If you've been on duloxetine (Cymbalta) for chemotherapy-induced nerve pain and it's helping some — but not enough — you may have come across a newer drug name in oncology and pain forums: mirogabalin. It's been making the rounds, especially in conversations about CIPN (chemotherapy-induced peripheral neuropathy), and patients want to know: Is this the same thing as gabapentin? Is it better than duloxetine? And the most important question for most of us reading from the United States — can I even get it?
I've spent the last few weeks digging through the research, the clinical trial registries, and the patient stories. I want to share what I found in plain language, because some of what's being said online is overstated and some of it is sold short. Mirogabalin is a real, interesting drug. It's also not what most US patients hope it is — at least not yet.
Let's walk through it together.
What Mirogabalin Actually Is
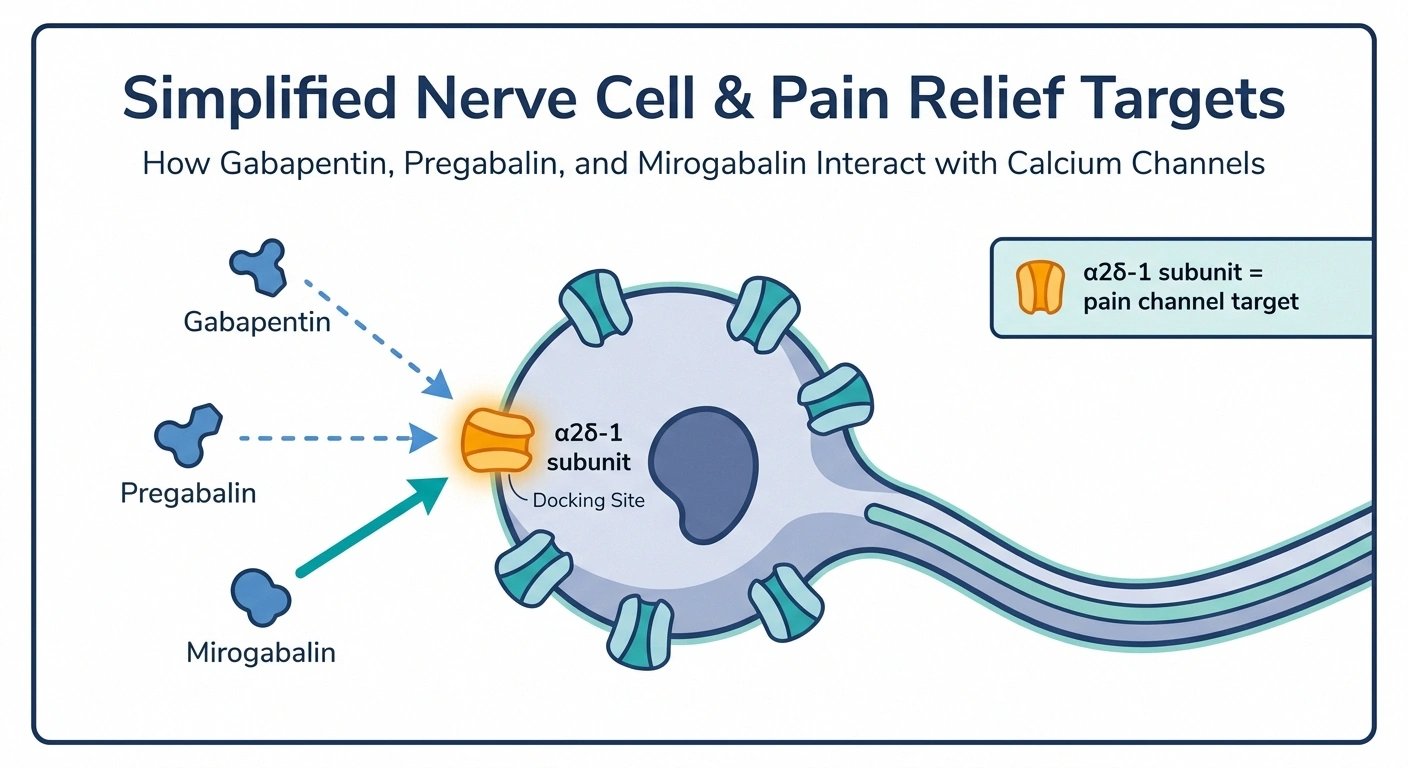
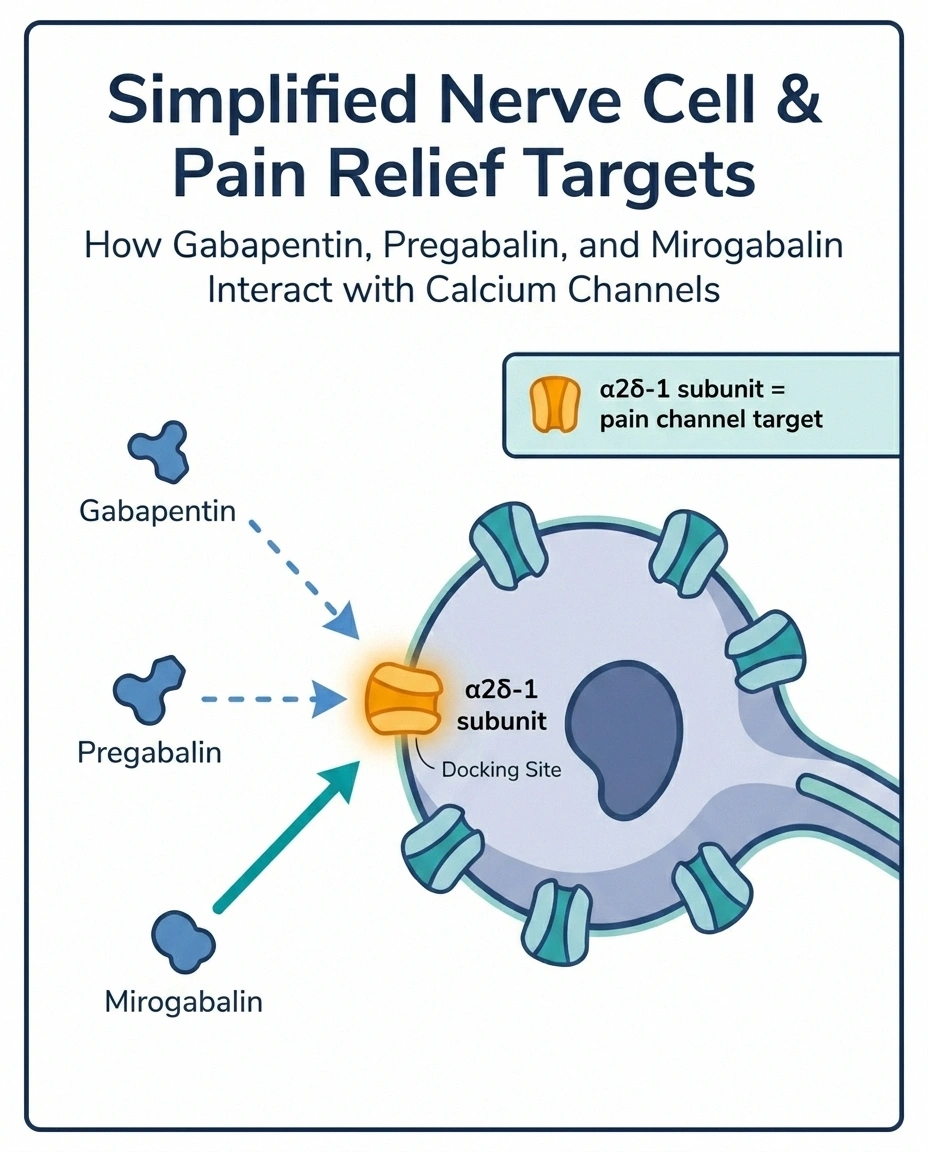
Mirogabalin (brand name Tarlige in Japan) is part of the same drug family as gabapentin and pregabalin (Lyrica). All three are called “gabapentinoids.” That's a fancy way of saying they all work on the same target in your nervous system: a tiny protein piece called the α2δ-1 subunit, which sits on calcium channels in nerve cells.
When nerves are damaged — by chemotherapy, by diabetes, by shingles, by any number of insults — they tend to fire wildly and inappropriately. Gabapentinoids quiet those channels. The nerves stop screaming quite so loudly. The result, for many people, is less burning, less tingling, less of that electric-shock pain that wakes you up at 2 a.m.
The difference with mirogabalin is in how tightly it grabs onto that target. Researchers found that mirogabalin binds more selectively to the α2δ-1 subunit (the one most involved in pain) and lets go more slowly. In theory, that should mean better pain relief with fewer of the foggy, drowsy side effects that come with pregabalin.
That's the theory. The real world is a little more complicated.
Where Mirogabalin Is Approved (And Where It Isn't)
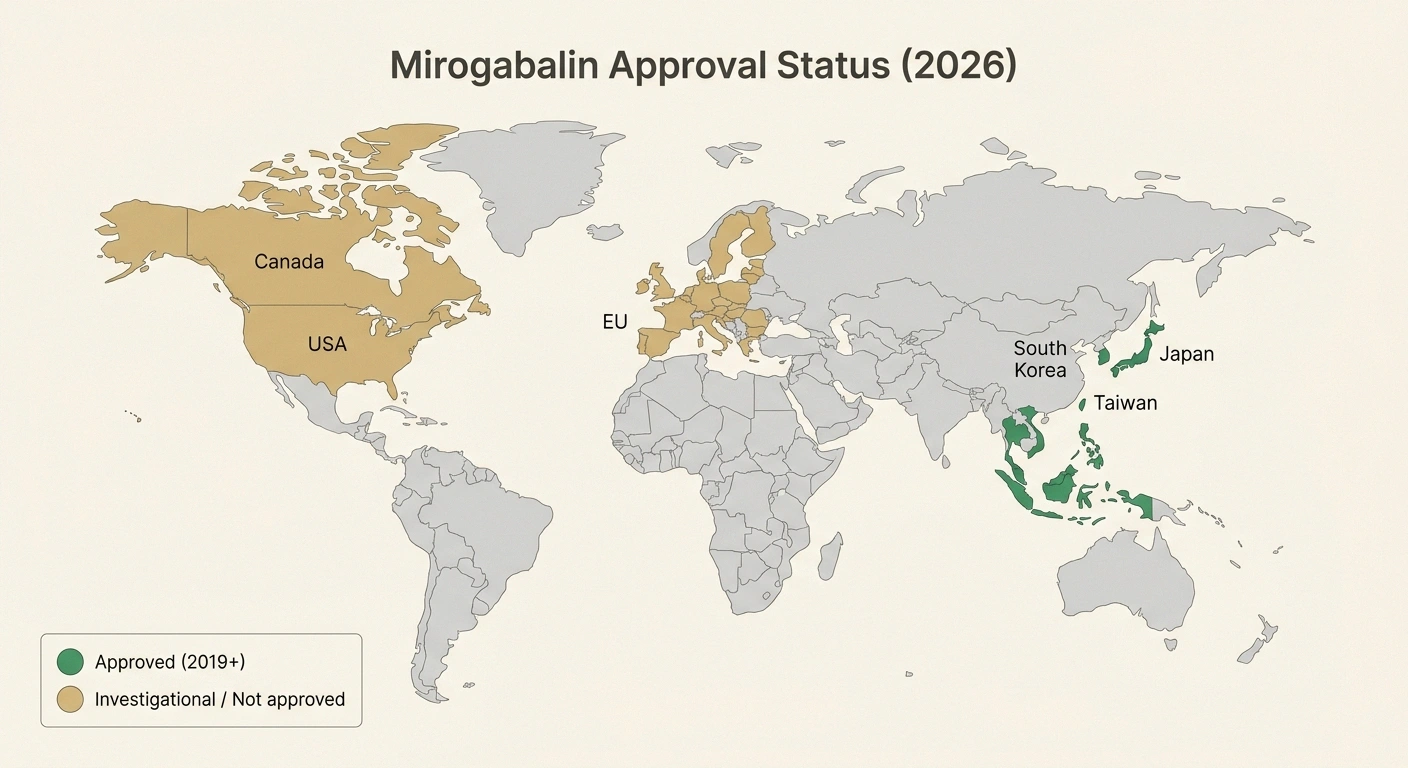
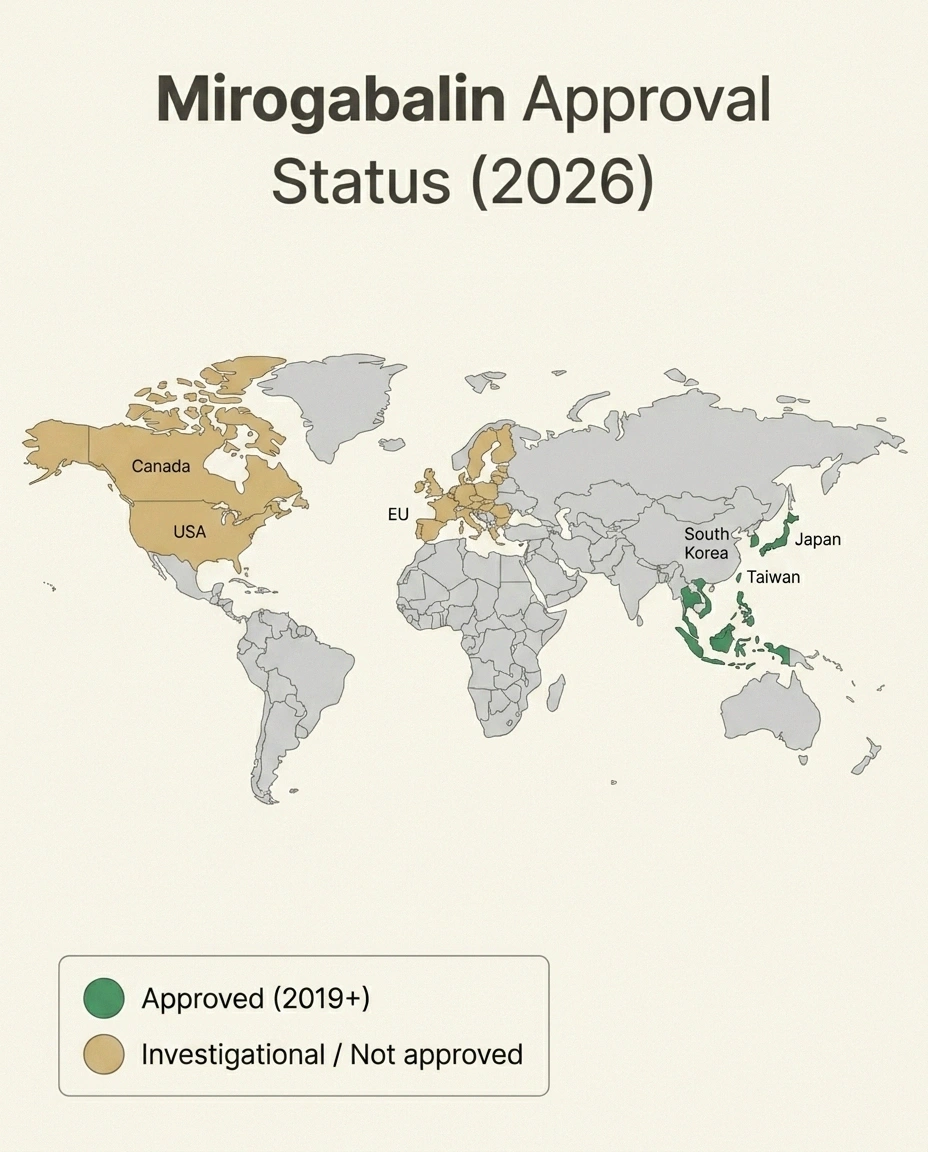
This is where I want to slow down and be very honest, because I see a lot of confusion online. Mirogabalin is currently approved in Japan (it has been since 2019), and more recently in some other Asian countries. Japan uses it for several types of peripheral neuropathic pain, including diabetic peripheral neuropathy and post-herpetic neuralgia.
It is not FDA-approved in the United States. As of 2026, you can't walk into a US pharmacy and pick up mirogabalin. Your insurance won't cover it. Most US doctors have never prescribed it. The clinical trials that would support a US approval — including head-to-head studies with duloxetine — are either ongoing or recently completed, but the drug hasn't crossed the FDA finish line for any US indication.
What that means practically: if you live in the US and want to try mirogabalin, your realistic options today are very limited. You might find it through a clinical trial (more on that in a minute). You might have a complicated international pharmacy situation if you travel. But this isn't a “ask your doctor for a prescription tomorrow” drug for American patients yet — and any website telling you otherwise is selling you something.
So why am I writing about it? Because the research is genuinely interesting, because patients with severe CIPN deserve to know what's in the pipeline, and because some of the side-by-side comparisons with duloxetine are starting to come out and they matter.
A Quick Refresher on Duloxetine for CIPN
Before we compare, let's make sure we're on the same page about duloxetine. If you've already taken it, feel free to skip down a paragraph or two.
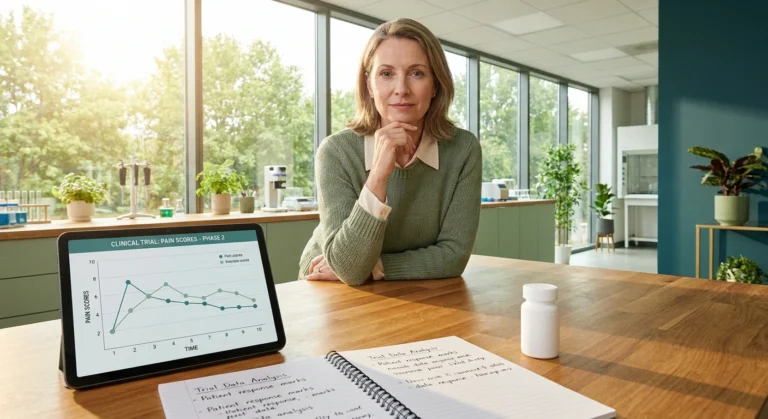
Duloxetine (sold as Cymbalta and as a generic) is the only medication currently recommended by the American Society of Clinical Oncology (ASCO) for already-established chemotherapy-induced peripheral neuropathy. That recommendation is in their 2020 guideline update on CIPN management. It's based largely on a 2013 randomized trial published in JAMA showing that duloxetine produced about a 1-point greater reduction in pain (on a 0–10 scale) compared to placebo after 5 weeks of treatment.
One point may sound modest, and honestly, it is. CIPN is brutally hard to treat, and even the best-supported drug we have only takes the edge off for many patients. But for some, that one point of relief is the difference between sleeping through the night and not.
Duloxetine isn't a gabapentinoid. It's an SNRI — a serotonin-norepinephrine reuptake inhibitor — which means it works on different brain and spinal cord chemistry to dampen pain signals. Common side effects include nausea (especially in the first week or two), dry mouth, fatigue, decreased appetite, and constipation. Stopping it abruptly can cause a withdrawal-like discontinuation syndrome, so it should always be tapered.
If you want a deeper dive on duloxetine specifically, I wrote a full piece on it at Duloxetine (Cymbalta) for Neuropathy that walks through dosing, what to expect, and how to know if it's working.
What the Research Says About Mirogabalin for CIPN
Now let's look at what we actually know about mirogabalin in chemo-related nerve pain. I want to be careful here — most of the evidence is from Japan, the studies aren't enormous, and the gold-standard head-to-head versus duloxetine trial results aren't fully published yet at the time I'm writing this.
The most important study so far is called the MiroCIP trial, published in BMC Cancer in late 2023. It was a single-arm prospective study of mirogabalin in CIPN patients. “Single-arm” means everyone got the drug — there was no placebo group — so the comparison was to historical data from earlier duloxetine trials. The headline finding: mirogabalin's effect on pain looked comparable to what duloxetine produced in its phase 3 trial. The two drugs landed in similar territory for pain reduction.
Another important set of findings comes from a study in pancreatic cancer patients receiving chemotherapy, which compared mirogabalin to pregabalin (the older, FDA-approved gabapentinoid). In that study, mirogabalin produced a significantly higher rate of CIPN improvement than pregabalin did. So at least within the gabapentinoid family, mirogabalin appears to be a step forward.
A separate Japanese study focused specifically on taxane-induced CIPN — the kind that comes from drugs like paclitaxel and docetaxel, often given for breast cancer and other cancers — and found mirogabalin to be effective in that population too.
And there's a fascinating case report (published in Case Reports in Oncology) describing a patient with severe eribulin-related CIPN who got meaningful relief from a combination of mirogabalin and duloxetine — using both drugs together. Because the two drugs work through different mechanisms, the authors argued that combining them may produce additive or synergistic effects without overlapping toxicities. That's still investigational, not standard practice, but it's the kind of idea that suggests these drugs aren't competitors so much as potential teammates.
The big study to watch is a randomized controlled trial out of Pusan National University in South Korea (registered as NCT06711978), which is directly comparing mirogabalin to duloxetine for CIPN pain reduction. The primary data collection wrapped up in 2025; the full peer-reviewed results will be the first true head-to-head comparison and should land sometime this year or next.
Side-by-Side: How They Compare on Paper
Here's how the two drugs stack up across the things patients usually care about most:
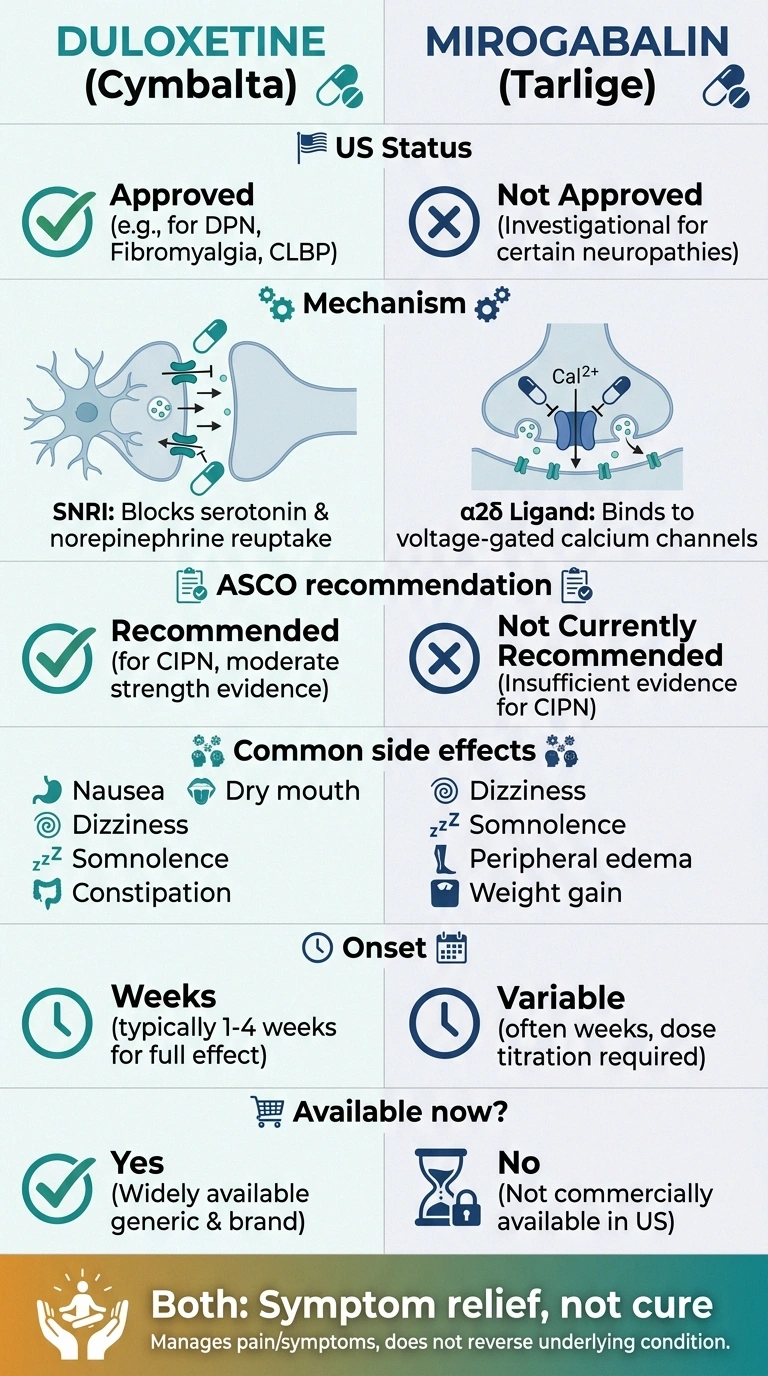
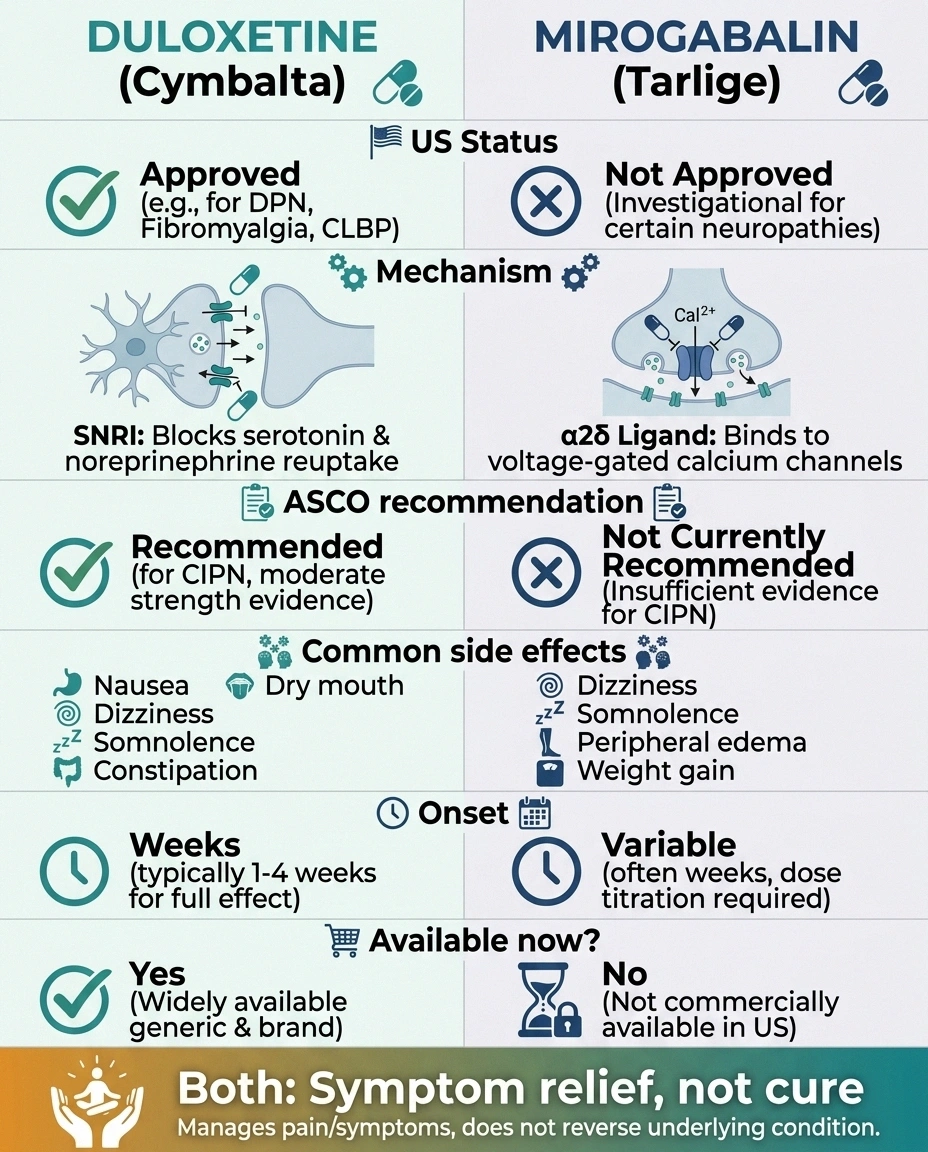
- Approval status (US): Duloxetine is FDA-approved and easy to get. Mirogabalin is not FDA-approved.
- ASCO recommendation for CIPN: Duloxetine is the only recommended drug. Mirogabalin is not mentioned in current US guidelines.
- Mechanism: Duloxetine works on serotonin and norepinephrine in pain pathways. Mirogabalin works on calcium channels at nerve endings. Very different gears.
- Onset of relief: Both typically take 1–4 weeks to show effect. Neither is a quick-acting painkiller.
- Common side effects: Duloxetine — nausea, dry mouth, fatigue. Mirogabalin — sleepiness, dizziness, mild weight gain, sometimes ankle swelling.
- Sleep impact: Mirogabalin often makes people sleepy (which can be helpful if pain wrecks your sleep, or unhelpful if you're already foggy). Duloxetine is more activating for some, sedating for others.
- Discontinuation: Duloxetine has a real discontinuation syndrome — must be tapered. Gabapentinoids should also be tapered to avoid rebound.
- Cost in the US: Duloxetine generic is usually inexpensive. Mirogabalin isn't realistically available.
If you're outside the US (Japan, much of Asia, parts of Europe where it's reaching) and have the choice, the conversation is more interesting. Inside the US in 2026, for almost everyone reading this, duloxetine is the practical option and mirogabalin is something on the horizon.
Where Mirogabalin Might Fit In
Let's say mirogabalin does eventually get FDA approval (which is not guaranteed — drug development is a tough road). Where would it fit in the CIPN toolkit? Here's my read of the research so far:
For people who haven't responded to duloxetine. Because mirogabalin works through a different mechanism, it's a reasonable next try when SNRI therapy isn't enough. Some patients respond better to gabapentinoid mechanics than to serotonin-noradrenaline modulation. Your nervous system has its own preferences.
For people who couldn't tolerate duloxetine's side effects. If you tried Cymbalta and the nausea or dry mouth or mood changes were too much, having another mechanistically distinct option matters.
For people already on pregabalin who want something more selective. Mirogabalin's tighter binding to the pain-related α2δ-1 subunit (versus pregabalin's broader binding) is the theoretical reason it may cause less of the foggy, sedated, “out of it” feeling some people get on Lyrica.
Possibly in combination. The case report I mentioned above hints that mirogabalin and duloxetine together may be more powerful than either alone — without overlapping toxicities, since they work on completely different parts of the pain pathway. That's a possibility researchers are watching closely.
What it's not: a cure. A nerve regenerator. A magic bullet. It's a symptom-management medication, like the rest of the gabapentinoid family, and CIPN treatment in 2026 is still very much a “best available” rather than “satisfying” situation.
The Drugs Already on Your Doctor's Shelf
While we wait for newer options, the existing toolkit matters. Talking with your oncologist or neurologist about CIPN should include conversations about:
- Duloxetine — the first-line option per ASCO guidelines
- Gabapentin — widely used off-label for CIPN despite weaker evidence, often because it's cheap and tolerated
- Pregabalin (Lyrica) — older sibling of mirogabalin, FDA-approved for some neuropathies
- Tricyclic antidepressants like amitriptyline or nortriptyline — older but still useful for some patients
- Topical agents like capsaicin or lidocaine patches — focal relief without systemic side effects
You can read more about how these compare in Chemo-Induced Neuropathy (CIPN) and the broader landscape in Neuropathy Treatments Compared and Ranked by Evidence. If you're interested in the pipeline of newer drugs being developed for nerve pain — including mirogabalin and others — I keep a running guide at New Neuropathy Treatments in 2026.
How to Have the Mirogabalin Conversation With Your Doctor

If you do want to bring this up with your oncologist or neurologist — and there are good reasons to, especially if you're at a major academic medical center — here are some specific things worth asking:
- “Am I a candidate for any CIPN clinical trial in this area?” Trials are how US patients access drugs like mirogabalin legally and safely. ClinicalTrials.gov is the registry; you can search by condition, location, and trial status.
- “Is duloxetine the best fit for my situation, or should we consider other agents first?” The “best” drug depends on your other medications, your other conditions (depression, anxiety, kidney function, sleep issues), and your tolerance for specific side effects.
- “If duloxetine doesn't help enough, what's our plan B?” Knowing the next step ahead of time saves weeks of “wait and see.”
- “Are we addressing the non-medication side of CIPN too?” Things like duloxetine plus physical therapy, plus appropriate supplements (acetyl-L-carnitine has some evidence, alpha-lipoic acid has some), plus exercise during chemo, plus cold therapy during certain infusions, plus addressing sleep and mood. Medication alone is rarely the whole answer.
You may also want to bring a short symptom diary. Tracking your pain on a 0–10 scale before and after starting a new medication is the single most useful thing patients can do to help their doctors make decisions. I keep a simple template in Neuropathy Symptom Diary: What to Track Daily.
What I Hope You Take Away

Three things, if nothing else:
- Mirogabalin is real progress in gabapentinoid design — selective binding, slower dissociation, potentially fewer side effects than older drugs in the family.
- It's not available in the US outside clinical trials. Promises of overseas mail-order are not safe routes.
- Duloxetine remains the right first step for CIPN in the US, with several second-line and combination strategies if it isn't enough.
First, mirogabalin is a real drug with real evidence, particularly in CIPN, and it represents genuine progress in how researchers are designing gabapentinoids. The selective binding and the slower dissociation aren't marketing — they're actual pharmacology that may translate into a better side-effect profile.
Second, it's not yet available in the United States, and the most likely path for an American patient to access it in the next few years is through a clinical trial. Be wary of online pharmacies promising mirogabalin from overseas — that's not a safe or reliable path.
Third, duloxetine remains the right starting point for CIPN pain in the US per current oncology guidelines. If you haven't tried it and you're suffering, that's the conversation to have first. If you've tried it and it didn't work or didn't agree with you, there are other options now and there will be more soon — including, eventually, this newer family of selective gabapentinoids.
The pace of research in nerve pain is finally picking up after decades of relative quiet. Mirogabalin is one of several drugs I'm watching closely (others include cebranopadol, pilavapadin, and a class of Nav1.7/Nav1.8 sodium-channel blockers that are in late-stage trials). I'll keep you updated as the head-to-head data lands.
In the meantime — be patient with yourself. CIPN is one of the hardest forms of nerve pain to treat, and finding the right combination of medication and lifestyle support often takes several rounds of trying things. You're not failing. The system is just slow to catch up to your suffering. We're getting there.
Frequently Asked Questions
Is mirogabalin available in the United States?
No, not as of 2026. Mirogabalin is approved in Japan and some other Asian countries, but it has not received FDA approval in the United States. It is not stocked by US pharmacies, and US insurance plans do not cover it. The most realistic way for a US patient to access mirogabalin is through participation in a clinical trial.
Is mirogabalin the same as gabapentin or pregabalin (Lyrica)?
It's in the same family. All three are called gabapentinoids and they work on the same general target — the α2δ subunit of voltage-gated calcium channels in nerve cells. The differences are in how selectively they bind, how long they stay bound, and what their side-effect profile looks like in practice. Mirogabalin was designed to bind more selectively to the pain-related part of the target, which in theory should mean more pain relief with less of the cognitive fogginess that some people get on pregabalin.
How does mirogabalin compare to duloxetine for chemo neuropathy?
The available evidence — which is mostly from Japan and mostly single-arm or smaller studies — suggests mirogabalin produces pain reductions comparable to what duloxetine has produced in its older trials. A direct head-to-head randomized controlled trial comparing the two for chemotherapy-induced peripheral neuropathy was completed in 2025, and the full results are expected to be published in 2026 or 2027. Until then, the comparison is largely indirect.
Can mirogabalin be taken together with duloxetine?
There's an interesting case report describing a patient with severe eribulin-related CIPN who responded well to the combination, because the two drugs work through different mechanisms and don't overlap meaningfully in their side effects. This is not standard practice and would only be considered under careful specialist supervision. It is something a small number of pain specialists are watching closely as a future option.
What are the most common side effects of mirogabalin?
Based on Japanese post-marketing data and clinical trial reports, the most common side effects are sleepiness (about 12 percent of users), dizziness (about 9 percent), mild weight gain, and occasional swelling in the ankles. The side-effect profile is generally similar to pregabalin's, though several head-to-head studies have suggested mirogabalin may cause less sedation and cognitive fogginess.
If I'm on duloxetine and it's helping but not enough, what should I do next?
Talk to the doctor managing your CIPN. Options include increasing the duloxetine dose (if tolerated), adding a complementary medication like gabapentin or a topical agent, adding non-pharmacologic strategies like physical therapy or appropriate supplements, or exploring clinical trial participation. The right next step depends on your specific situation, your other medications, and what side effects you can tolerate. Adding another drug or switching drugs is a clinical decision, not a guess from the internet, but knowing the options helps you have a better conversation.
Will mirogabalin be FDA approved soon?
That's hard to predict. As of 2026, the manufacturer (Daiichi Sankyo) has not publicly announced an active FDA submission, and the drug's path to US approval would require dedicated US clinical trials. Several head-to-head and indication-specific studies are underway internationally, but a US approval is likely still years away if it happens at all. In the meantime, other novel drugs for nerve pain are moving through the US FDA pipeline more rapidly — I cover those in my New Neuropathy Treatments 2026 guide.
Are there other clinical trials I should know about for CIPN?
Yes — ClinicalTrials.gov is the official US registry and you can search by your specific cancer type, your chemotherapy regimen, and your geographic area. Major cancer centers (NCI-designated comprehensive cancer centers) often have CIPN-specific trials. Your oncology team should be able to help you identify any that fit your situation. The Foundation for Peripheral Neuropathy also maintains a curated list of neuropathy trials worth bookmarking.