
One of the most frustrating things about living with neuropathy is trying to explain the pain to people who haven't experienced it. “It's like my feet are on fire.” “It feels like I'm walking on glass.” “Electric shocks shoot through my legs for no reason.” If you've said something like that, you're not alone — and you're not imagining it. Neuropathic pain is real, it's measurable, and there are concrete biological reasons why damaged nerves hurt the way they do.
What makes neuropathic pain so different from other types of pain is that it comes from the nervous system itself. When you stub your toe, pain signals follow a normal, predictable path — tissue damage triggers nerve endings, the signal travels to your brain, and you feel pain. When the injury heals, the pain stops. But with neuropathic pain, the nerves themselves are the source of the problem. They're sending pain signals not because of an injury happening right now, but because the wiring has been damaged and is misfiring.
In this article, I'll explain the science behind why damaged nerves cause pain, what the different types of neuropathic pain mean, and why understanding the mechanism matters for managing your symptoms effectively.
Normal Pain vs. Neuropathic Pain: Why They're Fundamentally Different
To understand neuropathic pain, it helps to first understand how pain is supposed to work.
The Broken Alarm Analogy
Normal pain is your body's alarm system detecting a real threat. Neuropathic pain is a broken alarm system — the wiring itself is damaged, generating false alarms even when there's no fire. This is why regular painkillers like ibuprofen often don't work: they're designed to put out fires, not fix broken alarms.
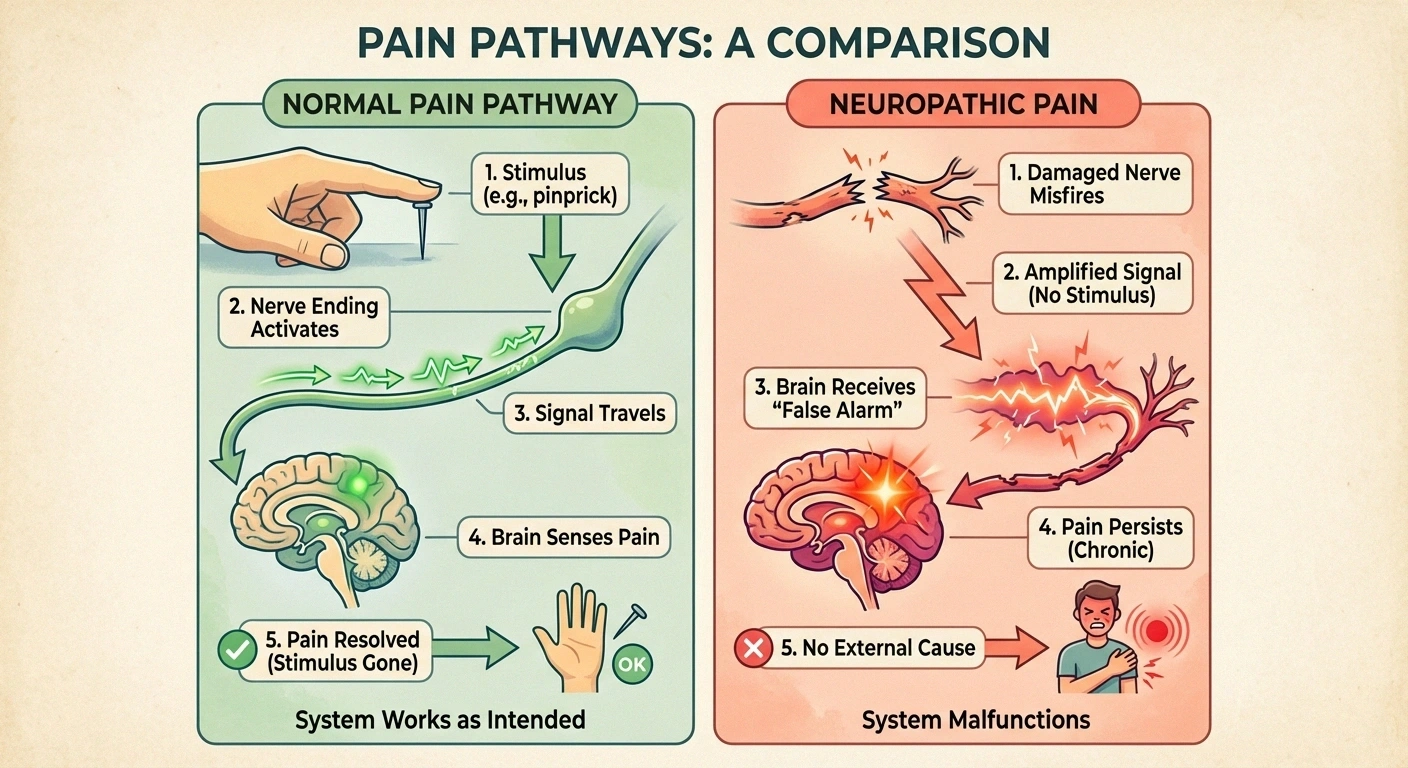
Normal pain (nociceptive pain) serves a protective function. You touch a hot stove, specialized nerve endings called nociceptors detect the danger, and they send a clear signal through your nerves to your spinal cord and brain: “Move your hand!” The pain is proportional to the threat, it has a clear cause, and it resolves when the cause is removed. This type of pain, while unpleasant, is your body's alarm system working exactly as designed.

Neuropathic pain is fundamentally different. Instead of the alarm system detecting a real threat, the alarm system itself is broken. The nerves that carry pain signals have been damaged by diabetes, chemotherapy, infection, or other causes, and now they're generating false alarms. The pain signals don't represent actual tissue damage happening in your feet or hands — they represent a nervous system that has been disrupted at its core.
This distinction matters because it affects treatment. Normal pain responds well to anti-inflammatory drugs like ibuprofen, because there's actual inflammation to treat. Neuropathic pain often doesn't respond to those same medications, because the problem isn't inflammation at the site — it's misfiring in the nerves themselves. That's why doctors often turn to medications like gabapentin or duloxetine that target the nervous system directly.
What Happens Inside a Damaged Nerve
When a peripheral nerve is damaged — whether gradually by high blood sugar or more acutely by chemotherapy — the changes that lead to pain happen at multiple levels. Let me walk you through the main mechanisms in language that makes sense.
Why Pain Gets Worse at Night
Reduced Sensory Input
Quiet rooms unmask pain signals
Cortisol Drops
Natural anti-inflammatory hits low point
Temperature Changes
Cooling extremities trigger nerve firing
Position Effects
Lying down affects nerve compression
Four Mechanisms Behind Neuropathic Pain
⚡
Ectopic Firing
Damaged nerves spark spontaneously
🔊
Sodium Channels
Volume knob turned past ten
↔️
Demyelination
Signals cross-talk between fibers
🚫
Lost Inhibition
Braking system fails (reduced GABA)
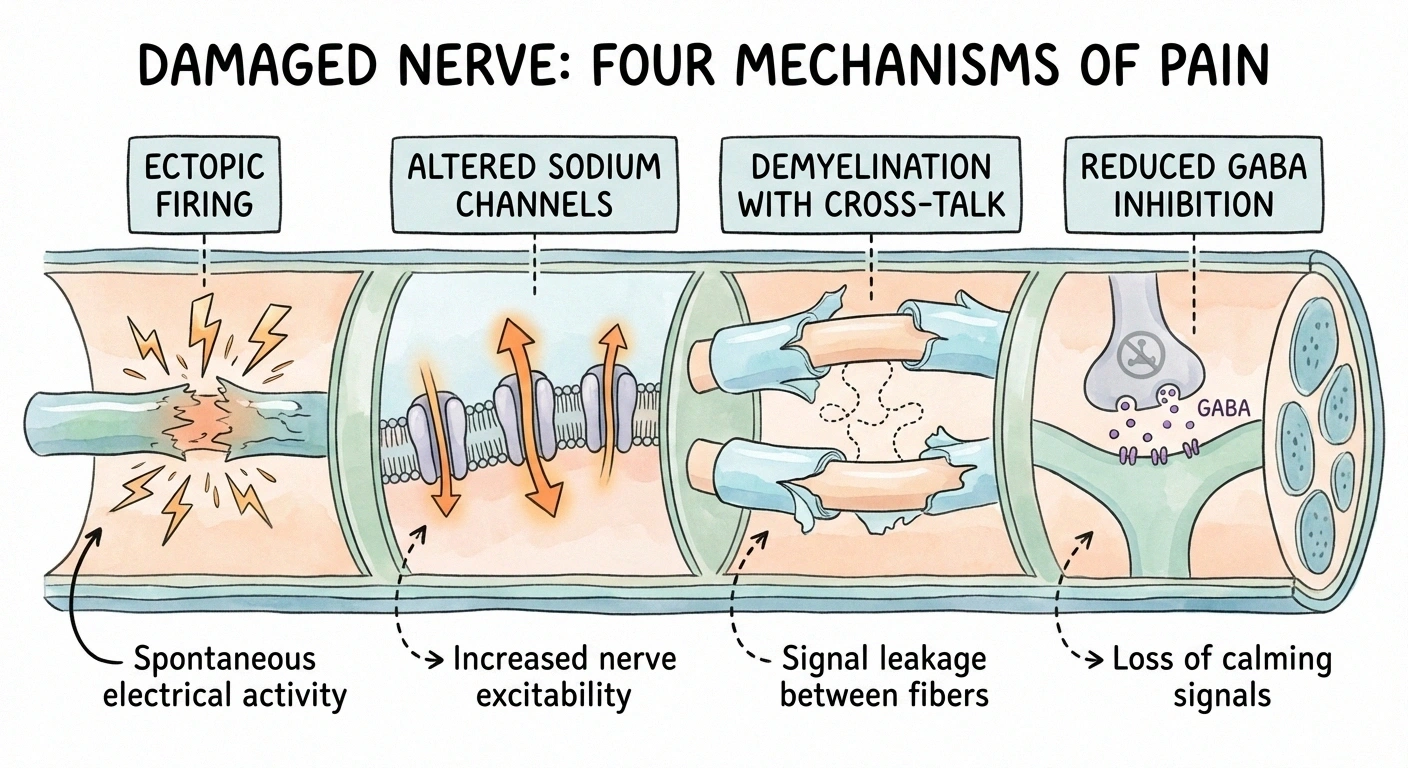
Ectopic firing. Healthy nerves only fire when they receive a genuine stimulus. But damaged nerve fibers can develop abnormal areas along their length that spontaneously generate electrical signals — like a frayed wire that sparks on its own. These random signals are interpreted by your brain as pain, even though nothing is touching or threatening your foot or hand. This is one reason neuropathic pain can seem to come from nowhere, including waking you up at night when you're perfectly still.
Sodium channel changes. Nerve signals are carried by the flow of sodium ions through tiny channels in the nerve membrane. When a nerve is damaged, the number and type of sodium channels change dramatically. The nerve ends up with more “excitable” channels that open more easily and stay open longer. The result: the nerve fires more readily, more intensely, and for longer than it should. It's like the volume knob on the nerve has been turned up past ten.
Demyelination effects. The myelin sheath that insulates nerve fibers doesn't just speed up signals — it also prevents signals from leaking between adjacent fibers. When myelin is damaged, signals can “cross-talk” between neighboring nerves. A touch signal traveling along one fiber can leak into a pain fiber next to it. This helps explain why even gentle pressure — like bed sheets on your feet — can trigger pain in neuropathy patients.
Loss of inhibitory control. Your nervous system has a built-in volume control. Certain nerve fibers (called inhibitory interneurons) constantly work to dampen and regulate pain signals, using a neurotransmitter called GABA. When neuropathy damages these control circuits, the braking system fails. Pain signals that would normally be muted now blast through at full volume. Research has shown that GABA function is reduced in the spinal cord of neuropathy patients, contributing directly to increased pain perception.
Central Sensitization: When Your Spinal Cord and Brain Amplify Pain
The changes in damaged peripheral nerves are only part of the story. Over time, persistent pain signals cause changes in the spinal cord and brain that amplify the pain experience even further. This process is called central sensitization, and understanding it is one of the most important things a neuropathy patient can learn.
Understanding Allodynia and Hyperalgesia
Allodynia: Pain from stimuli that shouldn't hurt at all — like the weight of bed sheets, a sock seam, or a gentle breeze on your skin.
Hyperalgesia: An exaggerated pain response — a small bump that normally causes mild discomfort becomes excruciating because the nervous system is amplifying every signal.
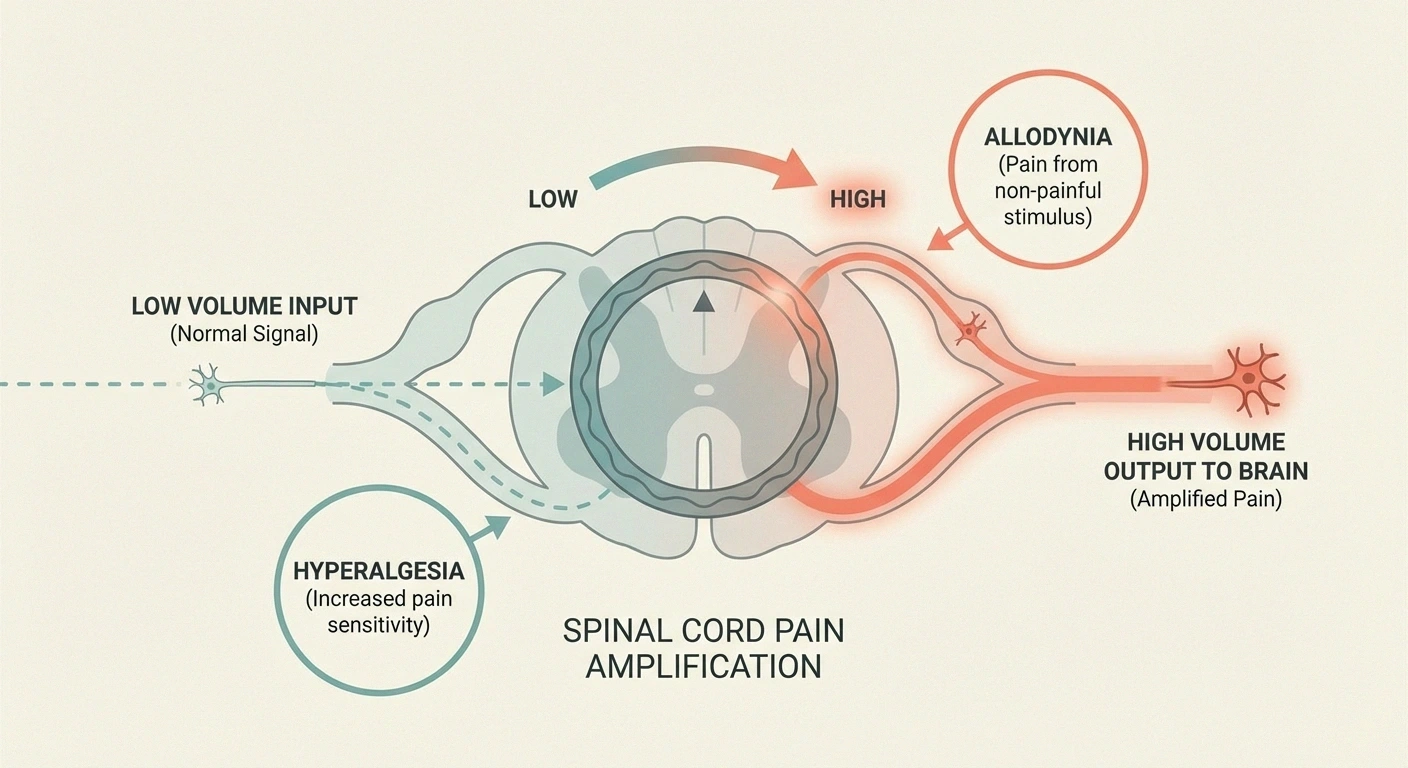
Here's how it works: when pain signals from damaged nerves repeatedly bombard the spinal cord neurons, those neurons gradually become more and more responsive. They start reacting to signals they would normally ignore. It's like a smoke detector that's been triggered so many times it becomes hypersensitive and starts going off when you toast bread.
This sensitization leads to two hallmark symptoms that many neuropathy patients recognize:
Allodynia — pain from stimuli that shouldn't be painful at all. The weight of a bed sheet, the seam of a sock, a gentle breeze on your skin. These sensations normally travel through non-pain pathways, but central sensitization rewires the spinal cord so that these signals get rerouted into pain circuits. If even light touch feels painful, allodynia is likely a factor.
Hyperalgesia — an exaggerated pain response to something that is mildly painful. A small bump that would normally make you wince becomes excruciating. The pain is disproportionate to the stimulus because the central nervous system is amplifying every signal.
There's also a phenomenon called wind-up, where repeated low-level stimulation causes a progressive escalation in pain intensity. If someone lightly taps the same spot on your foot repeatedly, each tap may feel more painful than the last — not because the tapping is getting harder, but because the spinal cord is ramping up its response with each signal.
Central sensitization is a key reason why neuropathic pain often gets worse over time and why it can be so difficult to treat. The pain is no longer just about the damaged nerves in your feet — it involves changes throughout the central nervous system.
What Different Types of Neuropathic Pain Mean
Neuropathic pain isn't one-size-fits-all. Most patients experience multiple types simultaneously, and each type provides clues about what's happening in the nervous system:
Pain Types and What They Indicate
Burning
Small C-fiber damage — constant, often worse at night
Electric Shock / Stabbing
Larger myelinated fiber misfiring — sudden, unpredictable jolts
Pins and Needles
Random sensory fiber activity — common in earlier stages
Deep Aching
Deeper sensory nerve involvement — sometimes confused with arthritis
Numbness with Pain
Different fiber types affected differently — worst of both worlds
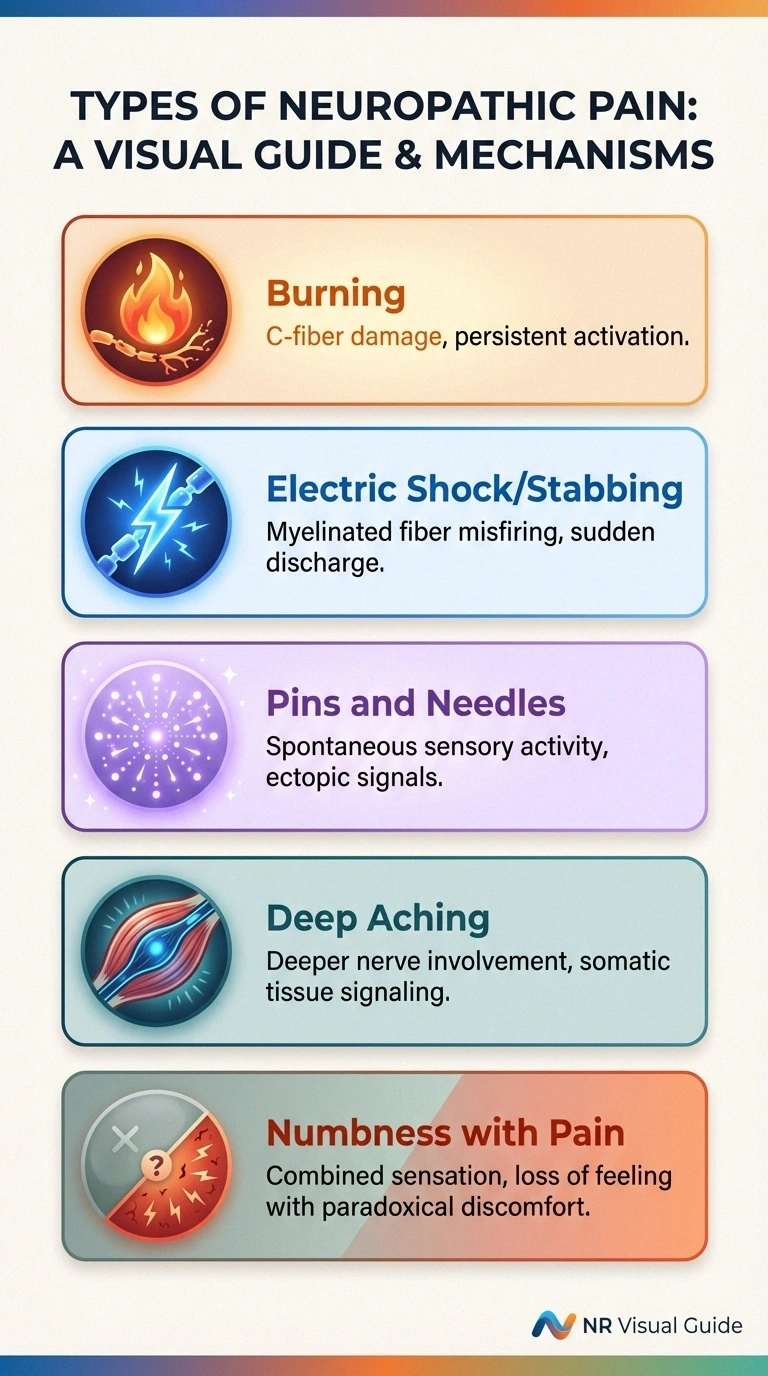
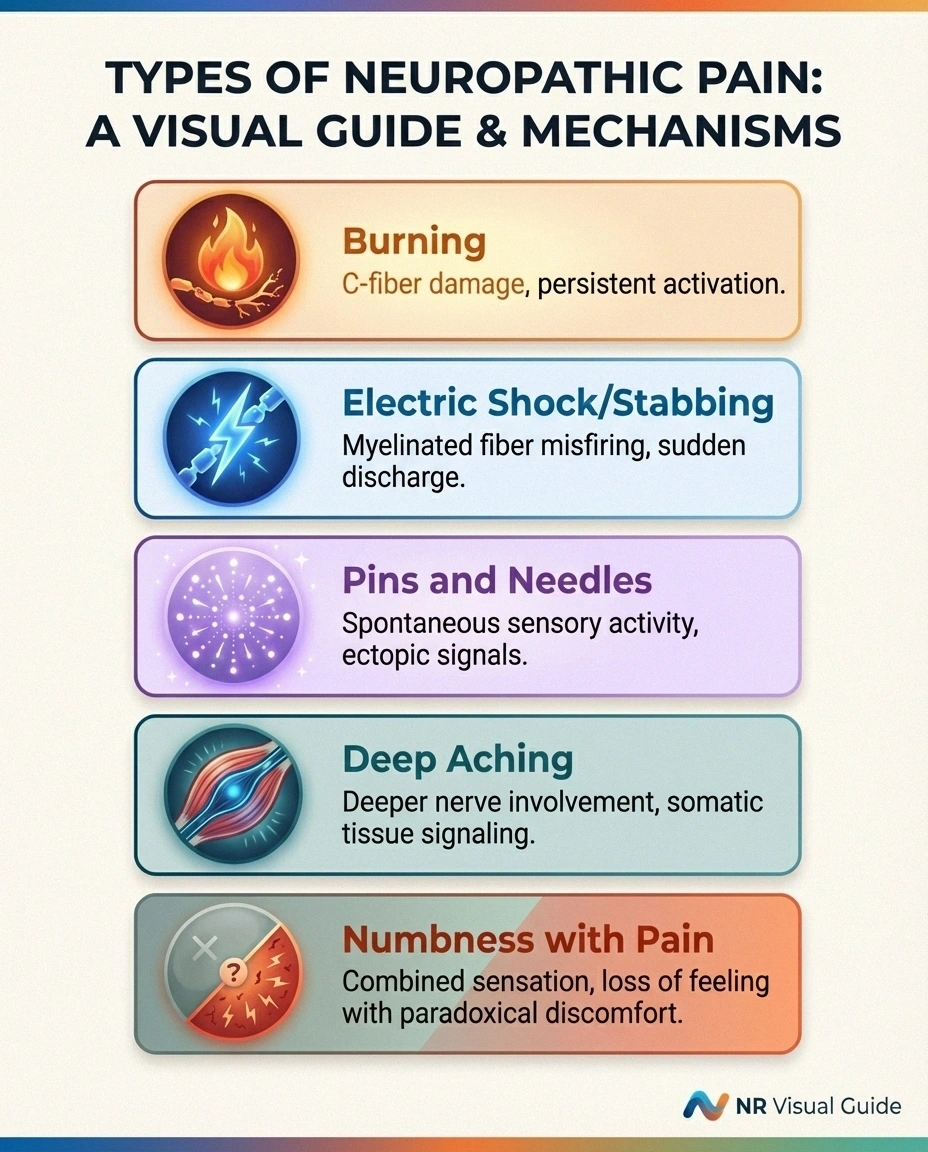
Burning pain is one of the most common descriptions of neuropathic pain. That constant, searing sensation in your feet often indicates small fiber neuropathy — damage to the thin, unmyelinated nerve fibers (called C-fibers) that normally detect temperature and pain. When these fibers are injured, they can generate continuous low-level signals that your brain interprets as burning. This type of pain tends to be constant and often worse at night.
Electric shock or stabbing pain typically comes from larger, myelinated nerve fibers that are firing spontaneously or in bursts. These fibers normally carry sharp, well-localized pain signals, and when they're damaged and misfiring, the result is those sudden, jolting sensations that feel like lightning bolts. This type tends to come and go unpredictably.
Pins and needles (paresthesia) is caused by spontaneous activity in sensory nerve fibers that normally carry touch and vibration signals. The nerves are generating random low-level signals that your brain interprets as tingling or prickling. Paresthesia is common in earlier stages of neuropathy and may precede more intense pain.
Deep, aching pain can indicate involvement of sensory nerves that innervate deeper structures — muscles, joints, and connective tissue. This type of neuropathic pain is sometimes confused with arthritis or musculoskeletal pain, which can complicate diagnosis.
Numbness with pain — this seeming contradiction is one of the most confusing aspects of neuropathy for many patients. How can your feet feel numb and painful at the same time? The answer lies in the fact that different types of nerve fibers are affected differently. Pain-carrying fibers may be damaged and misfiring (producing pain), while touch and pressure fibers are damaged and non-functional (producing numbness). You're experiencing the worst of both worlds simultaneously.
The Brain's Role: Pain Processing and Maladaptive Plasticity
Your brain isn't a passive receiver of pain signals — it actively processes, interprets, and modifies them. In chronic neuropathic pain, the brain itself undergoes structural and functional changes that sustain and intensify the pain experience.
Brain imaging studies have shown that people with chronic neuropathic pain have changes in the somatosensory cortex (the part of the brain that maps body sensations), the prefrontal cortex (involved in how you think about and evaluate pain), and the limbic system (which governs emotions). These changes, collectively called maladaptive plasticity, mean the brain has literally reorganized itself around the chronic pain experience.
This helps explain something that many neuropathic pain patients notice: the emotional weight of the pain often feels disproportionate. It's not just that your feet hurt — the pain seems to drain your energy, affect your mood, disrupt your ability to think clearly, and change how you see the world. This isn't weakness or overreaction. It's the neurological reality of how chronic pain reshapes brain function.
Research has shown significant overlap between the brain areas that process chronic pain and those involved in depression and anxiety. This is why many patients with chronic neuropathic pain also experience mood changes — and why treating the emotional dimension isn't separate from treating the pain. It's all connected in the same nervous system.
The Emotional and Psychological Dimension
I want to spend a moment on this because I think it's one of the least acknowledged aspects of neuropathic pain, and it matters enormously for your quality of life.
It's Neurology, Not Character
The emotional toll of chronic neuropathic pain isn't weakness or overreaction. Brain imaging shows that chronic pain physically changes the brain regions that regulate mood, emotion, and cognition. Treating the emotional dimension — through mindfulness, therapy, or medication — directly targets the same neurological systems driving the pain.

Living with pain that never fully stops — that doesn't have a visible wound, that other people can't see, that medications may only partially control — takes a psychological toll that goes far beyond physical discomfort. Research consistently shows that neuropathic pain is associated with higher rates of depression, anxiety, sleep disorders, social withdrawal, and reduced cognitive function.
And here's what the science tells us: these emotional effects aren't just a reaction to being in pain. The same neurological changes that cause the pain are directly affecting the brain systems that regulate mood and emotional processing. Pain catastrophizing — a pattern of exaggerated negative thinking about pain — is both a consequence of and a contributor to central sensitization. The pain makes you think catastrophically, and catastrophic thinking amplifies the pain.
This is not your fault. It's neurology, not character. But understanding this connection opens up treatment pathways that many patients overlook. Mindfulness practices, cognitive behavioral approaches, and treating coexisting depression or anxiety aren't “soft” additions to pain management — they target the same neurological systems that are driving the pain. Talk to your doctor about whether a comprehensive approach that addresses both the physical and emotional dimensions of neuropathic pain might be right for you.
Why Neuropathic Pain Gets Worse at Night
Almost every neuropathy patient I've talked to reports that pain is worse at night. There are several neurological reasons for this:
Reduced sensory input. During the day, your brain is processing a flood of sensory information — sights, sounds, touch, movement. This “sensory noise” partially masks pain signals through a mechanism called gate control. At night, when sensory input drops dramatically, the pain signals become more prominent. It's like how a ticking clock that's inaudible during the day becomes impossible to ignore in a quiet room.
Cortisol patterns. Cortisol, your body's natural anti-inflammatory hormone, follows a daily cycle — it peaks in the morning and drops to its lowest levels around midnight. As cortisol declines in the evening, the body's ability to suppress inflammation-related pain signals decreases.
Body temperature. Your core body temperature drops slightly as you prepare for sleep, and extremities — your feet and hands — cool more dramatically. Temperature changes can trigger increased firing in damaged sensory nerves, particularly the small fibers that detect temperature.
Position and blood flow. Lying down changes blood pressure distribution and can affect nerve compression. For some patients, the specific position of lying in bed places pressure on already-compromised nerves.
If nighttime pain is a major issue for you, our guide to managing neuropathy that's worse at night has specific, practical strategies that may help.
Current Approaches to Managing Neuropathic Pain
Understanding the mechanisms behind neuropathic pain helps explain why certain treatments work and others don't. Here's a brief overview of how the main approaches target the biology we've discussed:
Treatment Approaches by Target
Anticonvulsants (gabapentin, pregabalin) — reduce nerve excitability
Antidepressants (duloxetine, amitriptyline) — restore pain-control pathways
Topical treatments (capsaicin) — desensitize peripheral nerve endings
TENS units — activate gate control to mask pain signals
Mind-body approaches — target central sensitization and brain plasticity
Most doctors recommend a multimodal approach combining treatments that target different parts of the pain pathway. Talk to your doctor about which combination is right for you.
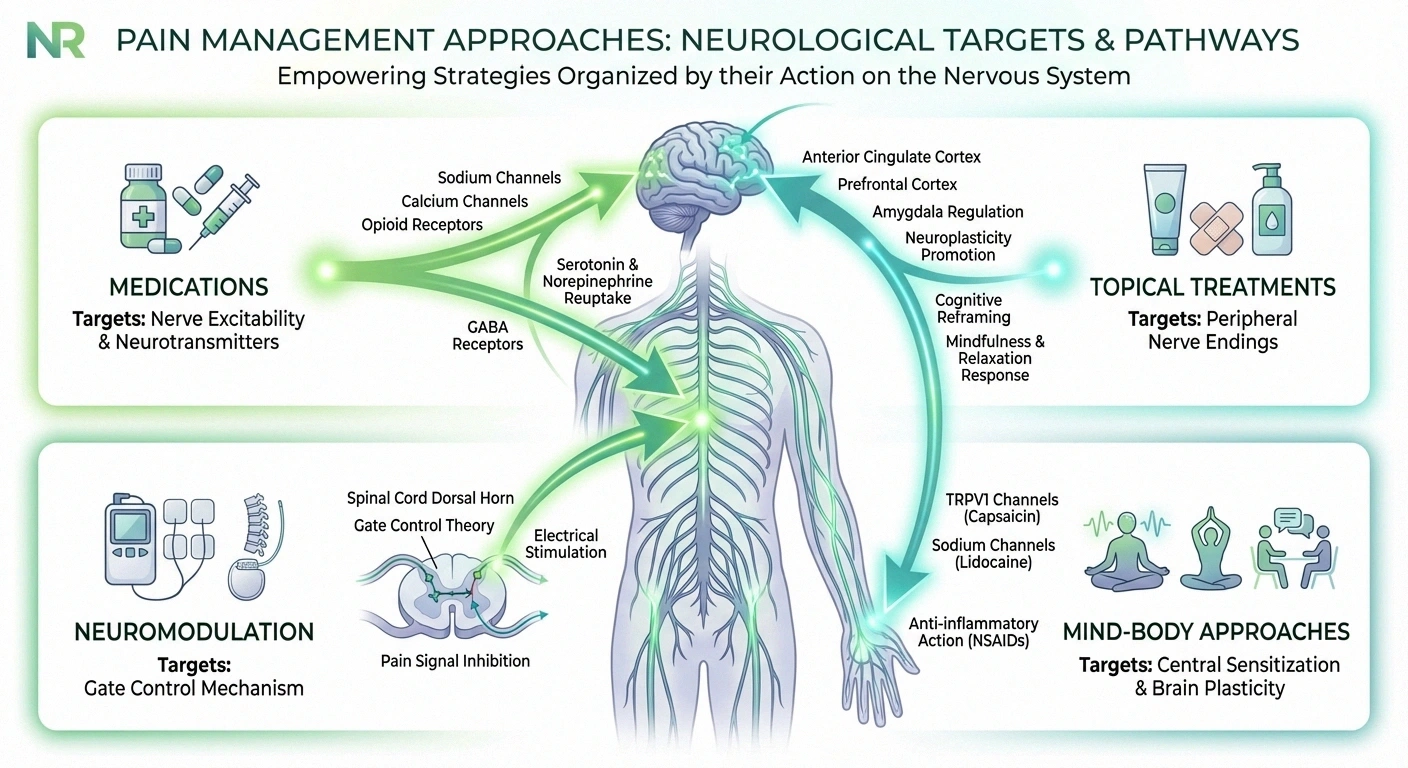
Anticonvulsants (gabapentin, pregabalin) work by reducing the excitability of neurons and blocking the excessive calcium channel activity that contributes to pain signal amplification. They target the “turned-up volume” we discussed earlier.
Antidepressants (duloxetine, amitriptyline) work by boosting the neurotransmitters serotonin and norepinephrine in the descending pain-control pathways — the brain's built-in system for dialing down pain signals. They help restore the inhibitory control that neuropathy disrupts.
Topical treatments like capsaicin cream work locally by desensitizing the nerve endings in the skin. Capsaicin depletes substance P, a chemical that pain-carrying nerves use to transmit signals.
TENS units use low-level electrical stimulation to activate the gate control mechanism — flooding the nervous system with non-painful signals that help close the “gate” on pain transmission in the spinal cord. Learn more in our guide to TENS therapy for neuropathy.
Mind-body approaches target central sensitization and the brain's maladaptive plasticity directly. Mindfulness meditation, for example, has been shown in brain imaging studies to reduce activity in the brain's pain-amplification circuits.
No single treatment addresses all the mechanisms of neuropathic pain, which is why many doctors recommend a multimodal approach — combining treatments that work on different parts of the pain pathway. Talk to your doctor about which combination might be most appropriate for your specific situation.
Frequently Asked Questions
Why does neuropathic pain feel like burning, stabbing, or electric shocks?
Different types of nerve fibers produce different pain sensations when damaged. Small unmyelinated C-fibers that normally detect temperature tend to produce burning pain when they misfire. Larger myelinated fibers that carry sharp pain signals produce stabbing or electric shock sensations when they fire spontaneously. Most neuropathy patients experience multiple types because different fibers are affected simultaneously.
How can my feet feel numb and painful at the same time?
This common paradox happens because different nerve fiber types are affected in different ways. Touch and pressure fibers may be damaged and non-functional, causing numbness, while pain-carrying fibers are damaged and misfiring, generating pain signals. You are experiencing the loss of some nerve functions and the malfunction of others simultaneously.
What is central sensitization and why does it matter?
Central sensitization is when persistent pain signals cause the spinal cord and brain to become hypersensitive, amplifying pain beyond what the original nerve damage would produce. It matters because it means neuropathic pain is not just about damaged nerves in your feet or hands. The entire pain processing system changes, which is why the pain can seem disproportionate and why it often requires treatments targeting the central nervous system, not just the peripheral nerves.
Why is neuropathic pain worse at night?
Several factors combine to make neuropathic pain more noticeable at night. Reduced sensory input removes the masking effect of daytime stimulation. Cortisol, the body's natural anti-inflammatory hormone, drops to its lowest levels. Body temperature changes in the extremities can trigger increased nerve firing. The quiet, still environment makes pain signals more prominent to the brain.
Can neuropathic pain be cured?
In some cases, treating the underlying cause of neuropathy can reduce or eliminate neuropathic pain over time, particularly when the cause is identified early and is reversible, such as a vitamin deficiency. In many cases, however, neuropathic pain is managed rather than cured, using a combination of medications, lifestyle modifications, and complementary therapies. Effective management can significantly improve quality of life even when complete resolution is not achievable.
Why don't regular painkillers like ibuprofen work well for nerve pain?
Over-the-counter painkillers like ibuprofen and acetaminophen target inflammation and tissue damage pathways, which are not the primary drivers of neuropathic pain. Neuropathic pain arises from misfiring nerves, altered sodium channels, lost inhibitory control, and central sensitization. Medications that target these specific mechanisms, such as gabapentin, pregabalin, and duloxetine, are generally more effective because they address the actual source of the pain signals.
Does neuropathic pain cause depression, or does depression make pain worse?
Research shows it works both ways. Chronic neuropathic pain directly affects the brain systems that regulate mood, increasing the risk of depression and anxiety. At the same time, depression amplifies pain perception through shared neurological pathways and can worsen central sensitization. This bidirectional relationship is why comprehensive pain management that addresses emotional well-being alongside physical symptoms often produces better outcomes than treating either one alone.



