When I first heard that an antidepressant might help with my neuropathy pain, I had a lot of questions. My brain and my feet seemed like completely separate problems. Why would a medication for depression have anything to do with the burning in my toes?
The answer, it turns out, has to do with how the brain processes pain — and how certain antidepressants work on exactly the same neurotransmitter systems that turn the volume up or down on nerve signals. Venlafaxine, sold as Effexor, is one of the medications that researchers have studied for neuropathic pain. It's not a first-line choice, and it won't work for everyone, but for some people it offers real relief when other options haven't.
If your doctor has mentioned venlafaxine, or if you're exploring options beyond gabapentin or pregabalin, this article will walk you through what the research actually says, what dosing looks like for nerve pain, what side effects to expect, and how it compares to similar medications.
What Is Venlafaxine (Effexor)?
Venlafaxine is a prescription antidepressant in a class called SNRIs — Serotonin-Norepinephrine Reuptake Inhibitors. It's FDA-approved for major depressive disorder, generalized anxiety disorder, social anxiety disorder, and panic disorder. It is not FDA-approved for neuropathic pain — but it's commonly prescribed off-label for exactly that purpose, and a meaningful body of clinical research supports this use.
Key Takeaway
Venlafaxine (Effexor) is FDA-approved for depression and anxiety — but it's regularly prescribed off-label for neuropathic pain. The pain-relieving mechanism is distinct from the antidepressant mechanism and requires higher doses to activate.
You may recognize the brand names Effexor and Effexor XR (the extended-release version, which most patients take). The extended-release formulation is generally preferred because it's taken once daily and tends to have fewer side effects than the immediate-release version.
Venlafaxine belongs to the same drug class as duloxetine (Cymbalta), another SNRI that is FDA-approved for diabetic neuropathy. The two medications work through very similar mechanisms, but there are meaningful differences in how they're used, their side effect profiles, and what the research shows.
How Does Venlafaxine Work for Nerve Pain?
Understanding why an antidepressant relieves nerve pain requires a brief detour into pain neuroscience. This is actually fascinating, and it changed how I think about pain medication in general.
How Venlafaxine Dose Affects Pain Relief
37.5 – 75 mg/day — Low Dose
Primarily serotonergic effect. Mood and anxiety benefit likely; pain relief minimal at this range. This is why low doses “don't work” for neuropathy.
75 – 150 mg/day — Moderate Dose
Norepinephrine activity begins. Some analgesic benefit appears. This is a transition zone — often where initial pain response is assessed.
150 – 225 mg/day — Therapeutic Pain Range
Strong noradrenergic effect. Research shows 30-50% pain reduction vs placebo at this range. This is the target dose for neuropathic pain.
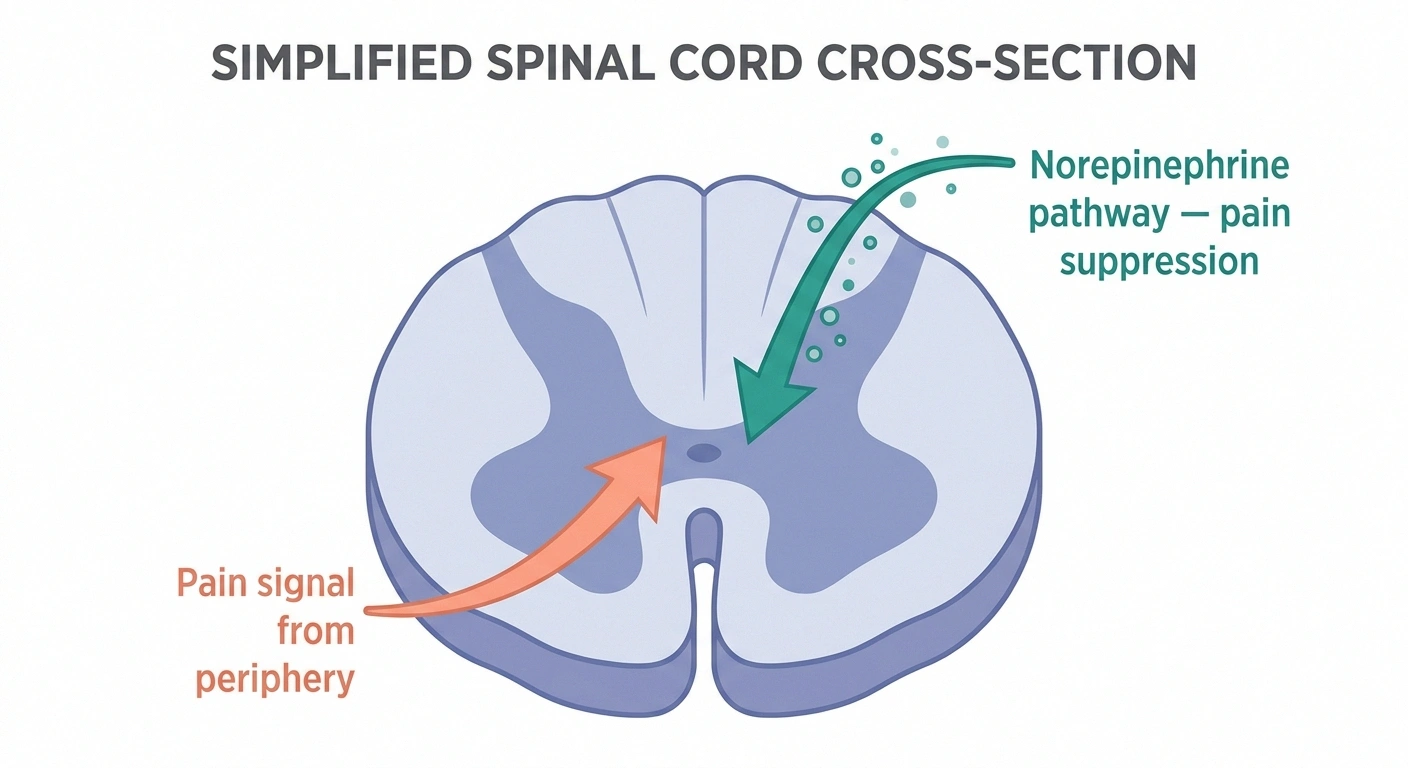
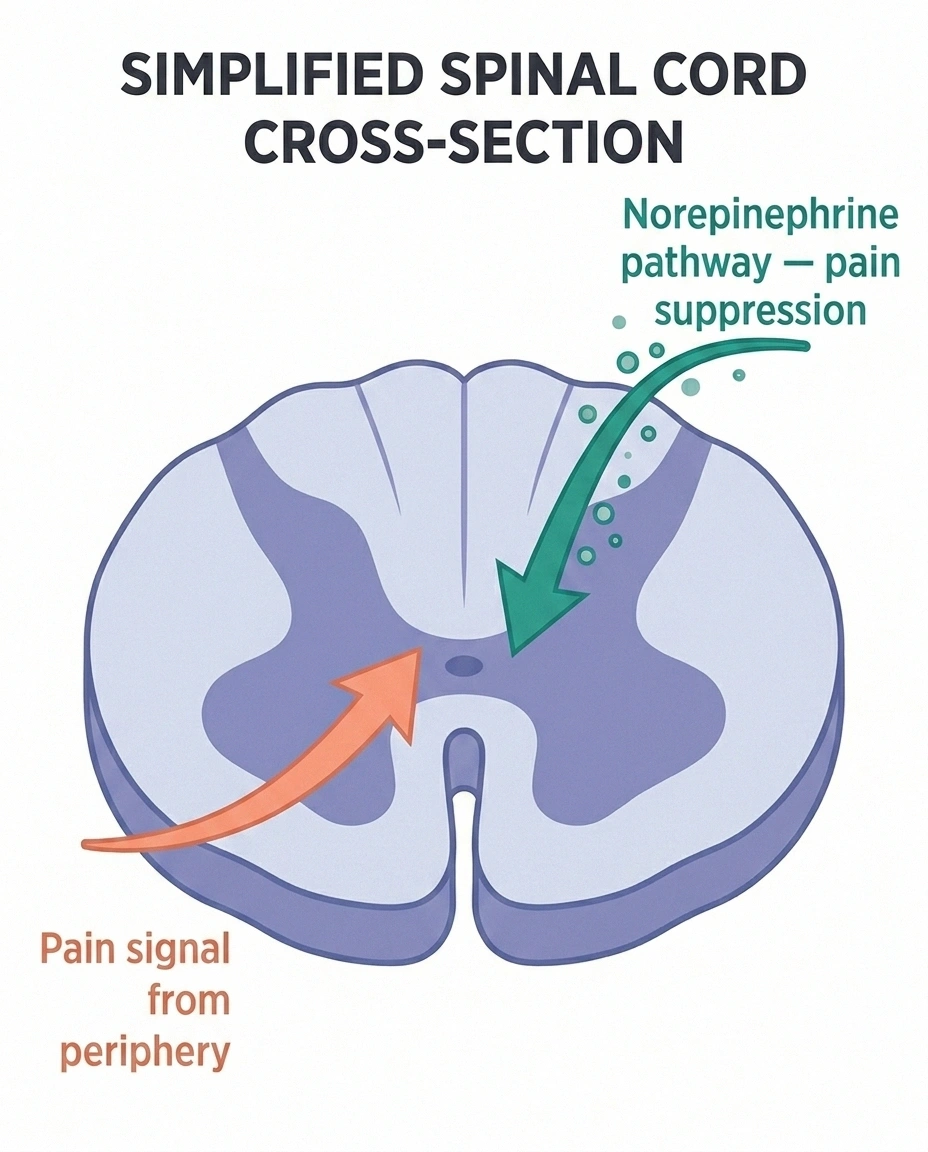
Your brain isn't a passive receiver of pain signals — it actively modulates them. There are descending pathways in the spinal cord that can either amplify or suppress incoming pain signals before they reach conscious awareness. These pathways use two key neurotransmitters: serotonin and norepinephrine.
When norepinephrine is abundant in these descending pain pathways, it tends to suppress pain signals — turning down the volume. SNRIs like venlafaxine prevent the reuptake of both serotonin and norepinephrine, leaving more of these neurotransmitters available in the synapse. The result, particularly from the norepinephrine side, is enhanced descending pain inhibition.
Here's the key detail that matters for dosing: at lower doses, venlafaxine is primarily serotonergic — it's acting like an antidepressant. At higher doses (150mg and above), its noradrenergic activity kicks in substantially. This is why the analgesic effect is strongly dose-dependent, and why studies consistently show that the pain relief from venlafaxine requires doses higher than what's typically used for depression alone.
This is not a placebo effect, and it's not incidental. The same mechanism is why duloxetine, the better-studied SNRI cousin, got FDA approval for diabetic peripheral neuropathy. Venlafaxine is working through the same biological pathway — it just hasn't gone through the FDA approval process for this specific indication.
What Does the Research Show?
The evidence base for venlafaxine in neuropathic pain is real, though not without caveats.
🔎 Research Says
A systematic review in Pain Medicine (2017) found venlafaxine at 150-225 mg/day produced 30-50% pain reduction compared to placebo in neuropathic pain — a clinically meaningful effect size comparable to other established neuropathic pain medications.
A landmark trial published in Neurology compared venlafaxine to imipramine (a tricyclic antidepressant) in patients with painful polyneuropathy. Venlafaxine produced clinically meaningful pain reduction and was comparable in efficacy to imipramine — with a more favorable side effect profile, since imipramine carries significant cardiac risks that venlafaxine largely avoids.
A systematic review published in Pain Medicine (2017) analyzed the existing controlled trials and found that at doses of 150-225 mg/day, venlafaxine produced a 30-50% reduction in neuropathic pain compared to placebo — a magnitude of effect that's clinically meaningful. The review characterized the effect as “mild to moderate analgesic.”
A Cochrane-style review (available through NIH PMC) looked at the available evidence more broadly and concluded that while there are fewer high-quality trials than exist for gabapentin or duloxetine, the data consistently point in the same direction: venlafaxine at adequate doses reduces neuropathic pain in a meaningful proportion of patients.
The honest picture: venlafaxine is not the most extensively studied option for neuropathic pain — duloxetine and gabapentin have larger evidence bases. But the available evidence is generally positive, and venlafaxine occupies an important clinical niche: patients for whom duloxetine wasn't effective or wasn't tolerated, or who have comorbid depression and anxiety alongside their neuropathy.
Who Might Benefit Most from Venlafaxine?

Venlafaxine isn't appropriate for everyone with neuropathy, and it's certainly not a first-line treatment. But there are specific situations where it becomes a particularly sensible option to discuss with your doctor:
When duloxetine didn't work or wasn't tolerated
Duloxetine (Cymbalta) is the SNRI with FDA approval for diabetic neuropathy, so doctors typically try it first in this class. But not everyone responds to duloxetine, and its side effects (nausea, fatigue, liver enzyme elevation) cause some people to stop. Venlafaxine may have a slightly different tolerability profile for some individuals, and it's reasonable to try when duloxetine fails.
When you have depression or anxiety alongside neuropathy
The coexistence of chronic pain and depression is extremely common — they share neurobiological pathways and reinforce each other. An SNRI addresses both simultaneously, potentially with a single medication rather than separate prescriptions. The mental health impact of neuropathy is significant, and having a medication that targets both is a meaningful advantage.
Chemotherapy-induced peripheral neuropathy (CIPN)
There is specific evidence for venlafaxine in CIPN, including a randomized trial showing meaningful pain reduction compared to placebo. For people dealing with chemo-induced neuropathy, venlafaxine is one of the options that some oncology teams reach for.
When pain is the primary driver, not the underlying cause
Venlafaxine treats pain symptoms, not the underlying nerve damage. In conditions where the cause can be addressed (like B12 deficiency or blood sugar management in diabetic neuropathy), those root cause interventions should always be the priority. Venlafaxine is a symptom management tool, not a disease-modifying therapy.
Dosing for Neuropathic Pain: What to Expect
The dosing protocol for neuropathic pain is different from what's used for depression, and understanding this is important for setting realistic expectations and avoiding disappointment if the initial low dose doesn't seem to be doing much.
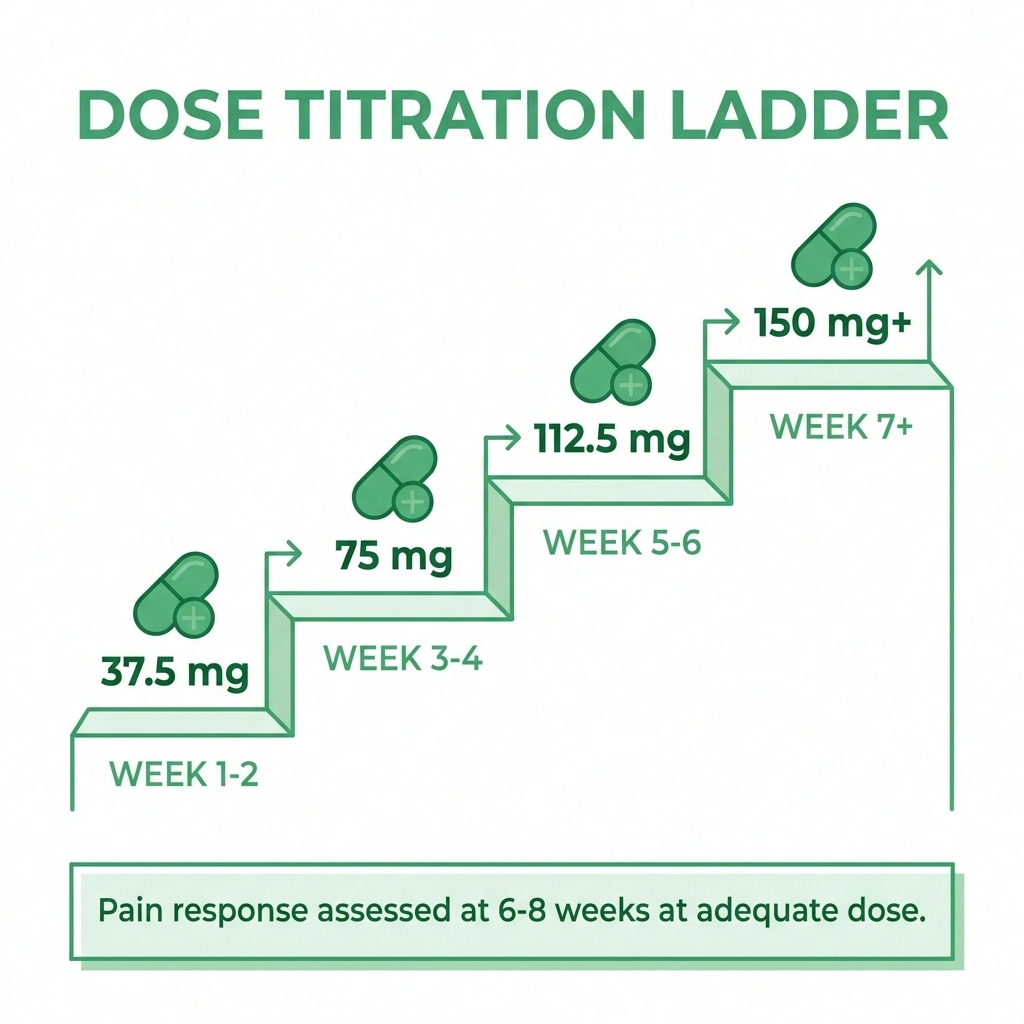
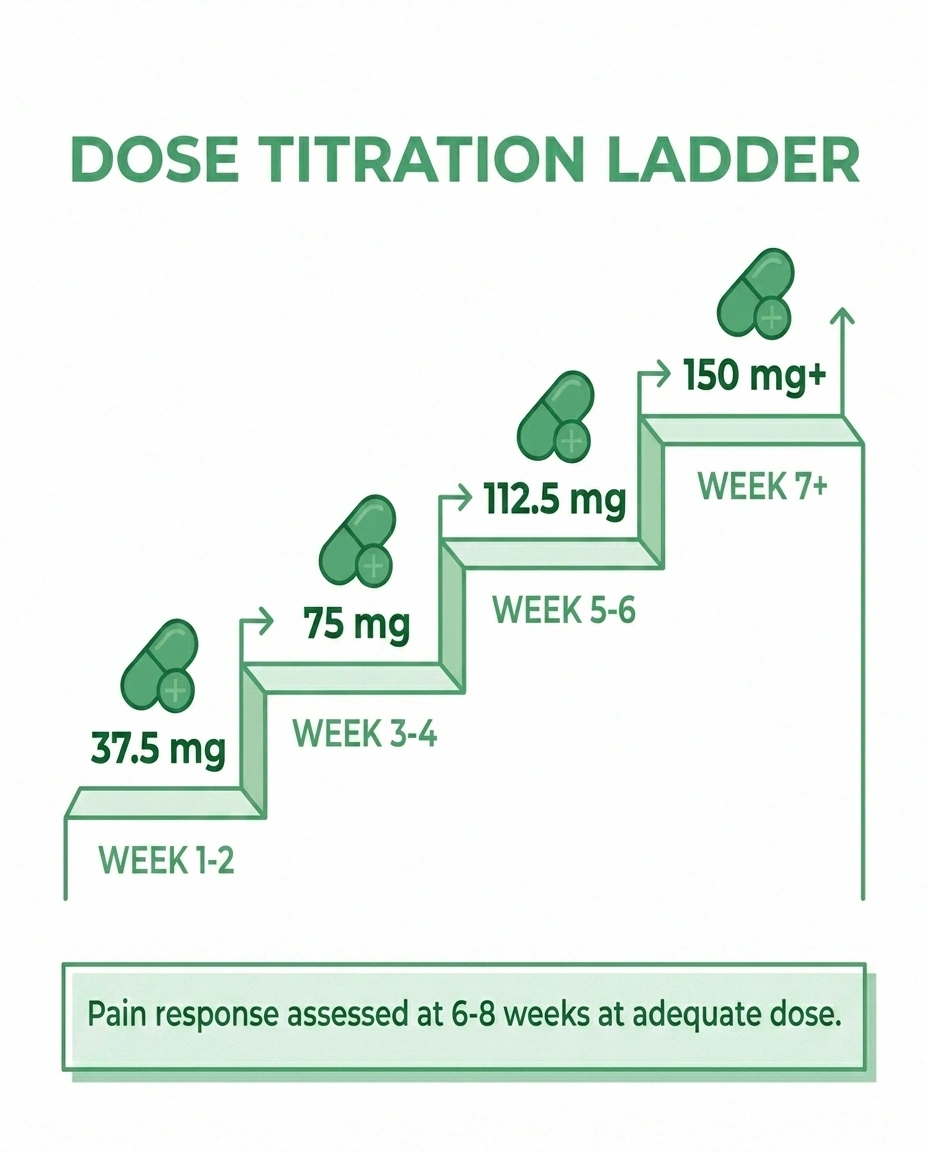
Starting Dose: 37.5 mg daily, taken with food to minimize nausea
Titration: Increase by 37.5 mg every 1-2 weeks as tolerated. Most protocols aim to reach at least 75 mg before evaluating response, and often 150 mg for the pain indication.
Target Range for Pain Relief: 75-150 mg/day (functional threshold); 150-225 mg/day for optimal noradrenergic pain effect
Timing: Extended-release (XR) formulation is taken once daily, usually in the morning. Immediate-release may be split into two daily doses.
Duration before assessing response: Give it 6-8 weeks at an adequate dose before concluding it isn't working. Pain medications in this class often require weeks to reach full effect, and it's very common for people to give up before reaching a therapeutic dose or waiting long enough.
One thing I want to emphasize: if you've been prescribed venlafaxine and you're still at 37.5 mg or 75 mg and not feeling improvement, this doesn't mean the drug doesn't work for you. You may simply not have reached the dose where the norepinephrine effect kicks in. Talk to your doctor about whether increasing the dose makes sense before concluding it's not effective.
Side Effects: What to Watch For

Venlafaxine has a real side effect profile, and being informed about it helps you navigate the first few weeks more successfully.
Never Stop Venlafaxine Suddenly
Discontinuation syndrome from abruptly stopping venlafaxine includes “brain zaps” (electric shock sensations), dizziness, nausea, and intense irritability. Even missing a single dose can trigger early symptoms. Always taper slowly under your doctor's guidance — do not stop on your own.
Nausea is the most common early side effect. It tends to be most intense in the first 1-2 weeks and often diminishes substantially with time. Taking the medication with food helps. Starting at a lower dose and titrating slowly also reduces nausea significantly. Most people who experience early nausea find it manageable if they stick with it.
Headache and dizziness are common early on, particularly around dose increases. These typically settle.
Sweating — often increased sweating, including at night — is a recognized side effect that can persist throughout treatment. For some people this is minor; for others it's bothersome enough to affect the decision to continue.
Sexual side effects are dose-dependent and can include decreased libido, delayed orgasm, and erectile dysfunction. These are among the most common reasons SNRIs are discontinued. Worth discussing honestly with your doctor.
Blood pressure elevation — venlafaxine at higher doses can increase blood pressure modestly. This is why it requires monitoring, particularly in patients with pre-existing hypertension. At the doses typically used for neuropathy (150-225 mg), the effect is usually small but should be tracked.
Discontinuation syndrome is an important and often underemphasized consideration. Stopping venlafaxine suddenly — or even missing doses — can cause a specific, uncomfortable syndrome: dizziness, electric shock-like sensations (“brain zaps”), flu-like symptoms, irritability, and insomnia. This medication must be tapered slowly, not stopped abruptly. Always work with your doctor on a tapering plan if you decide to stop.
Venlafaxine vs. Duloxetine: The SNRI Comparison
Since both are SNRIs prescribed for neuropathic pain, this comparison comes up frequently.
Venlafaxine vs. Duloxetine: Quick Comparison
| Factor | Venlafaxine (Effexor) | Duloxetine (Cymbalta) |
|---|---|---|
| FDA approval for neuropathy | Off-label use | Yes (diabetic neuropathy) |
| Evidence base | Moderate | Larger |
| Cost (generic) | Generally lower | Moderate |
| Typical use order | Second-line in this class | First-line SNRI |
| Discontinuation syndrome | Yes — taper required | Yes — taper required |
Duloxetine advantages: FDA-approved for diabetic peripheral neuropathy (and fibromyalgia), which means more insurance coverage and more clinical familiarity. Larger evidence base for neuropathic pain specifically.
Venlafaxine advantages: More flexible dosing. Generally lower cost (generic venlafaxine is widely available and inexpensive). Some patients tolerate one better than the other, which can only be determined by trying.
Clinical reality: Most doctors will try duloxetine first in this class because of FDA approval and familiarity. Venlafaxine is the logical next step when duloxetine fails or causes problems. Occasionally, venlafaxine is preferred upfront if the patient has tried duloxetine before for depression and didn't tolerate it.
Both medications have a discontinuation syndrome risk, both need to be tapered, and both require adequate dosing to produce pain relief. The choice between them is often individual and pragmatic.
Venlafaxine vs. Gabapentin and Pregabalin
These are different drug classes with different mechanisms and different side effect profiles.
Gabapentin/Pregabalin work by reducing the excitability of pain-signaling neurons via calcium channels. They're among the most commonly prescribed medications for neuropathic pain and have the largest evidence bases. Their main side effects are sedation, dizziness, weight gain, and cognitive fog.
Venlafaxine works by enhancing descending pain inhibition via norepinephrine. Its side effects are distinct (nausea, sweating, blood pressure) and some patients find them more manageable than gabapentin-class sedation.
In practice, many patients take combinations — the mechanisms are different enough that combination therapy sometimes works when single agents don't. This is a conversation to have with your doctor, as medication interactions need to be assessed individually.
Who Should Not Take Venlafaxine
There are several important contraindications and cautions:
- MAOIs: Do not take venlafaxine within 14 days of stopping an MAOI antidepressant (or vice versa). The combination can cause serotonin syndrome, which is a serious medical emergency.
- Uncontrolled hypertension: Venlafaxine can raise blood pressure. If your BP is poorly controlled, this needs to be addressed before starting.
- Bipolar disorder: Like all antidepressants, venlafaxine can potentially trigger a manic episode in people with bipolar disorder. Careful psychiatric evaluation is needed.
- Liver disease: Significant liver impairment affects venlafaxine metabolism; dosing adjustments are needed.
- Pregnancy: SNRI use during pregnancy requires a careful risk-benefit discussion with your doctor.
Always provide your doctor with a complete medication list before starting venlafaxine. It has several drug interactions worth checking, including with certain pain medications and some blood thinners. The questions to ask before starting neuropathy medication guide can help you prepare for that conversation.
How Long Does Venlafaxine Take to Work for Nerve Pain?

Patience is genuinely required here. Most people don't feel significant pain relief in the first two weeks — they may mostly feel the side effects of starting a new medication, which can be discouraging.
Patience Required
The two most common reasons venlafaxine “doesn't work” for neuropathy: stopping too soon (before 6-8 weeks at an adequate dose) or never reaching an adequate dose. Track your pain weekly on a simple 1-10 scale and bring that data to your next appointment.
Antidepressants for pain typically require:
- 2-4 weeks at any given dose to assess tolerability
- 6-8 weeks at an adequate dose to assess pain response
- Sometimes longer to see the full effect
The two most common reasons people conclude venlafaxine “didn't work” for neuropathy are: stopping too soon (before 6-8 weeks at an adequate dose), or never reaching an adequate dose. The noradrenergic pain relief mechanism requires 150 mg or more — at 37.5 or 75 mg, you're primarily getting an antidepressant effect, not the pain analgesic effect.
Track your pain on a simple scale (1-10) daily or weekly so you have objective data to bring to your doctor. This helps separate actual changes in pain from week-to-week variation.
Frequently Asked Questions
Is venlafaxine effective for neuropathic pain?
Research shows venlafaxine produces meaningful pain reduction in neuropathic pain at doses of 150-225 mg/day, with studies showing 30-50% pain reduction compared to placebo. It is not FDA-approved for this indication (it's used off-label), but it has a solid evidence base and is commonly prescribed for neuropathic pain when other options haven't worked or aren't tolerated. It's generally considered more effective at higher doses due to increased norepinephrine activity.
How long does venlafaxine take to work for neuropathy?
Most people need 6-8 weeks at an adequate dose (typically 150 mg or higher) to see meaningful pain relief. The first 2-4 weeks are largely about tolerating the side effects of starting the medication. Pain improvement tends to develop gradually rather than suddenly. Stopping too soon or staying at a low dose are the most common reasons the medication appears ineffective when it might have worked at a higher dose or with more time.
What dose of venlafaxine works for nerve pain?
The analgesic effect of venlafaxine is dose-dependent and tied to its noradrenergic activity, which kicks in substantially above 150 mg/day. Most clinical studies finding meaningful pain relief used doses of 150-225 mg/day. Starting doses (37.5 mg) produce primarily serotonergic effects and are unlikely to provide much pain relief. Titration should be slow — increasing by 37.5 mg every 1-2 weeks as tolerated.
What are the main side effects of venlafaxine?
The most common side effects are nausea (especially early, usually improves over 1-2 weeks), headache, dizziness, sweating, and sexual side effects including decreased libido and delayed orgasm. At higher doses, blood pressure elevation is possible. The most important caution is discontinuation syndrome — stopping venlafaxine suddenly causes a specific withdrawal-like reaction with brain zaps, dizziness, and flu-like symptoms. Always taper slowly under medical guidance.
How does venlafaxine compare to duloxetine for neuropathy?
Both are SNRIs that work through the same basic mechanism for pain. Duloxetine (Cymbalta) has FDA approval for diabetic peripheral neuropathy and a larger evidence base for neuropathic pain. Venlafaxine is typically tried when duloxetine doesn't work or isn't tolerated. Some patients tolerate one better than the other. Generic venlafaxine tends to be less expensive. The clinical choice between them is often pragmatic — try one, and if it fails or causes problems, try the other.
Can you stop venlafaxine suddenly?
No. Stopping venlafaxine abruptly commonly causes discontinuation syndrome, characterized by dizziness, electric shock sensations in the head (brain zaps), nausea, flu-like symptoms, and intense irritability. This syndrome is unpleasant but not medically dangerous. To avoid it, venlafaxine should be tapered gradually — typically by reducing the dose by 37.5 mg every 1-2 weeks, though the exact schedule depends on the dose and duration of treatment. Always work with your prescribing doctor on a tapering plan.
Is venlafaxine or gabapentin better for neuropathy?
They work through completely different mechanisms and have different side effect profiles, so this comparison is usually about which fits your specific situation better rather than which is objectively superior. Gabapentin tends to cause sedation, cognitive dulling, and weight gain. Venlafaxine tends to cause nausea, sweating, and has discontinuation syndrome concerns. Many patients end up trying both over the course of managing their neuropathy, and some benefit from combination therapy — a conversation to have with your doctor.