When someone receives a multiple myeloma diagnosis, neuropathy is probably not the first thing on their mind. Cancer treatment, prognosis, the road ahead — these understandably dominate the conversation. But for a large percentage of people living with multiple myeloma, nerve damage becomes a significant and sometimes debilitating part of their experience — caused either by the cancer itself or by the very medications used to fight it.
Understanding the connection between multiple myeloma and neuropathy matters for several reasons. It helps patients recognize symptoms early, when they're most likely to be manageable. It helps in conversations with oncologists about treatment choices. And it prepares people for what to watch for so they can advocate effectively for themselves throughout treatment.
Let's walk through what's happening, why it happens, and what can be done about it.
What Is Multiple Myeloma?
Multiple myeloma is a cancer of plasma cells — a type of white blood cell found in the bone marrow that normally produces antibodies to help fight infections. In myeloma, malignant plasma cells multiply out of control and crowd out healthy blood cells. They also produce abnormal proteins — often called M proteins or paraproteins — that can cause widespread damage throughout the body.
Multiple myeloma is the second most common blood cancer, diagnosed in approximately 35,000 Americans each year. Treatment has improved dramatically over the past two decades, with many patients now living for many years after diagnosis. But that longer survival also means more time living with treatment-related side effects — including neuropathy.
Two Distinct Causes of Neuropathy in Multiple Myeloma
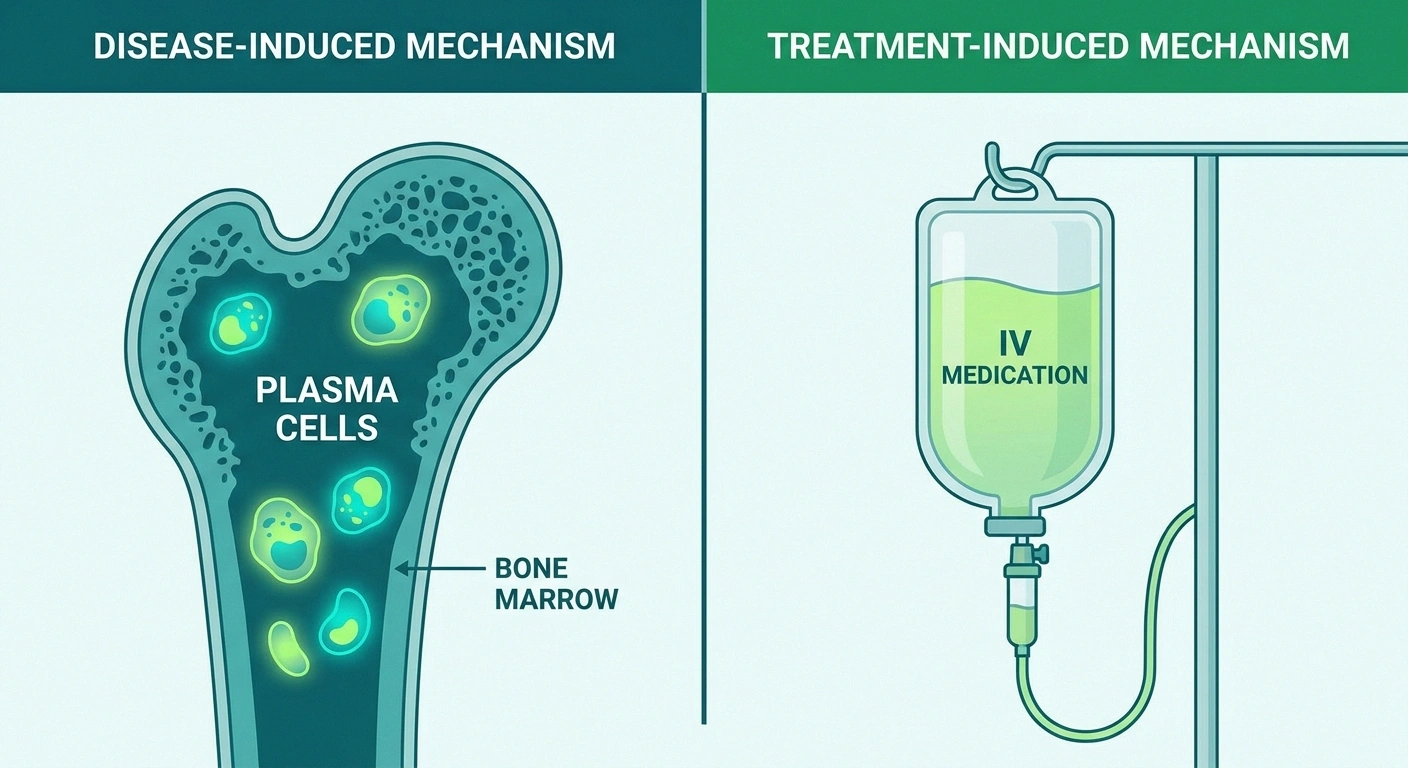
When a myeloma patient develops neuropathy, it's important to understand which mechanism is responsible — because the treatment implications differ. There are two main pathways:
Neuropathy in myeloma has two distinct causes — the disease itself and the drugs used to treat it. Understanding which cause is driving your symptoms matters for choosing the right management approach.
1. Disease-Induced Neuropathy
The cancer itself can damage nerves through several mechanisms:
Paraprotein deposits: The abnormal M proteins produced by malignant plasma cells can deposit in and around peripheral nerves, directly damaging the myelin sheath — the protective coating that allows nerve signals to travel efficiently. This paraprotein-associated neuropathy can cause a mix of sensory and motor symptoms and may progress as the disease advances.
Amyloidosis: In some myeloma patients, abnormal proteins form misfolded protein aggregates called amyloid fibrils that deposit in nerves, blood vessels, and organs. AL amyloidosis (amyloid light chain disease) is closely associated with multiple myeloma and can cause a distinctive painful peripheral neuropathy, often accompanied by autonomic symptoms affecting the heart, gut, and blood pressure.
Blood hyperviscosity: High levels of paraprotein in the blood can make it thicker, slowing blood flow and reducing oxygen delivery to peripheral nerves — leading to ischemic nerve damage.
Nerve compression: Myeloma lesions in the bone — particularly in the spine — can compress nerve roots or the spinal cord, causing radiculopathy or myelopathy rather than true peripheral neuropathy, though the symptoms can overlap.
Overall, approximately 20-25% of multiple myeloma patients develop neuropathy directly from the disease. This neuropathy tends to be sensorimotor in character — affecting both sensation and movement — and may involve autonomic features in AL amyloidosis cases.
2. Treatment-Induced Neuropathy
Ironically, some of the most effective drugs for treating multiple myeloma are among the most neurotoxic. Treatment-induced peripheral neuropathy is far more common than disease-induced neuropathy in myeloma patients, affecting a significant majority of those receiving certain regimens.
Newer agents like daratumumab have significantly lower neuropathy rates — an important consideration in treatment planning.
Thalidomide was one of the first disease-modifying drugs in multiple myeloma and remains in use. It causes peripheral neuropathy in an estimated 70-80% of patients with long-term use — a strikingly high rate. Thalidomide neuropathy typically affects sensation more than motor function, is length-dependent (feet before hands), and can be permanent if not recognized and managed early.
Bortezomib (Velcade) is a proteasome inhibitor that kills cancer cells by causing a toxic buildup of protein in them — but this same mechanism can damage peripheral nerve cells. Bortezomib-induced neuropathy occurs in 30-60% of patients. It tends to be painful, sensory-predominant, and in many cases partially reversible after dose reduction or discontinuation, particularly when caught early.
Ixazomib (Ninlaro) is a newer oral proteasome inhibitor in the same drug class as bortezomib. It causes neuropathy, though at somewhat lower rates than its predecessor — approximately 20-30% of patients develop it.
Vincristine is an older chemotherapy agent still used in some myeloma regimens. It causes a well-recognized peripheral neuropathy that is typically sensory at first and can progress to include motor involvement and autonomic symptoms. Vincristine neuropathy can be severe and is not always fully reversible.
Pomalidomide (Pomalyst) is related to thalidomide but generally produces less neuropathy — though it remains a consideration.
Newer agents, including daratumumab and carfilzomib, have significantly lower neuropathy risk profiles — an important reason why treatment options have expanded and quality of life has improved for many myeloma patients in recent years.
The overlap of medication-induced neuropathy with disease-caused nerve damage creates a complex picture that requires ongoing monitoring and individualized management.
Symptoms: What Neuropathy Feels Like in Myeloma Patients

The symptoms of neuropathy in multiple myeloma vary somewhat based on the cause, but common presentations include:
Sensory symptoms (most common):
- Numbness and tingling in feet and hands — the classic “glove and stocking” distribution seen in length-dependent neuropathies
- Burning or aching pain, particularly in the feet
- Electric shock sensations or sharp, shooting pain
- Heightened sensitivity to touch — even light contact can be painful
- Reduced ability to feel temperature changes, increasing the risk of burns or injuries going unnoticed
Motor symptoms (less common initially, but important to watch for):
- Muscle weakness, particularly in the feet and lower legs
- Difficulty with fine motor tasks — buttoning shirts, gripping objects
- Balance problems and increased fall risk
- Foot drop in severe cases
Autonomic symptoms (particularly in AL amyloidosis-associated neuropathy):
- Postural hypotension — dizziness when standing up
- Constipation or diarrhea — altered gut motility
- Urinary problems
- Abnormal sweating
- Heart rhythm irregularities
Early recognition of these symptoms is critical. The earlier neuropathy is identified, the more treatment options are available and the better the chances of limiting permanent damage — especially for treatment-induced neuropathy, where dose modification or drug changes can be made before irreversible damage accumulates.
Why Early Reporting Matters So Much

In the context of multiple myeloma treatment, early reporting of neuropathy symptoms to your oncologist isn't just a quality-of-life issue — it's a strategy to preserve nerve function.
Early intervention dramatically improves the chance of reversibility:
- New tingling, numbness, or burning in hands or feet during treatment
- Increasing difficulty walking, gripping, or performing fine motor tasks
- Balance problems or increased falls
- Dizziness when standing (possible autonomic involvement)
- Any sensation changes that are interfering with daily function
For bortezomib and thalidomide in particular, neuropathy is dose-dependent. The more drug you receive over time, the more likely significant neuropathy becomes. But if neuropathy is caught early and the dose is reduced or the drug is temporarily held, nerve damage often stabilizes or partially reverses. Wait until symptoms are severe, and permanent damage is far more likely.
Many oncology centers now routinely use formal neuropathy assessment tools — grading neuropathy from Grade 1 (mild, no functional impairment) through Grade 4 (life-threatening) — to guide treatment decisions. You can help your care team by reporting symptoms specifically and early, rather than minimizing them out of concern about disrupting your cancer treatment.
Your oncologist needs to know. Your cancer treatment is important — but so is your ability to walk, balance, and use your hands. In most cases, dose modifications can be made that maintain meaningful anti-myeloma activity while significantly reducing neuropathy risk.
Diagnosis: How Myeloma-Related Neuropathy Is Evaluated
Diagnosing neuropathy in a myeloma patient involves several components:
Clinical assessment: A detailed history of symptom onset (before or after treatment?), distribution, character, and progression, combined with a neurological examination testing reflexes, sensation, coordination, and strength.
EMG and nerve conduction studies: These tests measure how well electrical signals travel through your nerves and muscles, and can characterize whether neuropathy is primarily sensory or motor, and whether it involves demyelination (damage to the nerve's coating) or axonal injury (damage to the nerve fiber itself). This distinction matters for understanding prognosis and mechanism. Understanding your EMG results can help you engage more meaningfully with your neurologist.
Laboratory evaluation: Relevant blood work includes M protein quantification, free light chain assay, comprehensive metabolic panel, complete blood count, vitamin B12 levels, and in some cases, testing for AL amyloid.
Nerve biopsy: In selected cases where the cause of neuropathy is unclear or amyloidosis is suspected, a nerve biopsy may be performed to look for amyloid deposits or other pathological changes.
Skin punch biopsy: This simpler test can assess small fiber nerve density — a useful tool when small fiber neuropathy is suspected (particularly in early or subtle cases).
Management and Treatment Approaches

Managing neuropathy in the context of multiple myeloma requires coordination between oncology, neurology, and often pain management. The strategies depend on whether the neuropathy is disease-induced or treatment-induced:
For bortezomib specifically, subcutaneous administration (under the skin) has been shown to cause significantly less neuropathy than intravenous administration — with equivalent anti-cancer activity. Asking your oncologist about this option is appropriate if you're starting or continuing bortezomib.
For Treatment-Induced Neuropathy
Dose modification: The most impactful intervention when symptoms are caught early. Reducing the dose or changing the administration schedule of the offending drug — without abandoning effective cancer treatment — is often possible. For bortezomib specifically, subcutaneous administration (injected under the skin rather than intravenously) has been shown to produce significantly less neuropathy than IV administration, and is now standard practice where possible.
Drug substitution: If neuropathy is progressing despite dose modifications, switching to a regimen with lower neuropathy risk — such as substituting ixazomib for bortezomib, or transitioning to daratumumab-based regimens — may be appropriate. This decision requires balancing cancer control with quality of life and must involve your oncologist.
Symptomatic Pain Management
Once neuropathy is established, several approaches can help manage symptoms while cancer treatment continues:
Gabapentinoids: Gabapentin and pregabalin are frequently used for neuropathic pain in myeloma patients, as in other forms of peripheral neuropathy. They need to be dosed appropriately for renal function, which can be affected by myeloma.
Tricyclic antidepressants: Amitriptyline and nortriptyline can help with neuropathic pain but require caution in older patients due to side effects.
SNRIs: Duloxetine is particularly worth discussing with your oncology team — it has evidence for chemotherapy-induced neuropathy specifically.
Topical treatments: Capsaicin cream, lidocaine patches, and compounded topical formulations can provide localized relief without significant systemic effects — an important consideration for patients already managing a complex medication burden.
Nutritional Support
Nutritional deficiencies can compound neuropathy in myeloma patients, who are at elevated risk for malnutrition during active treatment. Vitamin deficiency — particularly B12 — can both mimic and worsen neuropathy independently of the myeloma itself. Ensuring adequate B12, B1, B6, and D levels is important.
Alpha-lipoic acid has been studied as a potential protective supplement against chemotherapy-induced neuropathy, with some positive findings. While evidence is not definitive, it's considered low-risk and is used by many oncology centers as an adjunct. Discuss with your oncologist before adding supplements, as some can interfere with chemotherapy.
Physical and Occupational Therapy
Physical therapy for balance, strength, and fall prevention is important for myeloma patients with motor or proprioceptive neuropathy. Occupational therapy can help with adaptive strategies for hand weakness or sensory changes affecting daily function. Both should ideally be part of a comprehensive supportive care plan.
Living With Neuropathy During Myeloma Treatment

For many people, neuropathy becomes a companion to their myeloma journey — something to manage and adapt to rather than something that disappears. This is genuinely hard, and I don't want to minimize that.
Inspect your feet daily for cuts, blisters, or pressure marks you may not have felt
Test bath water with your elbow, not your foot — temperature sensitivity may be reduced
Use grab bars, non-slip mats, and adequate lighting to reduce fall risk
Report any new or worsening neuropathy symptoms to your oncologist at your next appointment — or sooner if they're significant
Some practical considerations that can make a real difference:
Foot care: Careful foot care is critical when you have numbness — you may not feel injuries as they happen. Inspect your feet daily, protect them from temperature extremes, and wear well-fitted shoes.
Fall prevention: Balance problems from neuropathy significantly increase fall risk, particularly concerning given the bone fragility that often accompanies myeloma. Grab bars in the bathroom, removing trip hazards, and using mobility aids appropriately can prevent serious injury.
Temperature precautions: Reduced ability to sense temperature means hot baths, heating pads, and hot pavement can cause burns before you realize it. Home safety modifications specifically for temperature sensitivity are worth implementing.
Keep your team informed: Don't minimize symptoms when talking to your oncology team. If your neuropathy is affecting your daily function — your ability to walk, use your hands, work, or sleep — that's critical information for treatment decision-making.
Frequently Asked Questions
Is myeloma-related neuropathy reversible?
It depends on the cause and how quickly it's caught. Bortezomib-induced neuropathy caught early and managed with dose modification often partially or substantially reverses over months after treatment adjustment. Thalidomide neuropathy is less predictable and can be permanent. Disease-induced neuropathy may improve if the underlying myeloma responds well to treatment, but amyloidosis-related neuropathy tends to be more fixed. Early reporting to your oncologist gives you the best chance of reversibility.
Should I ask my oncologist about my neuropathy risk before starting treatment?
Absolutely yes. Before starting any myeloma regimen, asking about the neuropathy risk profile of the proposed drugs — and what monitoring and dose-modification protocols are in place — is appropriate and important. If you already have some baseline neuropathy (from diabetes, for example), this should factor prominently into treatment selection.
Can I take supplements to protect my nerves during myeloma treatment?
Some supplements have been studied for nerve protection during chemotherapy — alpha-lipoic acid and B vitamins most prominently. However, some supplements can interact with myeloma drugs or interfere with treatment efficacy. Always discuss supplements with your oncologist before starting them during active treatment. This is not an area to self-treat without guidance.
How is myeloma neuropathy different from diabetic neuropathy?
Both can produce similar sensory symptoms (numbness, tingling, burning in feet and hands), but the mechanisms differ. Diabetic neuropathy is driven by sustained metabolic damage from elevated blood sugar. Myeloma neuropathy may be driven by paraprotein deposits on nerves, amyloidosis, blood hyperviscosity, or neurotoxic drugs. The treatment approaches also differ accordingly. An accurate diagnosis of cause matters for appropriate management.
My myeloma is in remission — will my neuropathy improve?
It may. When disease-induced neuropathy is present, achieving remission and reducing the paraprotein burden can allow some nerve recovery. However, recovery is variable and often incomplete, particularly if significant nerve damage has already occurred. Treatment-induced neuropathy may also improve after the neurotoxic drugs are stopped or reduced, depending on the extent of damage.
The Bottom Line
Neuropathy in multiple myeloma is common, underreported, and often inadequately managed — not because effective approaches don't exist, but because patients may not know to report early symptoms, and because the focus during active cancer treatment is understandably on the disease itself.
Understanding that neuropathy can come from both the disease and its treatment, recognizing symptoms early, reporting them honestly to your oncology team, and accessing supportive care from neurology, physical therapy, and pain management — these steps can make a meaningful difference in both quality of life and long-term nerve outcomes.
You're already dealing with a lot. Neuropathy doesn't have to be the silent, unmanaged part of your myeloma experience. Advocate for your nerves the same way you advocate for your cancer care — because managing both well matters for the life you're fighting to live.