
Can Neuropathy Cause Headaches? The Surprising Connection
When people think of neuropathy, they think of tingling feet, burning hands, numbness in the toes. Headaches aren't usually part of the conversation. But if you're living with neuropathy and also dealing with frequent headaches — especially migraines — you're not imagining a connection. Recent research suggests these two conditions share deeper links than most doctors have recognized.
I hear from readers regularly who describe this exact frustration: “My feet burn, my hands tingle, AND I get terrible headaches — but my doctors treat them as completely separate problems.” As it turns out, the research is starting to show they may not be separate at all.
What the Research Says: Neuropathy and Headache Prevalence
A landmark study from Massachusetts General Hospital and Harvard Medical School, published in Medical Research Archives in 2024, examined headache prevalence in patients being evaluated for small fiber neuropathy. The findings were striking:
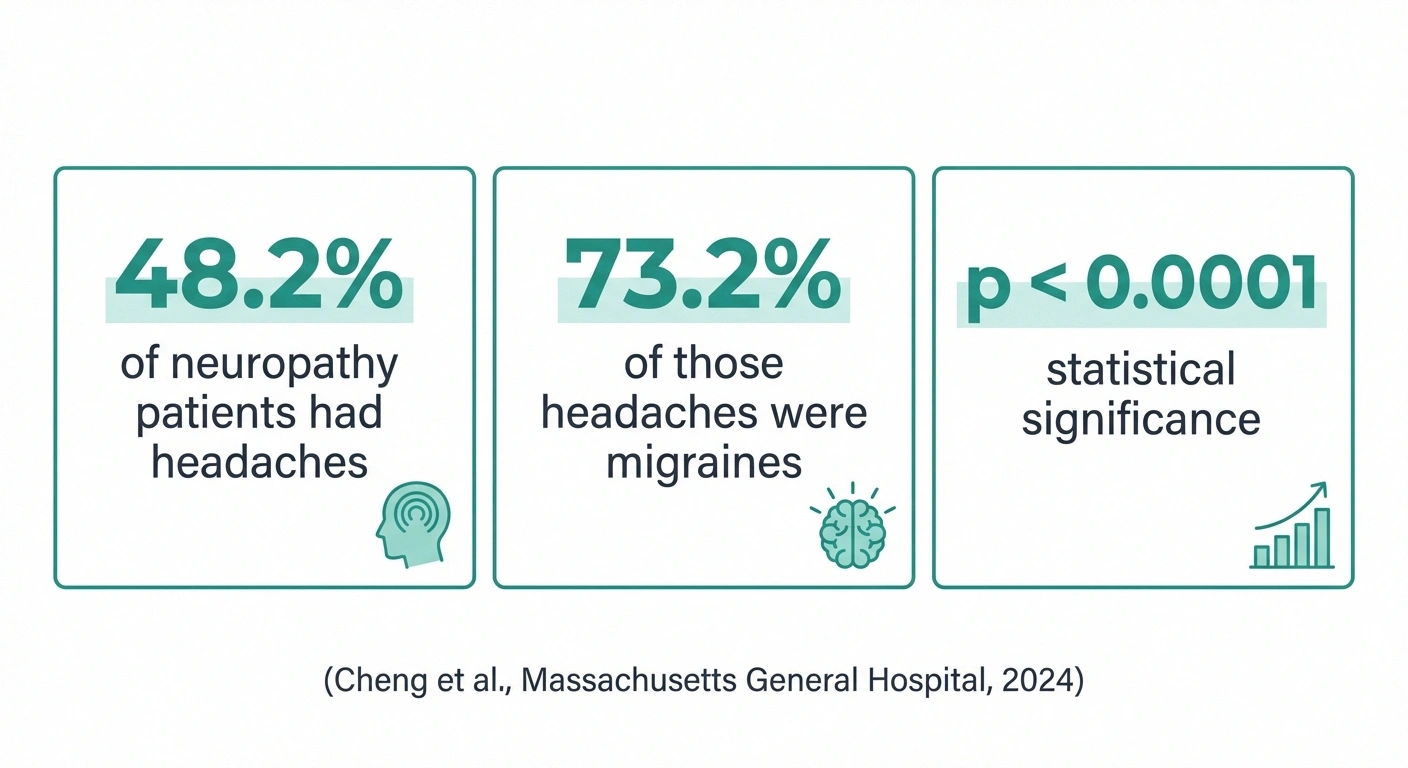
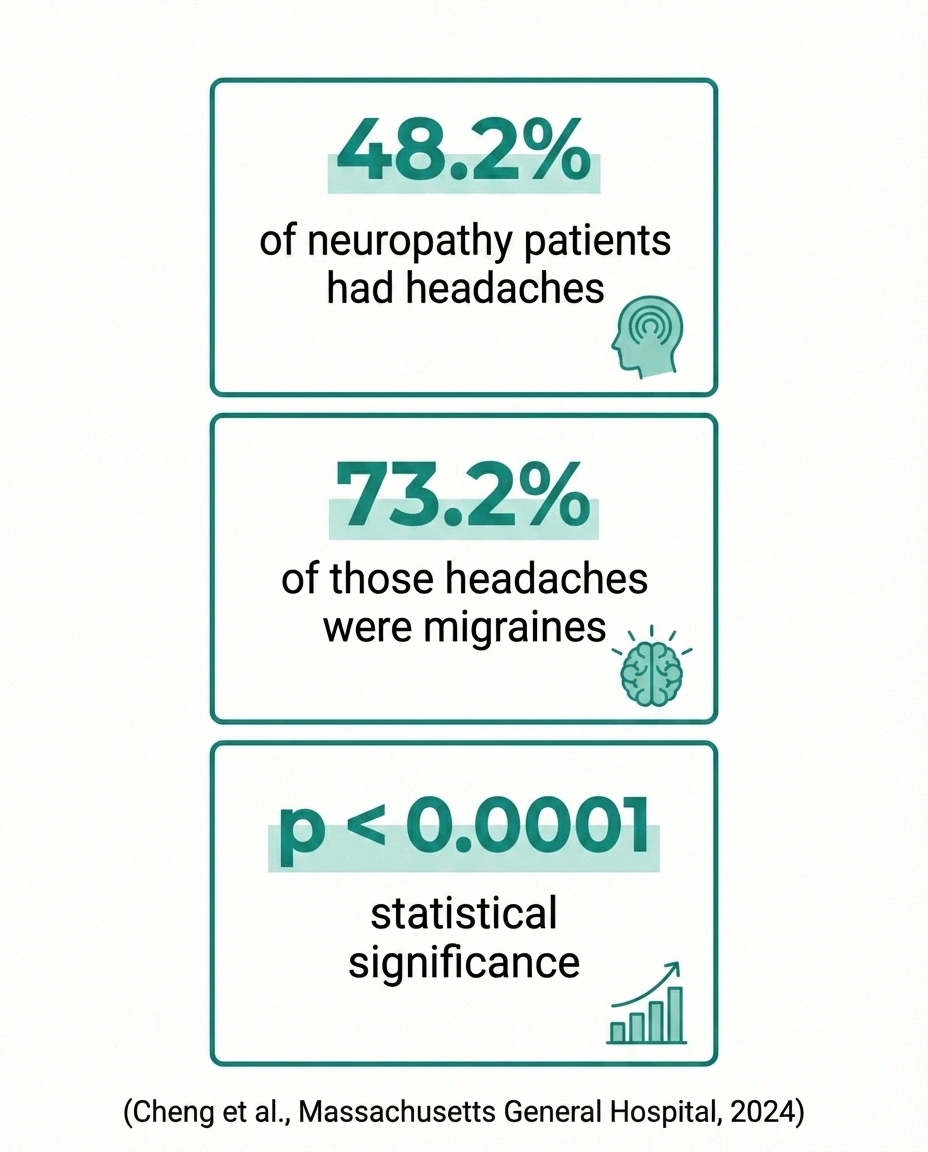
- 48.2% of patients with neuropathic symptoms also had headaches
- Of those headaches, 73.2% met the criteria for migraine
- There was a statistically significant correlation between neuropathic pain and headaches (p < 0.0001)
- Autonomic symptoms — like blood pressure changes, heart rate issues, and digestive problems — were also significantly correlated with headaches (p < 0.01)
A separate study presented at the 2025 American Academy of Neurology annual meeting confirmed these findings, reporting a significant correlation between neuropathic pain and both headaches and migraine prevalence.
Nearly half of neuropathy patients having headaches — with three-quarters of those being migraines — is far beyond what you'd expect by chance. Something is connecting these conditions at a biological level.
Why Neuropathy and Headaches May Be Linked
The connection between peripheral neuropathy and headaches involves several overlapping mechanisms. Understanding these may help explain why treating them as unrelated conditions often fails.
Central Sensitization: When Your Nervous System Amplifies Everything
When peripheral nerves are damaged, they send continuous pain signals to the spinal cord and brain. Over time, this barrage causes the central nervous system to become “wound up” — a process called central sensitization. Once sensitized, your brain amplifies all incoming signals, including those from the head and face.
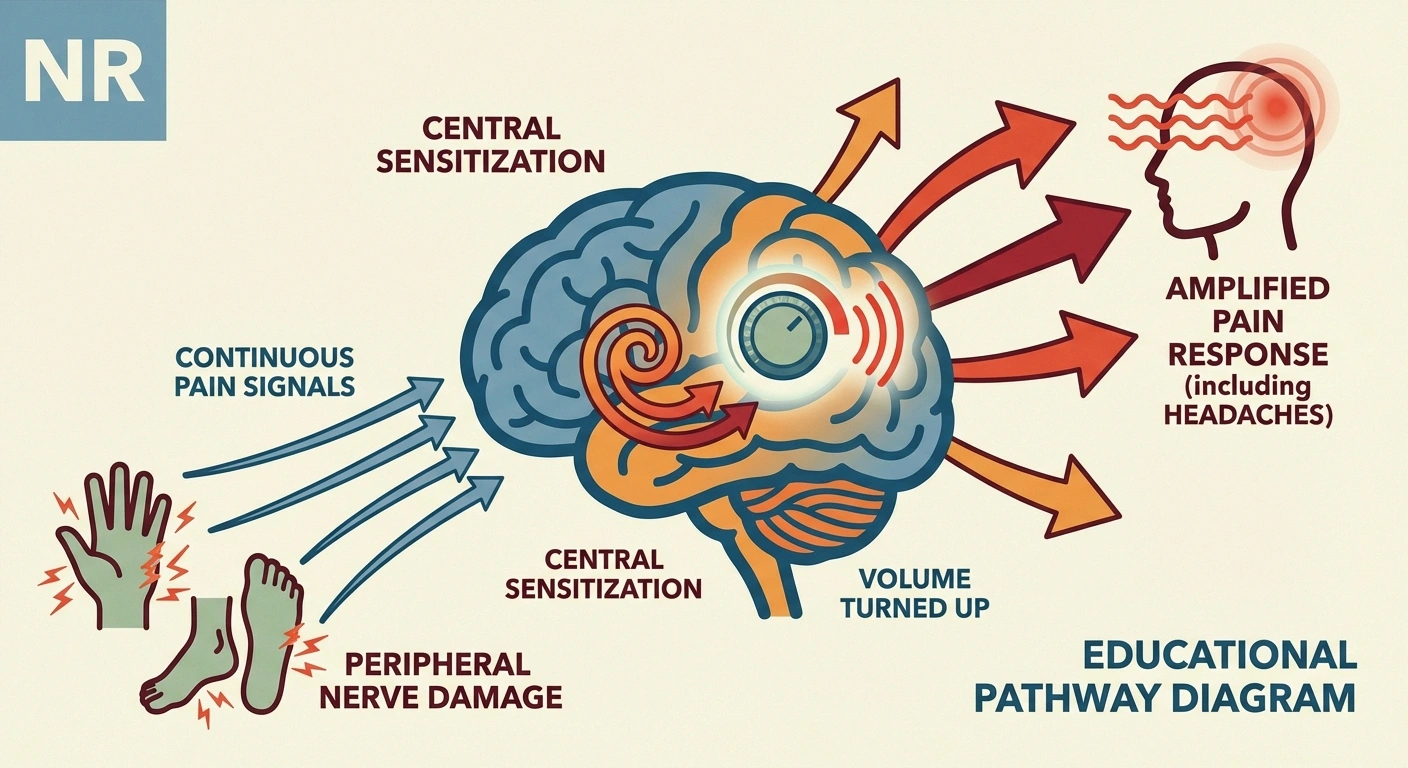
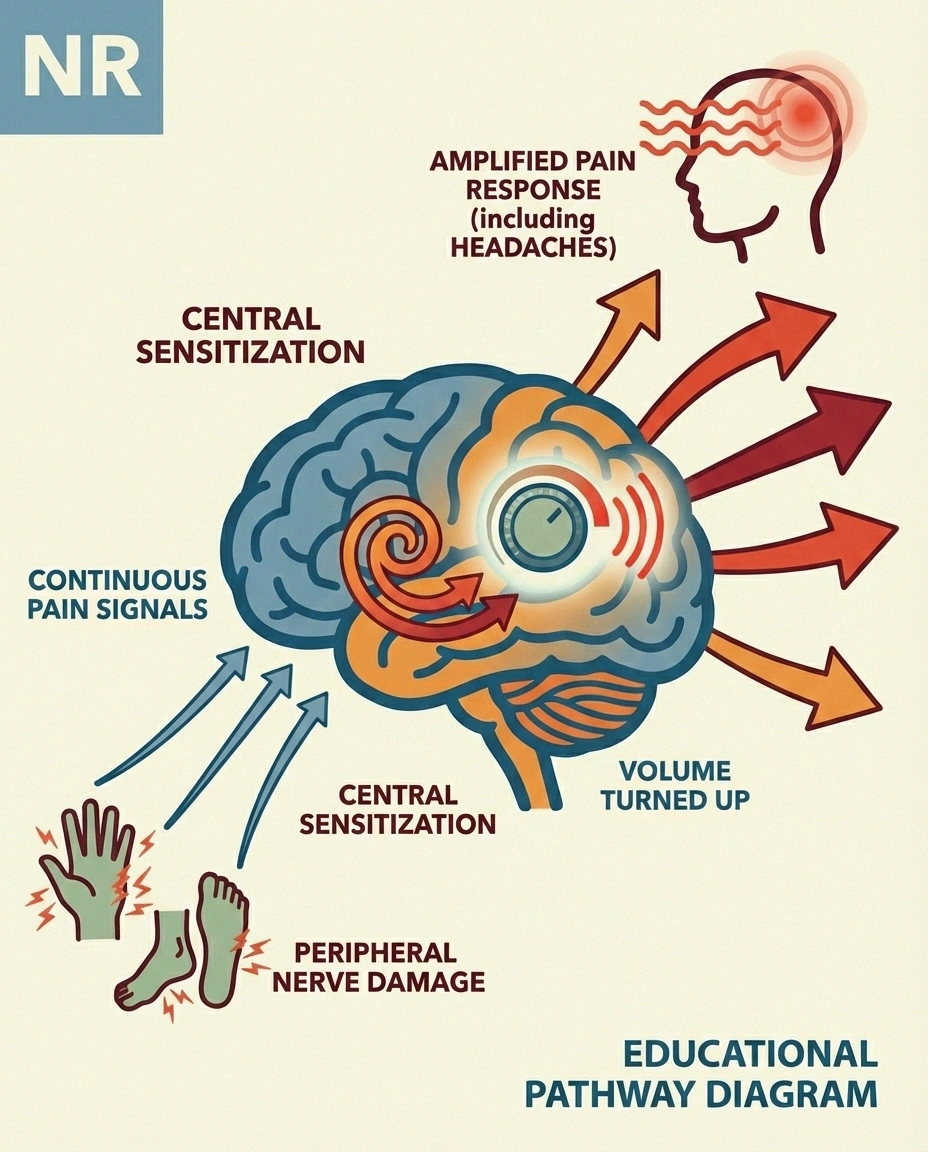
This is likely the most important link between neuropathy and headaches. The Harvard study specifically noted that positive skin biopsy results for small fiber neuropathy did not correlate with headache prevalence — suggesting the headaches aren't caused by peripheral nerve damage in the head, but by centralized mechanisms in the brain itself. The peripheral neuropathy triggers central changes, and those central changes produce headaches.
Shared Inflammatory Pathways
Both neuropathic pain and migraines involve inflammatory mediators — particularly calcitonin gene-related peptide (CGRP), substance P, and various proinflammatory cytokines. Damaged peripheral nerves release these chemicals systemically, and the same chemicals play central roles in migraine pathophysiology. The trigeminal nerve, which is the primary nerve involved in most headaches, is particularly sensitive to these inflammatory signals.
Autonomic Nervous System Dysfunction
The Harvard study found a significant link between autonomic symptoms and headaches. Autonomic neuropathy — which affects the nerves controlling blood pressure, heart rate, digestion, and blood vessel regulation — can directly contribute to headaches through impaired blood vessel control in the brain. Many migraine sufferers also have autonomic symptoms like lightheadedness, nausea, and blood pressure fluctuations during attacks, further supporting this connection.
Small Fiber Neuropathy and the Trigeminal System
Small fiber neuropathy doesn't just affect your feet and hands. The same small nerve fibers exist throughout your body, including your face and scalp. When small fiber neuropathy affects the trigeminal system — the nerve network responsible for sensation in the face and head — it can directly contribute to headache and facial pain. Some researchers have proposed that migraine itself may involve a form of neuropathic pain processing through the trigeminal pathway.
If you've been experiencing scalp tingling alongside your headaches and peripheral neuropathy, this trigeminal involvement may be particularly relevant.
Types of Headaches Associated with Neuropathy
Not all headaches connected to neuropathy are the same. Several distinct types have been documented:
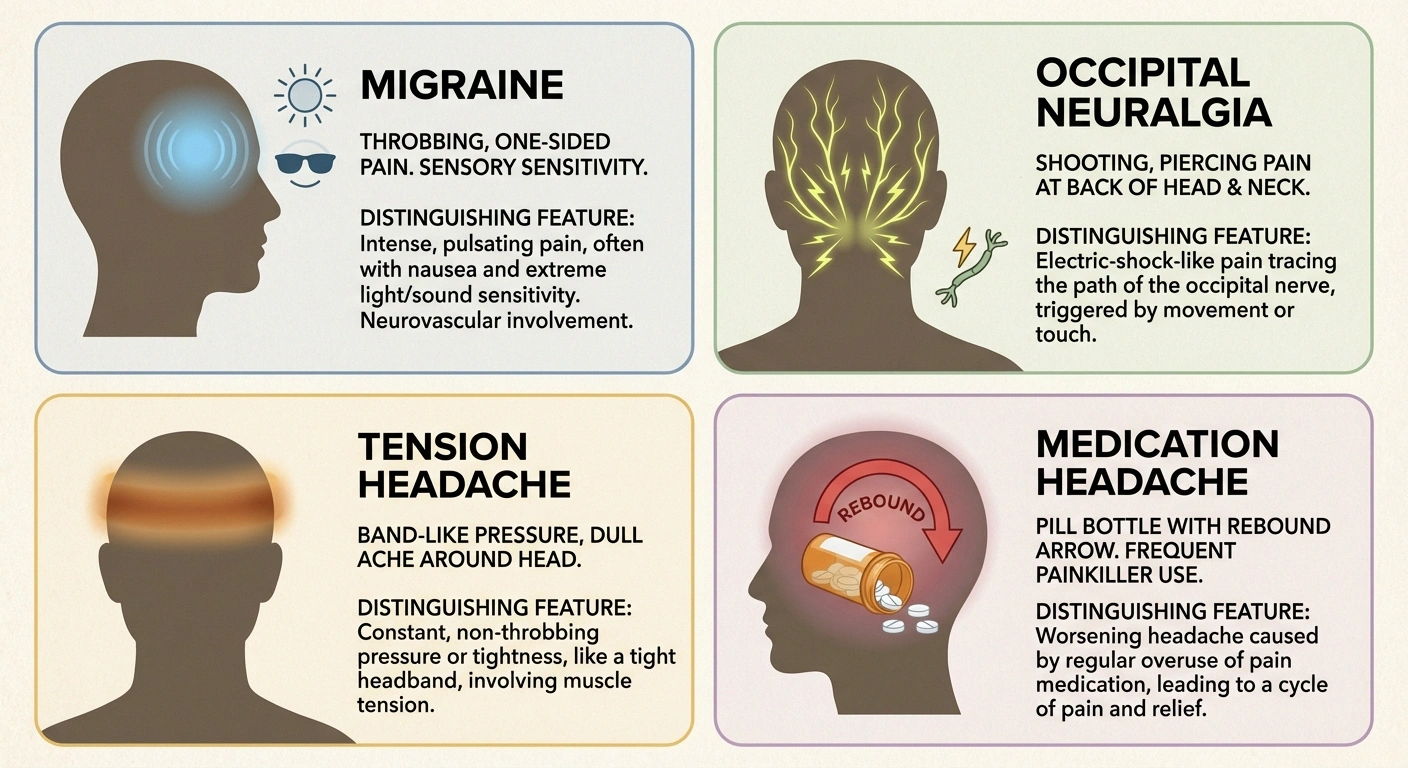

Migraines — By far the most common headache type in neuropathy patients, according to the Harvard data. These are characterized by throbbing pain (usually on one side), sensitivity to light and sound, nausea, and episodes lasting hours to days. The overlap between migraine and neuropathy is so strong that some researchers have asked whether migraine itself is a neuropathic pain syndrome.
Occipital neuralgia — Sharp, shooting pain at the back of the head caused by irritation of the occipital nerves. This is a true cranial neuropathy — the nerve itself is damaged or compressed. It's characterized by electric shock-like pain that radiates from the base of the skull to the scalp.
Tension-type headaches — Dull, band-like pressure around the head. While these are common in the general population, they may be more frequent and severe in people with neuropathy due to central sensitization amplifying the pain experience.
Medication-related headaches — Some neuropathy medications can themselves trigger headaches. Gabapentin and pregabalin occasionally list headache as a side effect, and medication overuse headache (rebound headache) can develop from frequent use of over-the-counter pain relievers used to manage neuropathy discomfort.
Cranial Neuropathies: When Nerve Damage Directly Causes Head Pain
While most neuropathy-headache connections work through indirect mechanisms like central sensitization, some headaches are caused directly by damage to cranial nerves — the nerves that originate in the brain and serve the head, face, and neck.
There are 12 pairs of cranial nerves, and neuropathy can affect any of them. The most relevant to headaches include:
- Trigeminal nerve (CN V) — The major sensory nerve of the face. Damage or irritation causes trigeminal neuralgia, one of the most severe pain conditions known.
- Occipital nerves — While technically peripheral nerves rather than cranial nerves, they emerge from the upper cervical spine and serve the back of the head. Compression or inflammation causes occipital neuralgia.
- Glossopharyngeal nerve (CN IX) — Can cause sharp pain in the throat, ear, and back of the tongue.
Cranial neuropathies are less common than peripheral neuropathy in the limbs, but they're worth considering if your headaches have a shooting, electric quality or follow a specific nerve distribution pattern.
Which Neuropathy Conditions Are Most Linked to Headaches?
Not all types of neuropathy carry equal headache risk. Based on the research, certain conditions show stronger associations:

Small fiber neuropathy — The Harvard study specifically examined SFN patients and found the highest headache prevalence. Because small fibers are involved in both pain signaling and autonomic function, SFN creates the ideal conditions for headache development through multiple pathways.
Diabetic neuropathy — Diabetes damages both peripheral nerves and blood vessels, and the metabolic disruption contributes to central sensitization. Migraine prevalence is elevated in diabetic patients with neuropathy compared to diabetic patients without it.
Autoimmune neuropathies — Conditions like Sjögren's syndrome, lupus, and vasculitis can cause both peripheral neuropathy and headaches through shared autoimmune inflammation. In these cases, the same inflammatory process attacking your peripheral nerves may also be affecting blood vessels and nerves in the head.
Neuropathy with autonomic involvement — If your neuropathy includes autonomic symptoms — blood pressure instability, rapid heartbeat, digestive issues — the headache risk increases significantly. Autonomic dysfunction directly impairs the blood vessel regulation that, when disordered, triggers many types of headaches.
Managing Headaches When You Have Neuropathy
If you're dealing with both conditions, the most effective approach treats them as connected rather than separate problems. Here are practical strategies:

Talk to your neurologist about both conditions together. Don't let your headaches get discussed at one appointment and your neuropathy at another. Ask your doctor to consider the shared mechanisms and choose treatments that address both.
Consider medications that target both. Several medications used for neuropathy also prevent migraines — including amitriptyline (a tricyclic antidepressant effective for both nerve pain and migraine prevention), duloxetine (which addresses central sensitization), and anti-CGRP medications (newer migraine drugs that target the same inflammatory pathways involved in neuropathic pain). If you're already on a medication for neuropathy, your doctor may be able to adjust it to help with headaches too.
Address autonomic dysfunction. If you have autonomic symptoms, managing them — through hydration, compression garments, dietary salt adjustments, and medications if needed — may improve headaches as well.
Reduce central sensitization. Regular moderate exercise, adequate sleep, stress management, and mindfulness practices all help calm an overactive nervous system. These approaches benefit both neuropathy pain and headache frequency.
Track your patterns. Use a symptom journal to record both neuropathy symptoms and headaches together. You may discover that flares of one predict flares of the other, or that specific triggers (stress, poor sleep, certain foods) worsen both simultaneously.
Check your medications. Review all your current medications with your doctor. Some neuropathy drugs can cause or worsen headaches, and adjusting doses or timing may help. Conversely, if you're using over-the-counter headache medication more than 2 to 3 days per week, you may be developing medication overuse headaches.
When to See a Doctor About Headaches and Neuropathy
While most headaches in neuropathy patients are migraines or tension-type headaches, some red flags require urgent medical attention:

- Sudden, severe headache unlike any you've had before (“thunderclap headache”)
- Headache with vision changes, confusion, difficulty speaking, or facial drooping
- New headaches that started after beginning a new medication
- Headache with fever and stiff neck
- Progressive worsening over days or weeks
- Headache after a head injury
For the more common migraine-neuropathy overlap, schedule a neurology appointment to discuss the connection. If you're seeing separate specialists for headaches and neuropathy, ask if a single neurologist can coordinate both.
Frequently Asked Questions
Can peripheral neuropathy directly cause migraines?
Peripheral neuropathy doesn't directly cause migraines, but it creates conditions that make migraines more likely. Central sensitization from ongoing nerve damage lowers the threshold for migraine attacks, and shared inflammatory pathways mean the same biological processes driving neuropathy may also trigger migraines.
Are headaches a symptom of small fiber neuropathy?
Headaches are not a classic diagnostic criterion for small fiber neuropathy, but research shows they are very common in SFN patients — nearly half experience them. If you have SFN and headaches, they are likely related rather than coincidental.
Can treating my neuropathy improve my headaches?
Potentially, yes. If your headaches are driven by central sensitization from peripheral neuropathy, improving your neuropathy management may reduce headache frequency. Medications that address central sensitization — like duloxetine and amitriptyline — can benefit both conditions. Reducing overall pain load helps calm the nervous system.
Do neuropathy medications cause headaches?
Some neuropathy medications list headache as a possible side effect, though it's usually mild and temporary. Gabapentin and pregabalin occasionally cause headaches, especially during dose adjustments. If headaches start or worsen after beginning a new medication, discuss this with your doctor.
Should I see a neurologist or a headache specialist?
Ideally, see a neurologist who can evaluate both conditions together. Many neurologists treat both neuropathy and headache disorders. If your headaches are severe or complex, a headache subspecialist who understands the neuropathy connection may be beneficial. The key is having one doctor consider both conditions as potentially related.
The Takeaway
If you have neuropathy and headaches, you're not imagining a connection. Research from Harvard, the American Academy of Neurology, and other institutions confirms that neuropathic pain significantly increases headache risk — particularly migraines. The link runs through central sensitization, shared inflammatory pathways, and autonomic dysfunction.
The most important step you can take is to stop treating these as unrelated problems. Bring both conditions into the same conversation with your neurologist. Explore treatments that address both. And recognize that managing your neuropathy may be one of the best things you can do for your headaches — and vice versa.
For more on understanding how neuropathy affects your whole body — not just your hands and feet — browse our guides on autonomic neuropathy, neuropathic pain explained, and the stages of neuropathy.


