
EMG and Nerve Conduction Studies: What to Expect During Testing
Your doctor just told you that you need an EMG and nerve conduction study. If you're like most people, your immediate reaction is somewhere between confusion and anxiety. What exactly are these tests? Will they hurt? What will they tell you about your neuropathy? I remember sitting in the doctor's office after being told I needed electrodiagnostic testing, nodding as if I understood, and then going home to panic-search the internet for answers.
Here's the reassuring truth: EMG and nerve conduction studies are among the most valuable diagnostic tools for understanding what's happening with your nerves, and while they're not exactly pleasant, they're safe, well-tolerated by most people, and usually over within sixty to ninety minutes. This guide walks you through exactly what these tests involve, how to prepare, and what the results might mean — so you can walk into your appointment feeling informed rather than anxious.
What Are EMG and Nerve Conduction Studies?
EMG and nerve conduction studies (NCS) are two related but distinct tests that are often performed together as a single appointment. Together, they're sometimes called “electrodiagnostic testing” or simply “an EMG” — even though that technically refers to only one part of the exam. According to the Mayo Clinic, these tests assess the health of muscles and the nerve cells that control them.
Quick Summary
Nerve conduction study (NCS) = electrode stickers on skin, brief electrical pulses measure nerve speed and strength. Needle EMG = thin needle in muscles records electrical activity at rest and during contraction. Together, they take 60–90 minutes and tell your doctor exactly what's happening with your nerves.
Nerve conduction study (NCS) measures how well and how fast electrical signals travel along your nerves. Small electrode stickers are placed on your skin, and brief electrical pulses are delivered to stimulate specific nerves. The test records how quickly the signal travels from one electrode to another and how strong it is when it arrives. Think of it like checking the speed and quality of an electrical wire — if the signal is slow or weak, it suggests the nerve's insulation (myelin) or the nerve fiber itself is damaged.
Electromyography (EMG) evaluates the electrical activity of your muscles. A very thin needle electrode is inserted into specific muscles to record their electrical signals both at rest and during contraction. A healthy resting muscle should be electrically silent — like a quiet room. If damaged nerves are supplying a muscle, the EMG will pick up abnormal electrical activity even when you're not moving, like hearing static on a radio. According to the Cleveland Clinic, the needle acts like a microphone — it only records, it doesn't deliver electrical stimulation.
Why Your Doctor Ordered This Test
If you're experiencing symptoms like tingling, numbness, burning pain, muscle weakness, or the classic signs of neuropathy, your doctor needs to understand exactly what's happening at the nerve level — and that's something a physical exam alone can't fully determine. Here's what electrodiagnostic testing can reveal:
⚡ Nerve Conduction Study
Measures nerve signal speed and strength
Surface electrode stickers on skin
Feels like brief static shocks
~30–45 minutes
📍 Needle EMG
Records muscle electrical activity
Thin needle electrode inserted into muscles
Feels like a brief pinch per insertion
~20–40 minutes
Confirming or ruling out neuropathy. While your symptoms may strongly suggest neuropathy, other conditions can mimic nerve damage. An EMG and NCS can confirm whether peripheral nerve damage is actually present.
Determining the type of nerve damage. These tests can distinguish between damage to the nerve's insulation (demyelinating neuropathy) and damage to the nerve fiber itself (axonal neuropathy). This distinction matters because different types of neuropathy have different causes and respond to different treatments.
Identifying the location of damage. Is the problem at the nerve root (where it exits the spine), along the nerve's pathway, or at the nerve endings? Is it affecting one nerve or many? These tests can pinpoint where along the nervous system things are going wrong.
Assessing severity. The results help your doctor understand how much nerve damage has occurred and may provide clues about whether it's reversible. This information is crucial for planning treatment and understanding what stage your condition may be at.
Diagnosing specific conditions. EMG and NCS can help identify conditions including diabetic neuropathy, carpal tunnel syndrome, ulnar neuropathy, Guillain-Barré syndrome (GBS), Charcot-Marie-Tooth disease, radiculopathy (pinched nerve in the spine), and many other neuromuscular conditions.
How to Prepare for Your Test
Good preparation can make a real difference in both your comfort and the accuracy of the results. Here's what to do (and not do) before your appointment:
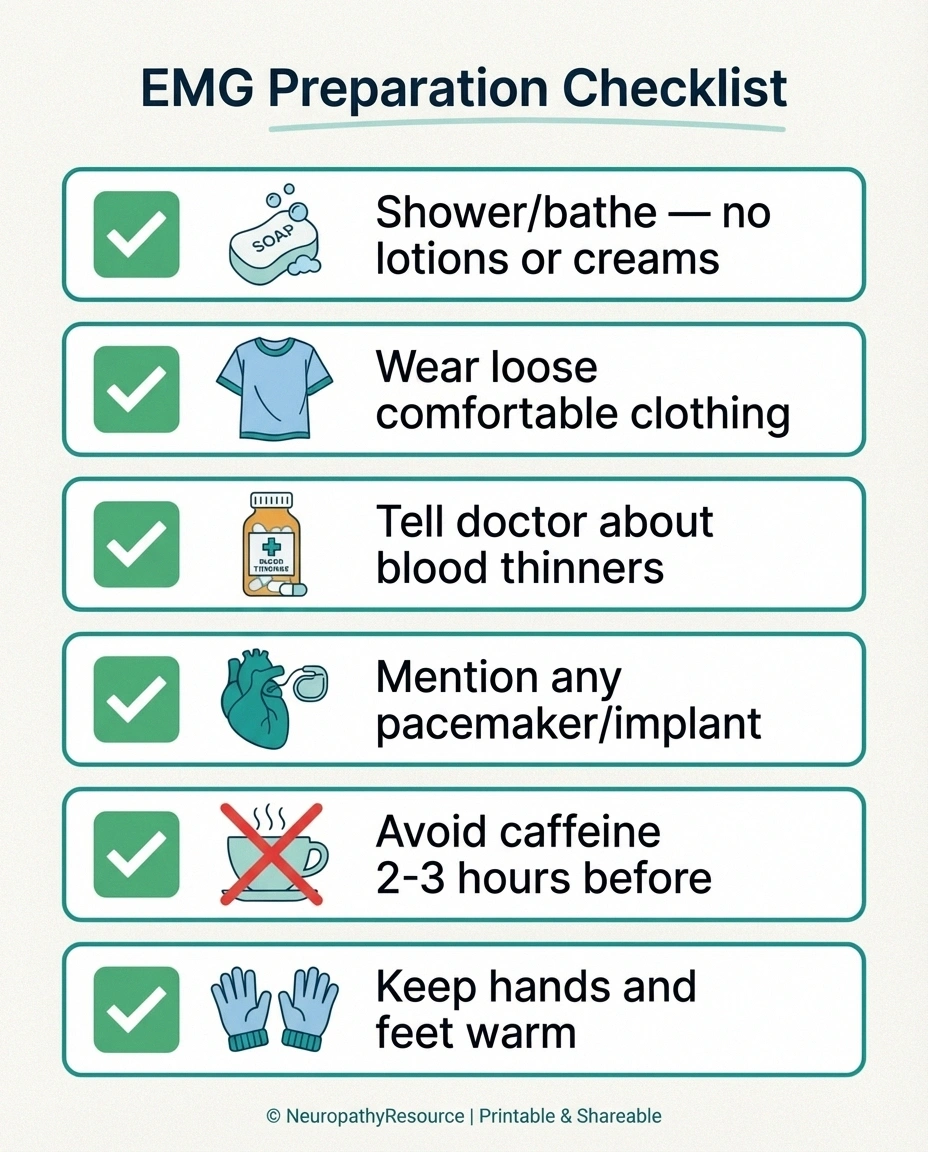
Shower or bathe before the test. Clean skin is important because the surface electrodes need good contact with your skin. Don't apply any lotions, creams, oils, or perfumes to your arms or legs on the day of the test — these create a barrier that can interfere with the electrical signals and reduce accuracy.
Wear comfortable, loose-fitting clothing. You may need to expose your arms and legs for electrode placement. Loose shorts and a short-sleeved shirt, or clothing that can be easily rolled up, works well. Some facilities provide a gown.
Tell your doctor about your medications. Blood thinners (anticoagulants) like warfarin don't necessarily need to be stopped, but your doctor should know about them because the needle portion of the test carries a small bleeding risk. If you take pyridostigmine (Mestinon), ask whether it should be held before the test. Don't stop any medication without first checking with the prescribing doctor.
Mention any implanted devices. If you have a pacemaker, defibrillator, or other implanted electrical device, inform the testing team. These typically don't prevent the test from being performed, but the technician may need to take precautions.
Avoid caffeine and cigarettes for two to three hours before the test if your doctor advises it, as these substances can affect nerve and muscle activity.
Stay warm. Cold muscles and nerves conduct signals more slowly, which can affect your results. If it's cold outside, wear warm clothing and try to keep your hands and feet warm on the way to your appointment. Some labs even have warming devices available if your extremities are cold when you arrive.
What Happens During the Nerve Conduction Study
The nerve conduction study is usually performed first. Here's exactly what to expect, step by step:

What Happens Step by Step
Electrode Sticker Placement
Small flat electrodes are placed on your skin along nerve pathways in hands, feet, arms, or legs.
Nerve Conduction Testing
Brief electrical pulses are delivered — feels like static electricity. Your muscles may twitch. Several nerves are tested.
Needle EMG
Thin needle inserted into muscles (brief pinch). You'll rest, then flex the muscle while the doctor listens to the electrical activity.
Results Discussion
The neurologist often shares preliminary findings immediately. Full written report goes to your referring doctor within days.
You'll sit or lie down on an examination table in a comfortable position. The technician or neurologist will identify the nerves they need to test based on your symptoms. They'll place small, flat electrode stickers on your skin at specific points along the nerve's pathway — typically on your hands, feet, arms, or legs.
The testing device will deliver brief, low-voltage electrical pulses through one electrode while recording the nerve's response at another. Each pulse produces a quick sensation that most people describe as a mild shock or a “static electricity” feeling, similar to a rubber band snapping against your skin. The sensation is brief — lasting only a fraction of a second — and while surprising, it's rarely described as truly painful.
You may notice your muscles twitching involuntarily during each pulse. This is completely normal — the electrical stimulation is activating the nerve, which in turn triggers the muscle. The twitching is part of what's being measured.
The technician will test several nerves, stimulating at different points along each nerve's path. For a typical neuropathy evaluation, they'll likely test nerves in both your arms and both your legs. The entire nerve conduction portion usually takes about thirty to forty-five minutes.
What Happens During the EMG (Needle Exam)
After the nerve conduction study, the neurologist will perform the needle EMG. This part of the test provides different but complementary information about how your muscles are functioning.

The neurologist will insert a very thin needle — about the diameter of an acupuncture needle — through your skin and into specific muscles. Each needle contains a tiny electrode that records the electrical activity of the muscle. Unlike the nerve conduction study, no electrical stimulation is delivered through the needle. It's purely a recording device.
You'll feel a brief pinch or sting when the needle goes in, similar to getting a blood draw. Some muscles are more sensitive than others — feet and hands tend to be the most uncomfortable, while larger muscles in the arms and legs are typically easier. Most people describe the discomfort as “annoying but tolerable” rather than severely painful.
The neurologist will listen to your muscle's electrical activity through a speaker (it sounds like static or crackling), and watch the wave patterns on a screen. They'll ask you to rest the muscle completely, then contract it gently, then squeeze harder. They're looking at how the muscle behaves at each stage.
Here's what the neurologist is listening and watching for:
At rest: A healthy muscle should be electrically quiet. If the neurologist hears spontaneous electrical activity when you're relaxing the muscle, it may indicate nerve damage is causing the muscle fibers to fire on their own — a sign of denervation.
During gentle contraction: The pattern of electrical signals tells the neurologist about the health of individual motor units — the connection between a nerve fiber and the muscle fibers it controls.
During maximum effort: How many motor units are firing and how they're organized reveals whether nerve damage is limiting the number of working connections to the muscle.
Each muscle is typically tested for one to two minutes. The neurologist will test several muscles — usually anywhere from six to twelve depending on what they're looking for. The needle exam portion usually takes about twenty to forty minutes.
Does It Hurt? An Honest Answer
Let's address the question everyone really wants answered. Yes, there is some discomfort involved — it would be dishonest to say otherwise. But the level of discomfort is usually much less than people fear. Here's a realistic picture:
What Patients Say
“EMG testing may result in some discomfort, but it is usually well tolerated without any need for pain medication.” — Hospital for Special Surgery. Most patients report the test was better than expected. The nerve conduction shocks are startling but brief, and the needle portion feels like a quick pinch followed by mild pressure.
The nerve conduction study feels like brief electrical shocks. Most people describe them as startling more than painful. The intensity varies — testing some nerves requires a stronger stimulus than others. The shocks to motor nerves (which cause muscle twitching) tend to feel stronger than those testing sensory nerves. But each shock lasts less than a second, and you get brief breaks between stimulations.
The needle EMG involves multiple small needle insertions. The insertion itself feels like a quick pinch. Once the needle is in position, you may feel a mild ache or pressure, but many people feel nothing at all. The most uncomfortable moments tend to be when the needle is repositioned to sample different areas of the same muscle.
Here's what may help with the discomfort: breathe steadily and try to relax your muscles — tension makes the needle portion harder. Let the neurologist know if you're struggling — they can adjust their approach, take breaks, or provide reassurance. Focus on the fact that the test is temporary and provides valuable information about your condition. Remember that most people who've had the test say it was better than they expected.
According to Hospital for Special Surgery, EMG testing “may result in some discomfort, but it is usually well tolerated without any need for pain medication.”
After the Test: What to Expect
The good news is that recovery from an EMG is minimal. Here's what's normal afterward:
You may have some muscle soreness in the areas that were tested with the needle. This is similar to the soreness you might feel after exercising a muscle you don't normally use. It usually resolves within a few hours, though some people experience mild tenderness for a day or two.
You might see small bruises where the needles were inserted. This is more common if you take blood thinners but can happen to anyone. The bruises are harmless and resolve on their own.
You can resume all normal activities immediately — driving, working, exercise, bathing. No special post-test care is needed. There are no lasting effects from the electrical stimulation or the needle insertions.
If you experience unusual swelling, increasing pain, warmth, or redness at any of the needle sites, contact your doctor — while infection is extremely rare (the needles are single-use and sterile), it's good to be aware.
Understanding Your Results
The neurologist who performs your test will analyze the data and prepare a report for your referring doctor. In many cases, the neurologist will share preliminary findings with you right after the test. Here's what the results might show:
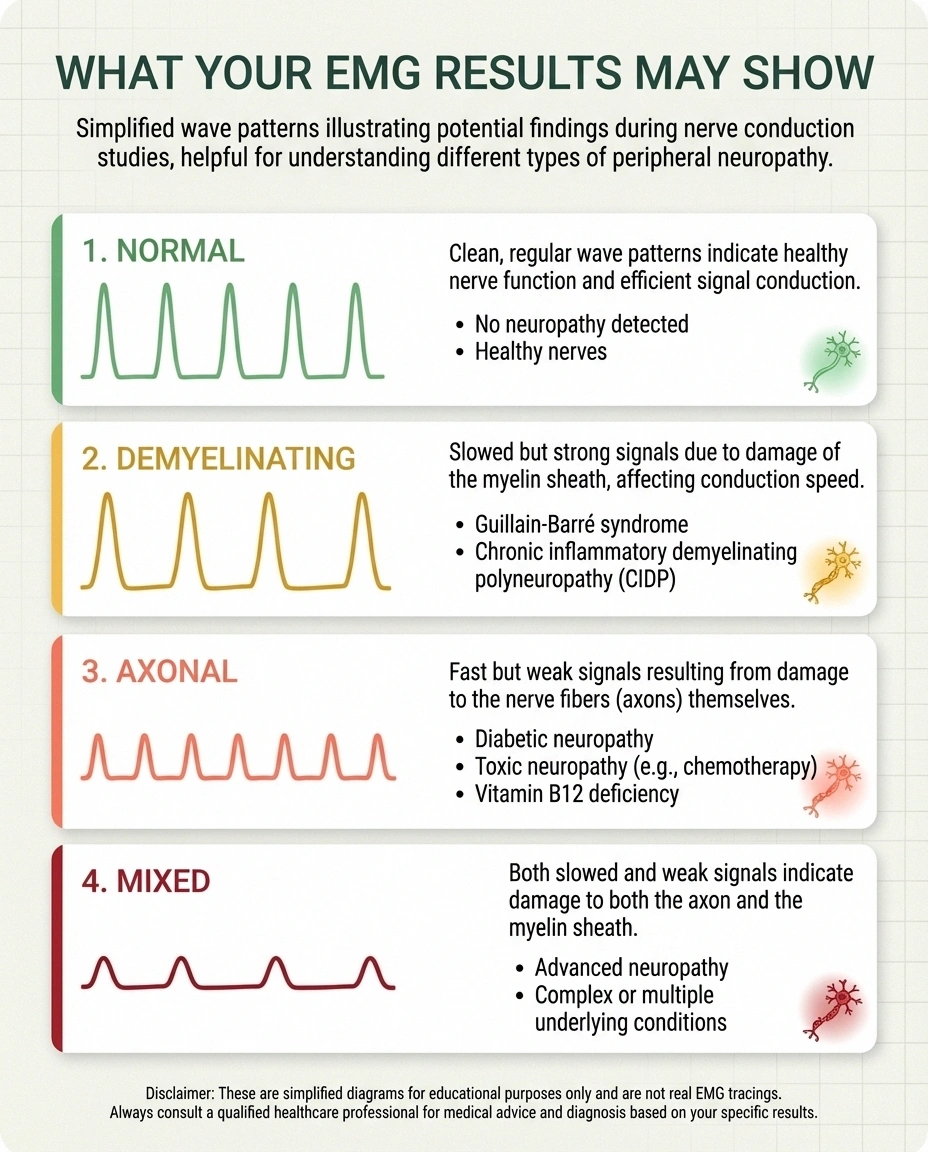
Normal Results
If your nerve conduction velocities and EMG findings are normal, it means the large nerve fibers and muscles tested are functioning properly. This doesn't necessarily mean nothing is wrong — small fiber neuropathy, for example, affects nerve fibers too small to be detected by standard EMG and NCS. If your symptoms are real but your tests are normal, your doctor may pursue additional testing like a skin punch biopsy or autonomic testing.
Demyelinating Pattern
If the nerve conduction study shows significantly slowed conduction velocities with relatively preserved signal strength, it suggests damage to the myelin sheath — the insulation around your nerves. This pattern is seen in conditions like GBS autoimmune neuropathy, chronic inflammatory demyelinating polyneuropathy (CIDP), and Charcot-Marie-Tooth disease. Demyelinating neuropathies often respond well to treatment because the underlying nerve fiber may still be intact.
Axonal Pattern
If the nerve conduction study shows reduced signal strength (amplitude) with relatively normal speed, it suggests damage to the nerve fibers themselves. This is the pattern seen in most cases of diabetic neuropathy, alcoholic neuropathy, nutritional deficiency neuropathy, and many other common forms of peripheral neuropathy.
Focal vs. Generalized
The test can also reveal whether nerve damage is concentrated in a specific area (focal, like carpal tunnel or ulnar neuropathy) or spread throughout the body (generalized, like diabetic polyneuropathy). This distinction is critical because focal neuropathies may be treatable with surgery or targeted interventions, while generalized neuropathies require systemic treatment.
Active vs. Chronic Damage
The EMG needle exam can distinguish between active (ongoing) nerve damage and chronic (old, stable) damage. Signs of active denervation suggest that nerve damage is continuing, which may prompt more aggressive treatment. Signs of chronic reinnervation suggest that your nerves have stabilized and are attempting to compensate — a more encouraging finding.
What These Tests Cannot Tell You
While EMG and nerve conduction studies are powerful diagnostic tools, they have important limitations:

Important Limitation
Standard EMG and nerve conduction studies CANNOT detect small fiber neuropathy (SFN). If your tests come back normal but you have burning pain, temperature sensitivity, or tingling, ask your doctor about a skin punch biopsy — the gold standard for diagnosing SFN. A normal EMG doesn't mean your symptoms aren't real.
They only test large nerve fibers. The standard EMG and NCS are designed to evaluate the larger, myelinated nerve fibers. If you have small fiber neuropathy — which affects the tiny unmyelinated C-fibers responsible for pain and temperature sensation — these tests may come back completely normal even though you have significant symptoms. If this happens, ask your doctor about a skin punch biopsy, which can detect small fiber damage.
They don't always identify the cause. The tests can confirm that nerve damage exists and characterize its pattern, but they can't always tell you why it's happening. Your doctor will use the EMG results alongside blood tests, your medical history, and other evaluations to determine the underlying cause.
They provide a snapshot in time. The results reflect your nerve function on the day of the test. Nerve damage can fluctuate, and early or very mild neuropathy might not yet show up on these tests. If your symptoms continue but initial tests were normal, your doctor may recommend repeating the tests in six to twelve months.
They don't measure pain directly. These tests measure nerve function — not your subjective experience of pain. You can have significant pain with only mild abnormalities on EMG, or significant EMG abnormalities with relatively little pain. The tests complement your symptom description; they don't replace it.
Common Concerns and Myths
“The test will make my neuropathy worse.” This is a common fear but is not supported by evidence. The electrical stimulation used in nerve conduction studies and the needle insertions used in EMG do not cause nerve damage. While you may feel temporarily more symptomatic from the stimulation, this settles within hours. The test does not change the course of your neuropathy.
“My friend said it was the most painful thing they've ever experienced.” People's pain tolerance varies enormously, and anxiety can amplify the perception of discomfort. While a small number of patients do find the test quite uncomfortable, the vast majority describe it as “not as bad as I expected.” Individual experiences differ, but going in with realistic expectations — some discomfort but generally tolerable — is the most accurate framework.
“An EMG can diagnose anything wrong with my nerves.” As discussed above, standard EMG and NCS cannot detect small fiber neuropathy, and they may miss very early or mild nerve damage. They're excellent tests, but they have limitations. A normal result doesn't always mean your nerves are fine — it means the specific nerve fibers tested are functioning within normal limits.
“I need to stop my medications before the test.” In most cases, you should continue taking your regular medications. The main exceptions are blood thinners (which need to be discussed with your doctor due to bleeding risk from the needle) and pyridostigmine (Mestinon). Always ask the testing facility about medication instructions when you schedule your appointment.
How EMG Results Guide Your Treatment
Your EMG results don't just sit in a file — they actively shape your treatment plan. Here's how:
Key Takeaway
Your EMG results serve as a medical baseline for tracking your nerve health over time. Request a copy of the full report — it contains objective data that helps multiple specialists understand your condition and can be compared to future tests to monitor progression or improvement.
If the test confirms peripheral neuropathy, your doctor will likely order blood work to identify treatable causes: vitamin deficiencies, thyroid problems, diabetes or prediabetes, autoimmune markers, and other metabolic issues.
If the pattern suggests a treatable condition like Guillain-Barré nerve disorder or CIDP, your doctor may recommend immunotherapy treatments that can halt or reverse the damage.
If the test shows carpal tunnel syndrome or another focal compression, surgical decompression may be recommended. The EMG results help determine whether surgery is likely to be beneficial.
If the test shows stable chronic neuropathy without active damage, the focus may shift to symptom management — medications like gabapentin or duloxetine, physical therapy, and lifestyle modifications.
The EMG serves as a baseline that can be compared to future tests if needed, allowing your medical team to track whether your neuropathy is progressing, stable, or improving with treatment.
Frequently Asked Questions
How long does the entire test take?
Most EMG and nerve conduction study appointments last sixty to ninety minutes total, though this can vary depending on how many nerves and muscles need to be tested. Simple evaluations (like checking for carpal tunnel) may be done in thirty minutes, while comprehensive neuropathy workups may take closer to ninety minutes.
Who performs the test?
EMG and nerve conduction studies are typically performed by a neurologist or physiatrist (a doctor specializing in physical medicine and rehabilitation) with specialized training in electrodiagnostic medicine. In some practices, a trained technician performs the nerve conduction study, and the physician performs the needle EMG and interprets all results.
Can I drive home after the test?
Yes. There's no sedation involved, and the test doesn't affect your ability to drive. You can return to all normal activities immediately after the appointment, including work and exercise.
Will my insurance cover the test?
Most insurance plans, including Medicare, cover EMG and nerve conduction studies when they're medically necessary — which they typically are when ordered by a doctor for symptoms like numbness, tingling, weakness, or pain. Check with your insurance provider about any copay or prior authorization requirements.
Can I have an EMG if I have a pacemaker?
Yes, in most cases. The nerve conduction study may need to be modified slightly to avoid interference with the pacemaker, but the needle EMG is generally safe. Always inform the testing team about any implanted devices before the test begins. According to the Hospital for Special Surgery, pacemakers and defibrillators will not create complications in most cases.
How soon will I get results?
The neurologist performing the test often shares preliminary findings immediately after the exam. A formal written report is typically sent to your referring doctor within a few days to a week. Schedule a follow-up with your doctor to discuss the results and next steps.
What if my EMG is normal but I still have symptoms?
A normal EMG doesn't mean your symptoms aren't real. It means the large nerve fibers tested are functioning normally. You may have small fiber neuropathy, early-stage nerve damage not yet detectable on standard tests, or a condition that doesn't show up on EMG. Your doctor may recommend additional testing like a skin punch biopsy, autonomic testing, or MRI depending on your specific symptoms.
Making the Most of Your Appointment
A few final tips to help you get the most value from your electrodiagnostic testing:
Bring your symptom history. Write down when your symptoms started, where exactly you feel them, what makes them better or worse, and any progression you've noticed. The neurologist performing the test will use this information to decide which nerves and muscles to test.
Bring a list of medications and supplements. Include everything you take, including over-the-counter medications and neuropathy supplements. Some supplements and medications can affect nerve function and may be relevant to interpreting your results.
Ask questions. Don't be afraid to ask the neurologist to explain what they're finding during the test. Many neurologists are happy to share preliminary observations and explain what the patterns mean. Understanding your results in real time can reduce anxiety and help you feel more in control.
Request a copy of the full report. When the formal results are ready, ask for your own copy. This is valuable if you see multiple specialists, want a second opinion, or need to track your condition over time. The report contains objective data that provides a medical baseline for your nerve function.
EMG and nerve tests distinguish neuropathy from fibromyalgia studies are a key part of the neuropathy diagnostic process. They're not fun, but they're rarely as bad as people fear — and the information they provide is genuinely important for getting the right diagnosis and the right treatment plan. Walk into your appointment prepared, breathe through the uncomfortable moments, and remember that you're taking a proactive step toward understanding and managing your nerve health.


