
One of the most disorienting things about living with neuropathy isn't the pain — it's the sensations that don't match reality. Feeling like you're stepping on sand or small pebbles when the floor is perfectly smooth. A warm dripping sensation on your arm when nothing is there. The insistent feeling of a bunched-up sock when you're not wearing any.
These are phantom sensations — experiences generated entirely by damaged nerves, with no external cause. They're not imagined. They're not a sign of mental illness. They're the nervous system doing something deeply strange and surprisingly well-documented.
Understanding what's happening when your nerves invent sensations out of nothing can help you make sense of your own experience — and know what management options actually exist.
What Makes a Sensation “Phantom”?
In everyday language, “phantom” sensations are most often associated with amputees who feel pain or tingling in a limb that's no longer there. But people with peripheral neuropathy experience a different but related phenomenon: sensations that arise from nerve fibers that are still present — but damaged and misfiring.
The key distinction is this: in healthy nerves, sensations are generated in response to actual stimuli. Touch your hand to a warm mug, and heat receptors fire, sending a signal to your brain that correctly reports warmth. In neuropathy, the sensory pathway itself begins generating signals without any stimulus — spontaneously, and often in ways that don't match what the external world is actually doing to your body.
Medical terminology for these experiences includes:
- Paresthesia: Abnormal sensations that aren't typically painful — tingling, pins and needles, buzzing, crawling sensations. The limb is present and intact, but the sensation arises without cause.
- Dysesthesia: Abnormal sensations that are uncomfortable or painful. These include burning without a heat source, electric shocks without contact, or painful pressure sensations without applied force.
- Spontaneous pain: Pain arising without any stimulus at all — the nerve generates a pain signal from nothing.
All of these qualify as “phantom” in the sense that they're generated internally rather than triggered by the outside world. And for most people with neuropathy, they represent some of the most confusing and frustrating symptoms of the condition.
The Neuroscience Behind Spontaneous Nerve Firing
To understand why damaged nerves generate phantom sensations, it helps to understand a little about how nerves normally work.
Three Mechanisms Behind Phantom Sensations
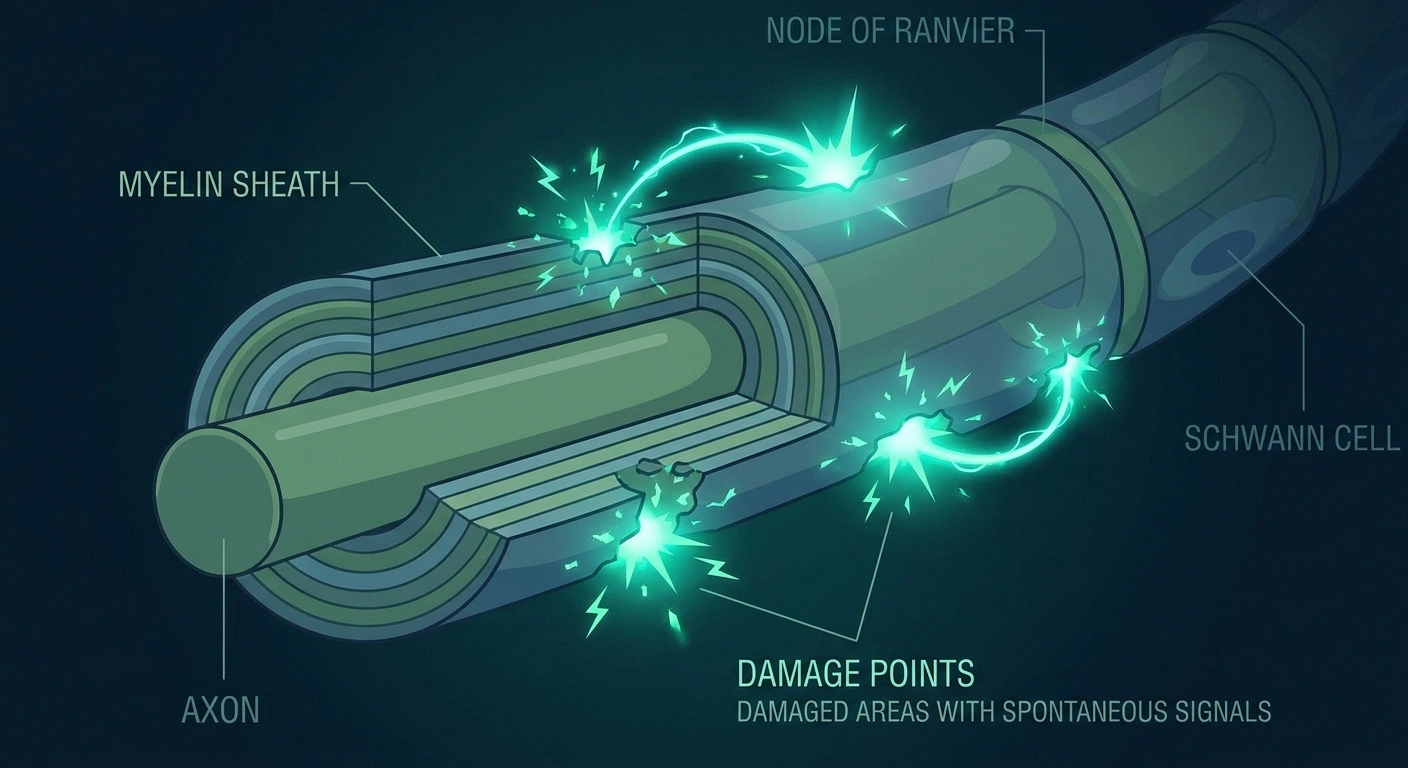
Ectopic Discharge
Damaged axons develop unstable sodium channels that fire spontaneously. The brain receives signals with no cause.
Fiber Cross-Talk
Electrical signals “leak” between damaged nerve fibers, triggering sensations that don't match the original signal.
Central Sensitization
Repeated abnormal signals sensitize the spinal cord, which amplifies and sustains the phantom experiences.
Healthy nerve fibers transmit signals through a carefully regulated system of ion channels — proteins embedded in the nerve membrane that open and close in precise sequences to generate electrical impulses. The process is orderly: a stimulus at one end triggers a cascade that travels predictably toward the brain.
Nerve damage disrupts this order in several ways:
Key Takeaway
Phantom sensations in neuropathy are not imagined — they are real neurological events generated by damaged nerve fibers firing without any external trigger. Understanding the mechanism helps separate the experience from fear about what it means.
Ectopic discharge: Damaged nerve fibers develop abnormal sodium channels at injury sites — and sometimes along the entire length of the damaged axon. These channels are unstable, triggering spontaneous electrical activity without any stimulus. The brain receives signals it interprets as sensations, even though nothing in the external world caused them. This is the most direct mechanism behind phantom sensations.
Abnormal ion channel expression: Nerve injury changes which types of ion channels a nerve produces. Some nerve damage leads to upregulation of channel subtypes that lower the threshold for firing — meaning the nerve fires more easily, more often, and more spontaneously than it should.
Cross-talk between nerve fibers (ephaptic transmission): When nerve fibers are demyelinated or tightly packed in areas of injury, electrical activity in one fiber can leak into adjacent fibers and trigger them. A signal intended to convey “light touch” can spill over and activate pain fibers — creating pain from nothing, or creating sensations that blend inappropriately.
These mechanisms operate in the peripheral nervous system, at the nerve fiber level. But the brain and spinal cord also play a role.
How the Brain and Spinal Cord Amplify Phantom Sensations
The peripheral nerve is where phantom sensations start, but not always where they end.
When peripheral nerves send abnormal signals repeatedly and persistently, the spinal cord begins to change in response. Spinal cord neurons become sensitized — they fire more easily, respond to weaker signals, and sometimes begin generating their own spontaneous activity. This process, called central sensitization, means that phantom sensations originally generated in a damaged peripheral nerve can become amplified and self-sustaining at the spinal cord level.
At the brain level, chronic abnormal input from damaged nerves can trigger cortical reorganization — the brain's sensory maps literally rewire in response to changed input patterns. This reorganization can perpetuate abnormal sensory experiences even when the peripheral nerve damage stabilizes, and it helps explain why phantom sensations can persist or worsen long after the initial nerve injury.
This is a different mechanism from what's purely happening in the peripheral nerve, and it's one reason why treatments aimed only at the nerve fiber level sometimes fail to resolve phantom sensations completely — the central nervous system has developed its own contribution to the problem.
Common Phantom Sensation Patterns in Neuropathy

People with neuropathy report a striking variety of phantom sensations. Some of the most commonly described include:
Common Reports from Neuropathy Patients
- “Walking on sand or gravel — barefoot”
- “My feet are burning but they feel cold”
- “Water dripping down my leg”
- “My sock is bunched up — but I have no socks on”
- “Random electric shocks from nowhere”
- “My foot feels swollen but looks normal”
“Walking on sand or pebbles”: The feeling of small granular material underfoot, even on a smooth surface and without shoes. This is one of the most common descriptions in peripheral neuropathy, particularly in diabetic neuropathy. It results from spontaneous activity in the sensory fibers that normally report surface texture.
Phantom warmth or burning: Feeling intense heat — sometimes described as burning coals, hot sand, or scalding water — when the affected area is actually cool or at normal temperature. This is a form of thermal dysesthesia driven by misfiring heat-sensing C-fibers.
Dripping or moisture sensation: Feeling liquid running down the leg, foot, or arm when nothing is there. This results from spontaneous firing of mechanoreceptors that normally detect fluid contact or pressure changes.
Vibration sensations: Feeling a buzzing, vibrating, or trembling sensation in the feet or legs when no vibration source exists. This is distinct from tremor — the limb isn't moving, only the sensation is present.
Wrinkled sock / bunched insole: A persistent sensation of fabric texture, lumps, or folds under the foot when the foot is bare or wearing well-fitting footwear. The sensory fibers that detect material contact continue firing inappropriately.
Electric shock sensations: Sudden brief shocks or stabs that feel like touching a live wire. These are sharp, unexpected, and can occur spontaneously or be triggered by movement. They're the hallmark of electric shock sensations in neuropathy.
Swelling sensations: Feeling that a foot or hand is swollen when it visibly isn't. The sensory fibers that normally detect tissue pressure and stretch misfire, creating internal pressure sensations without external cause.
Phantom Sensations vs. Allodynia vs. Hyperalgesia
These terms are often used interchangeably, but they describe distinct phenomena:
Phantom sensations / spontaneous dysesthesias: Arise without any external trigger. Nothing touches you, no temperature change occurs, no pressure is applied — yet you feel burning, tingling, dripping, or other sensations. The nerve generates experience from nothing.
Allodynia: Pain provoked by stimuli that normally don't cause pain — the light pressure of bedsheets, a gentle breeze, water temperature that anyone else would call neutral. The stimulus is real, but the response is wildly disproportionate. The nerve is over-responsive, not spontaneously firing.
Hyperalgesia: An exaggerated pain response to stimuli that do normally cause pain. A mildly painful stimulus produces severe pain. Like allodynia, a real trigger is present — but the nerve's response is amplified far beyond normal.
Many people with neuropathy experience all three simultaneously in affected areas. A foot might have spontaneous burning (phantom), pain from sock contact (allodynia), and extreme pain from stubbing a toe that would be a minor event for anyone else (hyperalgesia). They reflect different aspects of the same underlying dysfunction — and understanding which is dominant can help guide treatment decisions.
Which Types of Neuropathy Produce the Most Phantom Sensations?
Phantom sensations and spontaneous dysesthesias are most prominent in conditions affecting small nerve fibers — the thin, lightly myelinated A-delta fibers and unmyelinated C-fibers responsible for pain and temperature sensation.
Small fiber neuropathy is particularly associated with spontaneous burning, phantom heat sensations, and the sand/pebble walking sensation — often with surprisingly little objective evidence of nerve damage on standard tests, because standard nerve conduction studies measure large fibers, not small ones.
Diabetic peripheral neuropathy tends to produce significant phantom sensations, especially spontaneous burning and electric shock symptoms — often most intense at night. Chemotherapy-induced neuropathy from taxanes and platinum-based agents is also strongly associated with persistent dysesthesias.
Idiopathic neuropathy — nerve damage without a known cause — frequently presents with prominent phantom sensations. In fact, for many people with unexplained tingling and burning, the phantom sensation pattern may be an early clue that small fiber neuropathy is present even when large-fiber tests are normal.
What Phantom Sensations Tell Your Doctor
Documenting your phantom sensations accurately is genuinely useful clinical information. The character, timing, and location of spontaneous sensations helps your doctor:
- Determine whether small or large fiber systems are primarily affected
- Identify whether central sensitization may have developed
- Guide medication choices — certain drugs work better for spontaneous burning, others for shooting/electric sensations
- Track progression or improvement over time
When describing phantom sensations, try to specify: What does it feel like exactly? When does it happen — all the time, at night, after activity? What makes it better or worse? Does anything seem to trigger it? Using a neuropathy symptom diary can help you capture this information systematically between appointments.
Treatment Options for Phantom Sensations in Neuropathy

No single treatment eliminates phantom sensations in all patients, but several approaches can reduce their frequency and intensity.
Treatment Principle
The most effective approaches for phantom sensations target both peripheral nerve stability (gabapentin, lidocaine, capsaicin) and the central amplification that develops over time (CBT, mindfulness, sleep improvement). Addressing only one level often produces partial results.
Medications: Anticonvulsants like gabapentin and pregabalin work by stabilizing abnormal nerve firing — they reduce ectopic discharge and raise the threshold for spontaneous activity. SNRIs like duloxetine reduce central sensitization and peripheral pain signal amplification. Tricyclic antidepressants like amitriptyline also modulate pain signal processing at the spinal cord level.
Topical agents: Lidocaine patches applied to the affected area can reduce ectopic discharge locally. Capsaicin — initially intensely stimulating, then depleting the neuropeptides that drive spontaneous fiber activity — can reduce phantom burning and dysesthesias with regular use.
TENS (Transcutaneous Electrical Nerve Stimulation): Provides controlled electrical stimulation that may competitively inhibit the spontaneous signals from damaged fibers. Some people find it helpful for reducing phantom sensations during and after use.
Desensitization techniques: Occupational therapists sometimes use graded texture exposure and gentle sensory stimulation of affected areas to help the nervous system recalibrate its response to sensory input. This is most effective when allodynia and altered sensory processing accompany phantom sensations.
Pain psychology and CBT: The emotional response to unpredictable phantom sensations — fear, frustration, hypervigilance — can amplify central sensitization. Cognitive behavioral therapy and mindfulness approaches help reduce the catastrophizing response that often accompanies phantom sensations and can worsen them. If neuropathy-related anxiety is a factor, addressing it directly often reduces perceived sensation intensity.
Sleep hygiene: Phantom sensations are notoriously worse at night — there are fewer competing signals from the daytime environment, and the brain's pain-suppression systems are less active. Addressing sleep quality indirectly helps with nighttime phantom sensations.
Living with Sensations That Don't Match Reality

Perhaps the most important thing I want to say about phantom sensations is this: they are not a sign that something worse is happening to your nerves in that moment. They are not a reliable indicator of disease progression. They can be wildly variable day to day without that meaning anything significant is changing underneath.
When to See a Doctor Promptly
Day-to-day variation in phantom sensations is expected and doesn't usually signal a crisis. However, contact your neurologist if you notice:
- Rapid worsening over days to weeks
- New symptoms that differ significantly in character
- Sensations spreading to previously unaffected areas quickly
- New weakness or coordination problems alongside phantom sensations
That variability is itself one of the most stressful aspects of phantom sensations — you can go from a day with minimal symptoms to a night of relentless burning with no obvious trigger. Understanding that this fluctuation is normal for damaged nerves, and doesn't necessarily mean you're getting worse, can help reduce the fear response that often amplifies the sensations themselves.
If you've found a combination of things that help — positioning, medication timing, distraction, temperature management — trusting that toolkit matters even on the bad nights. And if you haven't yet had your symptom pattern evaluated by a neurologist familiar with small fiber neuropathy, that's often worth pursuing, because the right characterization of what your nerves are doing shapes the choice of treatment significantly.
Frequently Asked Questions
Why do I feel sensations that aren't caused by anything?
Damaged nerve fibers develop abnormal ion channels that generate spontaneous electrical activity without any external trigger. The brain receives these self-generated signals and interprets them as real sensations — burning, tingling, pressure, dripping, or other experiences. This is called ectopic discharge and is a core mechanism of neuropathic symptoms.
Is the feeling of walking on sand or pebbles a phantom sensation?
Yes. The sensation of walking on small granular material even on a smooth surface is one of the most commonly reported phantom sensations in peripheral neuropathy. It results from spontaneous activity in sensory nerve fibers that normally detect surface texture. It is very common in diabetic peripheral neuropathy and small fiber neuropathy.
Are phantom sensations in neuropathy the same as phantom limb pain?
They share similar mechanisms — both involve the nervous system generating experiences that do not correspond to external reality. However, phantom limb pain occurs after amputation, when nerves still fire despite having no limb to report on. Phantom sensations in neuropathy occur in limbs that are still present, from damaged fibers that misfire. The underlying mechanisms of ectopic discharge and central sensitization overlap considerably.
What makes phantom sensations worse at night?
Several factors converge at night to amplify phantom sensations. Daytime activity provides competing sensory input that can partially suppress abnormal nerve signals. At night, this background stimulation disappears. Additionally, cooler temperatures can affect nerve conduction in already-damaged fibers, and the brain's natural pain-suppression systems are less active during sleep. Anxiety about sleep can also heighten awareness of symptoms.
Can phantom sensations in neuropathy be cured?
Complete elimination of phantom sensations is difficult to achieve, especially when central sensitization has developed alongside peripheral nerve damage. However, meaningful reduction is achievable for most people with the right combination of medication, lifestyle management, and in some cases psychological support. The goal is usually reduction to a manageable level rather than complete elimination.
What is the difference between phantom sensations and allodynia?
Phantom sensations arise without any external trigger. Allodynia is pain caused by stimuli that normally do not cause pain, such as the pressure of bedsheets or a light breeze. Both reflect abnormal nerve function, but phantom sensations require no stimulus, while allodynia requires a real but normally innocuous one. Many people with neuropathy experience both.
Do phantom sensations mean my neuropathy is getting worse?
Not necessarily. Phantom sensations can fluctuate significantly day to day and night to night without indicating progression of underlying nerve damage. Many factors influence their intensity in the short term: fatigue, stress, sleep quality, temperature, and activity level. Consistent worsening over weeks or months is more meaningful than day-to-day variability.


