The first time my doctor wrote “nortriptyline” on a prescription pad and slid it across the desk, I remember thinking — wait, isn't that an antidepressant? I wasn't depressed. I was in pain. I went home, looked it up, and found myself in a confusing little corner of pharmacology where a 70-year-old class of drugs originally developed for melancholy still gets prescribed every day for neuropathy.
Nortriptyline (brand name Pamelor) is a tricyclic antidepressant — a TCA — that quietly does double duty in the world of nerve pain management. It's not the most exciting medication on the menu. It's not new. It's not heavily marketed. But it has a long, useful history with neuropathic pain, and for some people it works when other things haven't.
If your doctor has mentioned nortriptyline, or if you're weighing options beyond gabapentin or duloxetine, this article walks you through what nortriptyline actually does, what the research says, what dosing looks like, what side effects to expect, and how it stacks up against the medications it usually competes with.
What Is Nortriptyline?
Nortriptyline is a prescription tricyclic antidepressant in the secondary amine subgroup. It's FDA-approved for major depressive disorder and is one of the older medications still in regular clinical use — the original tricyclic antidepressants were introduced in the late 1950s, and nortriptyline has been around since 1964.
Key Takeaway
Nortriptyline is FDA-approved for depression but widely prescribed off-label for neuropathic pain at lower doses than the antidepressant range. Bedtime dosing leverages its sedative effect to help with sleep — a meaningful bonus for nighttime nerve pain.
Here's something interesting that helps the comparison make sense: nortriptyline is the active metabolite of amitriptyline. When you take amitriptyline, your liver converts a portion of it into nortriptyline. Doctors realized decades ago that you could just prescribe the metabolite directly and get a cleaner profile — fewer side effects, especially the ones tied to histamine and acetylcholine receptors that make older TCAs notoriously hard to tolerate.
For neuropathic pain, nortriptyline is used off-label. It does not have FDA approval specifically for nerve pain. But like several medications in the antidepressant class, the off-label use is well-established, supported by decades of clinical experience, and recommended by major pain management guidelines as a treatment option.
How Does Nortriptyline Work for Nerve Pain?
The mechanism is one of those satisfying scientific stories where a medication originally targeted at one problem turns out to address a completely different one through the same neurochemistry.
How Nortriptyline Affects Pain Signaling
1. Blocks Norepinephrine Reuptake
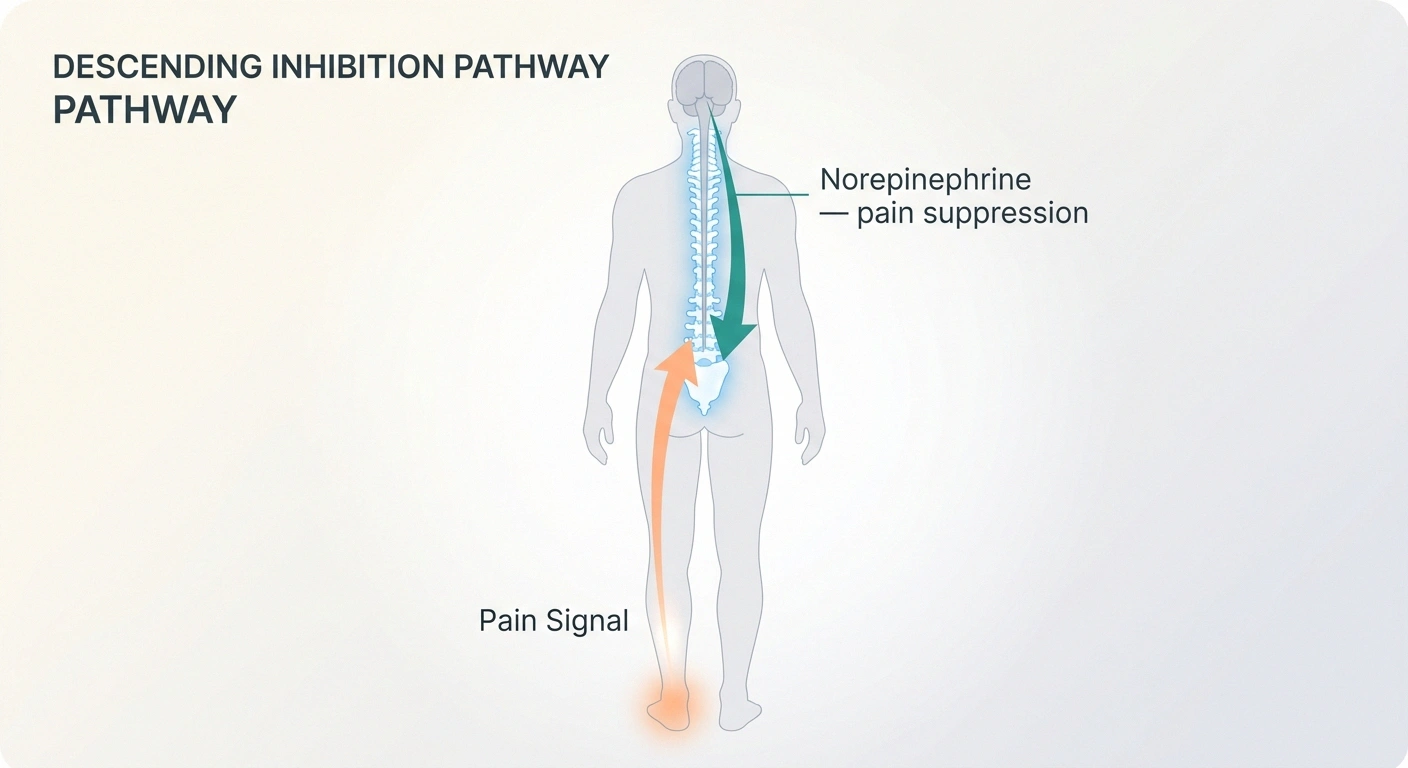
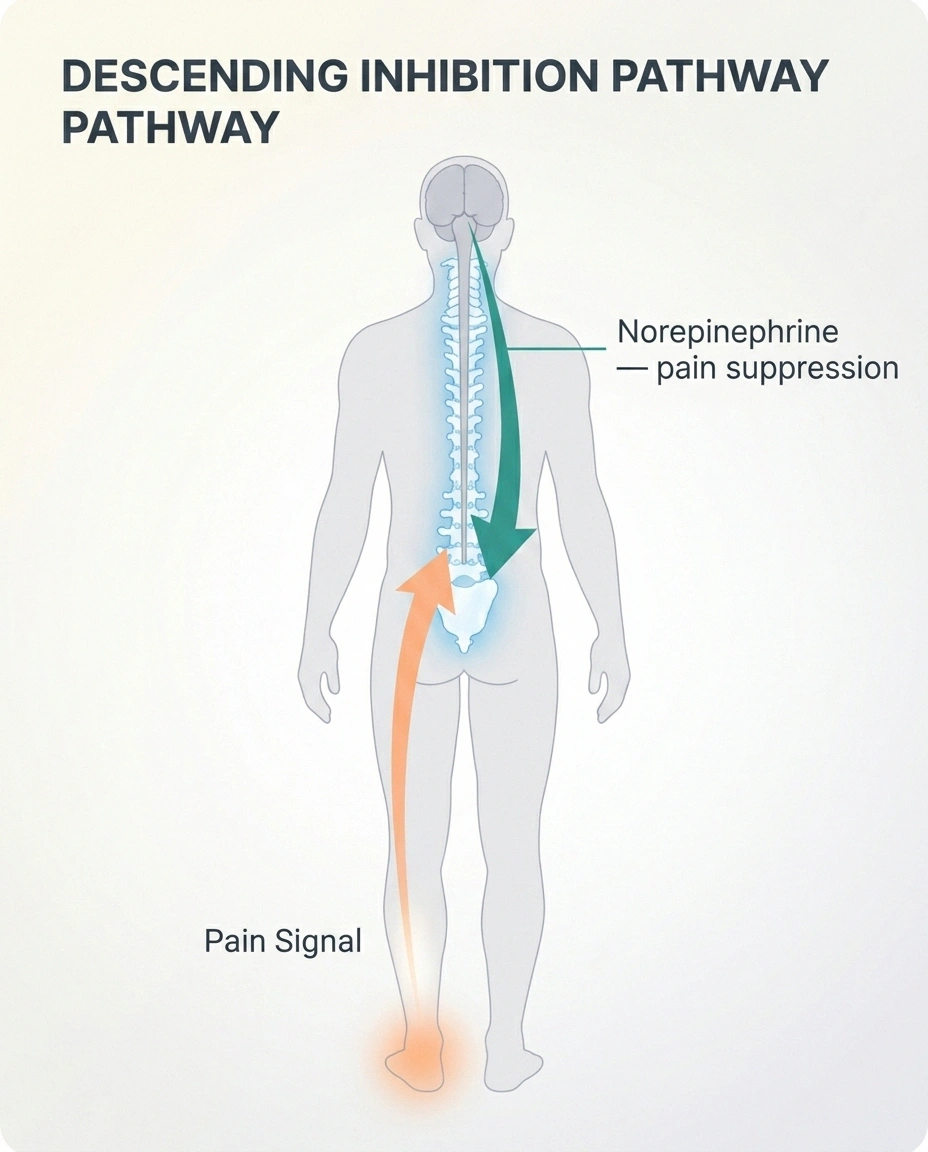
More norepinephrine stays available in the synapse — particularly in descending pain pathways from the brainstem to the spinal cord.
2. Strengthens Pain Suppression
Enhanced descending inhibition turns down the volume on incoming pain signals before they reach conscious awareness.
3. May Quiet Hyperexcitable Nerves at the Source
Norepinephrine acting on satellite glial cells in the dorsal root ganglia may reduce abnormal firing of damaged sensory nerves directly.
Nortriptyline blocks the reuptake of two neurotransmitters in the brain and spinal cord: norepinephrine (its main effect) and serotonin (a smaller effect). When reuptake is blocked, these neurotransmitters stay active in the synapse longer, which amplifies their signaling.
For pain, the relevant action is mostly about norepinephrine. Your spinal cord has descending pathways from the brainstem that can dampen incoming pain signals before they reach conscious awareness. These pathways are noradrenergic — they use norepinephrine as their messenger. When nortriptyline boosts available norepinephrine in those pathways, the brain's natural pain-suppression circuit gets stronger.
There's a second mechanism that may also matter for nerve pain specifically. Some research suggests that norepinephrine acting on β2-adrenoceptors of satellite glial cells around dorsal root ganglia (the bundles of sensory nerves outside the spinal cord) can quiet down hyperexcitable nerves at the source — not just modulate the signal in the spinal cord. This is part of why TCAs sometimes help neuropathic pain when other classes don't.
The dose required for pain relief is generally lower than the dose required for treating depression. People often hear “nortriptyline is an antidepressant” and assume they're being prescribed an antidepressant dose, but the analgesic effect appears at substantially lower doses than the antidepressant effect — typically 25-75 mg, compared to 75-150 mg for depression.
What Does the Research Show?
The honest answer is: the evidence base for nortriptyline in neuropathic pain is real but not enormous.
🔎 Research Says
The 2015 Cochrane review (Derry et al.) concluded high-quality trial evidence for nortriptyline in neuropathic pain is limited. Major guidelines still list TCAs as a first-line option — reflecting decades of clinical experience, not strong meta-analytic certainty.
The most rigorous review is a Cochrane analysis (Derry et al., 2015) that pooled the available randomized controlled trials. The conclusion was sobering — there was insufficient high-quality evidence to firmly support nortriptyline as a first-line treatment, and other neuropathic pain medications like duloxetine and pregabalin have larger, stronger evidence bases.
That said, “insufficient evidence” doesn't mean “doesn't work.” It means the studies that exist were small, often older, and used methods that don't meet modern trial standards. Decades of clinical experience suggest nortriptyline does help a meaningful proportion of patients — especially when:
- Other first-line medications haven't worked or weren't tolerated
- The patient has trouble sleeping (sedation becomes a feature, not a bug)
- Cost is a major factor (generic nortriptyline is inexpensive)
- The patient also has tension headaches, fibromyalgia, or other chronic pain conditions where TCAs help
Major guidelines — including those from the International Association for the Study of Pain and the European Federation of Neurological Societies — list TCAs (including nortriptyline) as a first-line option alongside duloxetine, gabapentin, and pregabalin for neuropathic pain. The “first-line” designation reflects clinical consensus more than meta-analytic certainty.
Who Might Benefit Most from Nortriptyline?

Nortriptyline isn't right for everyone, but there are situations where it becomes a particularly thoughtful choice to discuss with your doctor:
When you also struggle with sleep
Many people with neuropathy describe the worst pain hitting at bedtime — the way the burning seems to amplify in the quiet hours. Nortriptyline taken before bed has a sedative effect that can help you fall asleep and reduce pain. Two problems treated by one bedtime pill is a real win. If you're already taking a sleep aid plus a separate pain medication, nortriptyline can sometimes consolidate that. Why neuropathy gets worse at night — and how this kind of bedtime medication strategy fits in — is worth understanding.
When you've tried gabapentin and it didn't work or made you feel foggy
Gabapentin and pregabalin are common first attempts for neuropathic pain, but they don't work for everyone, and the cognitive side effects (“gabapentin fog”) drive many people to look for alternatives. Nortriptyline has a completely different mechanism and may work where gabapentin failed.
When cost is a factor
Generic nortriptyline is among the least expensive prescription pain medications available. Compare that to brand-name pregabalin or even some generic versions of newer drugs, and the difference can be hundreds of dollars per month.
When you're managing depression or anxiety alongside neuropathy
Although nortriptyline is no longer commonly used as a first-line antidepressant, the dual benefit isn't nothing. The connection between neuropathy and mental health is real, and a single medication that addresses both can be valuable in some situations.
For comorbid migraine, tension headache, or fibromyalgia
TCAs including nortriptyline have evidence for prevention of migraine and tension headache, and for fibromyalgia. If you have multiple chronic pain conditions, one medication that helps several is more elegant than a separate prescription for each.
Dosing for Neuropathic Pain: What to Expect
The dosing approach for neuropathic pain is gentler and more cautious than what's used for depression. The general principle is “start low, go slow” — and bedtime dosing.
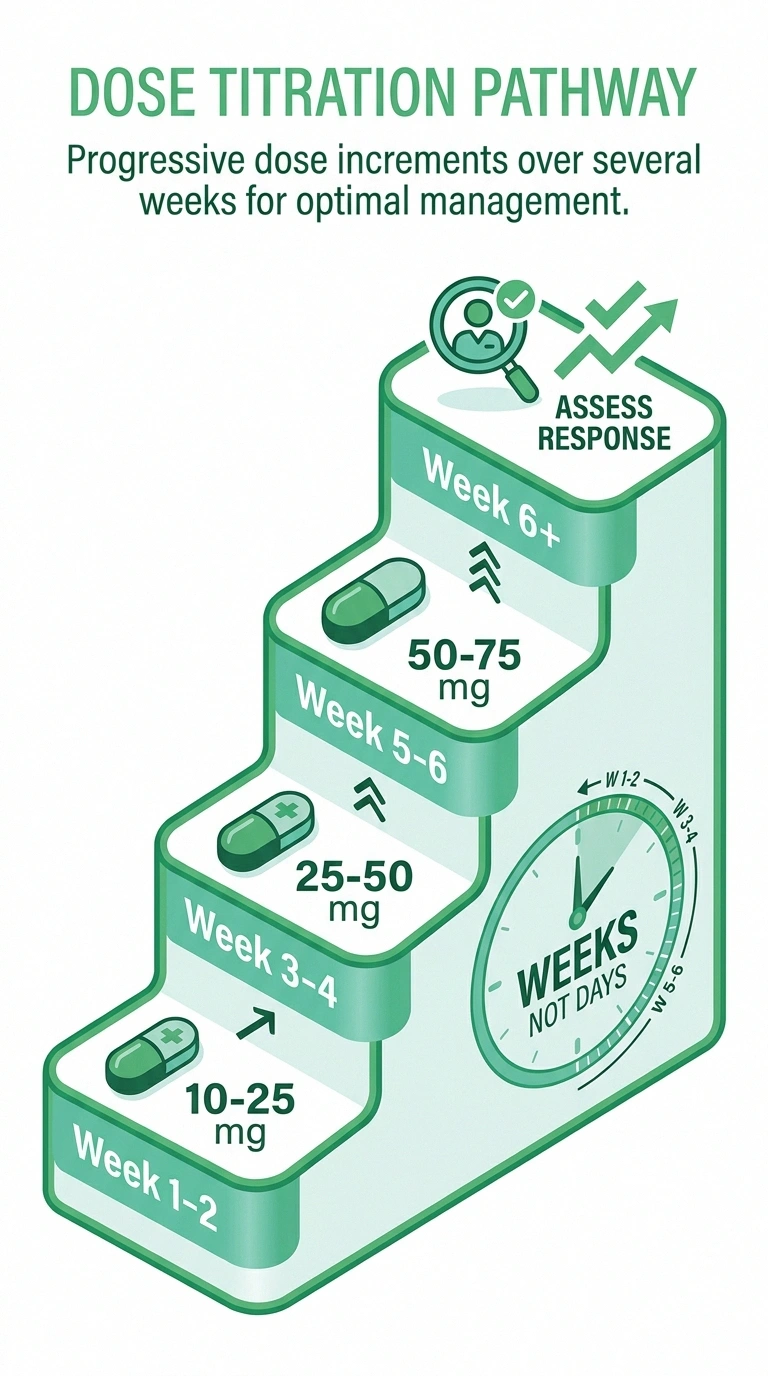
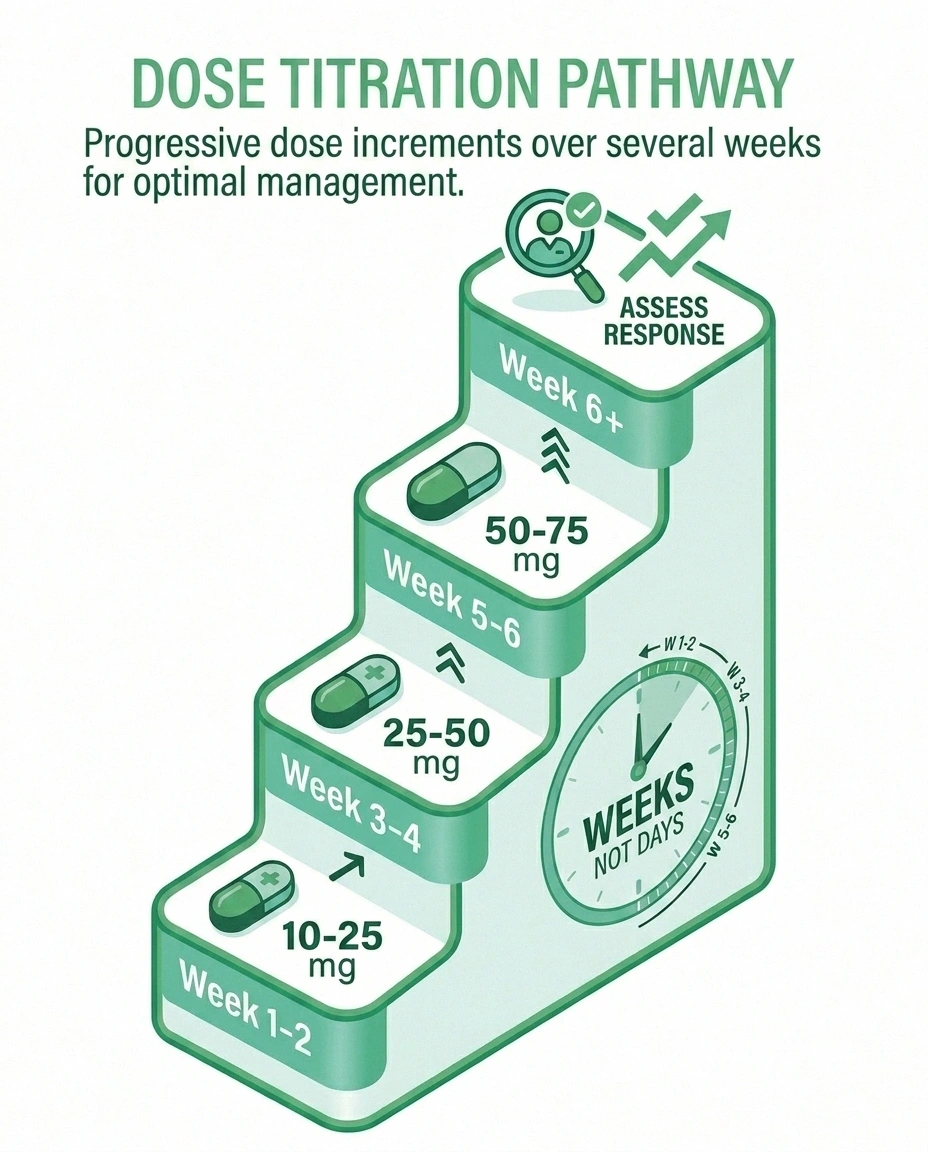
Typical Nortriptyline Titration for Nerve Pain
Week 1-2: 10-25 mg at bedtime
Week 3-4: Increase to 25-50 mg if tolerated
Week 5-6: Target dose typically 50-75 mg
Week 6+: Assess pain response. Some need up to 100 mg.
Take the dose 1-2 hours before bed to reduce morning grogginess.
Starting Dose: 10-25 mg taken at bedtime. Many doctors start at 10 mg in older adults to minimize side effects.
Titration: Increase by 10-25 mg every 1-2 weeks as tolerated, based on pain response and side effects. Typical target is 50-75 mg, though some people benefit at 25 mg and others need up to 100 mg.
Timing: Take at bedtime. The sedative effect helps with sleep, and morning grogginess is reduced if the dose is taken 1-2 hours before bed (rather than just as you're climbing in).
Onset of pain relief: Some people notice improvement within 1-2 weeks. Full effect typically takes 4-6 weeks at the target dose. Don't conclude it isn't working before giving it adequate time.
Therapeutic blood levels: For depression, blood level monitoring is sometimes used (the therapeutic window is roughly 50-150 ng/mL). For pain, blood level testing is usually unnecessary because the effective dose range is lower and clinical response is the guide.
One detail that helps people stick with nortriptyline through the early adjustment: the morning grogginess that's most pronounced in the first 1-2 weeks usually settles considerably as your body adjusts. If you're feeling like a zombie in the morning during week one, that's not a permanent verdict — it's a typical adaptation phase.
Side Effects: What to Watch For

Nortriptyline has a recognizable side-effect profile. Knowing what to expect helps you tell what's normal and what to flag to your doctor.
Cardiac Caution
Nortriptyline can prolong the QT interval. If you have a history of heart rhythm problems, recent heart attack, or take other QT-prolonging medications, your doctor should review this carefully — and an ECG before starting may be wise.
Anticholinergic side effects are the classic TCA pattern: dry mouth, blurred vision, constipation, urinary retention. Nortriptyline has these effects more mildly than older TCAs like amitriptyline, but they're still common. Most are manageable — sip water, use sugar-free hard candy for dry mouth, increase fiber and fluids for constipation.
Drowsiness and morning grogginess are most pronounced early on. As mentioned, taking the dose 1-2 hours before bed (rather than at bedtime itself) helps reduce morning fog.
Weight gain is a recognized effect of TCAs over time. It's typically modest at lower doses but worth tracking.
Dizziness on standing (orthostatic hypotension) — getting lightheaded when rising from sitting or lying. This is more common in older adults and is one of the reasons nortriptyline is often started at the very lowest dose in patients over 65. Standing up slowly helps.
Heart rhythm effects — nortriptyline can prolong the QT interval on an ECG. For most people this is clinically meaningless, but in patients with pre-existing heart rhythm issues, certain electrolyte abnormalities, or those taking other QT-prolonging medications, an ECG before starting and periodic monitoring may be wise. Your doctor should ask about cardiac history before prescribing.
Sexual side effects — TCAs can cause decreased libido and difficulty with arousal or orgasm. These are generally less severe than with SSRIs but still present.
Black box warning — like all antidepressants, nortriptyline carries an FDA black box warning for increased risk of suicidal thoughts in young adults under 25. For the older neuropathy population this is rarely the relevant concern, but it's a real consideration in younger patients.
Nortriptyline vs. Amitriptyline: Why the Newer Cousin Often Wins
If your doctor mentions tricyclic antidepressants for nerve pain, the two names that come up are amitriptyline and nortriptyline. Here's the practical comparison:
Amitriptyline is the older, parent compound. It has more anticholinergic effects (more dry mouth, more constipation, more urinary retention), more sedation, and more orthostatic hypotension. It also has more cardiac effects. It's well-studied for neuropathic pain, but its side effect profile makes it harder to tolerate, especially in older adults.
Nortriptyline is the active metabolite of amitriptyline — meaning your body makes nortriptyline from amitriptyline anyway. By prescribing nortriptyline directly, you avoid much of the side effect burden of the parent compound while keeping most of the analgesic effect. For most patients, nortriptyline is the better-tolerated TCA option.
The American Geriatrics Society's Beers Criteria — the standard guide for medications that may be inappropriate for older adults — lists amitriptyline as a medication to generally avoid in older adults due to its strong anticholinergic burden. Nortriptyline isn't on the same warning list, though caution is still advised. If you're over 65 and your doctor offers a TCA, nortriptyline is generally the safer choice.
Nortriptyline vs. Duloxetine and Gabapentin

These three medications are commonly considered together because they're often the first-line options for neuropathic pain. They work through different mechanisms and have different side effect profiles.
First-Line Neuropathic Pain Medications: Quick Comparison
| Factor | Nortriptyline | Duloxetine | Gabapentin |
|---|---|---|---|
| FDA approval for neuropathy | Off-label | Yes (diabetic) | Yes (post-herpetic) |
| Best for sleep? | Yes — sedating | Neutral | Mild sedation |
| Cost (generic) | Very low | Moderate | Low |
| Main side effects | Dry mouth, grogginess | Nausea, fatigue | Sedation, fog |
| Once-daily dosing | Yes (bedtime) | Yes | Usually 3x daily |
Nortriptyline (TCA): Norepinephrine reuptake inhibition. Bedtime dosing helps sleep. Side effects: dry mouth, constipation, weight gain, morning grogginess, mild cardiac effects. Inexpensive.
Duloxetine (SNRI): Norepinephrine and serotonin reuptake inhibition (more balanced). FDA-approved for diabetic neuropathy. Side effects: nausea (especially early), fatigue, sweating, sexual side effects, blood pressure effects. Larger evidence base.
Gabapentin (gabapentinoid): Modulates calcium channels on nerve endings. Side effects: sedation, dizziness, weight gain, cognitive fog, ankle swelling. Largest evidence base of the three.
Which is “best” depends on the individual. If sleep is a problem, nortriptyline often wins. If diabetic neuropathy is the diagnosis and FDA-approved medication is preferred, duloxetine has that edge. If anxiety co-exists, gabapentin sometimes addresses both. Combining medications is also common — a low-dose TCA at bedtime plus daytime gabapentin, for example, is a frequent regimen.
Who Should Not Take Nortriptyline
There are several important contraindications and cautions to be aware of:
- MAOIs: Do not take nortriptyline within 14 days of stopping a monoamine oxidase inhibitor (or vice versa). The combination can cause serotonin syndrome.
- Recent heart attack: TCAs are generally avoided in the first weeks to months after a myocardial infarction.
- Significant heart rhythm problems: Long QT syndrome, certain arrhythmias, and conduction blocks may make nortriptyline unsafe.
- Severe glaucoma: Anticholinergic effects can worsen narrow-angle glaucoma.
- Urinary retention: Particularly relevant for men with significant prostate enlargement.
- Bipolar disorder: Like other antidepressants, nortriptyline can potentially trigger a manic episode in undiagnosed or untreated bipolar disorder.
- Pregnancy and breastfeeding: A risk-benefit discussion with your doctor is needed.
Always provide your prescriber with a full list of medications, including over-the-counter products and supplements. Nortriptyline interacts with several common medications including SSRIs, MAOIs, certain antiarrhythmics, and others. The how to talk to your doctor about neuropathy pain guide can help you frame that conversation.
Stopping Nortriptyline: Tapering Required
Like other antidepressants, nortriptyline should not be stopped abruptly. Sudden discontinuation can produce a withdrawal syndrome with flu-like symptoms, vivid dreams, dizziness, headache, and rebound of cholinergic effects (excess saliva, GI symptoms, sweating). It's not as severe as the discontinuation syndrome from venlafaxine or some SSRIs, but it's real.
Don't Stop Cold Turkey
Stopping nortriptyline abruptly can cause flu-like symptoms, vivid dreams, dizziness, and rebound effects. Always taper gradually — typically 10-25 mg every 1-2 weeks — under your doctor's guidance.
The general approach is to taper gradually — typically reducing by 10-25 mg every 1-2 weeks. Your doctor should provide a specific tapering schedule based on your dose and how long you've been on the medication.
Frequently Asked Questions
Is nortriptyline effective for neuropathic pain?
Nortriptyline has been used for neuropathic pain for decades and is recommended as a first-line option in major pain guidelines, though the formal evidence base from randomized controlled trials is smaller than for medications like duloxetine and gabapentin. Many patients respond well, particularly at doses of 25 to 75 mg taken at bedtime. The 2015 Cochrane review concluded the high-quality evidence is limited but not absent — meaning it works for some people, even if the trials are not as definitive as those for newer drugs.
What is the typical starting dose of nortriptyline for nerve pain?
Most prescribers start at 10 to 25 mg taken at bedtime. Older adults often start at 10 mg to reduce side effects. The dose is increased every 1 to 2 weeks as tolerated, with a typical target range of 25 to 75 mg, though some people respond at lower doses and others need up to 100 mg. Pain relief usually takes 1 to 6 weeks to develop fully, so patience and adequate time at each dose are important.
How long does nortriptyline take to work for neuropathy?
Some people notice improvement within 1 to 2 weeks. Full pain relief typically takes 4 to 6 weeks at an adequate dose. The most common reasons people conclude nortriptyline is not working are stopping too soon and never reaching an adequate dose. Tracking pain weekly on a 1 to 10 scale helps you and your doctor judge whether the medication is helping or whether to adjust the dose.
What are the most common side effects of nortriptyline?
Dry mouth, drowsiness, morning grogginess, constipation, blurred vision, weight gain, and dizziness on standing are the most common side effects. Most are mild to moderate and improve over the first 1 to 2 weeks. The morning grogginess is often reduced by taking the dose 1 to 2 hours before bedtime rather than at bedtime itself. Cardiac rhythm effects can occur, so patients with pre-existing heart conditions may need an ECG before starting and periodic monitoring.
Is nortriptyline better than amitriptyline for nerve pain?
Nortriptyline is the active metabolite of amitriptyline and generally has fewer side effects, particularly fewer anticholinergic effects (dry mouth, constipation, blurred vision) and less sedation. The pain-relieving effect is comparable. For older adults especially, nortriptyline is usually preferred over amitriptyline because of better tolerability. Both work, but nortriptyline tends to be the easier of the two to live with.
Can you take nortriptyline with gabapentin?
Yes, nortriptyline and gabapentin are often combined for neuropathic pain because they work through different mechanisms — nortriptyline through norepinephrine reuptake inhibition and gabapentin through calcium channel modulation. The combination can produce better pain relief than either alone. The main caution is that both can cause sedation, so dosing is usually adjusted to minimize cumulative drowsiness. This is a conversation to have with your doctor or pharmacist.
Will nortriptyline make me gain weight?
TCAs including nortriptyline can cause modest weight gain over time, though the effect at the lower doses used for nerve pain is typically smaller than at antidepressant doses. The mechanism is thought to involve increased appetite and possibly slower metabolism. Maintaining regular exercise, monitoring weight monthly, and discussing significant changes with your doctor are reasonable strategies.
Can I drink alcohol while taking nortriptyline?
Combining nortriptyline with alcohol increases sedation and impairs coordination — a particular concern given that neuropathy already increases fall risk. Most prescribers recommend avoiding alcohol or limiting it significantly. Discuss your specific situation with your doctor or pharmacist if alcohol is a regular part of your life.