
Arm Pain and Weakness: Neuropathy vs. Cervical Radiculopathy vs. Thoracic Outlet Syndrome
When pain, tingling, or weakness radiates down your arm, the instinct is to blame the arm itself. But more often than not, the problem starts somewhere else entirely — in the nerves of your neck, the passageway behind your collarbone, or the peripheral nerves running from your spinal cord to your fingertips. I've talked with hundreds of people in our neuropathy community who spent months being treated for the wrong condition because arm pain is notoriously difficult to pin down.
Three conditions sit at the top of the differential diagnosis for arm pain and weakness: peripheral neuropathy, cervical radiculopathy, and thoracic outlet syndrome (TOS). Each one compresses or damages nerves — but at different anatomical locations, through different mechanisms, and with distinctly different treatment paths. Getting the right diagnosis matters because surgery for one condition won't help another, and physical therapy for TOS is essentially the opposite of PT for radiculopathy.
This guide breaks down each condition so you can walk into your doctor's appointment with sharper questions and a better understanding of what your arm is trying to tell you.
Why Arm Pain Is So Hard to Diagnose
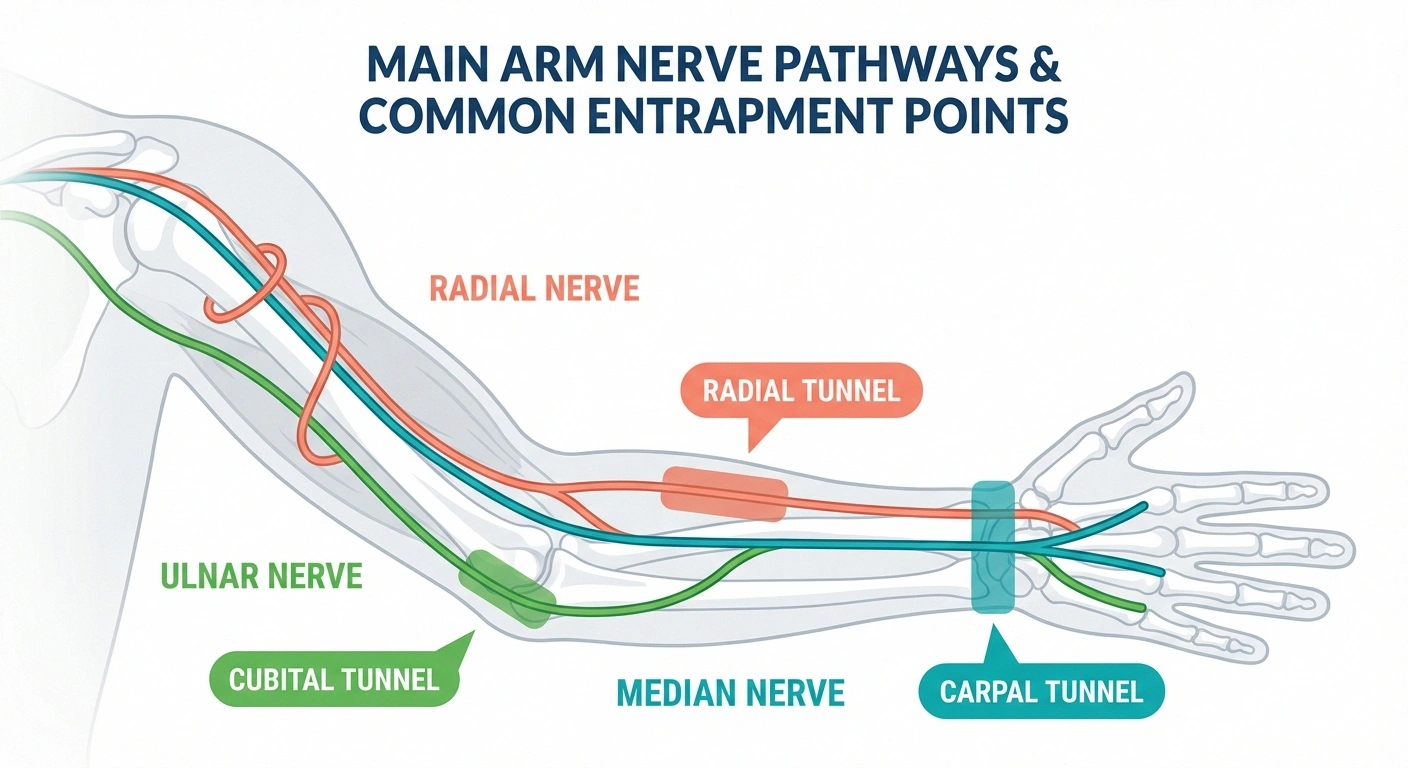
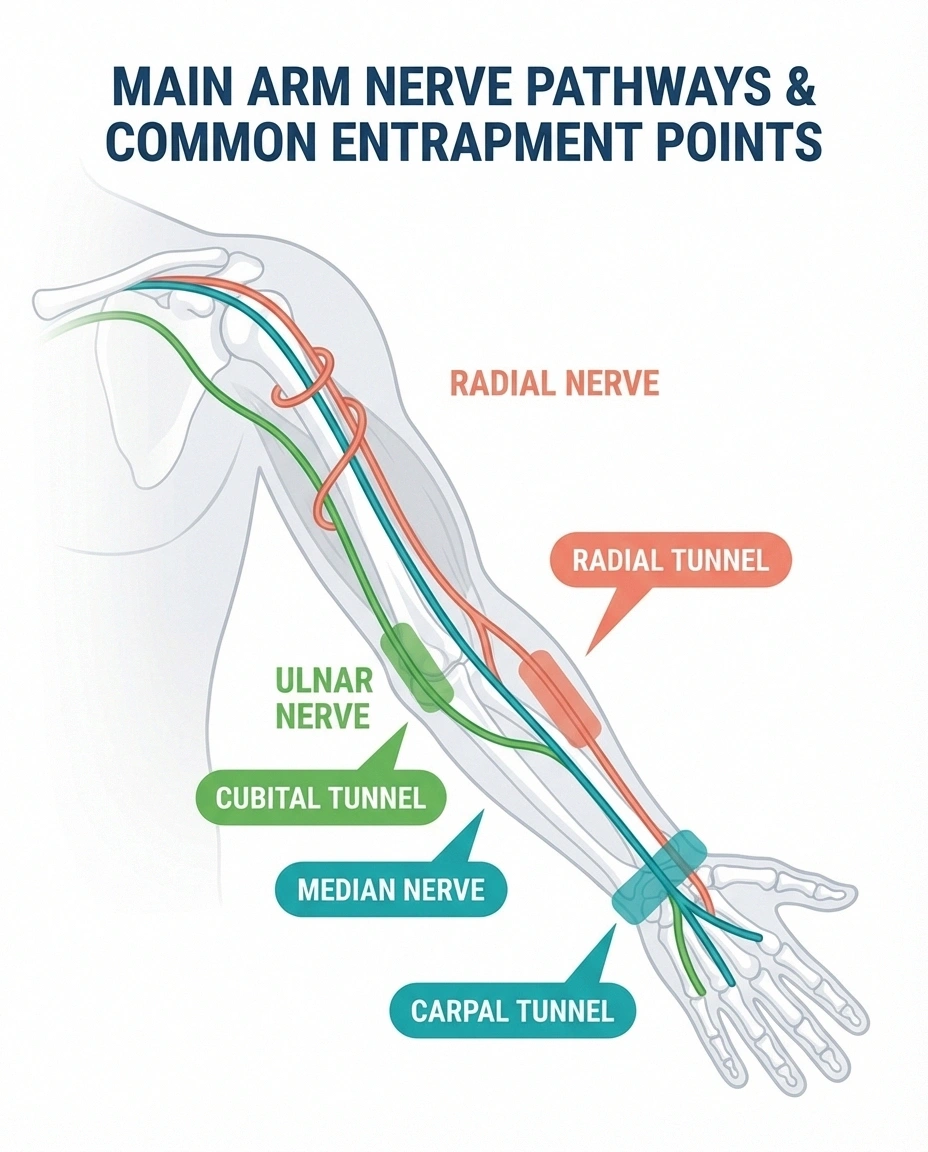
The nerves supplying your arm follow a long, complex path. They originate in the cervical spine (neck), bundle together into the brachial plexus behind your collarbone, then branch out into individual nerves (median, ulnar, radial) that travel through your arm to your fingertips. A problem at any point along this chain can cause pain, weakness, or numbness in your arm and hand.
The Diagnostic Key
Where exactly the symptoms are, what position makes them worse, and what position makes them better — these three clues do more to distinguish neuropathy, radiculopathy, and TOS than any single test.
What makes diagnosis challenging is that the symptoms overlap significantly. All three conditions can cause arm pain, tingling, numbness, and weakness. As noted in a landmark paper in the Journal of Neurosurgery: Spine, “thoracic outlet syndrome is often diagnosed when, in fact, the problem is radiculopathy or neuropathy” — and the reverse is equally true. Even experienced spine surgeons sometimes struggle with this differential.
The key to getting it right is paying attention to the specific pattern: where exactly the symptoms are, what makes them worse, what makes them better, and what other signs accompany the arm complaints.
Peripheral Neuropathy: When the Arm Nerves Themselves Are Damaged
Peripheral neuropathy affecting the arms involves damage to the nerves after they've left the brachial plexus — the median, ulnar, or radial nerves (or the smaller sensory nerve fibers throughout the arm and hand). The damage occurs within the nerve itself, not from external compression at the spine or thoracic outlet.
Like neuropathy in the feet, arm neuropathy often follows a predictable pattern. Symptoms typically start in the fingers and hands (the longest nerve fibers) and may gradually extend up toward the forearm. The pattern is usually bilateral — affecting both hands, though one may be worse than the other. Common sensory complaints include numbness, tingling, burning, and that uncomfortable “pins and needles” feeling that many people with neuropathy know well.
The causes overlap with lower extremity neuropathy: diabetes, B12 deficiency, chemotherapy, alcohol, autoimmune conditions, and idiopathic cases. Importantly, arm neuropathy from these systemic causes almost always appears after the feet are already affected — the feet-first rule. If your hands are numb but your feet are fine, pure peripheral neuropathy is less likely, and compression causes (carpal tunnel, radiculopathy, TOS) move up the suspect list.
Entrapment Neuropathies in the Arm
The arm also has specific nerve entrapment points where a peripheral nerve gets pinched by surrounding structures. These are technically a form of neuropathy, but the mechanism is compression rather than systemic damage.
The Feet-First Rule
Systemic neuropathies (diabetes, B12 deficiency, alcohol) almost always affect the feet before the hands. If your hands are numb but your feet feel fine, compression causes — carpal tunnel, radiculopathy, or TOS — are much more likely than peripheral neuropathy.
Carpal tunnel syndrome (median nerve compressed at the wrist) is by far the most common, causing numbness and tingling in the thumb, index, middle, and half of the ring finger. Cubital tunnel syndrome (ulnar nerve compressed at the elbow) causes numbness in the ring and little finger plus weakness in grip. Radial tunnel syndrome (radial nerve compressed in the forearm) causes deep forearm pain that can mimic tennis elbow.
These entrapment neuropathies can mimic cervical radiculopathy or TOS, but each has characteristic patterns. Carpal tunnel typically worsens at night and with repetitive wrist movements. Cubital tunnel worsens with prolonged elbow bending (like holding a phone). The distribution of numbness follows the specific nerve territory, which is different from the dermatomal pattern of radiculopathy.
Cervical Radiculopathy: When a Pinched Neck Nerve Sends Pain Down the Arm
Cervical radiculopathy occurs when a nerve root in the neck is compressed or irritated, usually by a herniated disc or degenerative bone spurs. The compressed nerve root sends pain, numbness, and weakness radiating down the arm in a pattern that follows the specific nerve root being affected.
of cervical radiculopathy involves C6 or C7 nerve roots
of TOS follows an ulnar (C8-T1) nerve distribution
This is by far the most common cause of arm pain that originates in the spine. According to clinical research, approximately 90% of cervical radiculopathy cases involve the C6 or C7 nerve roots — meaning the C5/C6 and C6/C7 disc levels are where the vast majority of problems occur.
Nerve Root Patterns: The Dermatomal Map
Each cervical nerve root supplies a specific region of the arm, and the symptoms follow that map reliably.
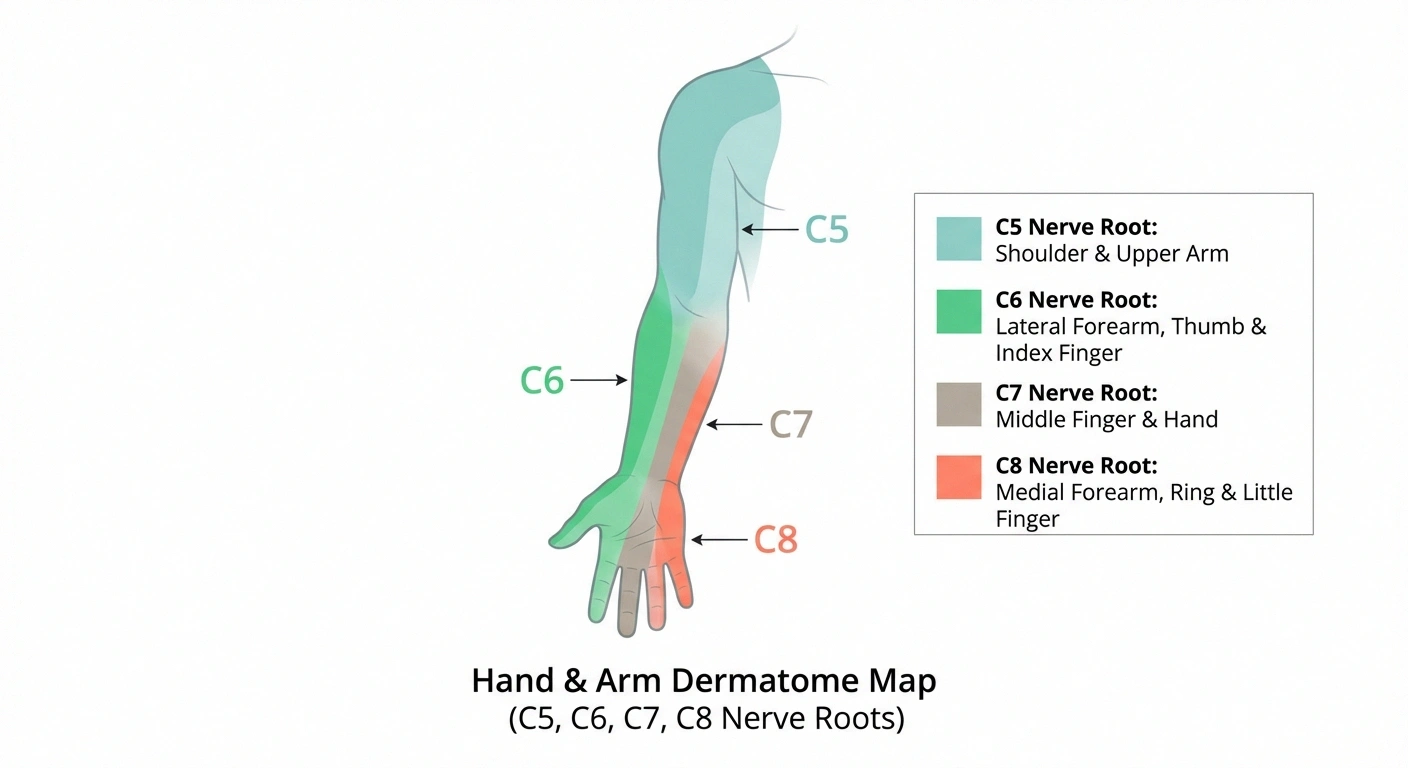
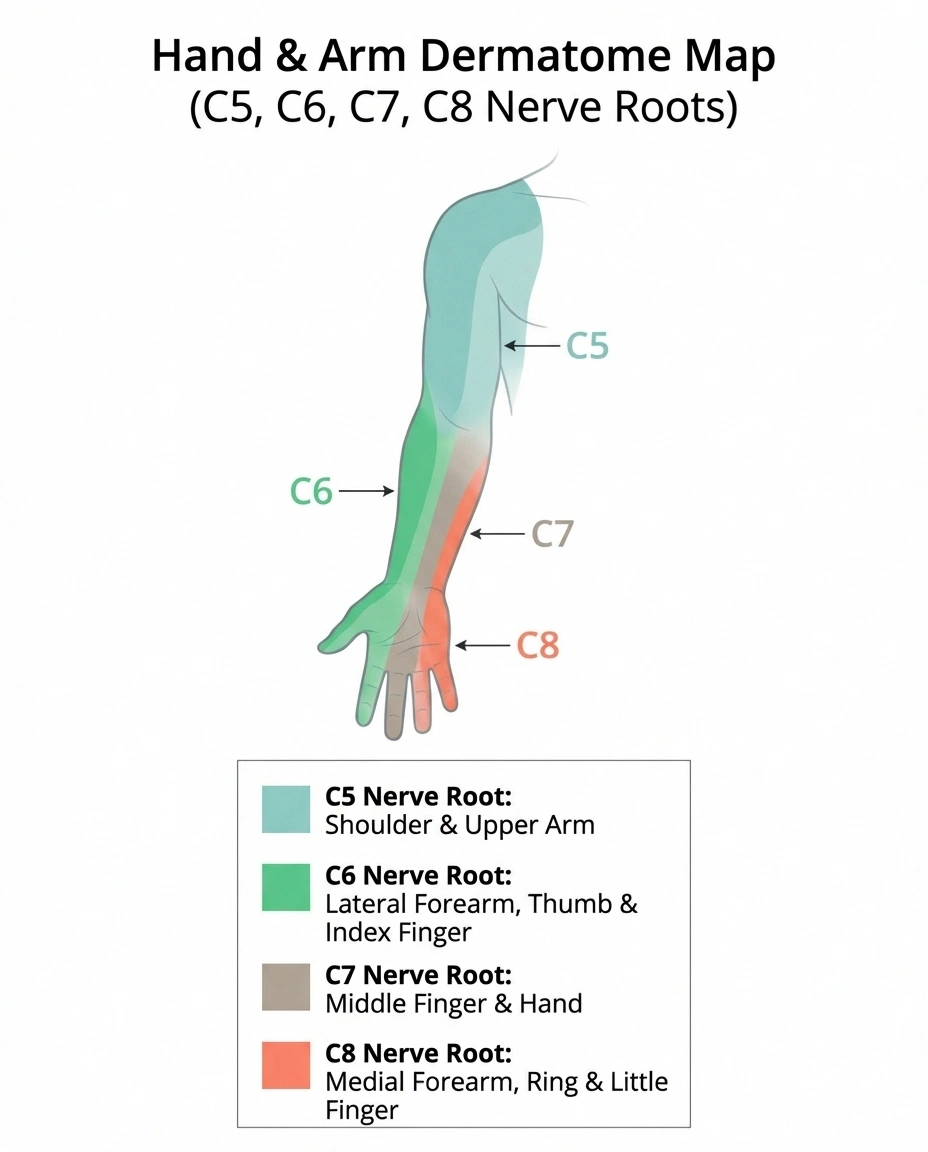
C5 radiculopathy causes pain in the shoulder and outer upper arm, with weakness in shoulder abduction (raising your arm to the side) and elbow flexion (bicep curl motion). Numbness affects the outer shoulder and upper arm.
C6 radiculopathy — the most common — causes pain radiating from the neck through the shoulder, down the outer arm, and into the thumb and index finger. Weakness affects the bicep and wrist extension (bending the wrist backward). The brachioradialis reflex may be diminished.
C7 radiculopathy — the second most common — sends pain down the middle of the arm into the middle finger. Weakness affects the tricep (straightening the elbow) and wrist flexion. The tricep reflex may be diminished.
C8 radiculopathy causes pain and numbness along the inner forearm to the ring and little finger. This is where confusion with TOS peaks, because TOS also affects the C8-T1 nerve distribution. Weakness in C8 radiculopathy affects grip strength and finger dexterity.
The Signature Clues of Cervical Radiculopathy
Neck movement provokes symptoms. Turning your head toward the affected side, looking up, or tilting your head back typically worsens the arm pain — because these motions narrow the neural foramen (the opening where the nerve exits the spine). Conversely, the shoulder abduction test can help confirm radiculopathy: holding the affected arm overhead often relieves symptoms because it takes tension off the compressed nerve root.
The onset can be sudden (after a neck injury or awkward movement) or gradual (from progressive disc degeneration). In patients under 50, disc herniation is the most common cause. Over 50, degenerative changes (bone spurs, disc narrowing) are more typical.
One important clinical pearl: if motor weakness or reflex changes are present — not just pain and numbness — it suggests true nerve compression rather than simple irritation, and warrants more urgent evaluation.
Thoracic Outlet Syndrome: The Overlooked Compressor
Thoracic outlet syndrome occurs when nerves, arteries, or veins are compressed in the thoracic outlet — the narrow space between the collarbone (clavicle) and the first rib. The structures passing through this tight corridor include the brachial plexus (the nerve bundle supplying the entire arm) and the subclavian vessels (the main blood supply to the arm).
TOS is divided into three types: neurogenic (nerve compression, accounting for about 95% of cases), venous (vein compression), and arterial (artery compression). Neurogenic TOS is the one most commonly confused with cervical radiculopathy and peripheral neuropathy, so that's our focus here.
A comprehensive review in Pain and Therapy notes that TOS “remains a challenging and highly controversial diagnosis” — in part because there's no single definitive test, and alternative compressive neuropathies must be excluded.
How TOS Symptoms Differ
The critical distinguishing feature: TOS symptoms follow an ulnar nerve distribution (C8-T1) in about 90% of cases. That means numbness and tingling primarily affect the ring finger, little finger, and inner forearm. This is different from the C6 and C7 patterns that account for 90% of cervical radiculopathy.
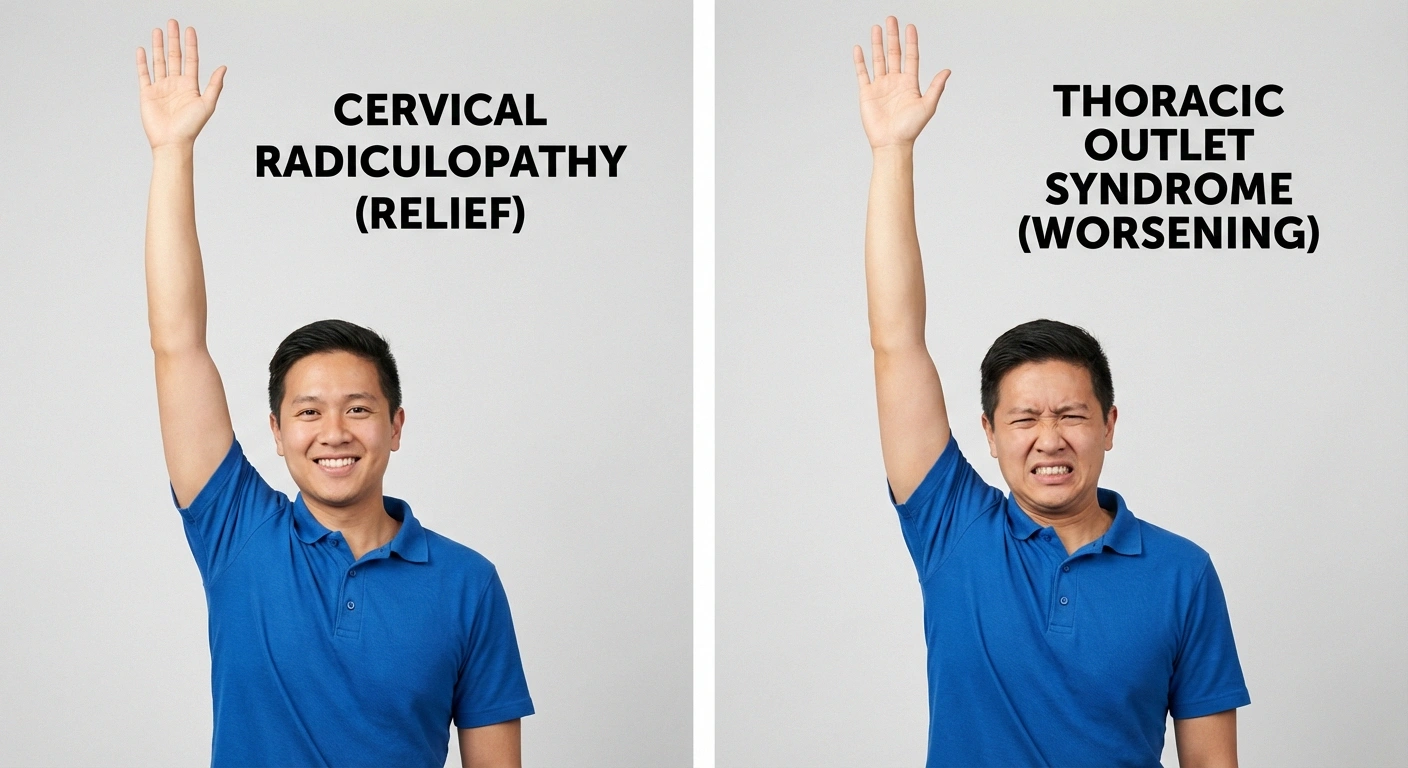
Here's the key positional test: raising the arm overhead. In cervical radiculopathy, overhead arm position typically relieves symptoms (the shoulder abduction sign). In TOS, the same position typically worsens symptoms — because raising the arm narrows the thoracic outlet further and increases compression on the brachial plexus.
TOS is aggravated by activities that involve overhead arm use: reaching up to shelves, blow-drying hair, sleeping with arms above the head, carrying heavy bags on the shoulder, and sustained computer work with poor posture. It's common in younger patients (20s-40s) and has associations with repetitive occupational arm use, anatomical variations (cervical rib, which occurs in about 0.5% of the population), and poor posture.
The Vascular Component
Unlike neuropathy and radiculopathy, TOS can include vascular symptoms — color changes in the hand (pale, blue, or mottled), coldness, and in venous TOS, arm swelling. These vascular signs are a strong differentiator. Peripheral neuropathy and cervical radiculopathy don't cause hand color changes or swelling. If you notice that your hand turns pale or blue with certain arm positions, mention this specifically to your doctor — it points toward TOS.
The Comparison: How to Tell Them Apart
Let's compare the three conditions across the features that matter most for diagnosis.
Where the Symptoms Are
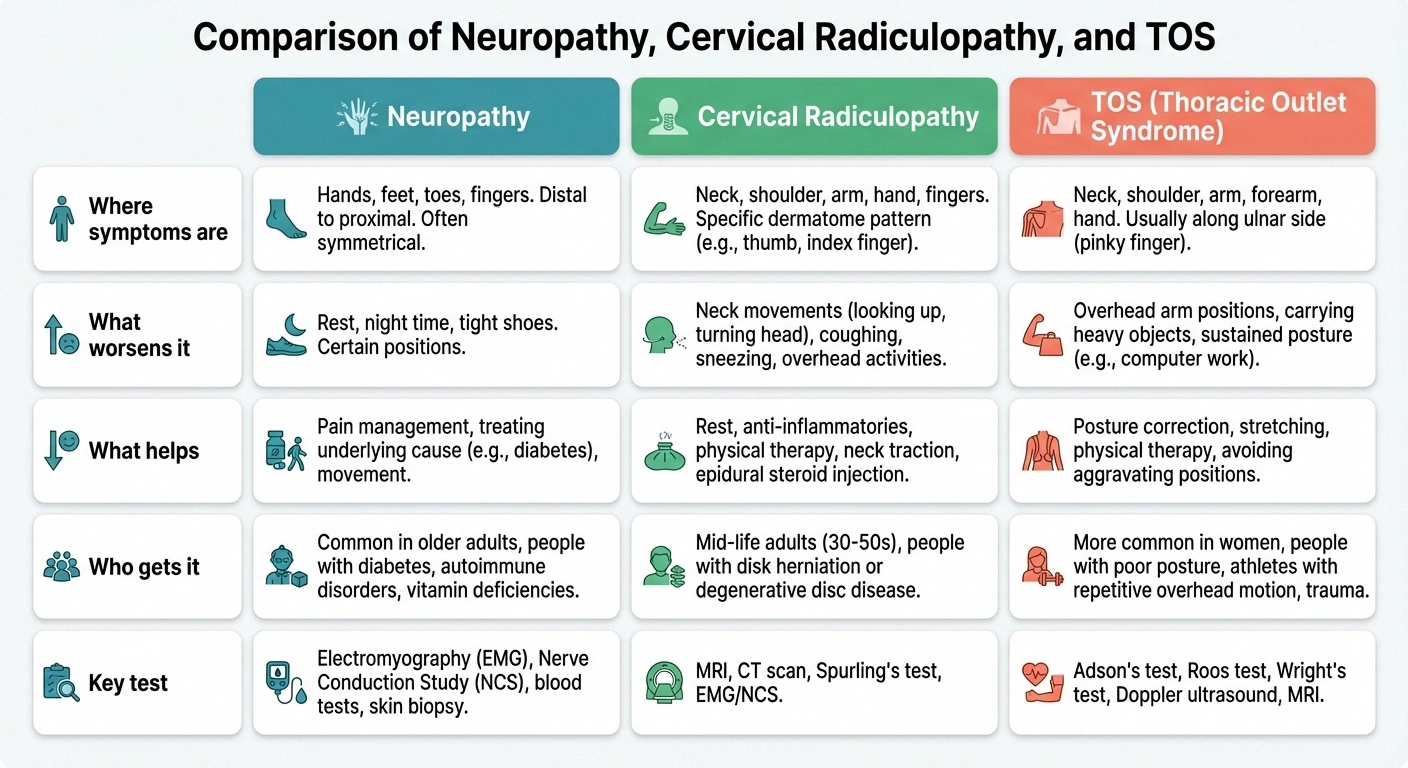
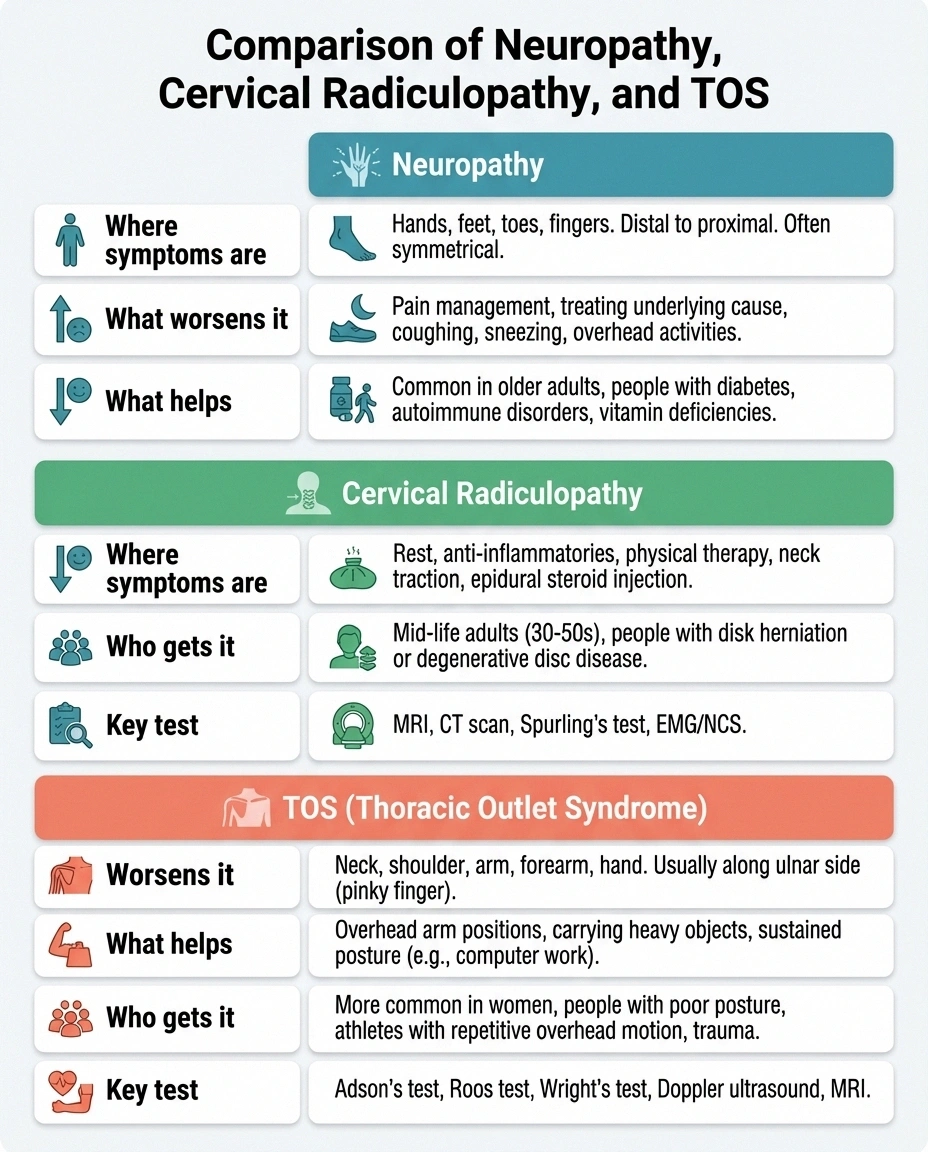
Neuropathy: Starts in fingers/hands, often bilateral. “Glove” distribution. Symmetrical or near-symmetrical. Sensory symptoms (numbness, tingling, burning) predominate.
Cervical Radiculopathy: Follows a specific nerve root pattern from neck through shoulder down arm to specific fingers. Usually one arm. C6 → thumb/index finger. C7 → middle finger. C8 → ring/little finger.
TOS: Predominantly C8-T1 territory — inner forearm, ring finger, little finger. Usually one arm. May include hand color changes or swelling (vascular component).
What Makes It Worse
Neuropathy: Symptoms are relatively constant. May worsen at night. Not significantly affected by arm or neck position.
Cervical Radiculopathy: Neck movement — turning head toward affected side, looking up, tilting head back. Coughing or sneezing can trigger sharp arm pain.
TOS: Overhead arm positions — reaching up, blow-drying hair, sleeping with arms above head. Carrying heavy items. Sustained poor posture.
What Makes It Better
Neuropathy: Treating the underlying cause. Symptoms don't change significantly with position changes.
Cervical Radiculopathy: Raising the arm overhead (shoulder abduction sign). Turning head away from the affected side. Supporting the arm with a pillow or sling.
TOS: Keeping the arm at or below shoulder level. Postural correction. Specific stretches that open the thoracic outlet. Avoiding overhead activity.
Who Gets It
Neuropathy: More common after age 50. Associated with diabetes, B12 deficiency, alcohol use, chemotherapy. Usually bilateral.
🧤 Neuropathy
Pattern: Both hands, glove distribution
Worsens: Constant, worse at night
Clue: Feet affected first
🦴 Radiculopathy
Pattern: One arm, follows nerve root
Worsens: Neck movement, looking up
Clue: Arm overhead = relief
🔄 TOS
Pattern: One arm, ring/little finger
Worsens: Overhead arm positions
Clue: Arm overhead = worse
Cervical Radiculopathy: Under 50, disc herniation is the usual cause. Over 50, degenerative changes predominate. Neck injury or heavy physical work may trigger it.
TOS: Often younger patients (20s-40s). More common in women. Associated with repetitive overhead work, poor posture, anatomical variations like a cervical rib, and sometimes neck trauma (whiplash).
The Double Crush Phenomenon
Here's a complicating reality that makes diagnosis even trickier: nerves that are compressed at one point become more vulnerable to compression at a second point. This is called the double crush phenomenon, and it's surprisingly common.
For example, someone with mild cervical radiculopathy (nerve root compression in the neck) may also develop carpal tunnel syndrome more readily, because the nerve — already stressed at the neck — has less reserve capacity to tolerate compression at the wrist. Studies suggest that up to 10-30% of patients with carpal tunnel syndrome also have cervical radiculopathy.
This means your arm pain might not have a single cause. A thorough evaluation that examines the entire nerve pathway — from the neck through the thoracic outlet through the arm to the hand — is essential for finding all the contributing factors.
Diagnostic Tests: Finding the Source
Each condition has characteristic test findings, though some tests are more definitive than others.

For Peripheral Neuropathy
EMG and nerve conduction studies are the gold standard. They measure how quickly and efficiently your nerves transmit signals and can identify which specific nerves are damaged and where. Blood work helps identify underlying causes — glucose, B12, folate, thyroid function, inflammatory markers. For small fiber neuropathy, which affects the thinnest sensory nerves, a skin biopsy may be needed as standard NCS can appear normal.
For Cervical Radiculopathy
MRI of the cervical spine is the primary imaging tool — it shows disc herniations, bone spurs, and neural foraminal narrowing that compress nerve roots. Physical examination tests include Spurling's test (compressing the neural foramen to reproduce arm symptoms) and the shoulder abduction test (relieving arm symptoms by raising the arm overhead). EMG can confirm which nerve root is affected and assess severity.
For Thoracic Outlet Syndrome
Diagnosis is more challenging because there's no single definitive test. Provocative maneuvers (Roos test, Adson's test, Wright's test) reproduce symptoms by stressing the thoracic outlet. Chest X-ray or CT can identify cervical ribs or other anatomical abnormalities. MR angiography with the arm in provocative positions can demonstrate vascular compression. EMG may show changes in the lower trunk of the brachial plexus (C8-T1 fibers), but findings can be subtle.
Treatment Approaches
Getting the right diagnosis is critical because the treatment paths diverge significantly.
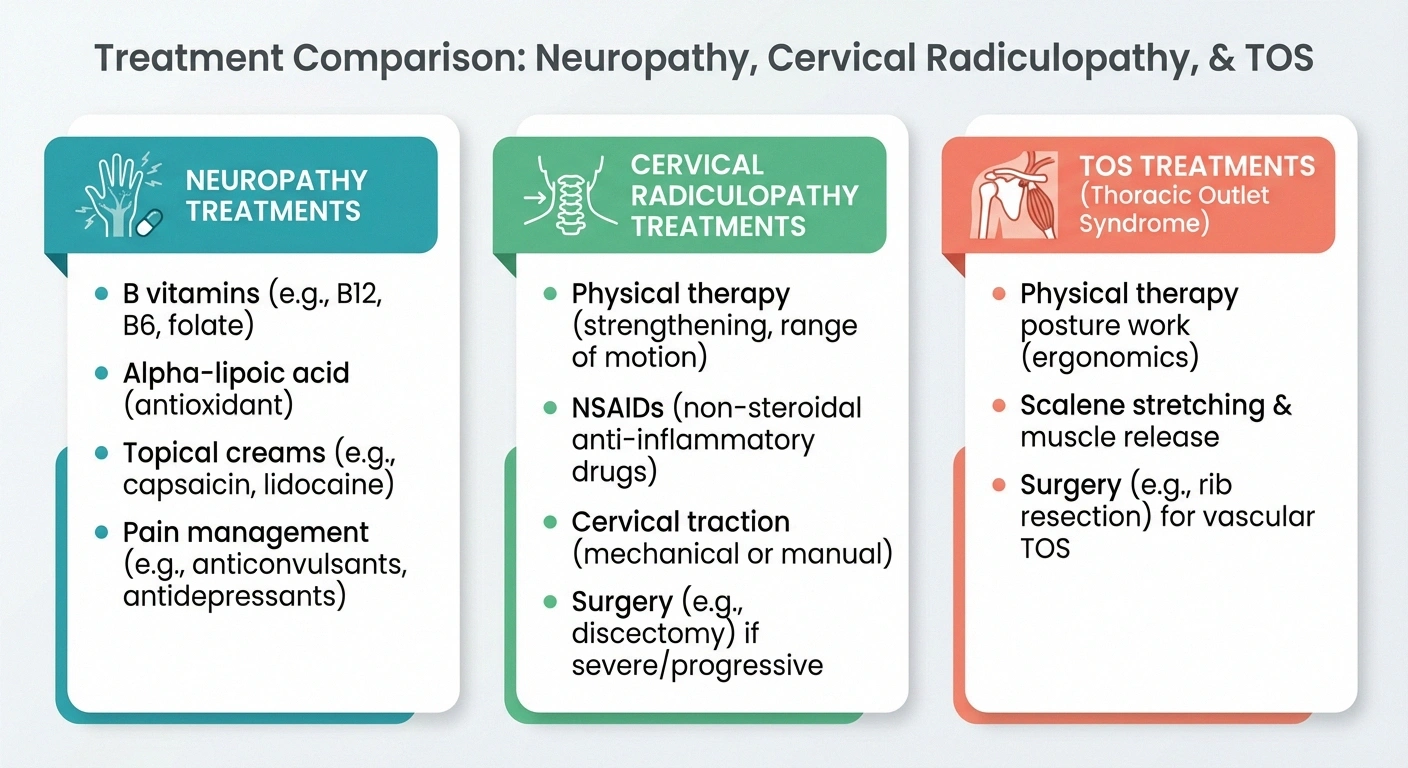
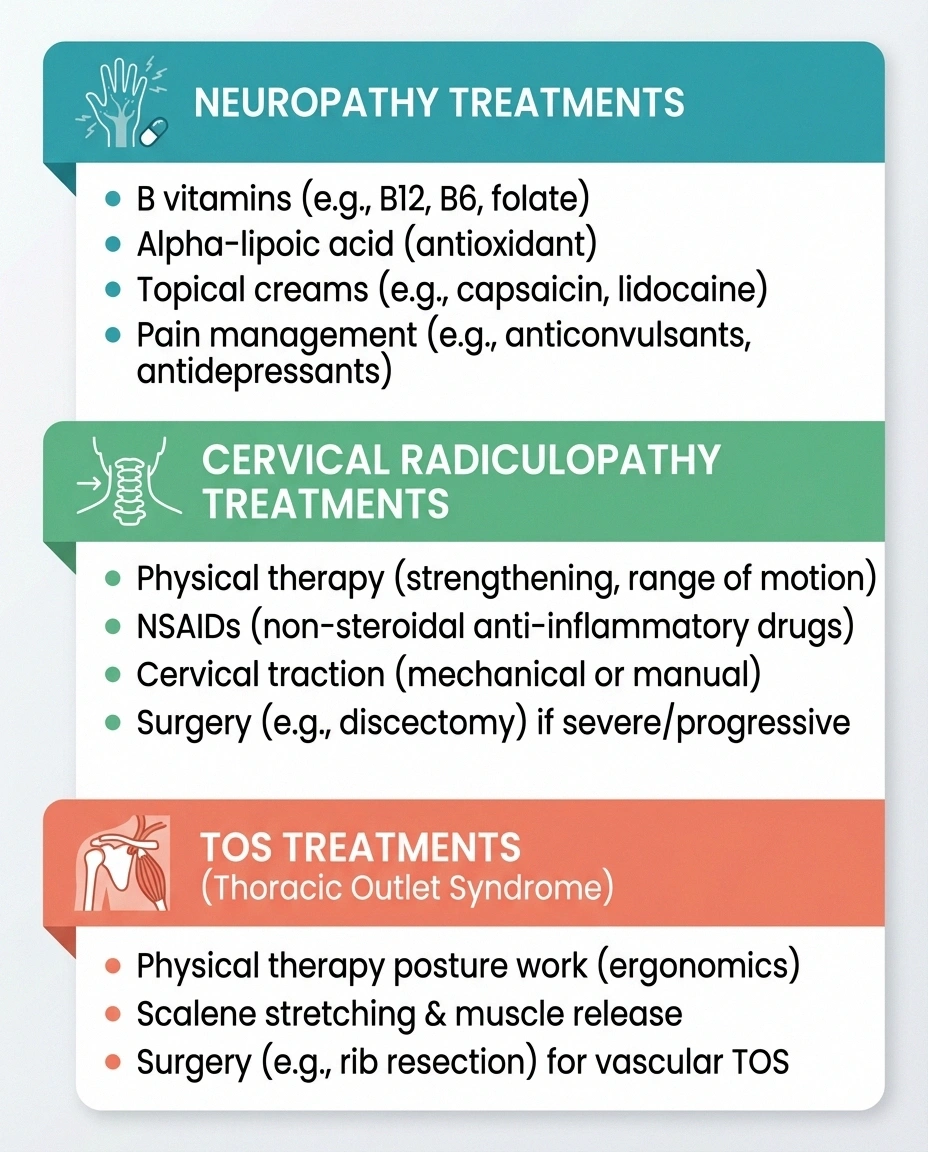
For peripheral neuropathy, treatment targets the underlying cause: tight blood sugar control for diabetic neuropathy, B12 supplementation for deficiency, stopping the offending medication for drug-induced cases. Symptom management may include gabapentin, duloxetine, or topical treatments. Occupational therapy can help maintain hand function.
For cervical radiculopathy, conservative treatment succeeds in most cases: physical therapy focused on cervical stabilization and nerve gliding exercises, oral anti-inflammatory medications, and sometimes epidural steroid injections. Surgery (anterior cervical discectomy and fusion) is reserved for cases with progressive weakness or failure of conservative treatment after 6-12 weeks.
For TOS, treatment starts with physical therapy — but the approach is essentially opposite to radiculopathy PT. TOS therapy focuses on opening the thoracic outlet through postural correction, scalene and pectoralis muscle stretches, and shoulder blade strengthening. Avoiding provocative positions is key. For cases with a cervical rib or vascular compression, surgical decompression (first rib resection) may be considered.
When Arm Symptoms Need Urgent Attention
Most arm pain and weakness can be evaluated in an outpatient setting. However, certain patterns require prompt attention. Seek urgent medical care if you experience rapidly progressive weakness in one or both arms over days (possible inflammatory condition), arm weakness with difficulty walking or bladder changes (possible spinal cord compression — myelopathy), sudden arm swelling with bluish discoloration (possible venous thrombosis in TOS), or sudden onset of weakness on one side of the body with facial changes or speech difficulty (possible stroke).
Seek Urgent Care If
Rapidly progressive arm weakness over days • Arm weakness with walking difficulty or bladder changes • Sudden arm swelling with blue/purple discoloration • One-sided weakness with facial or speech changes. These patterns may indicate spinal cord compression, vascular emergency, or stroke.
Preparing for Your Appointment
When you see your doctor about arm pain and weakness, come prepared with specific details. Note which fingers are numb or tingling. Track whether symptoms change with neck movement, arm position, or time of day. Document activities that make symptoms worse (overhead reaching? typing? sleeping?). Note whether the symptoms are in one arm or both. Record any neck pain, shoulder pain, or headaches that accompany the arm symptoms.

Be especially clear about what makes it better and what makes it worse. As we've discussed, the positional clues are some of the most powerful diagnostic tools: “My arm feels better when I hold it overhead” points to radiculopathy, while “My arm gets worse when I reach up” points to TOS. Your observations guide your doctor's examination and testing.
Frequently Asked Questions
Can carpal tunnel syndrome be confused with cervical radiculopathy?
Yes, this is one of the most common diagnostic confusions. Both can cause hand numbness and weakness. The key difference is the distribution: carpal tunnel affects the thumb, index, middle, and half of the ring finger (median nerve territory), while C7 radiculopathy affects the middle finger and C6 affects the thumb and index finger. Carpal tunnel typically worsens at night and with wrist bending, while radiculopathy worsens with neck movement. They can also coexist (double crush phenomenon).
Why do arm symptoms from cervical radiculopathy get better when I raise my arm?
When you raise your affected arm overhead (the shoulder abduction sign), it takes mechanical tension off the compressed nerve root in the neck. This position lifts the nerve root slightly away from the disc or bone spur that's pressing on it, providing temporary relief. This is the opposite of TOS, where overhead positioning narrows the thoracic outlet and worsens compression.
Does neuropathy in the arms mean my feet will be affected too?
In most systemic neuropathies (diabetic, B12 deficiency, alcohol-related), the feet are affected first because the longest nerve fibers are most vulnerable. If your feet are already numb and now your hands are becoming numb, that progression is consistent with peripheral neuropathy. If your hands are numb but your feet are perfectly normal, look for compression causes like carpal tunnel, cubital tunnel, cervical radiculopathy, or TOS rather than systemic neuropathy.
How long does cervical radiculopathy take to resolve?
Most cases improve significantly within 6 to 12 weeks with conservative treatment (physical therapy, anti-inflammatory medications, activity modification). Studies show that approximately 75 to 90 percent of cervical radiculopathy cases resolve without surgery. However, if weakness is progressive or severe, earlier surgical consultation is warranted because prolonged nerve compression can lead to permanent damage.
Is TOS a real diagnosis?
Yes, though it remains controversial in medical circles because neurogenic TOS — the most common type — lacks a single definitive diagnostic test. This has led some clinicians to question its existence. However, the condition is well-documented in the surgical and pain management literature. The controversy isn't about whether the condition exists; it's about diagnostic criteria and when surgery is justified. If your symptoms match the TOS pattern, seeking evaluation from a specialist experienced with this condition is important.
Can poor posture cause arm pain and numbness?
Yes. Chronically poor posture — specifically forward head position and rounded shoulders — can contribute to both cervical radiculopathy (by increasing disc pressure) and TOS (by narrowing the thoracic outlet). The modern “tech neck” posture from prolonged screen use is increasingly recognized as a contributor to both conditions. Postural correction is a first-line treatment for both, though the specific exercises differ.
The Bottom Line
Arm pain and weakness with neurological symptoms (numbness, tingling, weakness) always deserve a thorough evaluation, because the three most common causes — peripheral neuropathy, cervical radiculopathy, and thoracic outlet syndrome — require fundamentally different treatments. A physical therapy program designed for one condition can potentially worsen another.

Pay close attention to the positional clues: relief with overhead arm position suggests radiculopathy. Worsening with overhead arm position suggests TOS. Constant symptoms regardless of position suggest neuropathy. The distribution of numbness (which specific fingers), the relationship to neck movement, and whether one arm or both are affected all provide critical diagnostic information.
Don't settle for a generic “pinched nerve” diagnosis. Ask specifically: where is the nerve being compressed, and how does that guide treatment? Your arms do too much for you to leave this to guesswork. Browse all our symptom guides for more help understanding what your body is telling you.


