For the better part of forty years, A1C has been the gold standard for measuring diabetes control. Every three months, you get a single number — an average of where your blood sugar has been — and you and your doctor make decisions based on it. If the number is below 7%, things are “in target.” If it creeps up, the medications get adjusted. That has been the rhythm of diabetes management for decades.
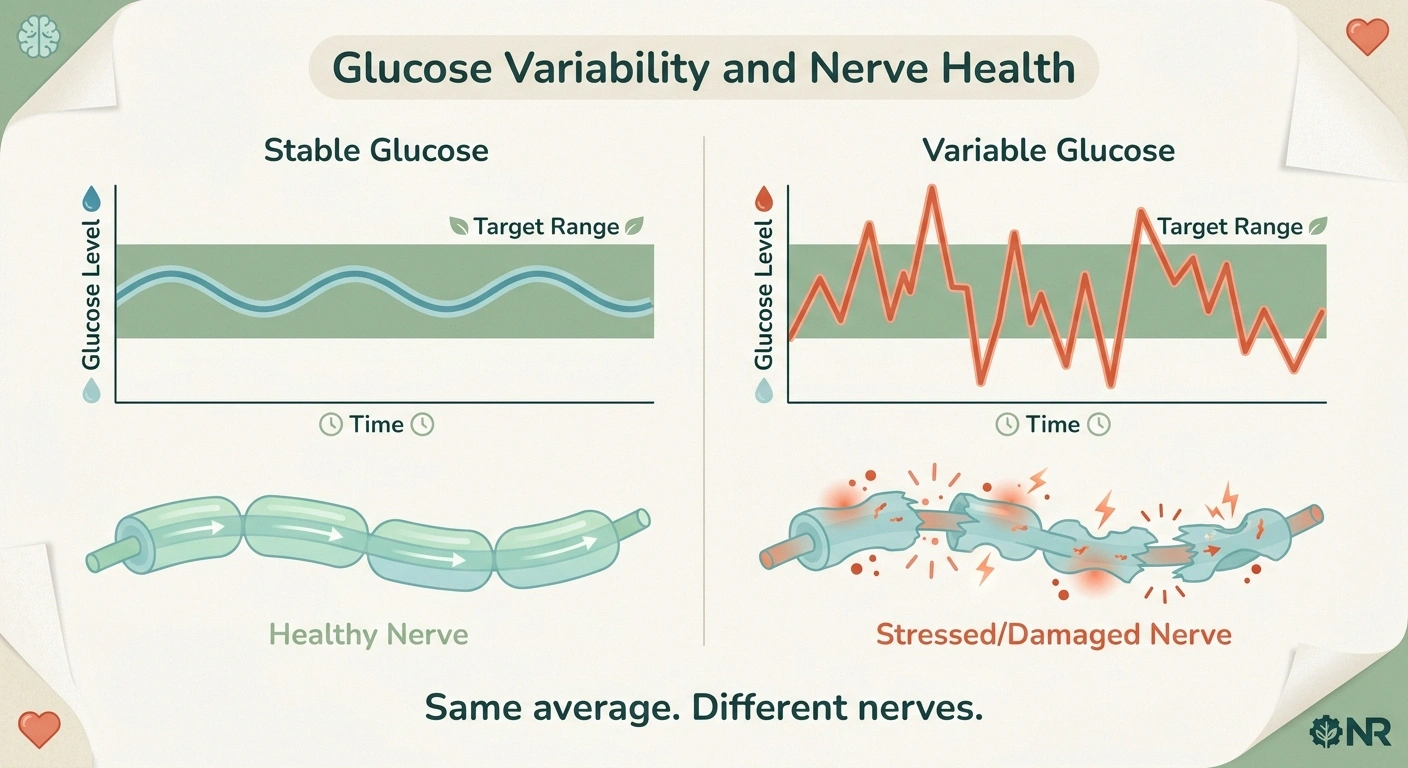
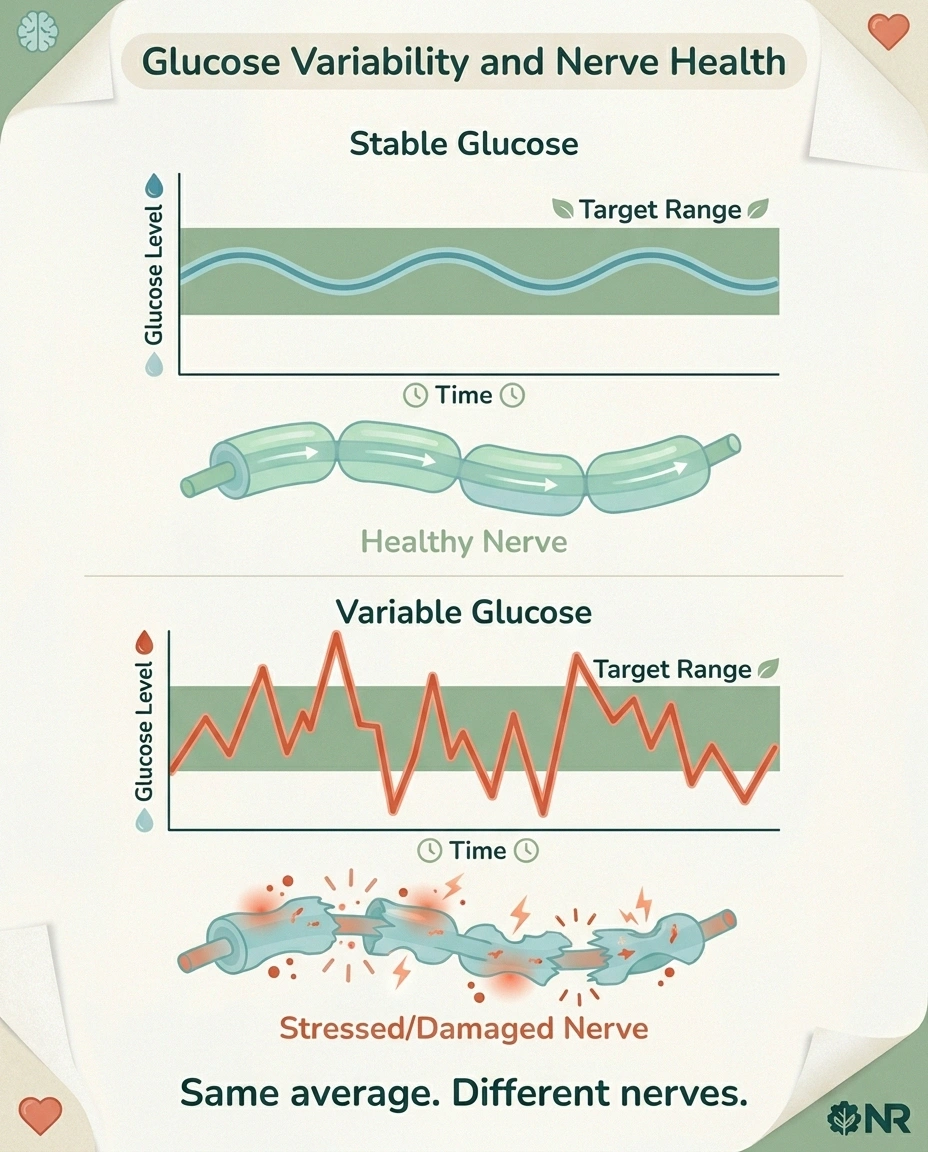
What that rhythm hid, and what we're finally getting good evidence about, is that two people with identical A1C numbers can be having radically different days. One can be cruising along steady. The other can be ricocheting between dangerous lows and screaming highs, and the average lands in the same place. Both look “well-controlled” on paper. Only one is actually protecting their nerves.
That's the gap that Time in Range — TIR — fills. And in 2026, the American Diabetes Association formally elevated TIR to a primary glycemic-assessment metric, putting it alongside A1C in the Standards of Care. For people worried about preventing or slowing diabetic neuropathy, this is one of the most practical shifts in diabetes management in a generation. Let me explain what changed, why it matters for your nerves specifically, and how to actually use it.
Why Time in Range Matters More Than A1C for Your Nerves
The reason A1C alone has always been an incomplete picture is that nerves don't experience “averages.” They experience the actual glucose level moment by moment. When blood sugar spikes high, the metabolic and inflammatory machinery that damages small sensory nerves runs hard. When blood sugar drops too low, a different kind of stress kicks in — and severe lows can themselves damage nerves over time. The wild swings between these states cause a kind of oxidative damage that a steady, only slightly-elevated glucose level does not.
Two people with the same 7.2% A1C might look identical on a quarterly lab report. But if Person A's blood sugar stays between 90 and 160 most of the day, and Person B spends two hours every afternoon at 280 and an hour every night at 55, the trajectory of their nerve health is going to diverge — even though their average is the same.
That's not theory. Research published in PMC has shown that lower Time in Range is independently associated with diabetic cardiovascular autonomic neuropathy AND with the severity of that neuropathy — even after controlling for A1C. Other research has tied TIR below 70% to elevated risk of diabetic peripheral neuropathy (the kind that affects your feet and hands). The pattern that keeps showing up: A1C tells you the average; TIR tells you whether the average is being achieved with steady control or with damaging swings.
What Time in Range Actually Means
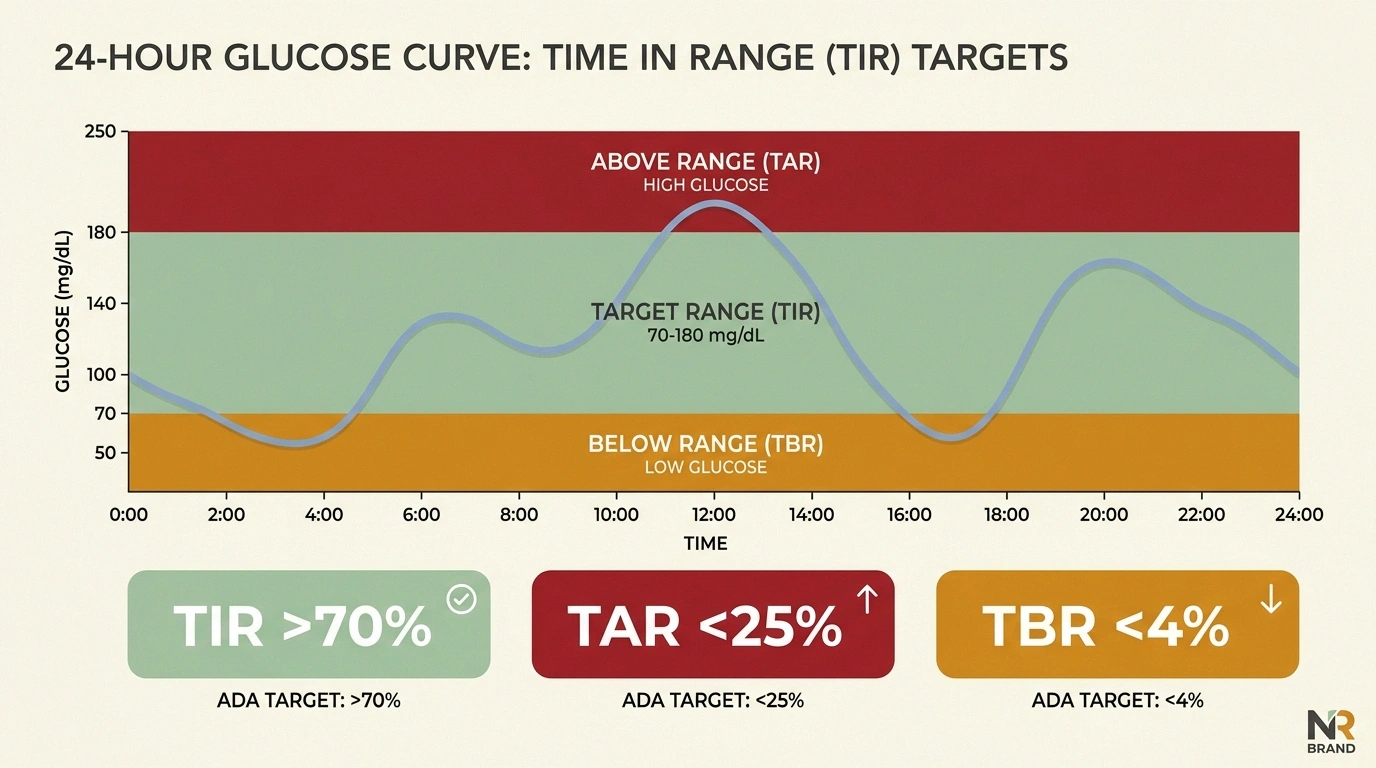
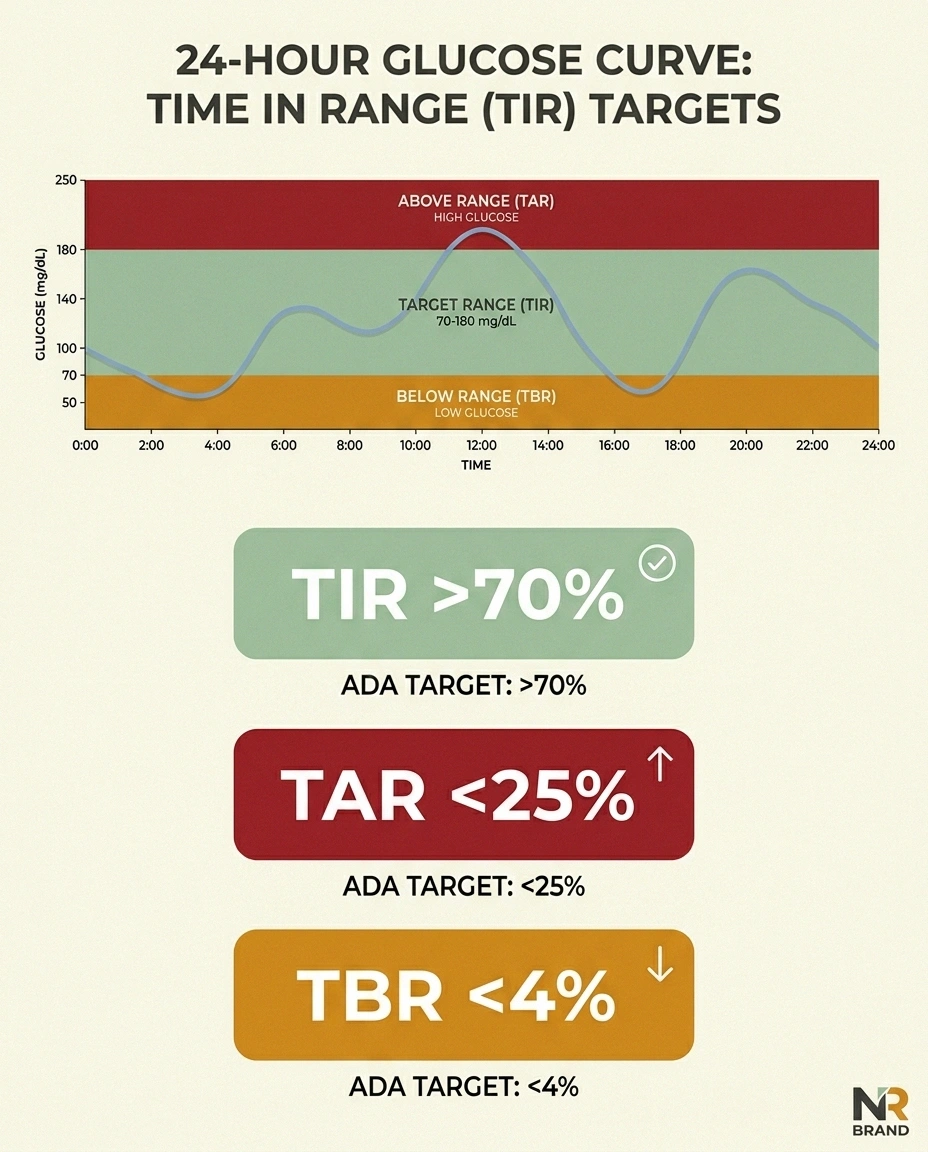
Time in Range is exactly what it sounds like: the percentage of the day you spend with your blood glucose inside a target zone. For most non-pregnant adults with diabetes, the target zone is 70 to 180 mg/dL. If you spend 17 hours of a 24-hour day inside that range, your TIR for the day is 71%.
You can't really know your TIR without a Continuous Glucose Monitor (CGM) — a small wearable sensor that reads your interstitial fluid glucose every few minutes for the duration that the sensor is on (typically 10 to 14 days per sensor). The sensor pairs with an app or receiver, and after about two weeks of wear, you have enough data to see your real glycemic life.
Finger-stick checks alone can't reasonably produce a TIR number. Even checking 6 times a day, you're sampling 6 of the 288 five-minute windows the day contains. The most carefully managed finger-stick patient is still flying blind for 282 of those windows.
The Three Numbers Every CGM Reports

Time in Range is the headline metric, but it's part of a three-number set, and you need all three to read your data properly.
Time in Range (TIR) — % of time at 70-180 mg/dL. Target for most adults: greater than 70%. Every 5% increase in this number meaningfully reduces microvascular complication risk, including neuropathy.
Time Below Range (TBR) — % of time under 70 mg/dL. Target: less than 4%, with less than 1% under 54 mg/dL. Hypoglycemia is dangerous in its own right (loss of consciousness, seizures), and severe or recurrent lows damage the nervous system. A high TIR achieved by allowing dangerous lows is not progress.
Time Above Range (TAR) — % of time over 180 mg/dL. Target: less than 25%, with less than 5% over 250 mg/dL. This is where most nerve damage from hyperglycemia happens.
If you're trying to protect your nerves, the order of priority is usually: first eliminate the dangerous lows (TBR), then chip away at the highs (TAR), and your TIR will rise as a result.
How TIR Connects to Neuropathy Risk: The Science
The biological reason TIR matters more than A1C for nerve health comes down to glycemic variability — the technical term for how much your blood sugar swings. When researchers compare patients matched on A1C, the ones with higher variability have worse measurable nerve outcomes.
The proposed mechanisms are several. Glucose spikes drive a burst of reactive oxygen species — molecular damage agents that injure the small unmyelinated nerve fibers in your feet and hands. Repeated spikes also drive inflammation in nerve tissue. The advanced glycation end-products (AGEs) that crosslink your tissues form preferentially under variable, high-glucose conditions. And the protective machinery of the small nerves — already running on tight metabolic margins — gets overwhelmed by the combination of insults.
TIR captures all of this in a way A1C cannot. A patient with TIR of 80% has a fundamentally different glucose pattern from a patient with TIR of 45%, even if their A1Cs are the same. Their nerves know the difference. And the research bears that out: a 5% increase in TIR is associated with measurable reductions in DPN risk, retinopathy progression, and albuminuria (kidney involvement).
The 70% Threshold: What 2026 ADA Standards Say
The 2026 American Diabetes Association Standards of Care formally recommend CGM for ALL people with diabetes — type 1, type 2, latent autoimmune diabetes in adults (LADA), gestational, and “any kind of diabetes.” That's a significant change from earlier years where CGM access was largely restricted to insulin-dependent type 1 patients.
The TIR target the ADA sets for most non-pregnant adults is greater than 70%. There are exceptions: pregnant women, frail older adults, and patients at high hypoglycemia risk have different targets (typically higher TIR target for pregnancy, more relaxed for frail elderly to prevent dangerous lows).
The ADA also formally recognizes TIR as a “valid glycemic assessment metric associated with the risk of microvascular complications” — meaning that physicians can now treat TIR as a primary outcome metric, not just an A1C supplement. That's the regulatory and clinical opening that lets your doctor adjust your medications based on the CGM data instead of waiting for the next quarterly A1C draw.
A1C vs TIR: Two People With Identical A1C, Very Different Nerves
To make this concrete, let me walk through what two patients might look like, both with a 7.2% A1C — comfortably below the 7.5% threshold most physicians use for “well controlled.”
Low, steady DPN risk
Active damage to nerves
Patient A: Type 2 diabetes, takes metformin and a low-dose SGLT-2 inhibitor. Wears a CGM. Her glucose stays between 95 and 155 about 75% of the day. She has occasional spikes to 200 after high-carb dinners and occasional mornings around 130. TIR: 78%. TAR: 20%. TBR: 2%. Her neuropathy risk is low and steady.
Patient B: Type 2 diabetes, same medications, same age, same A1C. But doesn't wear a CGM. He has 30-40 minutes of mid-90-mg/dL “lows” that feel uncomfortable to him, followed by overcorrections that send him to 240-260 for two or three hours twice a day. The average lands at the same place. TIR (if measured): 48%. TAR: 45%. TBR: 7%. Patient B's nerves are taking damage that Patient A's are not — but neither of them, and neither of their doctors, would know it without the CGM data.
The reason this matters practically is that the fix for Patient B isn't more medication — it's smaller, more frequent meals, fewer simple-carb spikes, better timing on the metformin dose. Behavioral changes informed by data he can SEE, not data hidden inside a quarterly average.
How to Get a CGM in 2026

The mechanics of getting a CGM are easier than they used to be, but still vary by insurance, diabetes type, and where you live.
Medicare: Covers CGM for both type 1 and type 2 patients on any insulin therapy. Recent updates expanded coverage to some non-insulin type 2 patients as well, particularly those with a history of hypoglycemia.
Private insurance: Most major plans cover CGM for type 1 and insulin-using type 2. Non-insulin type 2 coverage is more variable — some plans require prior authorization or proof of glycemic variability.
Over-the-counter: Several CGMs are now available without a prescription, including some lower-cost models targeted at non-diabetic users for general health monitoring. These typically aren't insurance-covered but provide the same TIR data.
Common brands include Dexcom G7, FreeStyle Libre 3, and Medtronic Guardian. Each has slightly different sensor-wear duration, smartphone compatibility, and accuracy profile. Your endocrinologist or diabetes educator can recommend one based on your specific situation.
How to Improve Your TIR: A Practical Playbook

Once you have a CGM and can see your TIR, the question becomes how to raise it. The answer depends on what your data is showing.
If your problem is post-meal spikes: Look at meal composition. Adding protein, fiber, and healthy fats to carbohydrate-containing meals slows glucose absorption. Walking 10-15 minutes after a meal blunts post-prandial peaks. Timing your medication (especially rapid-acting insulin) 15-20 minutes before eating instead of with the meal can also help.
If your problem is overnight or fasting highs: Talk to your doctor about basal medication adjustment. Some patients see fasting glucose drop substantially with a small change in long-acting insulin timing or with the addition of a low-dose SGLT-2 inhibitor (if appropriate).
If your problem is hypoglycemia (low TBR): This is the priority. Recurrent or severe lows are dangerous and damaging. Lows often indicate over-treatment — too much insulin or sulfonylurea for current diet and activity. Sometimes the fix is reducing medication; sometimes it's eating more consistently or timing food differently.
If your problem is general variability: Consistency in meal timing, meal composition, and activity level reduces variability. So does sleep — poor sleep drives morning glucose up and reduces insulin sensitivity all day.
The CGM lets you test changes in days, not months. That feedback loop is itself part of what makes TIR-driven management more effective than A1C-driven management for nerve protection. You can SEE the consequences of yesterday's dinner this morning, instead of finding out three months later that something in your routine wasn't working.
What If You Already Have Neuropathy?
If you already have diabetic peripheral neuropathy, improving TIR isn't going to reverse damaged nerves. But it can slow the progression — and that's the realistic goal. Damaged nerves are vulnerable. Continuing the metabolic stress that damaged them in the first place ensures more damage. Stabilizing your glucose stops adding insult to the existing injury.
This is also where TIR data becomes useful for your specialist visits. Walking into a neurologist or endocrinologist appointment with two weeks of CGM data is a fundamentally different conversation than walking in with a single A1C number. The doctor can see exactly when and how things are going wrong, and the treatment recommendations become specific instead of generic.
For more on managing existing diabetic neuropathy, see our complete diabetic neuropathy treatment guide. And if you're trying to prevent it from progressing, our evidence-based prevention guide covers the broader strategy.
The Honest Limitations
CGM and TIR aren't magic. A few honest caveats worth holding in mind.
CGMs measure interstitial glucose, not blood glucose directly. There's a small lag (5-15 minutes) between blood and interstitial values, especially during rapid changes. For most decisions this doesn't matter; for severe hypoglycemia treatment, the standard is still to confirm with a finger stick.
Adhesion, skin reactions, sensor failures, and accuracy can all vary by person. Not everyone wears the same sensor with equal success. Switching brands sometimes solves persistent problems.
The data can become an obsession for some people. If checking your CGM 50 times a day is making your life worse rather than better, the answer is to set check-in windows (morning, before meals, before bed) rather than continuous monitoring. The point of the data is informed decisions, not anxiety.
And TIR is one piece of a bigger picture. Blood pressure, lipid management, foot care, weight management, exercise, sleep — these all influence neuropathy risk independently of glucose. TIR isn't a replacement for the rest of the diabetes-management toolkit; it's a sharper tool inside it.
What to Ask Your Doctor

If you're not already on a CGM and you're worried about neuropathy progression, the conversation with your physician might look like this: “I want to know my Time in Range, not just my A1C. Can we get me on a CGM, and at the next visit, can we review the data together to see if there's a pattern we can fix?”
- “I want to know my Time in Range, not just my A1C — can we get me on a CGM?”
- “Can we review my CGM data together at the next visit?”
- “What can I change today to lift TIR by 5% this month?”
If you're already on a CGM and not getting much out of it, the question is: “Can we look at this data together and figure out where the worst hours are and what we can change?”
The 2026 ADA Standards make CGM-driven management the standard, not the exception. Your insurance company knows it. Your doctor probably knows it. Sometimes the conversation just hasn't happened yet.
Frequently Asked Questions
What is a “good” Time in Range number?
For most non-pregnant adults with diabetes, the ADA target is greater than 70% TIR (70-180 mg/dL). Pregnant women have higher targets (typically >70% within 63-140 mg/dL). Frail older adults may have more relaxed targets to prevent hypoglycemia. Discuss the right target with your doctor.
Does TIR replace A1C entirely?
No — both metrics are useful. A1C captures a 3-month average and is easy to measure with a single blood draw. TIR captures variability and the actual pattern of glucose over time. The 2026 ADA Standards recommend tracking both, with TIR weighted heavily for day-to-day management decisions.
Can I improve my TIR without medication changes?
Often yes. Meal composition, meal timing, post-meal walks, sleep quality, and stress management all influence TIR. Many people see meaningful improvement from lifestyle adjustments alone, especially in early type 2 diabetes. Significant medication changes should always be made with your doctor.
Will a CGM be uncomfortable to wear?
Most modern CGM sensors are about the size of a half-dollar coin and adhere to the back of the upper arm or abdomen for 10-14 days at a time. Most users report no significant discomfort. Some experience skin reactions to the adhesive, which can usually be managed with skin barrier wipes or rotating sensor sites.
How long do I need to wear a CGM to understand my TIR?
About 14 days of wear is generally considered sufficient to characterize a typical week. Some patterns (weekday vs weekend, work vs vacation, menstrual cycle effects) take longer to appear. Continuous long-term wear is increasingly common and provides the most actionable data.
Will improving my TIR reverse existing neuropathy?
Better TIR can slow progression and may modestly improve some symptoms over time, but established nerve damage is not typically reversed by glucose control alone. The realistic goal is prevention of further damage and stabilization of symptoms. Existing neuropathy is also managed with medications, supplements, lifestyle changes, and sometimes specialized therapies.
Is TIR the same as glycemic variability?
They're related but not identical. TIR captures both the level and the variability of glucose. Glycemic variability is specifically a measure of how much glucose swings (typically expressed as coefficient of variation or standard deviation). High variability is one cause of low TIR, but you can also have low TIR with low variability if your glucose is steadily too high.
Do I need a doctor's prescription for a CGM?
For insurance coverage, yes. Some over-the-counter CGMs are now available without prescription but generally aren't insurance-reimbursed. If you have diabetes and meet the coverage criteria, a prescription is the path that gets it covered.
What if my insurance won't cover a CGM?
Manufacturer patient-assistance programs, generic OTC sensors, and short-term professional CGM (where you wear a clinic-loaned sensor for 1-2 weeks and the data is shared with your doctor) are all options. A diabetes educator or social worker at your endocrinology clinic can help navigate coverage barriers.