
I'll start with the hard part, because the rest of this guide depends on understanding it: a heating pad on numb skin can produce a serious burn before you feel anything wrong. Not because heating pads are dangerous in some absolute sense — most people use them safely their whole lives. But because they assume the user can feel “too hot” and pull away. When neuropathy has taken that signal offline, the heating pad keeps doing exactly what it was designed to do, and the consequence shows up as blistered skin in the morning.
This is one of those topics where the safety conversation has to be specific to actually be useful. “Be careful with heating pads” doesn't tell you anything. What temperature is safe? For how long? On what body parts? With what barriers? When should you skip the heating pad entirely and reach for something else? Let me walk through the practical rules, the alternatives that work just as well without the burn risk, and the warning signs that mean you should call your doctor.
Why a Heating Pad Is Risky When Your Sensation Is Compromised
Healthy skin doesn't burn at low heating-pad temperatures because you feel the heat building up and adjust — you reposition, lower the setting, slip the towel underneath, get up for a minute. Neuropathy interrupts that loop. The temperature sensors in your skin send their signals through the same nerves that carry the burning and tingling sensations of nerve damage. When those nerves stop signaling normally, the “this is too hot” message either doesn't arrive or arrives garbled and late.
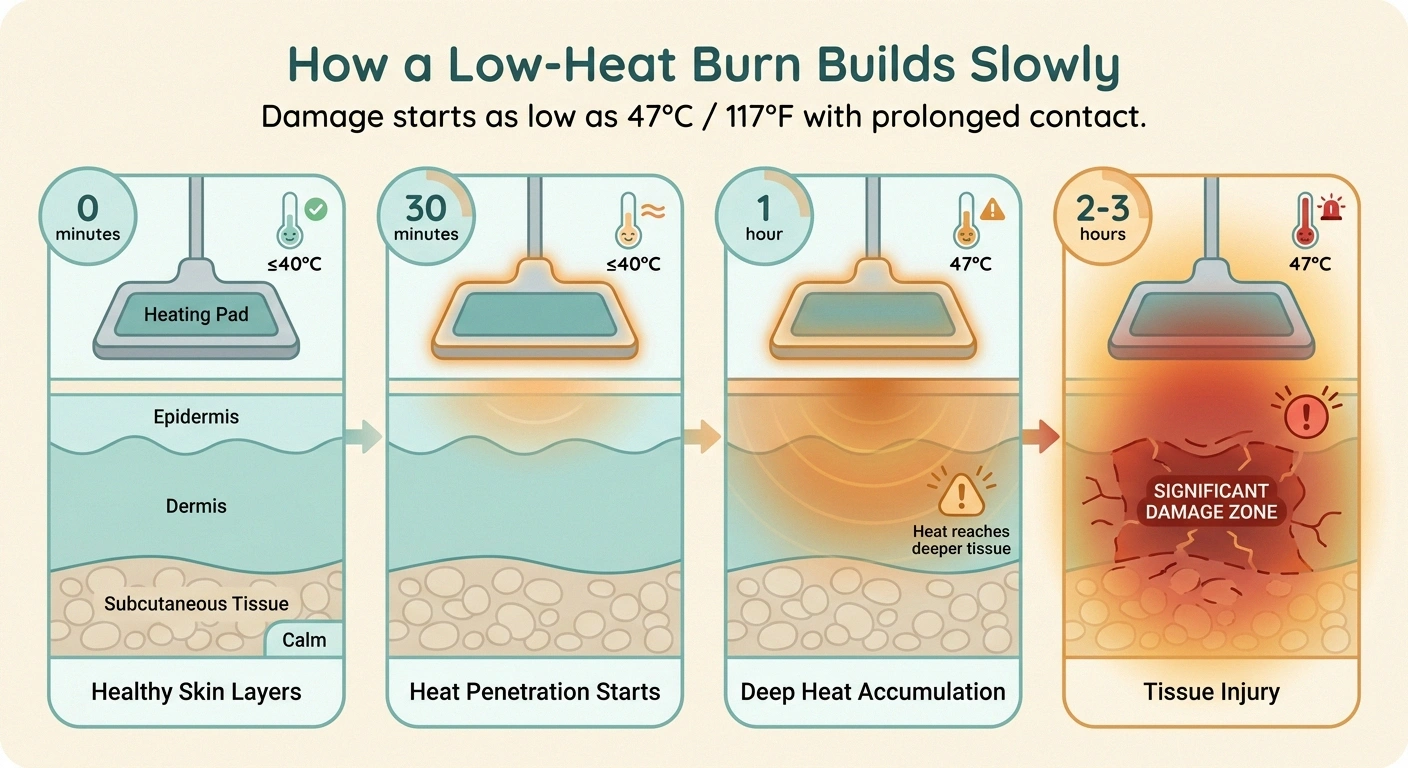
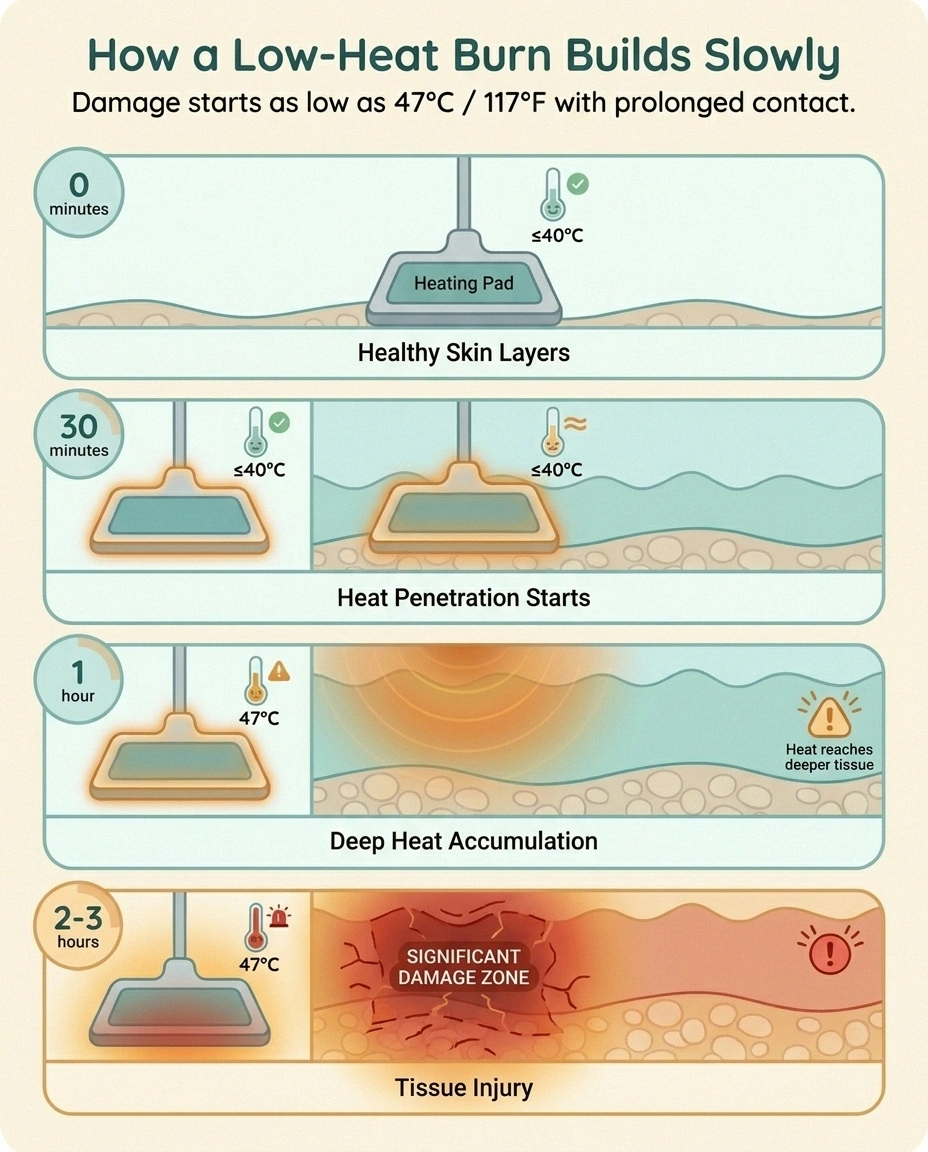
The burn itself doesn't need extreme heat. Research has documented that skin tissue can be damaged at sustained contact temperatures as low as 47°C (116.6°F) — well below what most healthy people would even describe as “very hot” — and the person experiencing it may feel nothing as it happens. Most heating pads, even on their low setting, can produce skin-contact temperatures above 47°C if pressed firmly against the body for thirty minutes or more.
The numbers around what happens when this goes wrong are sobering. In one study of 16 patients with diabetic neuropathy who suffered thermal burns from heat therapy, 44% developed infections, 6% required ICU care, and 19% required amputation. Roughly one in ten diabetic patients who burn their feet ends up needing amputation. These aren't theoretical risks. They're documented patient outcomes from exactly the scenarios this article is trying to help you avoid.
The Burn You Can't Feel: How It Happens
The mechanics are almost always the same. You set the heating pad on its low setting. You drape it over your feet or the back of your calves or wrap it around your hand. The temperature feels mild. You read, watch TV, fall asleep. Three hours later you wake up and the pad has been at the same temperature the whole time, in continuous contact with the same patch of skin.
What's been happening underneath is a slow accumulation. The first few minutes don't damage anything. After about twenty minutes, the deeper skin layers reach the heating pad's temperature. After an hour, the heat is penetrating into the tissue and starting to damage cells. After two or three hours of continuous low-grade heat, you can have a deep partial-thickness or full-thickness burn — even though the heating pad never felt scalding to a person with intact sensation.
The burn shows up as redness, blistering, or pale-and-leathery skin, often in the exact shape of the heating pad. Sometimes it's discovered in the morning. Sometimes a caregiver notices it. Sometimes it's not noticed until it gets infected days later. The combination of impaired sensation, often-poor circulation, and slowed wound healing in diabetic patients turns what would be a minor injury in a healthy person into a medical emergency.
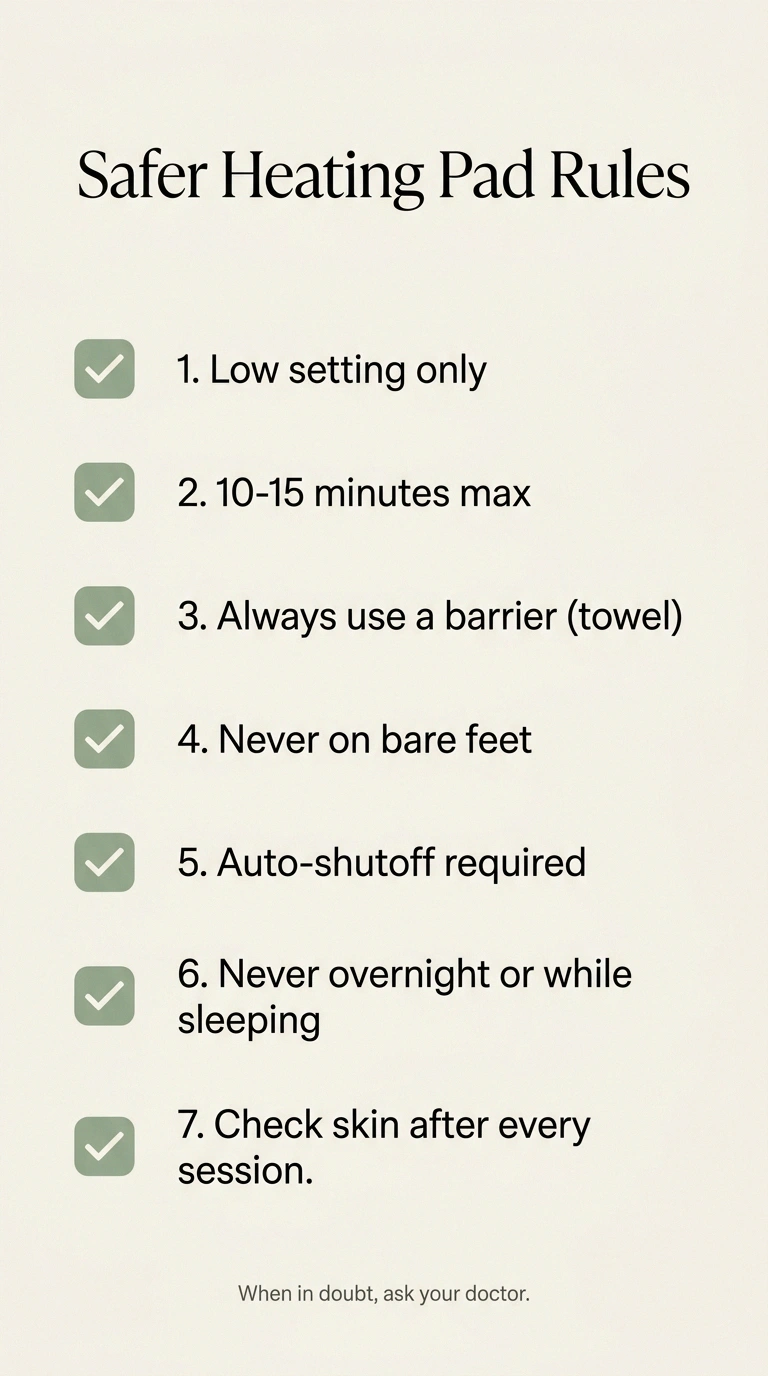
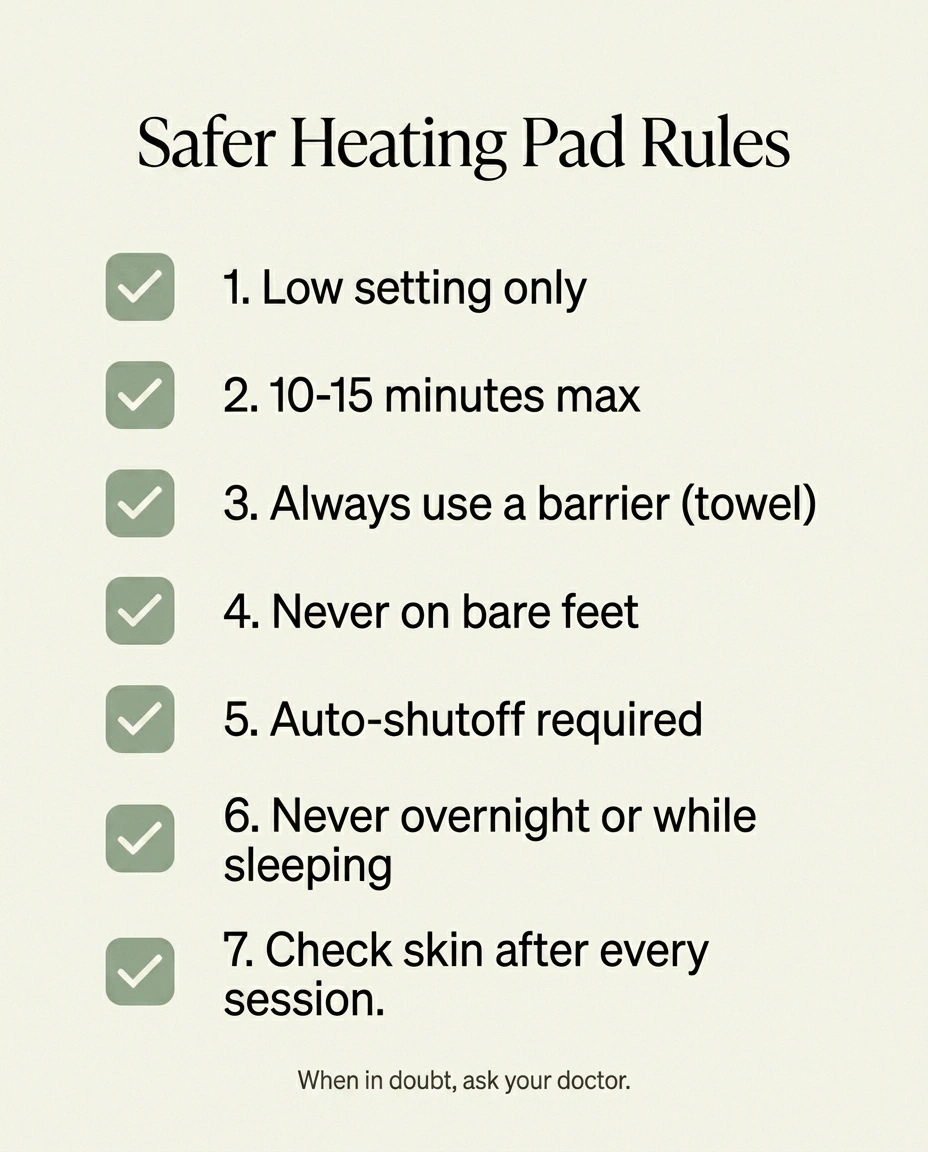
Safer Heating Pad Rules: A 7-Point Checklist
If you and your doctor have decided that you can use a heating pad — and many physicians recommend skipping them entirely for neuropathy patients, which I'll get to — these are the rules that meaningfully reduce risk.
1. Low setting only. Never medium or high. The lowest setting is more than enough heat for any therapeutic purpose, and the difference in burn risk between low and medium is significant.
2. Maximum 10-15 minutes per session. Set a timer. Don't trust your sense of how much time has passed. Some sources say 20 minutes is acceptable; for neuropathy I'd be more conservative and cap at 10. Then a full hour off before any next session.
3. Always use a barrier. A folded towel or pillowcase between the heating pad and your skin. Direct skin contact is the highest-risk configuration. A barrier reduces peak temperature and gives you something to absorb sweat (which can intensify heat conduction).
4. Never on bare feet. The feet are where most neuropathy is worst, where sensation is most compromised, and where the consequences of a burn are most severe (poor healing, infection risk, amputation risk). Heating pads on neuropathy-affected feet are the highest-risk configuration of all.
5. Auto-shutoff is mandatory. Modern heating pads should automatically turn off after a set period (usually 1-2 hours). Older pads without this feature should not be used. If your heating pad doesn't have a shutoff function, replace it with one that does — or skip it entirely.
6. Never sleep with a heating pad on. This is the single most common pattern behind serious burns. The intention is “just a few minutes to take the edge off before bed.” The reality is that fatigue and sedating evening medications send people to sleep before they remove it. If you're tempted to use heat at bedtime, use heated socks or a heated blanket on the upper body — not a pad in continuous contact with one area.
7. Check the skin after every session. Every time. Look at the area that was under the pad. Pink/red that fades within a few minutes is normal. Persistent redness, mottling, blistering, or any visible change in skin texture means stop using the pad and contact your doctor.
Body Areas to Avoid Entirely
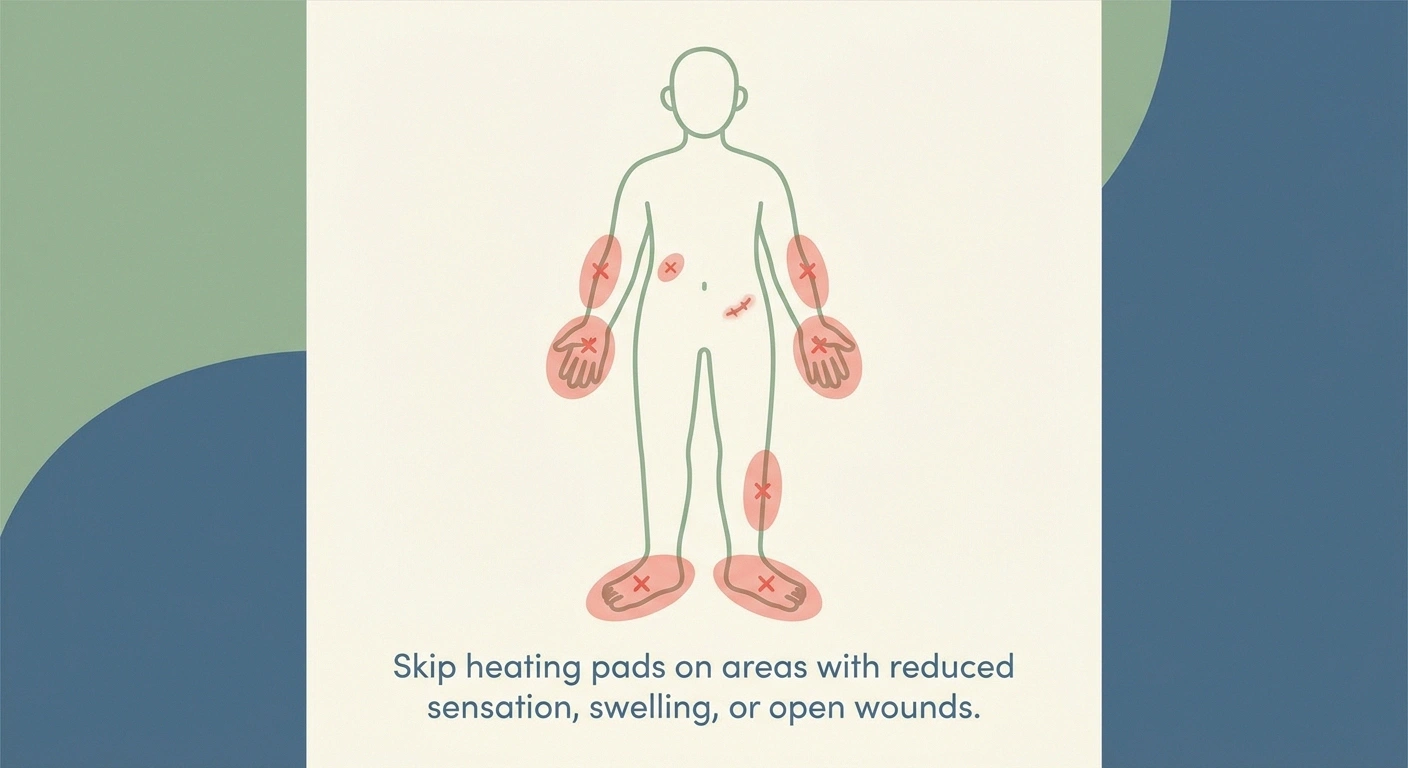
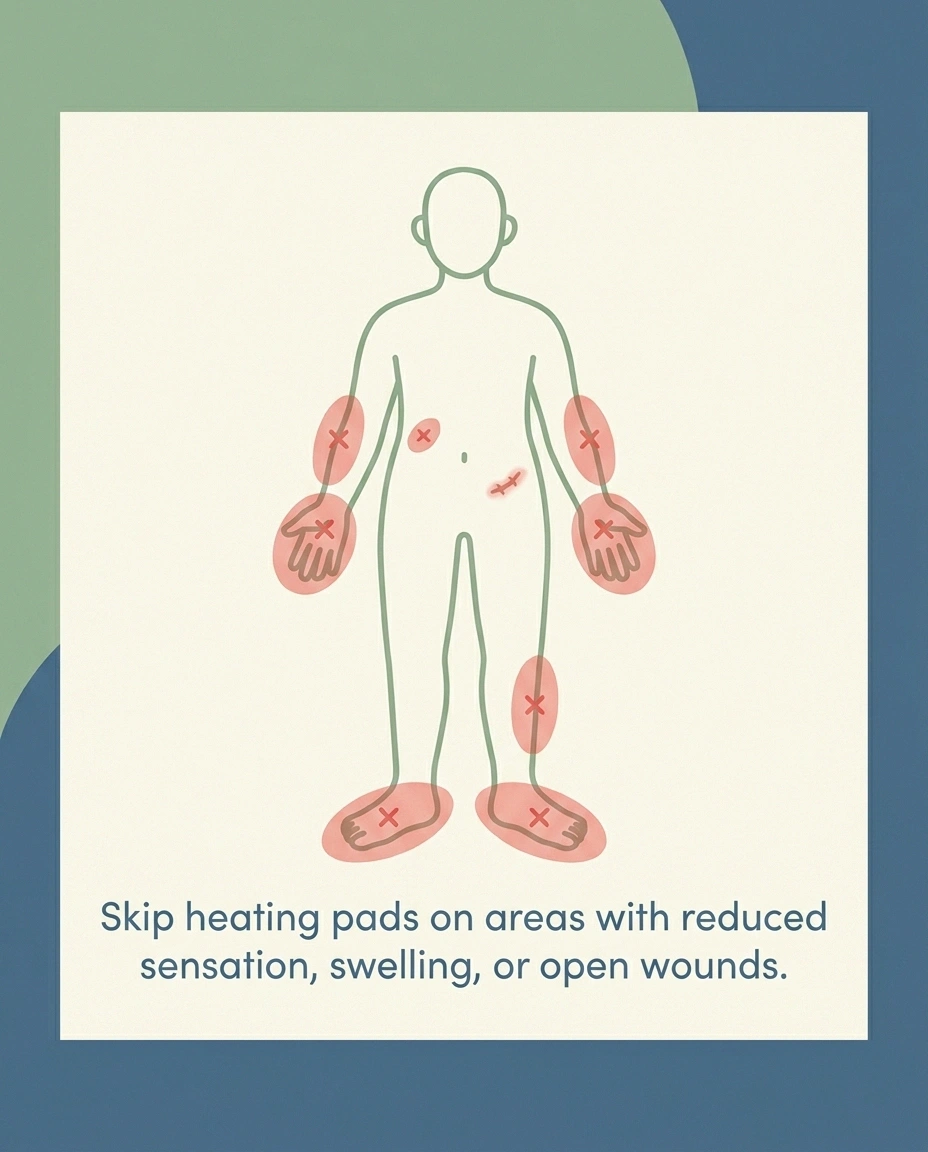
Some areas should never have a heating pad on them if you have neuropathy:
- Feet, especially the soles and toes. Most affected by diabetic neuropathy, hardest to heal if burned, highest amputation risk.
- Any area with an existing wound, ulcer, or open skin. Heat increases blood flow to fragile tissue and can accelerate breakdown.
- Swollen or edematous areas. Edema fluid conducts heat differently and changes burn dynamics.
- Areas recently treated with topical anesthetic (lidocaine cream, capsaicin) — the topical may further impair sensation.
- Areas with reduced circulation (peripheral artery disease, post-vascular-surgery sites). Reduced blood flow means less ability to dissipate heat.
The general rule: if you wouldn't notice an injury there within the first few minutes, don't put a heat source there.
Heat Alternatives That Are Safer for Numb Skin

There are gentler ways to get the comfort that heating pads provide, with substantially lower burn risk.
Heated socks and gloves with temperature regulation are generally safer than pads because the temperature is lower (designed for continuous body contact) and the contact pressure is much less than a pad pressed against you. Look for models with low/medium/high settings and use the lowest one that helps.
Warm (not hot) foot baths, with the water temperature tested by someone with intact sensation — typically a partner or family member — or with a thermometer. Aim for water at or below 95°F (35°C), and limit soaks to about 5-10 minutes. Pat dry thoroughly afterward, especially between the toes. Our guide to warm baths for neuropathy covers this in more detail.
Heated blankets on the upper body rather than the feet. The torso has more intact sensation in most peripheral neuropathy patients, and lower amputation/infection risk if a problem develops.
Warm room, layered clothing, and warm bedding as the first line. Sometimes the issue isn't that you need to apply heat — it's that the environment is too cold. Solving the environment is safer than applying point heat to numb skin.
Topical capsaicin or menthol creams for nerve discomfort. These work by a different mechanism — desensitizing the pain receptors or producing a cooling/warming sensation through specific channels — and don't carry burn risk. They're not without their own caveats (capsaicin causes a burning sensation initially that some people find intolerable), but they're not thermal burns. See our capsaicin cream guide.
Compression garments can help with the sensation of cold or discomfort without applying heat. Some patients find graded compression socks improve foot sensation without thermal risk.
When to Skip Heat and Call Your Doctor
There are situations where the answer isn't “use heat differently” — it's “don't use heat right now, and talk to your medical team about what's going on.”
Call your doctor if:
- You discover a burn mark, blister, or any unexplained skin change in an area where you've used a heating pad
- Pain or discomfort is getting consistently worse and the heating pad isn't helping anymore
- You have new swelling, redness, or warmth that doesn't fade after stopping heat
- You notice color changes — areas turning white, purple, or unusually pale
- You have a known foot ulcer or open wound on your foot that's not improving
- You're using heat to mask pain that's increasing — pain that's getting worse over weeks needs evaluation, not more heat
The general principle is that progressive nerve pain isn't something heat fixes; it's a signal that the underlying neuropathy may need attention. Heat can be part of comfort management, but it shouldn't be the only tool, and it shouldn't be a substitute for proper medical assessment.
What to Do If You Notice a Burn Mark

If you see a burn — even one that looks minor — treat it as a medical issue, not a household first-aid problem. The combination of neuropathy and any of its underlying causes (diabetes, autoimmune conditions, chemotherapy, alcohol-related nerve damage) means burns heal more slowly and infect more easily than they do in healthy patients.
- ✓ Stop using the heating pad immediately
- ✓ Do NOT pop blisters or apply home remedies
- ✓ Cover with a clean, dry dressing
- ✓ Call your doctor the SAME day (urgent for foot burns)
- ✓ Watch daily for infection: increased redness, warmth, pus, fever
Steps:
- Stop using the heating pad immediately. Don't try to “warm through” the discomfort — that's how minor burns become serious wounds.
- Don't pop blisters. The blister fluid is sterile; popping it introduces infection risk.
- Don't apply butter, oils, toothpaste, or other home remedies. Most worsen the situation.
- Cover with a clean, dry dressing if available.
- Call your doctor the same day, or go to urgent care or the ER for anything beyond a small superficial pink mark. If the burn is on your foot and you have diabetes, treat it as urgent.
- Watch for infection signs over the next several days — increased redness, warmth, pus, fever. Infection in a neuropathy-affected limb can escalate quickly.
The threshold for medical attention should be lower than it would be for a person without neuropathy. What looks like “a little blister” can hide deeper tissue damage that's not visible from the surface.
The Bigger Picture: Heat Is Comfort, Not Treatment
I want to close with something important about the role of heat in neuropathy management. Heating pads provide comfort, sometimes meaningful comfort. But major clinical guidelines, including Aetna's medical policy and a number of physician consensus statements, take the position that heating pads are not of proven therapeutic value for peripheral neuropathy itself. They don't fix nerve damage. They don't slow progression. They don't address the underlying cause.
What that means practically is that heat is best used as one tool in a broader management plan — alongside the medications your doctor has prescribed, the supplements you've discussed and added, the exercise routine that works for your situation, and the foot-care discipline that keeps you ahead of problems. Heat shouldn't be the substitute for any of those.
If you find yourself reaching for the heating pad more and more often because your other strategies aren't working, that's worth a conversation with your medical team rather than more heat sessions. Worsening symptoms generally mean something needs adjustment in the treatment plan, not more comfort measures on top of the existing one.
Our broader guide to neuropathy foot care covers the daily practices that prevent the kinds of injuries this article is warning about, and our daily foot-inspection routine is the two-minute habit that catches problems early — including burns from heating pads — before they become emergencies.
Frequently Asked Questions
Can I use a heating pad with neuropathy at all?
Some doctors say yes with strict precautions; others recommend skipping heating pads entirely for neuropathy patients because the burn risk is significant and the therapeutic value is limited. Talk with your doctor about your specific situation, especially if you have diabetes, foot ulcers, or known severe sensation loss.
What's the safest setting?
The lowest setting available, always. The temperature difference between low and medium can be the difference between safe and burning. There's no neuropathy benefit to higher settings that justifies the risk.
How long is safe?
Maximum 10-15 minutes per session, with at least an hour between sessions, never overnight, never while sleeping. A timer is essential — don't trust your sense of elapsed time.
Should I put a towel between the pad and my skin?
Yes, always. A folded towel or pillowcase reduces peak temperature, absorbs sweat, and gives a margin of safety if the pad runs warmer than expected.
Why is it especially dangerous on feet?
Feet are typically where neuropathy is worst (sensation most impaired), where circulation is often reduced (slower heat dissipation, slower healing), and where the consequences of a burn are most severe — diabetic foot burns have a documented amputation rate around 19% in some studies. Heating pads on feet are the highest-risk configuration.
Can I use a heating pad on my back if I have foot neuropathy?
If your back has normal sensation, the risk is lower than for affected areas. Use standard precautions — low setting, short sessions, barrier between pad and skin, never while sleeping. Some patients with peripheral neuropathy do have intact back sensation, but check yours before assuming.
Are infrared heating pads safer?
Infrared pads work by a different heating mechanism but still produce surface temperatures that can burn impaired skin. The same precautions apply — low setting, time limits, barriers, never on feet, never overnight.
What about heated blankets?
Heated blankets distribute heat over a larger area at lower temperatures than pads, which is generally safer. The same overnight risk applies — auto-shutoff is mandatory, and on the body (not feet) is safer than blankets that cover the feet.
What about microwaved heat packs (rice bags, etc.)?
These can actually be more dangerous than electric pads because temperature isn't regulated — they start very hot and cool gradually. If you use them, microwave for a shorter time than the package suggests, test the temperature against your forearm (assuming the forearm has intact sensation), and always use a barrier. Limit to 10 minutes maximum.
What if I notice a small burn the morning after?
Treat it as a medical issue, not first aid. Stop using the heating pad, cover it with a clean dressing, and call your doctor the same day. The combination of slower healing and infection risk with neuropathy means even small burns can become serious. Diabetic patients with foot burns should treat as urgent.


