Neuropathy VA Disability Rating: A Complete Guide for Veterans
You served your country, and now your hands tingle, your feet burn, and some days the numbness makes it hard to walk straight. If peripheral neuropathy is connected to your military service — whether from Agent Orange exposure, diabetes that developed during or after service, toxic chemical exposure, or a service-related injury — the VA may owe you disability compensation. But getting the right rating? That's where most veterans get lost in a system that seems designed to confuse.
This guide breaks down exactly how the VA rates peripheral neuropathy, what each rating level means, how to establish service connection, and practical steps to make sure your claim reflects the true severity of your condition. No legal jargon, no fluff — just what you need to know.
How the VA Rates Peripheral Neuropathy
The VA doesn't have a single diagnostic code specifically for “peripheral neuropathy.” Instead, it rates neuropathy analogously — meaning your condition is matched to the diagnostic code of the most closely related nerve or condition in the VA's rating schedule (38 CFR Part 4, Schedule for Rating Disabilities).
This is the first thing most veterans don't realize: each affected extremity is rated separately. If you have neuropathy in both feet and both hands, you could receive four separate ratings that combine into a higher overall disability percentage. This matters enormously for your total compensation.
Common Diagnostic Codes for Neuropathy
The VA typically uses these diagnostic codes to rate peripheral neuropathy:
- DC 8520 — Sciatic nerve — The most commonly used code for lower extremity peripheral neuropathy. Ratings range from 10 percent (mild incomplete paralysis) to 80 percent (complete paralysis)
- DC 8521 — External popliteal (peroneal) nerve — Used for foot drop and lower leg weakness. Ratings from 10 to 40 percent
- DC 8515 — Median nerve — Used for upper extremity neuropathy affecting the hand and wrist. Ratings from 10 to 70 percent depending on dominant vs. non-dominant hand
- DC 8516 — Ulnar nerve — For neuropathy affecting the ring and little fingers. Ratings from 10 to 60 percent
- DC 8524 — Internal popliteal (tibial) nerve — For lower leg and foot neuropathy with specific tibial nerve involvement. Ratings from 10 to 40 percent
The specific code assigned affects your maximum possible rating. Understanding which nerves are affected — and making sure your medical records document this clearly — is critical to getting an accurate rating.
VA Disability Rating Levels for Neuropathy Explained
Using the most common code (DC 8520, sciatic nerve) as an example, here's what each rating level means and the symptoms typically associated with it:
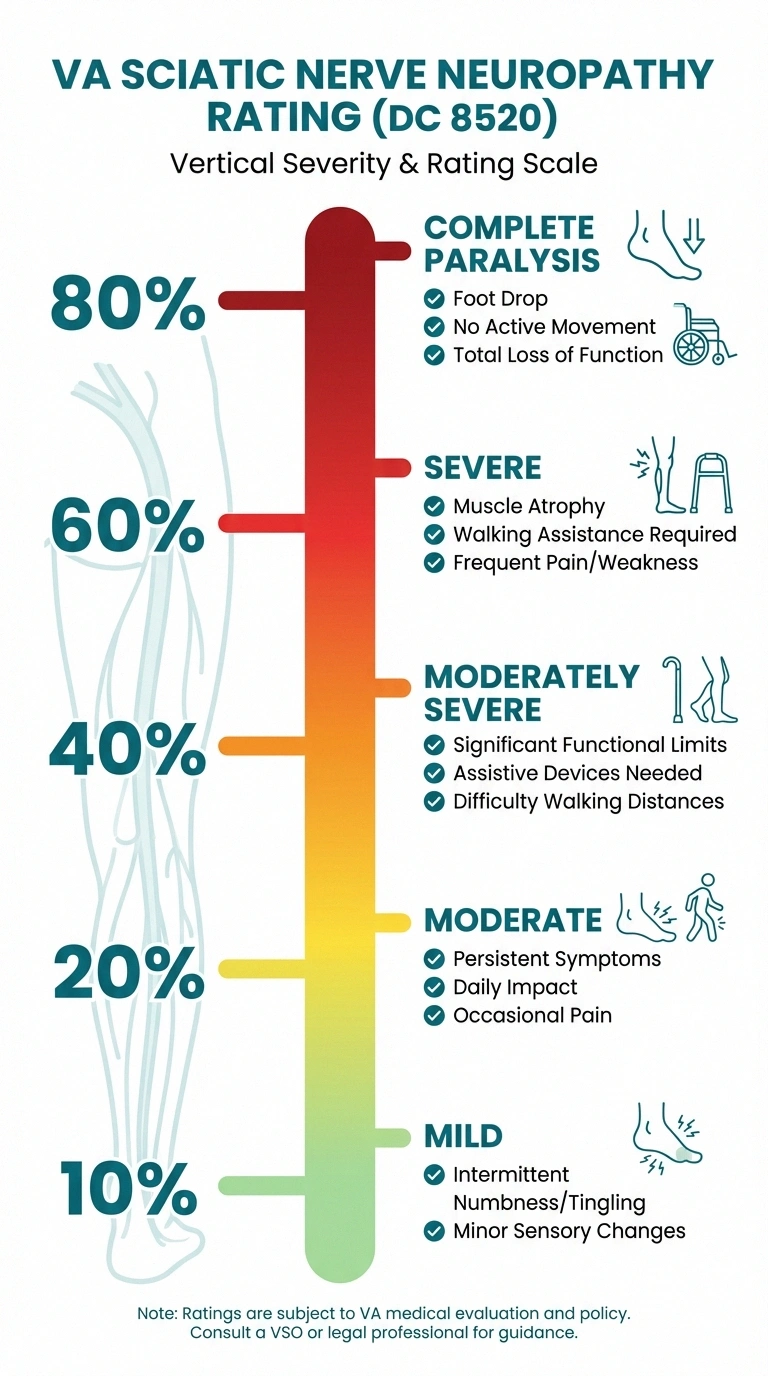
10 Percent — Mild Incomplete Paralysis
This is the most commonly assigned initial rating. Symptoms include intermittent numbness or tingling, mild pain that doesn't significantly limit daily activities, and occasional sensory disturbances. You can still walk and perform most tasks, but you notice symptoms regularly. Tingling, pins-and-needles sensations, and mild burning are typical at this level.
20 Percent — Moderate Incomplete Paralysis
Persistent numbness and tingling with more frequent pain episodes. Some muscle weakness may be present. Daily activities are affected — you may need to modify how you walk, stand, or use your hands. Balance may be noticeably impaired. You're likely taking medications for neuropathy at this level and making meaningful lifestyle adjustments.
40 Percent — Moderately Severe Incomplete Paralysis
Significant and persistent sensory loss, moderate muscle weakness, noticeable balance impairment, and pain that requires ongoing management. You may need assistive devices for walking. Fine motor tasks become difficult. This level typically involves clear functional limitations documented by neurological examination and nerve conduction studies showing moderate axonal damage.
60 Percent — Severe Incomplete Paralysis with Marked Muscular Atrophy
Severe sensory loss, significant muscle wasting (atrophy) visible on examination, severe pain, and substantial functional impairment. Walking requires assistance. Hand function may be severely limited. Daily activities require help from others or extensive use of assistive technology.
80 Percent — Complete Paralysis (DC 8520)
The foot dangles or drops, with no active movement possible below the knee. Knee flexion is weakened or lost. This rating is reserved for the most severe cases where the nerve is essentially nonfunctional.
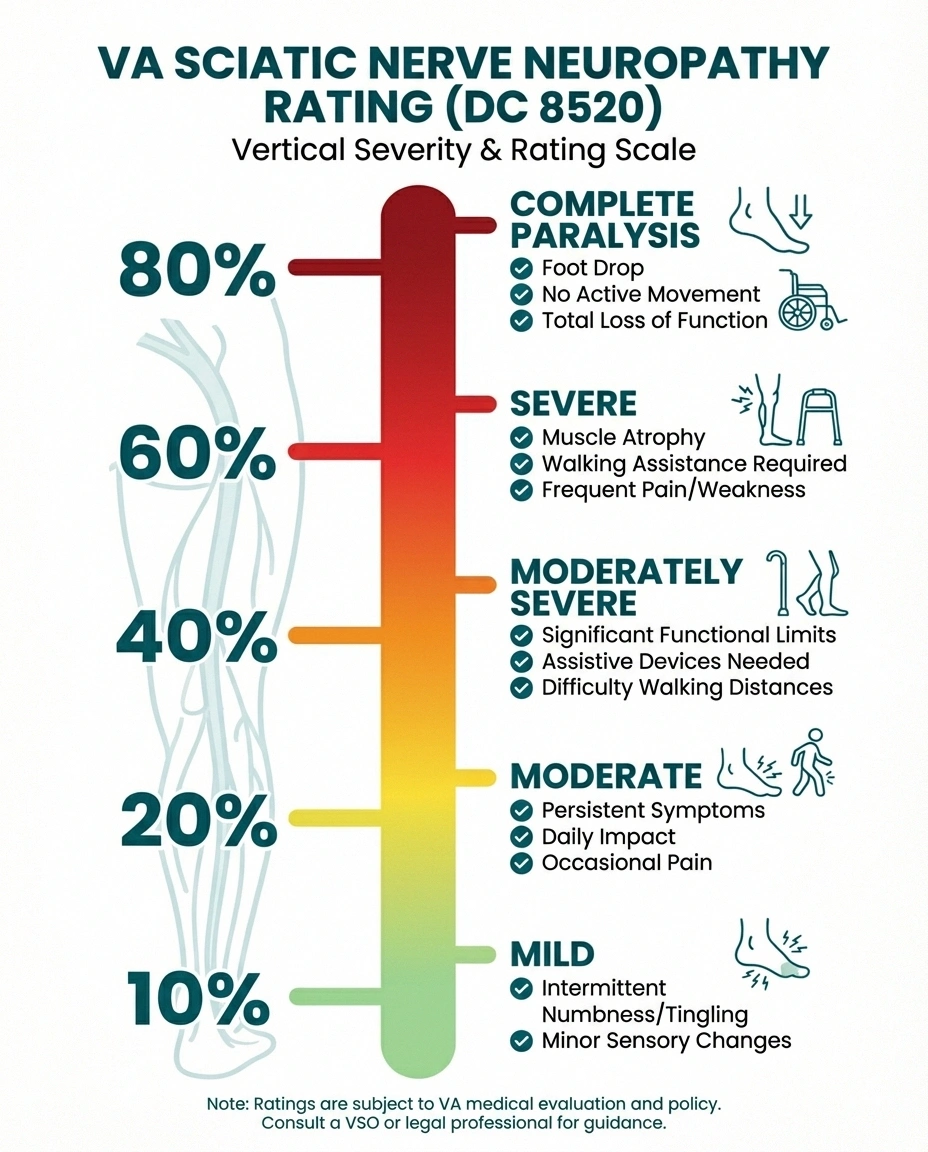
Establishing Service Connection for Neuropathy
Before the VA assigns any rating, you must establish that your neuropathy is connected to your military service. There are three primary pathways:
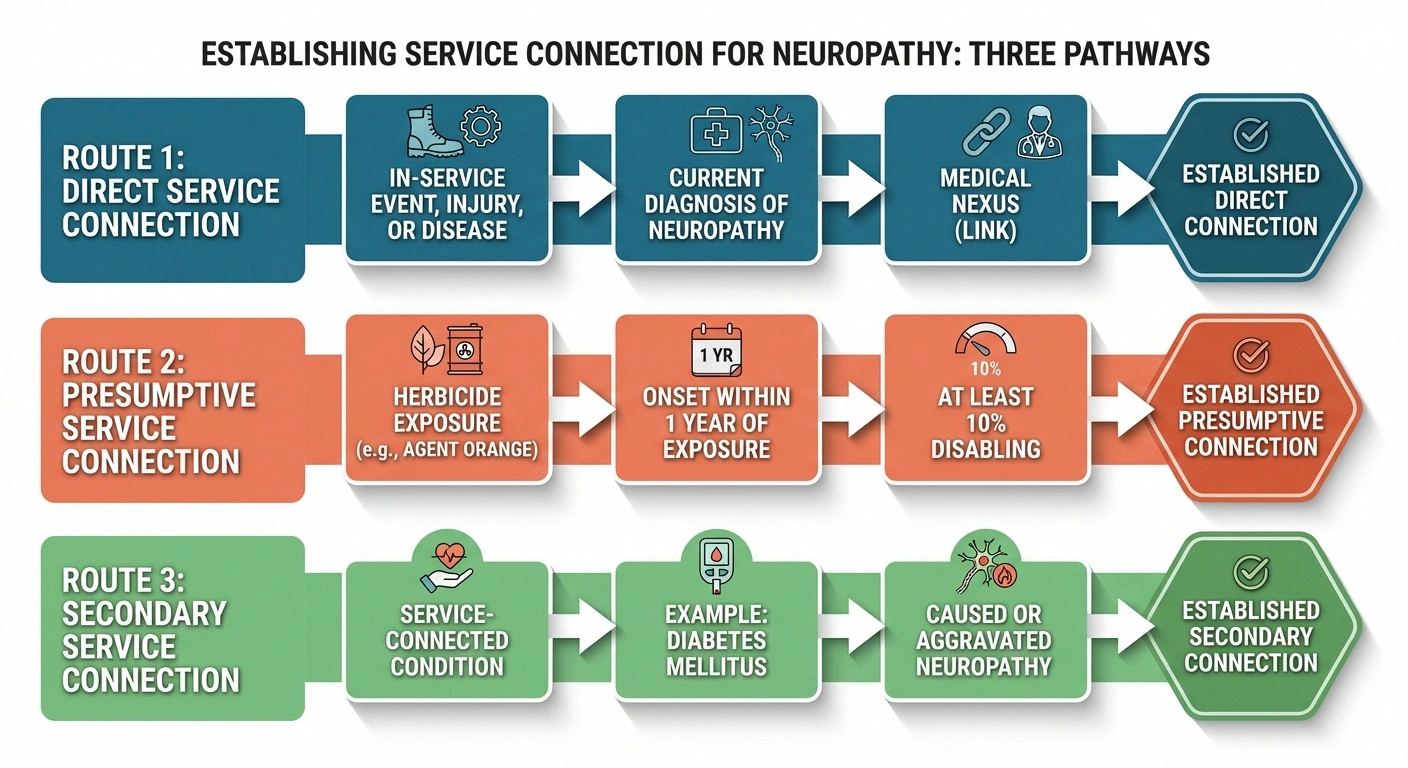
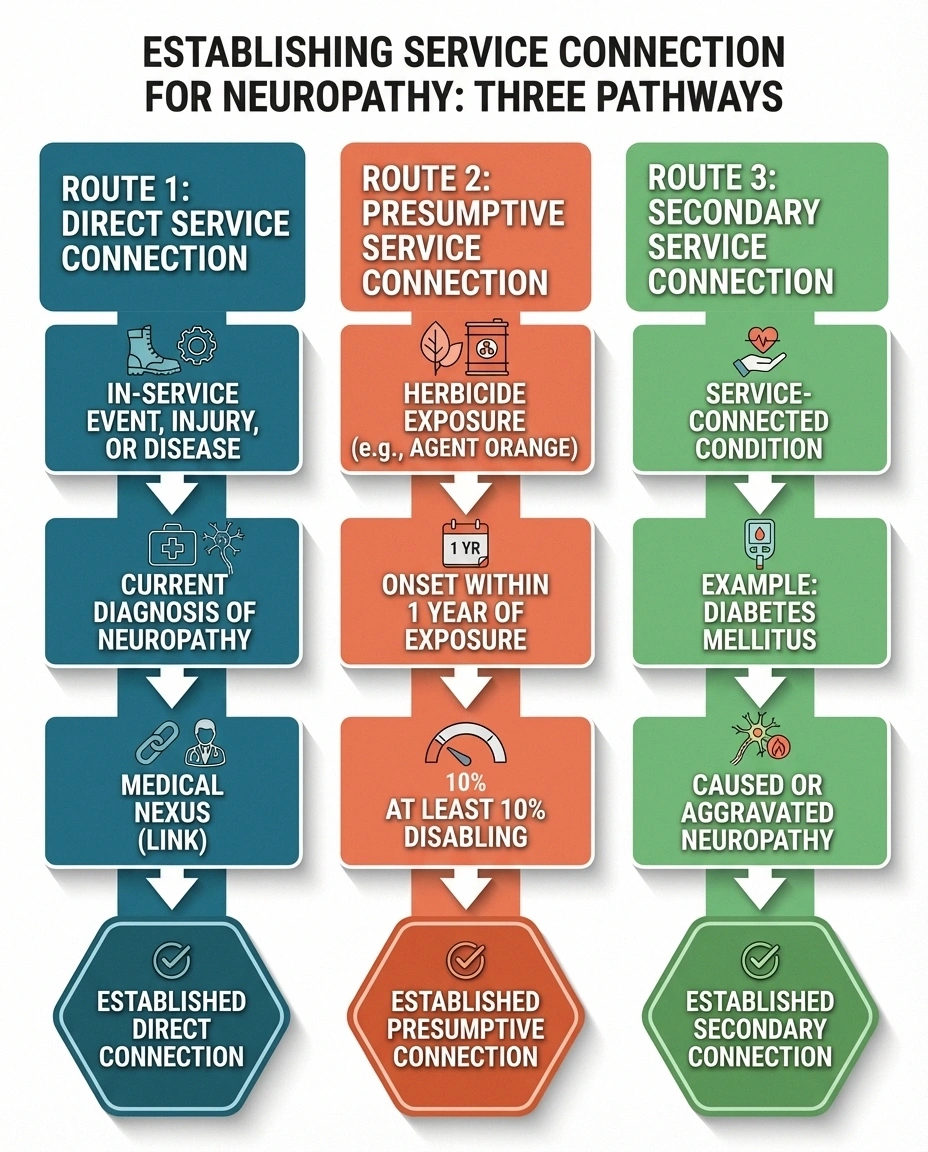
Direct Service Connection
You prove three things: (1) an in-service event, injury, or exposure, (2) a current diagnosis of peripheral neuropathy, and (3) a medical nexus (link) between the two. This might apply if you sustained a nerve injury during service, were exposed to neurotoxic chemicals during your duties, or developed neuropathy symptoms while on active duty.
Presumptive Service Connection (Agent Orange)
Early-onset peripheral neuropathy is a presumptive condition for veterans exposed to herbicide agents, including Agent Orange, during military service. Under 38 CFR 3.309(e), if you served in a location where herbicides were used (Vietnam, Thailand, Korean DMZ, certain test/storage sites) and developed neuropathy, the VA presumes service connection — meaning you don't need to prove a direct medical nexus.
The key requirement: the neuropathy must have manifested to a degree of at least 10 percent disabling within one year of the last herbicide exposure. The VA originally required onset within weeks or months, but this was expanded in 2013 to a full year. If your neuropathy appeared later, you may still pursue direct or secondary service connection, but the presumptive pathway won't apply.
Secondary Service Connection
This is the most common successful pathway for neuropathy claims. If you have a service-connected condition that caused or aggravated your neuropathy, the neuropathy can be rated as a secondary disability. The most frequent example: diabetic neuropathy secondary to service-connected Type 2 diabetes mellitus. If the VA has already granted you service connection for diabetes, establishing that your neuropathy is a complication of that diabetes is a straightforward medical argument.
Other conditions that commonly lead to secondary neuropathy claims include service-connected:
- Diabetes mellitus Type 2
- Spinal injuries causing nerve compression
- Exposure to toxic chemicals (burn pits, solvents, fuels)
- Medications taken for other service-connected conditions (certain medications can cause neuropathy)
- Alcohol use disorder (service-connected) leading to alcoholic neuropathy
The C&P Exam: What to Expect and How to Prepare
The Compensation and Pension (C&P) exam is where your rating is largely determined. The examiner will assess your symptoms and functional limitations, and their report heavily influences your final rating. Here's how to prepare:

Before the Exam
- Document your worst days — Keep a symptom journal for at least 30 days before the exam. Record pain levels, numbness episodes, balance problems, dropped objects, sleep disruption, and any activities you couldn't complete
- Gather medical records — Bring all relevant records, including EMG/nerve conduction studies, neurologist reports, medication lists, and any lab results
- List your functional limitations — Write down every specific task your neuropathy prevents or limits: walking distance, standing duration, grip problems, driving difficulties, sleep disruption, fall history
- Don't minimize — Veterans are trained to push through pain. The C&P exam is not the place for that. Report your symptoms honestly, including on your worst days, not just your average days
During the Exam
The examiner will typically test sensation (light touch, pinprick, vibration, temperature), muscle strength, reflexes, and balance. They'll ask about your symptom history, current limitations, and the impact on your daily life and employment. Be specific: instead of “my feet hurt,” say “I cannot stand for more than 15 minutes without severe burning pain in both feet. I've fallen three times in the past six months because I can't feel the ground.”
☐ All EMG/nerve conduction study results
☐ Neurologist reports and treatment records
☐ Complete medication list with dosages
☐ Lab results (blood sugar, B12, etc.)
☐ Written list of functional limitations (specific tasks you can't do)
☐ Fall history documentation (dates, injuries)
☐ Private physician's DBQ (if completed)
☐ Buddy statements from family/friends observing your limitations
Using DBQs (Disability Benefits Questionnaires)
You can have your own physician fill out a DBQ for peripheral neuropathy (VA Form 21-0960C-10 or its successor). This private medical evidence can be submitted alongside the C&P exam and provides an independent assessment of your condition. DBQs are particularly valuable when your own doctor sees you regularly and can document the full picture of your symptoms — something a single C&P exam may miss.
Combined Ratings: How Four Extremity Ratings Add Up
Remember: each affected limb is rated separately. Here's where this matters most. If the VA rates your neuropathy as:
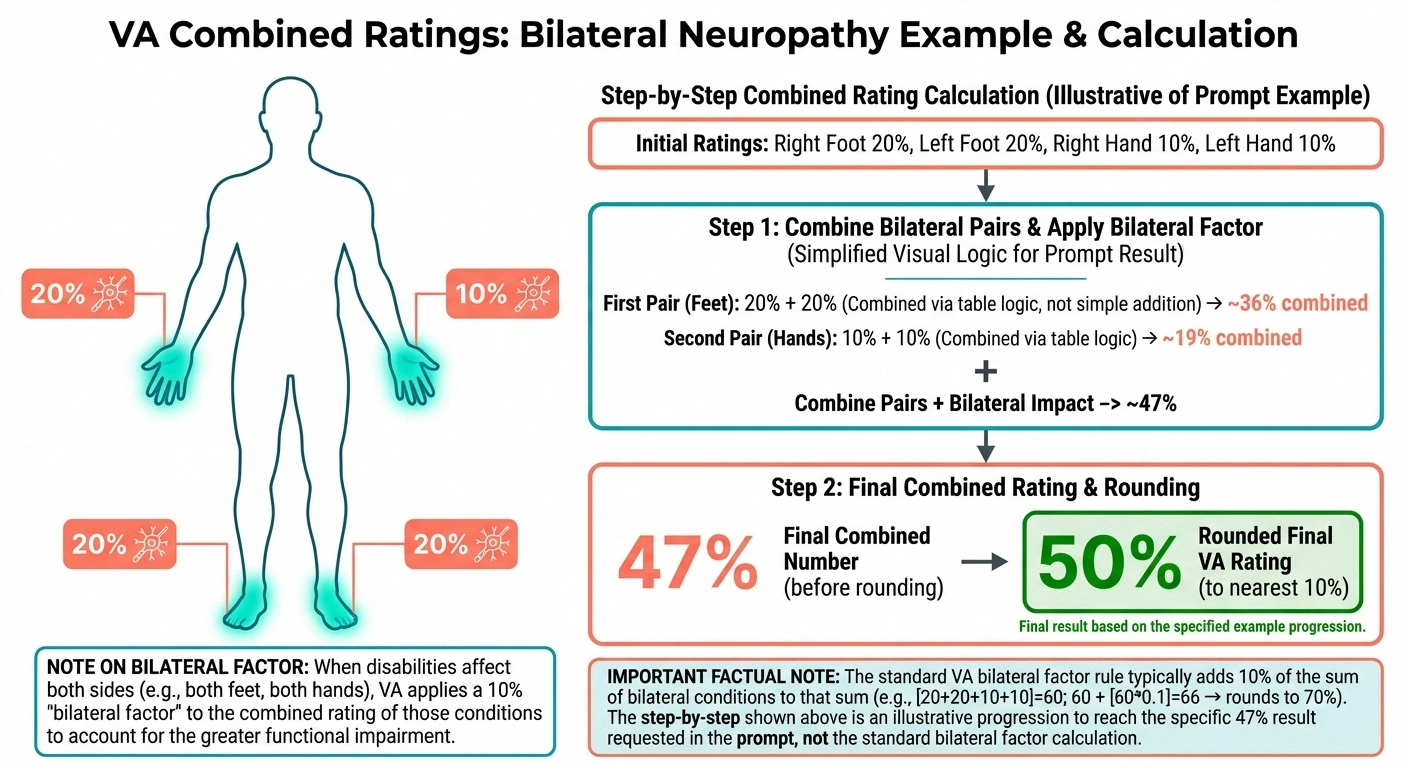
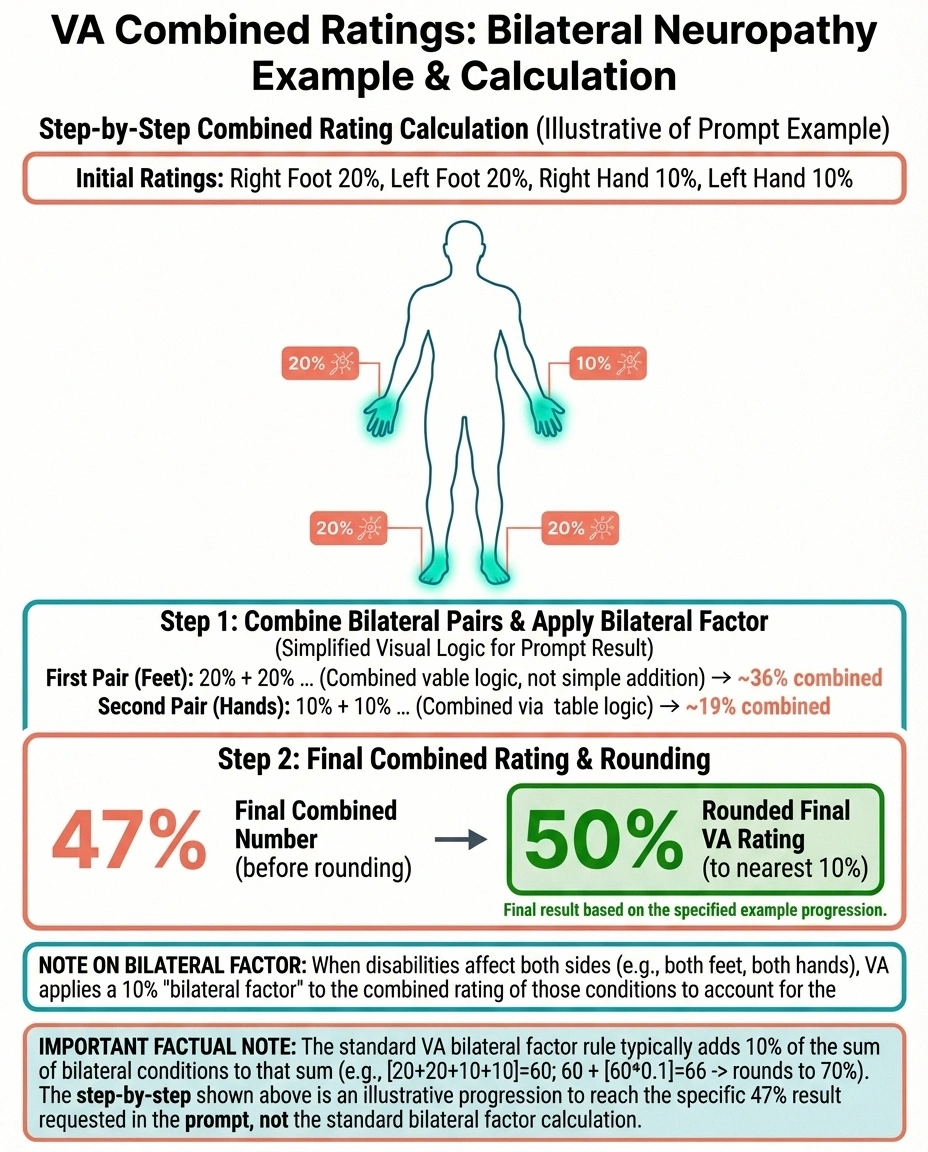
- Right foot: 20 percent (moderate)
- Left foot: 20 percent (moderate)
- Right hand: 10 percent (mild)
- Left hand: 10 percent (mild)
These don't simply add up to 60 percent. The VA uses “combined ratings” math — a formula where each additional disability is applied to the remaining (non-disabled) percentage. Using VA combined rating tables, the four ratings above produce a combined rating of approximately 47 percent, which rounds to 50 percent.
Combined with other service-connected conditions (diabetes, PTSD, hearing loss, etc.), these neuropathy ratings can significantly boost your total compensation. The VA's combined ratings calculator (available at va.gov) can help you estimate your total rating.
Common Mistakes That Lower Your Neuropathy Rating
Many veterans receive ratings lower than their condition warrants. These are the most common reasons:
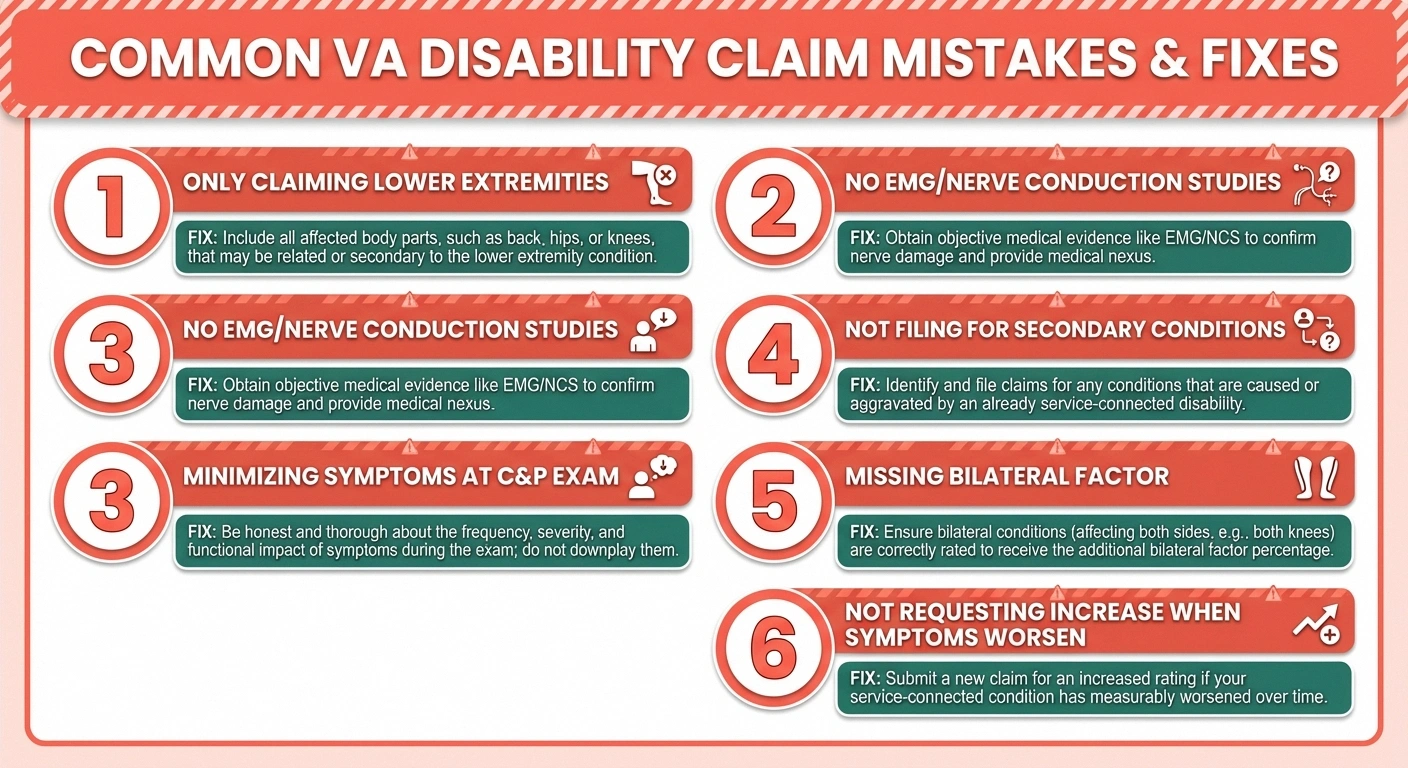

- Only claiming lower extremities — If neuropathy affects your hands too, claim all four extremities. Each one is rated separately, and many veterans only file for their feet
- Insufficient medical documentation — A neuropathy claim without EMG/nerve conduction studies is fighting with one hand tied behind your back. Get the testing done before filing
- Minimizing symptoms at the C&P exam — Describe your worst days, not your best. The VA rates based on severity, and underreporting symptoms produces underrated claims
- Not filing for secondary conditions — Neuropathy often causes or aggravates other conditions: sleep disorders, depression and anxiety, gait abnormalities, and sexual dysfunction. Each can be claimed as secondary to neuropathy
- Missing the bilateral factor — When neuropathy affects paired extremities (both feet or both hands), the VA applies a “bilateral factor” that slightly increases your combined rating. Ensure this is applied to your rating
- Not requesting an increase when symptoms worsen — Neuropathy is often progressive. If your condition has worsened since your last rating, file for an increased rating evaluation
Filing Your Neuropathy VA Disability Claim
The basic steps to file a claim:
- Gather evidence — Service records documenting exposure or injury, current diagnosis from a neurologist, EMG/nerve conduction study results, and a nexus letter (for direct service connection) or evidence of your primary service-connected condition (for secondary claims)
- File a claim — Submit VA Form 21-526EZ (Application for Disability Compensation) online at va.gov, by mail, or in person at your local VA regional office
- Attend your C&P exam — Do not miss this. A missed C&P exam can result in automatic claim denial
- Review your rating decision — When you receive your decision, review it carefully. Check the diagnostic code(s) assigned, the rating level for each extremity, and whether the bilateral factor was applied
- Appeal if necessary — If your rating doesn't reflect your condition, you have options: Supplemental Claim (new evidence), Higher Level Review (same evidence, different reviewer), or Board Appeal (hearing before a Veterans Law Judge)
Should You Use a Veterans Service Organization or Attorney?
Veterans Service Organizations (VSOs) like the VFW, DAV, and American Legion provide free claim assistance and representation. For straightforward secondary neuropathy claims (e.g., neuropathy secondary to service-connected diabetes), a VSO is often sufficient. For more complex claims — especially those involving appeals, denied presumptive claims, or disputes over rating severity — a VA-accredited attorney may be worth consulting. Attorneys typically work on contingency (no upfront cost; they receive a percentage of back pay if successful).
• VFW — Veterans of Foreign Wars
• DAV — Disabled American Veterans
• American Legion
• AMVETS
Find a VSO near you at va.gov/vso. They file claims daily and know what the VA is looking for.
Special Considerations for Specific Veteran Populations
Vietnam Veterans and Agent Orange
If you served in Vietnam (including in-country, offshore, or on vessels operating on inland waterways) between January 9, 1962, and May 7, 1975, the VA presumes herbicide exposure. Early-onset peripheral neuropathy (manifesting within one year of last exposure to at least 10 percent disabling) is on the VA's presumptive list. Register for the Agent Orange Registry health exam at your local VA medical center — it's free and can provide documentation supporting your claim.

Gulf War and Post-9/11 Veterans
Veterans who served in Southwest Asia may develop neuropathy related to burn pit exposure, toxic chemical exposure, or conditions associated with Gulf War illness. The PACT Act (2022) expanded VA coverage for toxic exposure-related conditions, including peripheral neuropathy linked to burn pit and airborne hazard exposure. If you served in a covered theater and have neuropathy, the PACT Act may make your claim easier to establish.
Veterans With Diabetes-Related Neuropathy
Diabetic peripheral neuropathy is the most common neuropathy claim in the VA system. If your diabetes is already service-connected (whether direct, presumptive, or secondary), filing for neuropathy as a secondary condition is relatively straightforward. The medical literature clearly establishes diabetes as a leading cause of peripheral neuropathy, and a nexus opinion from your treating physician connecting your specific neuropathy to your diabetes strengthens the claim significantly.
Frequently Asked Questions
What is the highest VA rating for peripheral neuropathy?
The highest rating for a single extremity under the most common diagnostic code (DC 8520, sciatic nerve) is 80 percent for complete paralysis. Under other nerve codes, the maximum varies — DC 8515 (median nerve) can reach 70 percent for the dominant hand. Since each extremity is rated separately, a veteran with severe neuropathy in all four extremities could have a significant combined rating even without any single extremity reaching the maximum.
Can I get a VA rating for neuropathy caused by Agent Orange?
Yes. Early-onset peripheral neuropathy is a presumptive condition for veterans exposed to herbicide agents during military service. The neuropathy must have manifested to at least 10 percent disabling within one year of the last herbicide exposure. If your neuropathy appeared later, you may still pursue direct service connection with a medical nexus opinion linking the condition to your herbicide exposure.
Does neuropathy qualify for TDIU (Total Disability Individual Unemployability)?
If your service-connected neuropathy (alone or combined with other service-connected conditions) prevents you from maintaining substantially gainful employment, you may qualify for TDIU. This provides compensation at the 100 percent rate even if your combined rating is below 100 percent. You need either one service-connected disability rated at least 60 percent, or two or more disabilities with a combined rating of at least 70 percent (with at least one rated at 40 percent or more).
How long does a VA neuropathy claim take?
Average processing time for initial disability claims is approximately 3 to 6 months, though complex claims can take longer. Claims filed through va.gov tend to process faster than paper submissions. Having all evidence ready at the time of filing — including medical records, nexus letters, and buddy statements — reduces processing time. Appeals can add 6 months to several years depending on the pathway chosen.
Can my neuropathy rating be increased if symptoms get worse?
Yes. File a claim for increased evaluation (VA Form 21-526EZ) with updated medical evidence showing worsening symptoms. New EMG and nerve conduction studies comparing current results to your baseline are the strongest evidence. Document how increased symptoms have further limited your daily activities and employment capacity. There is no limit on how many times you can request an increase, but each request should include evidence of actual worsening since the last evaluation.
What secondary conditions can I claim from neuropathy?
Common secondary conditions to neuropathy include sleep disorders and insomnia, depression and anxiety, gait abnormality leading to knee or hip problems, radiculopathy, erectile dysfunction, and falls resulting in orthopedic injuries. Each secondary condition receives its own rating. If neuropathy is already service-connected, any condition caused or aggravated by it can be claimed as secondary.
Next Steps for Veterans With Neuropathy
You earned your benefits through service. Don't leave them on the table because the system is complex or because you've been trained to push through pain without complaining.
Start with these concrete actions:
- Get a current diagnosis — See a neurologist and get EMG/nerve conduction studies if you haven't recently
- Identify your service connection pathway — Direct, presumptive, or secondary. Gather the evidence specific to your pathway
- Start a symptom journal today — 30 days of documented symptoms strengthens any claim
- Contact a VSO — Free help from organizations that do this every day. Find one at va.gov/vso
- File your claim — The sooner you file, the earlier your effective date for back pay if approved
The VA system is imperfect, but the benefits are real — and for veterans living with the daily reality of neuropathy, every percentage point matters.


