Medication Is Not Enough
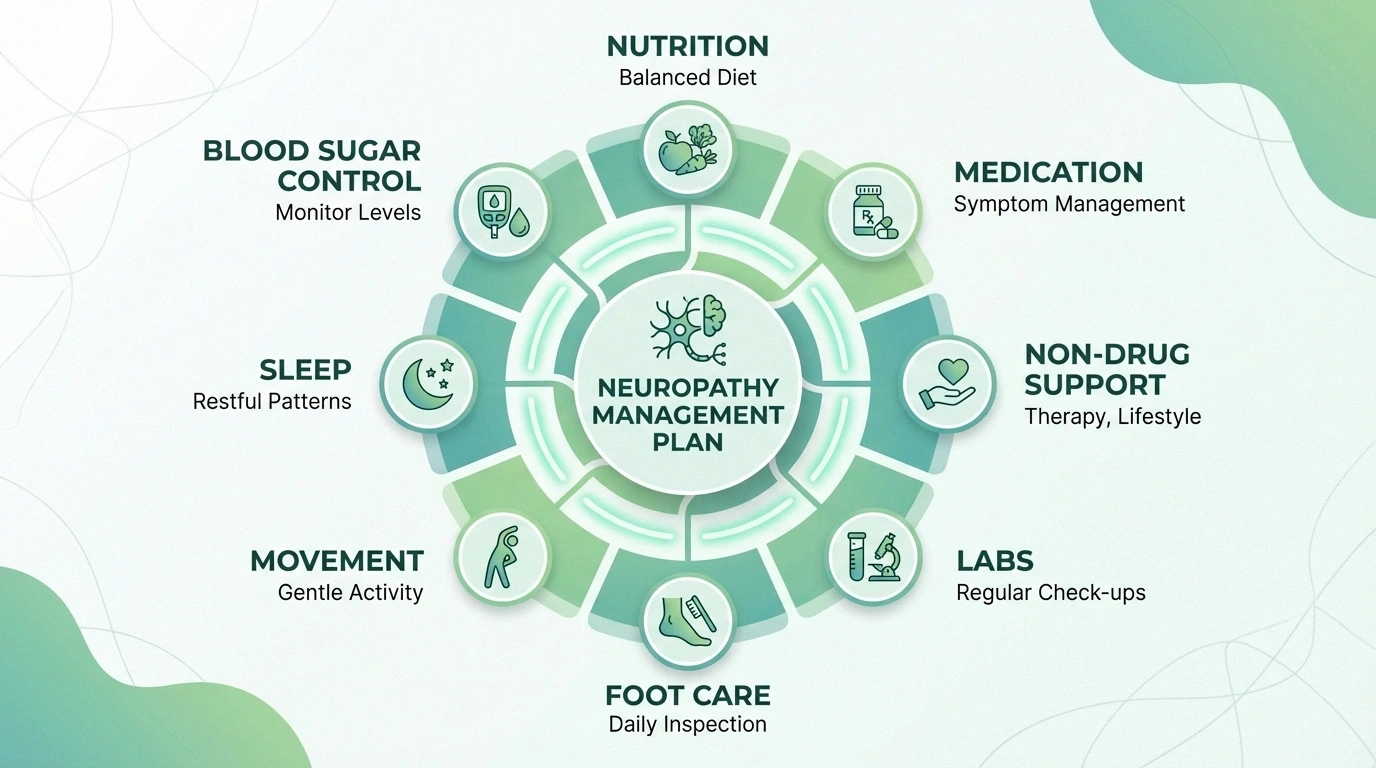

Medication is a layer, not the whole system. If you have diabetic neuropathy, blood sugar management still matters. If you have vitamin-related nerve damage, correcting the deficiency matters. If your symptoms worsen because of poor sleep, immobility, or constant flare-up triggers, medication alone will feel weaker than it should.
This is where people often regain leverage: combine a reasonable medication trial with movement you can tolerate, footwear that protects sensitive feet, targeted sleep changes, safer symptom tracking, and non-drug tools from our natural remedies hub or supplements hub. Not because “natural” replaces medication, but because the stack matters more than the single tool.
Frequently Asked Questions
What is the best medication for neuropathy?
There is no universal best option. Gabapentin, pregabalin, duloxetine, amitriptyline, lidocaine, and capsaicin all help some people. The right first choice depends on your symptoms, medical history, and side-effect tolerance.
Is gabapentin or pregabalin better for nerve pain?
Neither one wins for everyone. Pregabalin may feel more predictable for some patients, while gabapentin is often the more familiar starting point. Tolerability, cost, kidney function, and daytime sedation often drive the real decision.
Does duloxetine help neuropathy?
Yes, duloxetine can help painful neuropathy, especially when pain overlaps with low mood, anxiety, or poor sleep. It is not a fit for everyone, but it is one of the common first-line options doctors consider.
Do neuropathy medications heal nerves?
Usually no. Most neuropathy medications reduce abnormal pain signaling rather than repair the damaged nerve itself. That is why treating the underlying cause still matters.
What if the first neuropathy medication does not work?
That is common. Your doctor may adjust the dose, switch to another class, use a localized topical option, or revisit whether the diagnosis and workup are complete. One failed medication trial does not end the story.
The Bottom Line
The smartest way to think about neuropathy medication is not “Which pill is strongest?” It is “Which tool gives me the most relief with the fewest tradeoffs I cannot live with?”
Start there. Then build from reality: your symptoms, your age, your risks, your schedule, and your cause of neuropathy. That is how medication becomes useful instead of frustrating.
This article is for educational purposes only and does not constitute medical advice. Consult your healthcare provider before starting, stopping, or changing any medication.