
The first time it happened to me, I thought I'd left my phone on vibrate against my leg. I reached for it — and there was no phone. The buzzing was coming from inside me.
If you've felt this — a strange humming, trembling, fluttering, or “phone-vibrating” sensation deep inside your body, with nothing visibly moving on the outside — you are not imagining it, and you are not alone. Internal tremor is a real, documented symptom. It shows up in long COVID, in fibromyalgia, in Parkinson's disease, in multiple sclerosis, in essential tremor — and increasingly, researchers are seeing it pop up in people with small fiber neuropathy and other forms of nerve damage.
I want to walk you through what we know, what we don't, what your doctor should check for, and what you can actually try tonight to make it quieter. Because the worst part of this symptom — beyond how strange it feels — is the fear that something is deeply wrong and nobody is taking it seriously.
What “Internal Tremor” Actually Means
Internal tremor is a sensation of trembling, vibrating, buzzing, or fluttering felt inside the body, without any visible shaking that another person could see. Some people describe it as a phone on silent mode buried inside their chest, abdomen, or limb. Others describe it as a humming bee, a low electrical current, or the feeling you get just after a near-miss in traffic — that adrenaline-shaky feeling — but for no reason and lasting much longer.
It can be focal (limited to one area like the chest, abdomen, or a single limb) or it can feel like it's running through the whole body. It can come on suddenly or build slowly. It can be constant, or it can come in waves over hours or days.
This is different from essential tremor, the most common adult movement disorder, which produces visible hand or head shaking. It's also different from Parkinsonian tremor, the classic rest tremor of Parkinson's disease, which is visible to others. Internal tremor is the version you can feel but no one else can see.
That invisibility is part of why it's so distressing — and historically, why doctors sometimes dismissed it. That's beginning to change as more research documents the symptom.
Why It Happens — The Nerve Connection
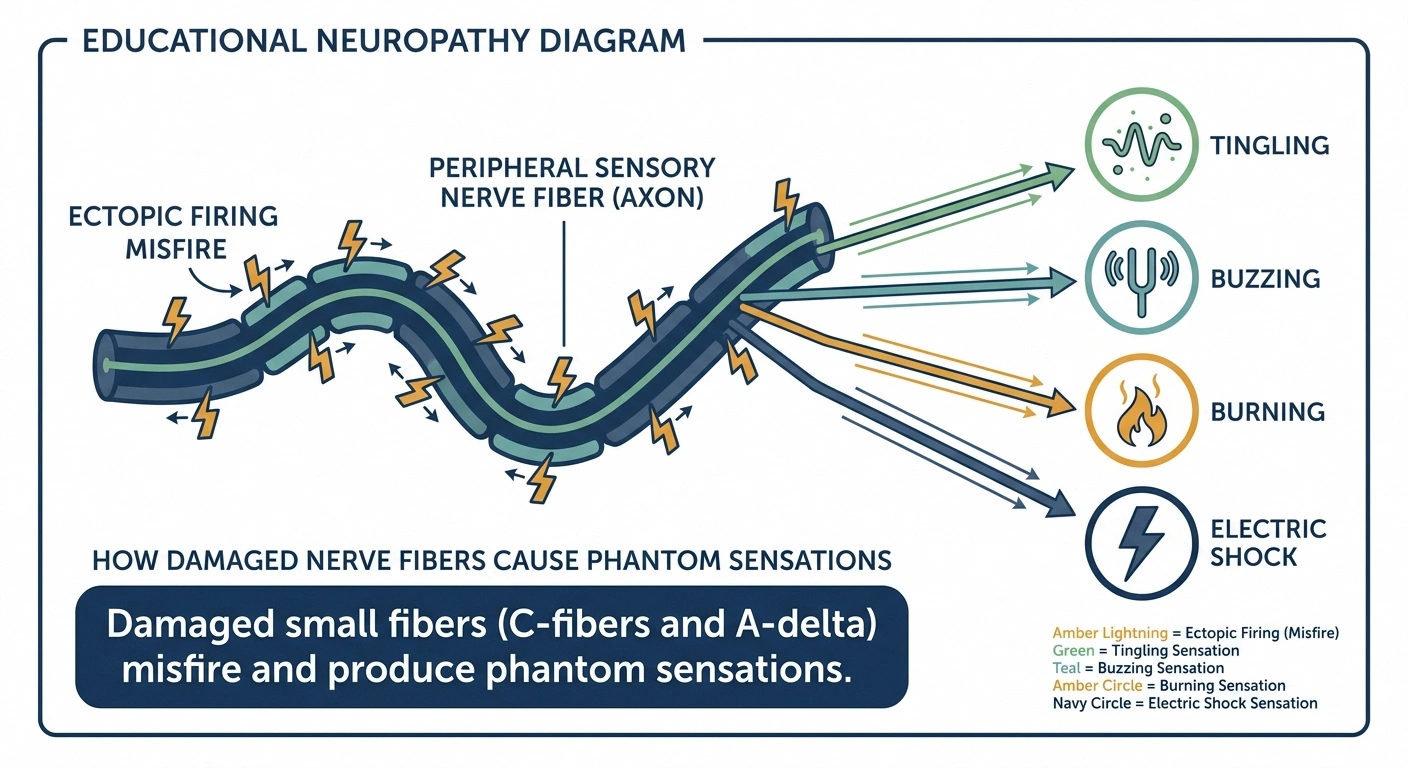
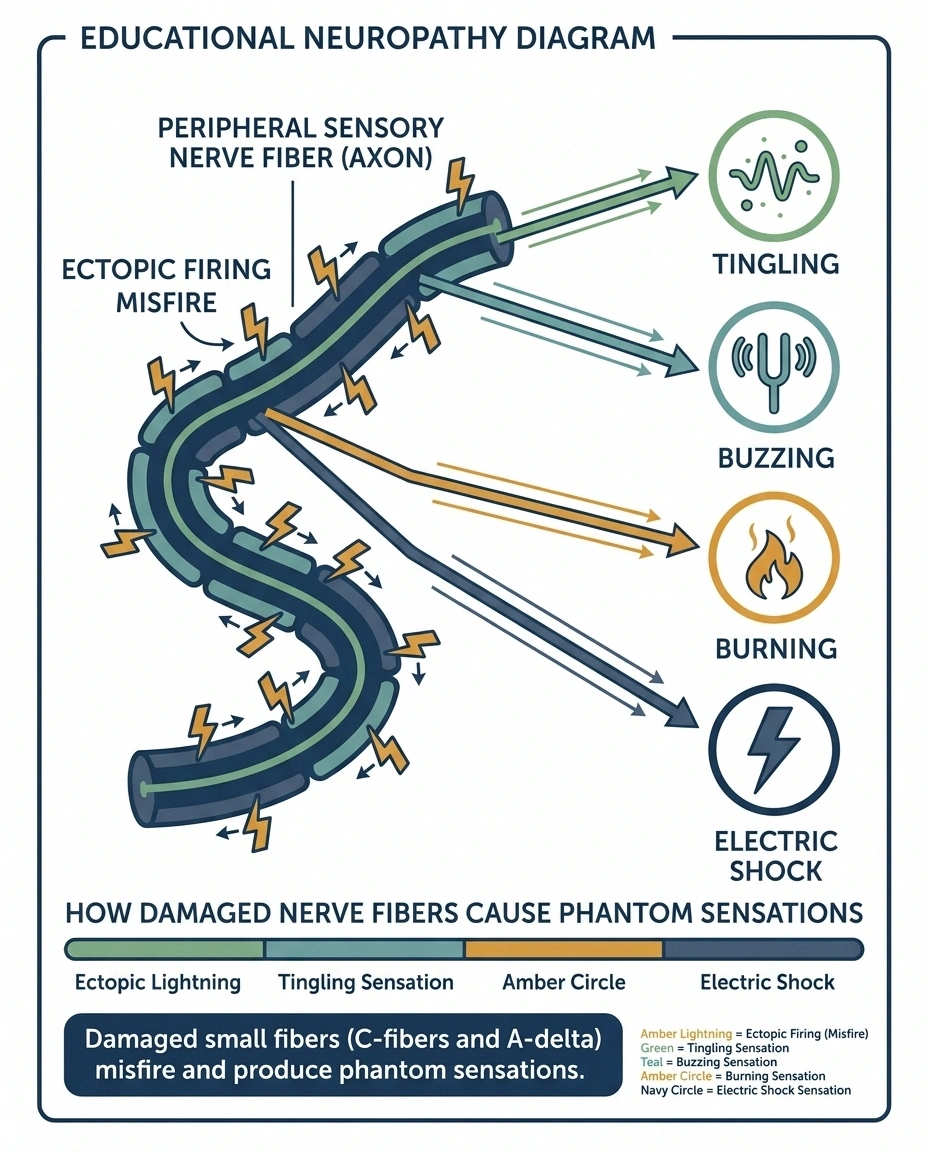
To understand internal tremor in neuropathy, you have to know a little bit about how nerves can misbehave. When small sensory fibers (the C-fibers and A-delta fibers that handle pain, temperature, and autonomic functions) are damaged or irritated, they don't just go silent. They often start firing wildly and inappropriately. That ectopic firing is what produces phantom sensations — pins-and-needles when nothing is touching you, electric shocks out of nowhere, burning feet on a cool floor, and sometimes a humming or buzzing that feels like motion inside the body even though nothing is moving.
In other words, internal tremor in neuropathy is the same family of phenomena as paresthesia, formication (the bug-crawling sensation), and electric shock sensations. They're all forms of misfiring sensory nerves producing an experience that has no external cause.
A 2026 paper in Neurology International documented internal tremor as one of the most common — and underrecognized — manifestations of small fiber neuropathy and autonomic dysfunction in long COVID patients. A separate 2023 characterization study found that internal tremors and vibration symptoms were also unusually common in people with fibromyalgia, multiple sclerosis, hypermobility syndromes, and post-viral states, where small-fiber involvement is increasingly suspected.
The takeaway: if your nerves are damaged or irritated, your nervous system can generate the feeling of motion without any actual motion. Internal tremor is one specific way that misfire shows up.
Other Causes — What Else Could Be Driving It
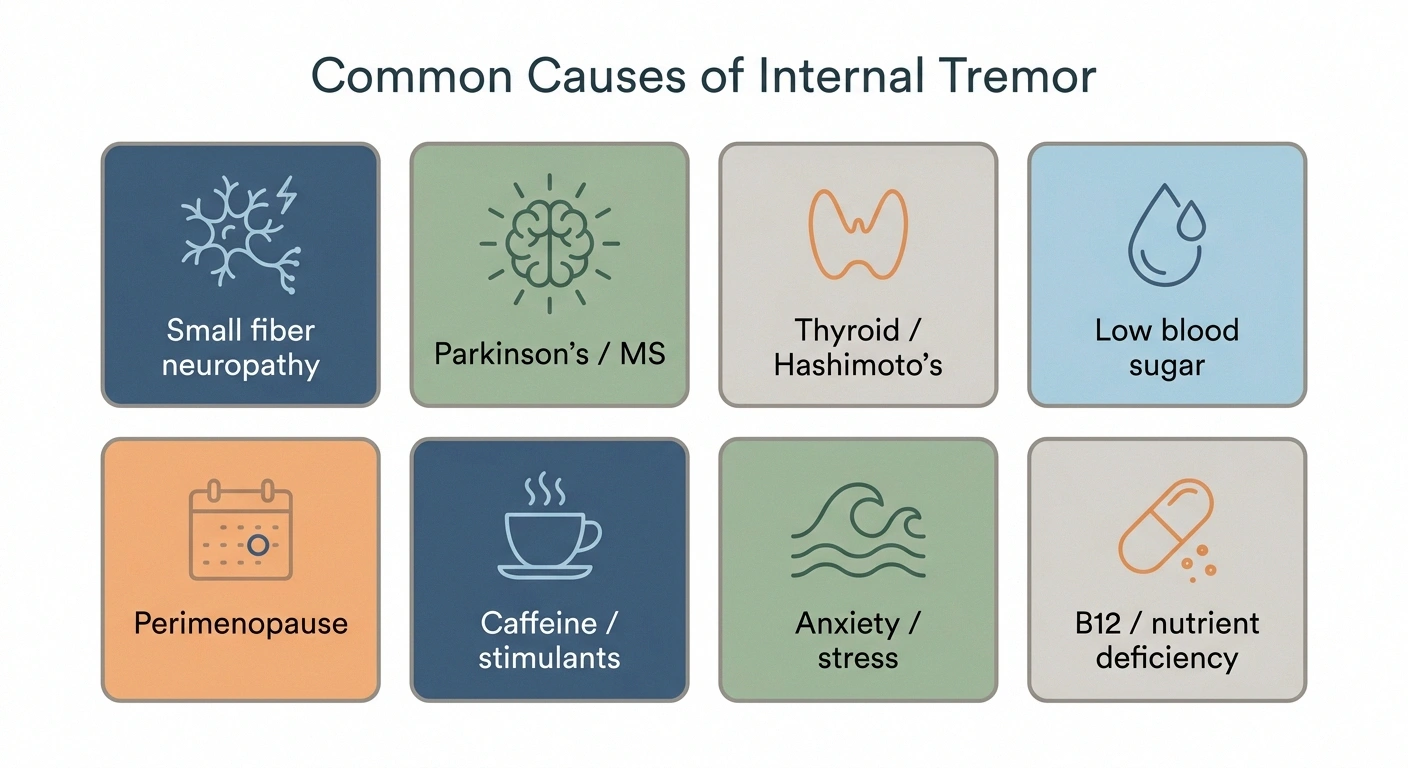
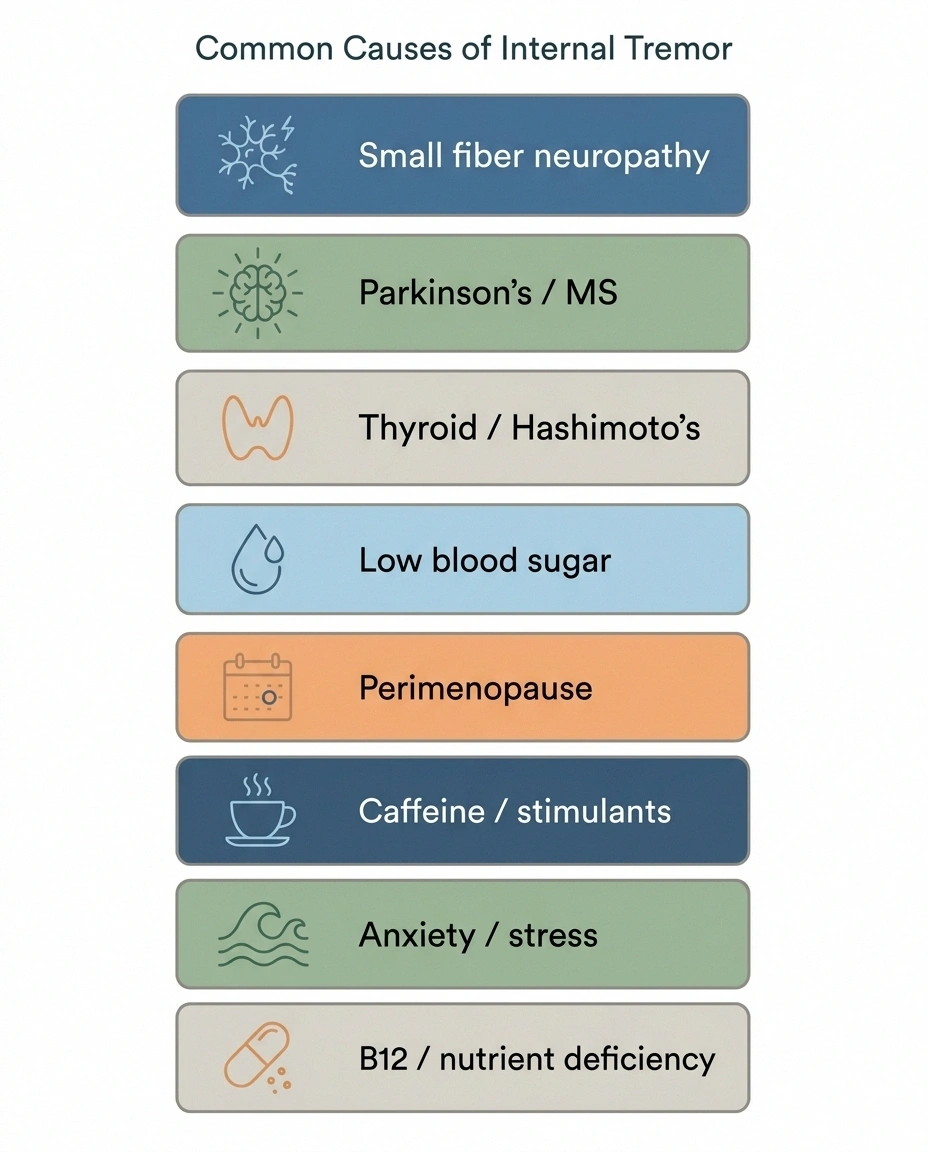
Before I lean too hard on the neuropathy angle, I have to be honest: internal tremor is a relatively non-specific symptom. It can come from a lot of different sources, and the right path forward depends heavily on which one is at play. A thoughtful workup should look at several possibilities.
Neurological Conditions Beyond Neuropathy
- Parkinson's disease (early or prodromal): Some people with early Parkinson's report internal tremor in the months or years before any visible tremor develops. This is not a reason to panic if you have internal tremor — most people with this symptom do not have Parkinson's — but it is on the differential and a neurologist should consider it.
- Multiple sclerosis: Demyelination of nerve fibers can cause ectopic firing that produces internal vibration sensations, especially in patients with established MS.
- Essential tremor (atypical presentation): Occasionally essential tremor can be reported as feeling internal before becoming visible.
- Orthostatic tremor: A high-frequency tremor of the legs felt mostly on standing, often described internally even when subtle externally.
Autonomic and Endocrine Drivers
- Hyperthyroidism or Hashimoto's: An overactive thyroid drives the sympathetic nervous system into overdrive — heart-racing, anxiety, and yes, a buzzy internal-tremor feeling.
- Hypoglycemia: Low blood sugar triggers a flood of adrenaline that feels exactly like internal tremor. People with diabetes (especially those on insulin or sulfonylureas) and people with reactive hypoglycemia know this one well.
- Perimenopause and menopause: Fluctuating estrogen can produce vasomotor symptoms (hot flashes, night sweats) and a sense of internal vibration in some women.
- Postural orthostatic tachycardia syndrome (POTS) and dysautonomia: Patients with autonomic dysfunction often describe internal tremor, especially on standing or with stress.
Lifestyle and Substance Drivers
- Excessive caffeine or stimulants: Coffee, energy drinks, decongestants (pseudoephedrine), ADHD medications, asthma inhalers — anything sympathomimetic can produce internal tremor.
- Alcohol withdrawal: Even mild reduction from regular drinking can cause internal tremulousness within 12–48 hours.
- Anxiety, panic, or chronic stress: A persistently activated fight-or-flight system feels like internal tremor.
- Sleep deprivation: Severe sleep loss raises adrenergic tone.
- Medication side effects: SSRIs, SNRIs, bupropion, beta-agonists, and some antibiotics can all trigger the sensation.
Nutritional Deficiencies
- Vitamin B12 deficiency: Worth checking in almost any neurological symptom workup. Linked to both neuropathy and tremulousness.
- Vitamin D, magnesium, and electrolyte imbalances: All can show up as buzzy nervous-system symptoms.
I list these not to alarm you with the possibilities, but to give you the language to advocate for an actual workup. “Internal tremor” without a rule-out plan is not a complete clinical evaluation.
What to Ask Your Doctor For
If you bring this symptom to a primary care doctor or neurologist, here's a reasonable starter list of things to discuss. Not every item is right for every patient — but at least these should be on the table.
- Basic blood work: CBC, comprehensive metabolic panel, TSH and free T4 (thyroid), vitamin B12 (with methylmalonic acid if B12 is low-normal), vitamin D, fasting glucose, and HbA1c.
- Medication and stimulant review: A careful look at every prescription, OTC, supplement, and caffeinated thing you take. Sometimes the trigger is hiding in plain sight.
- Neurological exam: Looking for subtle signs of Parkinsonism, hyperreflexia, weakness, or sensory abnormalities.
- If small fiber neuropathy is suspected: A skin punch biopsy with intraepidermal nerve fiber density measurement is the gold standard. This is the test that most patients with possible small fiber neuropathy have not yet had.
- Autonomic testing if relevant: Tilt-table test for POTS, sweat testing (QSART), and heart rate variability if orthostatic symptoms are present.
- Referral to neurology: If your primary care doctor isn't sure or the symptom is persistent, this is the specialist you want. You can read more about choosing a neurologist for neuropathy if you don't already have one.
Bring a brief written history. Something like: “I started feeling internal vibration in my torso about three months ago. It's worse when I'm tired or after coffee. It's not visible to anyone. No other neurological symptoms. Family history of thyroid disease.” That kind of compact summary goes much further than rambling through it in real time. A symptom diary can also help you spot patterns ahead of the appointment.
When Internal Tremor Is an Emergency
Most internal tremor is annoying but not dangerous. There are situations where it does need urgent attention, though, and I'd rather you have these in mind than not.
- Sudden one-sided weakness, numbness, or facial droop
- Slurred speech or sudden difficulty speaking
- Sudden severe headache (“worst of my life”)
- Sudden vision changes or vision loss
- Chest pain or pressure, severe palpitations
- Confusion, loss of consciousness, or first-ever seizure
Go to the ER (or call 911) if internal tremor comes along with:
- Sudden weakness or numbness on one side of the body
- Slurred speech, drooping face, or sudden difficulty speaking
- Sudden severe headache, especially “worst headache of my life”
- Sudden vision changes, double vision, or vision loss
- Chest pain or pressure
- Severe palpitations or heart racing that won't settle
- Confusion, disorientation, or loss of consciousness
- Severe shortness of breath
- A first-ever seizure
These are red flags because they suggest something acute — stroke, cardiac event, severe hypoglycemia, drug reaction — that needs immediate evaluation, not a scheduled visit.
Schedule with your doctor (not ER) but soon if internal tremor:
- Is new and has lasted more than a week
- Comes with new weakness, balance problems, or coordination issues
- Comes with significant unintentional weight loss or appetite changes
- Comes with new persistent palpitations, heat intolerance, or sweating changes
- Is worsening despite removal of obvious triggers (caffeine, stress)
What Helps — Things You Can Try Tonight

Now to the part most readers want. While you're working on the diagnostic side, there are several things you can do that often quiet internal tremor regardless of the underlying cause. None of these are cures. Several of them work because they tone down the same overactive nervous system that's producing the buzzing.
Calm the Sympathetic Nervous System
Slow, deep breathing. Specifically: 4-second inhale through the nose, 6 to 8-second exhale through the mouth, for five minutes. The long exhale is what activates the parasympathetic (rest-and-digest) nervous system. People often feel the buzzing soften noticeably during a five-minute session.
Cold face or cold water on the wrists. Splashing cold water on your face or holding a cold pack to your cheeks activates the dive reflex and slows the heart rate. This is one of the most reliable acute calming maneuvers and works in under a minute.
Get your feet on the ground. Literally: sit, put both feet flat on the floor, and notice the contact. This is a basic grounding technique that pulls attention out of the buzzing and into the present moment.
Address the Easy Triggers
- Cut caffeine. Not “reduce” — for a one-week trial, eliminate. Many cases of internal tremor are completely resolved by this single change. If it's the cause, you'll know quickly.
- Cut alcohol. Daily drinking, even modest amounts, raises sympathetic tone and disrupts sleep. A two-week dry stretch is the cleanest test.
- Watch decongestants and stimulant medications. Pseudoephedrine, Sudafed, “non-drowsy” cold medicines, ADHD stimulants — if any of these started around the time the buzzing started, talk to your doctor about alternatives.
- Stable blood sugar. Avoid long stretches without food. Aim for protein at every meal. Don't skip breakfast. If you're diabetic, this becomes even more important — check sugars when the buzzing happens to see if hypoglycemia is the driver.
The Supplements With Some Evidence
I want to be careful here — supplements are not regulated like medications, the evidence base is mixed, and what helps one person may do nothing for another. With that caveat:
- Magnesium glycinate, 200–400 mg in the evening. Magnesium is involved in nerve signaling and many people with internal tremor are mildly low. The glycinate form is gentle on the stomach. (Magnesium oxide is poorly absorbed and can cause loose stools.) Read more in Magnesium for Neuropathy.
- Vitamin B12, if blood levels are low or low-normal. Don't supplement blindly — get it checked. Methylcobalamin is the form many neurologists prefer.
- Vitamin D, if deficient. Same logic — test first, then treat.
- L-theanine, 100–200 mg. An amino acid from tea that has a mild calming effect without sedation. Some patients find it useful as needed during buzzy episodes.
Talk to your doctor before starting any new supplement, especially if you take prescription medications or have kidney or liver issues.
The Long-Game Strategies
If the underlying cause is small fiber neuropathy or another form of nerve damage, addressing the root condition matters more than chasing symptoms. That can mean tight blood sugar control if diabetes is involved, treating an underlying autoimmune driver, or working through the broader nerve-pain toolkit. You'll find a comprehensive overview in Small Fiber Neuropathy and in Best Natural Remedies for Peripheral Neuropathy Pain.
If anxiety, chronic stress, or a hyperaroused nervous system is the dominant driver, sleep, regular gentle exercise, and a structured stress-management practice (mindfulness, CBT, or appropriate professional support) often matter more than any supplement. I cover this connection in Neuropathy and Anxiety.
You Are Not Crazy

One of the hardest parts of this symptom — and I hear this from readers more than almost any other complaint — is the fear that it's all in your head because nobody can see it. You feel it, you describe it, and someone asks “well, are you stressed?” as if that closes the conversation.
Internal tremor is real. It's documented. It has multiple legitimate causes, several of which are treatable. It can be a symptom of small fiber neuropathy, of thyroid problems, of dysautonomia, of medication interactions, of post-viral nervous system dysfunction. It can also be benign and self-limiting once a trigger is removed.
What it is not is imaginary. The fact that no one else can see it doesn't mean it isn't happening. The most important thing you can do is find a clinician who will take the symptom seriously enough to actually look for a cause. The second most important thing is calming the nervous system in the meantime so you can sleep, eat, and function while you figure it out.
If you've had this symptom dismissed in the past, I'm sorry. Please don't give up. The research is finally catching up to what patients have been describing for years.
Frequently Asked Questions
Can internal tremors be a sign of neuropathy?
Yes, in some cases. Internal tremor has been documented as a symptom of small fiber neuropathy, particularly in long COVID patients and in people with autoimmune or post-viral nerve damage. The mechanism is misfiring of damaged small sensory fibers, the same kind of misfire that produces tingling, electric shocks, and burning sensations elsewhere in neuropathy. That said, internal tremor has many other causes too, so a workup should not assume neuropathy without checking other possibilities first.
Are internal tremors a sign of Parkinson's disease?
They can be, but most people with internal tremor do not have Parkinson's. Some people with early or prodromal Parkinson's report a sensation of internal tremor before any visible tremor develops, which is why a thorough neurological exam is part of the workup. The key Parkinson-related features your doctor will look for are slowing of movement, stiffness, changes in handwriting or facial expression, and a specific type of rest tremor that becomes visible over time. Internal tremor without those other features is far more likely to have a different cause.
Why is the buzzing worse at night?
Several reasons. The environment is quieter, so any nervous-system noise becomes more noticeable. Caffeine consumed earlier in the day is still active. Sleep deprivation can amplify the symptom. And the autonomic nervous system has natural daily rhythms that affect how nerve signals are processed. Many neuropathy symptoms are worse at night for similar reasons. The full picture is in our article on why neuropathy gets worse at night.
Can anxiety alone cause internal tremor?
Yes. Sustained anxiety and a chronically activated stress response can produce a sensation of internal vibration that is indistinguishable from the buzzing produced by nerve misfiring. The complicated part is that the two often coexist, because living with an undiagnosed strange symptom is anxiety-producing, and anxiety amplifies the symptom. Treating anxiety alongside a thoughtful medical workup is reasonable and often helpful.
Does long COVID cause internal tremor?
Researchers have documented internal tremor as one of the most common neurological manifestations of long COVID, particularly in patients who develop dysautonomia or small fiber neuropathy after their infection. A 2026 paper in Neurology International described internal tremor as a characteristic feature of post-COVID autonomic dysfunction in a substantial subset of patients. If your internal tremor started after a COVID infection and hasn't resolved, this is worth raising with your doctor.
What test diagnoses the cause of internal tremors?
There is no single test for internal tremor. The workup depends on what your doctor suspects. Reasonable starting tests include thyroid function, vitamin B12, fasting glucose and HbA1c, vitamin D, and a careful medication review. If small fiber neuropathy is suspected, a skin punch biopsy measuring intraepidermal nerve fiber density is the gold standard. If autonomic dysfunction is suspected, tilt-table testing and sweat testing may be added. A neurologist is often the right specialist to coordinate this workup.
Will magnesium help with internal tremor?
Sometimes, especially if your magnesium levels are low or low-normal. Magnesium is involved in nerve signaling and calming the nervous system. Many neurologists are comfortable suggesting a trial of magnesium glycinate at 200 to 400 mg in the evening for several weeks to see if it helps. It is not a substitute for figuring out what is actually driving the symptom, but it is a low-risk option for many people. Talk to your doctor before starting if you have kidney problems or take other medications.
How long does internal tremor last?
It depends entirely on the cause. If the trigger is caffeine, a medication, or a transient stressor, the symptom often resolves within days to weeks of removing the trigger. If the cause is an underlying condition like small fiber neuropathy, thyroid disease, or long COVID, the timeline is tied to treating that condition. Some people see significant improvement over months. Others find that nervous-system support strategies like good sleep, magnesium, and stress management make the symptom much quieter even if it doesn't fully resolve.


