
You're sitting quietly, maybe reading or watching television, when it happens — a sudden jolt through your foot or leg that feels exactly like you've grabbed a live wire. No warning. No obvious trigger. Just an electric shock sensation that's gone almost as quickly as it arrived, leaving you shaken and wondering what's happening to your body.
If you have peripheral neuropathy, these electric shock-like pains are among the most jarring and frightening symptoms you can experience. I remember when they started for me — I genuinely thought something was wrong beyond the neuropathy, that maybe I was having some kind of cardiac event or neurological crisis. Turns out, as unsettling as they are, these sudden shock sensations are actually a well-understood feature of nerve damage.
This article explains exactly why these electric sensations happen, what they tell you about your nerve damage, and — most importantly — what you can actually do to reduce how often they occur and how intense they feel.
What Are Electric Shock Sensations in Neuropathy?
The medical terms you might encounter for these sensations include paresthesias, dysesthesias, and specifically lancinating pain — that last one describing the sudden, stabbing, shooting quality that feels like an electric discharge. Some patients describe it as a “zap,” others as a “jolt,” and others as a brief but intense current running through a limb.
Key Takeaway
Electric shock sensations in neuropathy happen because damaged nerve fibers misfire spontaneously — they're not a sign of a new crisis, but they do signal that your nervous system needs attention. The same medications used for neuropathic pain (gabapentin, pregabalin, duloxetine) are the most effective treatments.
What they all have in common is that they're spontaneous — meaning they arise from damaged nerves firing on their own, without any external stimulus triggering them. You don't touch anything hot, you don't stub your toe. The nerves just misfire, generating a false signal that your brain interprets as a sudden, intense shock.
These sensations differ from the more constant burning, tingling, or numbness that many people with neuropathic pain experience. Electric shock sensations are intermittent and acute — short, sharp bursts rather than a chronic background hum. Understanding this distinction helps both in describing your symptoms to a doctor and in finding the right treatments.
Why Do Damaged Nerves Produce Electric Shock Sensations?
To understand why neuropathy causes electric shocks, it helps to understand what nerves actually do.
120 m/s
Speed of normal myelinated nerve signal. In damaged nerves, this drops dramatically — leading to erratic firing and electric shock sensations.
Your peripheral nerves are electrical communication cables. They carry signals from your brain to your muscles (motor nerves) and carry information about touch, temperature, and pain back from your skin and tissues to your brain (sensory nerves). These signals travel along nerve fibers as electrical impulses, controlled by channels in the nerve cell membrane that regulate the flow of ions like sodium and potassium.
When neuropathy damages these nerve fibers, several things go wrong:
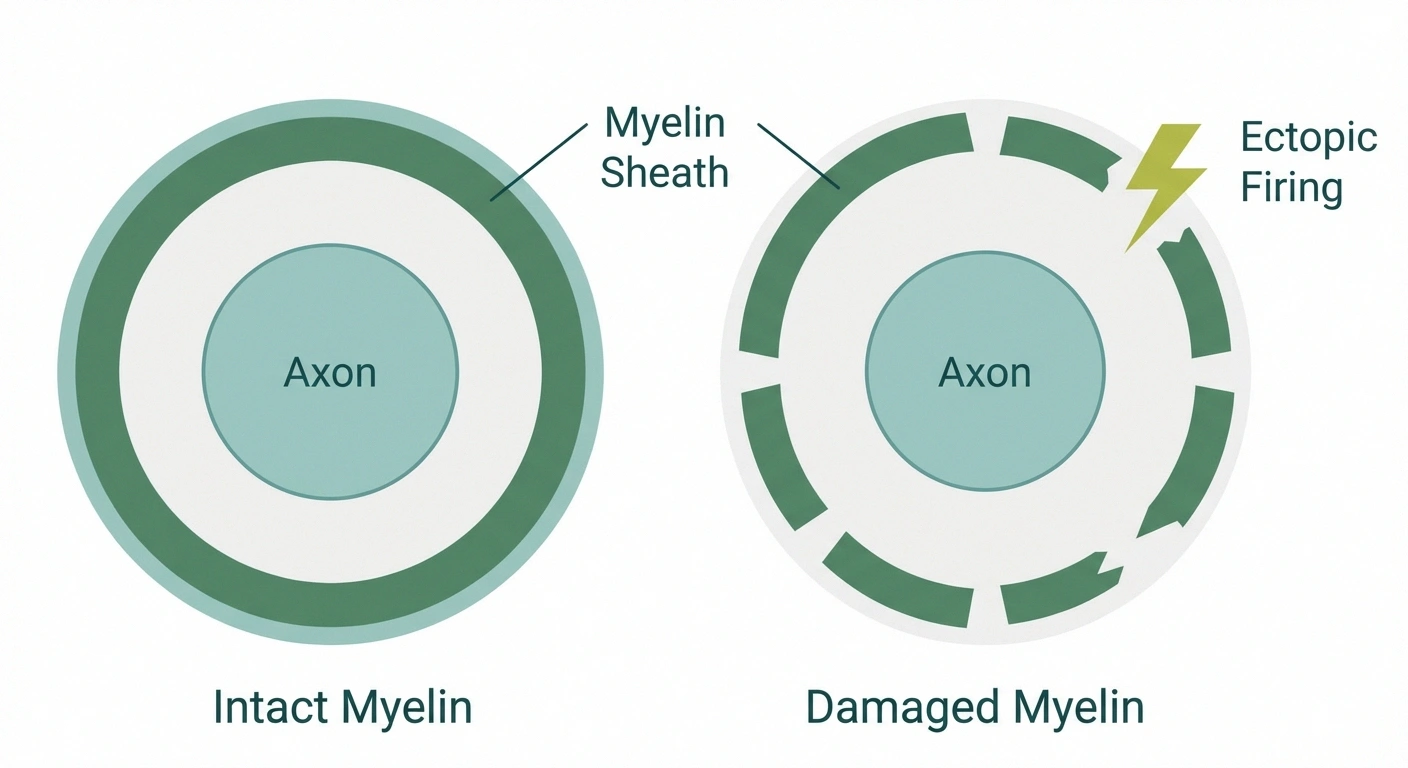
- Ectopic firing: Damaged nerve fibers develop abnormal electrical activity at the site of damage. They begin generating their own impulses spontaneously — not in response to any actual stimulus. This is called ectopic discharge, and it's the primary cause of electric shock sensations.
- Ion channel dysfunction: Nerve damage alters the density and behavior of sodium channels in the nerve membrane. Abnormally high numbers of these channels can accumulate at injury sites, making the nerve hypersensitive and prone to spontaneous firing.
- Cross-talk between fibers: In severe neuropathy, damaged nerve fibers can begin “talking” to neighboring fibers in abnormal ways (called ephaptic transmission). An impulse in one fiber triggers firing in adjacent fibers, amplifying the signal and creating the sensation of a sudden powerful discharge.
- Central sensitization: Over time, repeated pain signals change how your spinal cord and brain process incoming information. The nervous system becomes hypersensitive, amplifying even small misfires into intense perceived shocks.
The result is a nervous system that's misfiring — sending false alarm signals that your brain has no choice but to interpret as intense, shock-like pain.
What Causes Electric Shock Sensations in Neuropathy?
While the mechanism is similar across different types of neuropathy, various underlying causes affect nerves in ways that are particularly prone to producing these electric sensations.
Diabetic Neuropathy
Diabetic peripheral neuropathy is the most common cause of neuropathic pain, affecting approximately 30-50% of people with diabetes over their lifetime. Chronically high blood sugar damages nerve fibers and the small blood vessels that supply them, leading to the kind of fiber loss and abnormal firing that produces electric shock sensations. The feet and lower legs are typically affected first.
Chemotherapy-Induced Neuropathy
Several chemotherapy agents — particularly platinum-based drugs like cisplatin and oxaliplatin, as well as taxanes like paclitaxel — are neurotoxic. They damage nerve fibers in a characteristic “stocking and glove” pattern affecting the hands and feet. Oxaliplatin is particularly notorious for causing acute cold-triggered electric shock sensations during and immediately after infusion.
Post-Herpetic Neuralgia
After a shingles outbreak, the varicella-zoster virus can cause lasting damage to sensory nerve fibers in the affected area. Post-herpetic neuralgia is one of the conditions most frequently associated with lancinating, electric shock-type pain — often described as sudden, excruciating jolts across the skin.
Autoimmune Neuropathies
Conditions like Guillain-Barré syndrome, CIDP (chronic inflammatory demyelinating polyneuropathy), and Sjögren's-associated neuropathy involve immune-mediated attack on nerve fibers or their protective myelin coating. When the myelin sheath is damaged, nerve conduction becomes erratic and prone to the kind of spontaneous misfiring that produces electric sensations.
Small Fiber Neuropathy
Small fiber neuropathy specifically affects the thin, unmyelinated C-fibers and lightly myelinated A-delta fibers that carry pain and temperature information. These fibers are particularly prone to spontaneous discharge, making electric shock sensations a hallmark feature of this condition. Standard nerve conduction tests often miss small fiber neuropathy because these fibers aren't captured by EMG — a skin punch biopsy is needed for diagnosis.
Vitamin Deficiency Neuropathy
B12 deficiency is the most common nutritional cause of neuropathy. Without adequate B12, the myelin sheath deteriorates, and nerves begin misfiring. Copper deficiency and vitamin E deficiency can produce similar effects. The electric shock sensations from B12 deficiency often have an additional characteristic: they may shoot down the spine when you bend your neck (a classic symptom called Lhermitte's sign).
When Are Electric Shocks Worse? Common Triggers
For many people with neuropathy, electric shock sensations aren't random — they follow recognizable patterns. Understanding your triggers gives you some degree of control.

⚠ When to See a Doctor Promptly
- Electric shocks shooting down your spine when you bend your neck (Lhermitte's sign)
- New weakness accompanying the shocks
- Rapid worsening over days, not months
- Bladder or bowel changes appearing alongside new shock sensations
- Shock sensations in locations you've never experienced before
Nighttime: Many people find their electric shock sensations worsen significantly after dark. This is partly because the distractions of the day are gone, making you more aware of sensations, but there are also physiological reasons — blood pressure and circulation patterns change at night, and inflammatory processes can intensify. If this sounds familiar, the article on why neuropathy gets worse at night covers this in detail.
Rest and inactivity: When you stop moving, you lose the competing sensory input that active movement provides. The nervous system's “noise floor” drops, and misfiring nerves become more prominent. This is why many people experience a surge of electric sensations the moment they sit down or lie in bed after being active.
Cold temperatures: Cold can affect nerve conduction velocity and trigger ectopic firing in already-sensitized nerves. Some people find that cold weather reliably worsens their shock sensations; others find cold actually soothes them. This individual variation is real and worth tracking.
Positional changes: Moving from sitting to standing, or bending the knees or ankles, can stretch or compress already-damaged nerves. If your electric shocks happen predictably with certain movements, nerve compression at a specific site (like tarsal tunnel syndrome or lumbar radiculopathy) may be contributing alongside your peripheral neuropathy.
Stress: Emotional stress doesn't cause nerve damage, but it activates the sympathetic nervous system, which can amplify pain perception. Many people notice their electric shock sensations cluster during high-stress periods.
Fatigue: When you're exhausted, your brain's pain-modulating systems are less effective. Sensations that might be barely noticeable when you're rested can become overwhelming when you're depleted.
How to Describe Electric Shock Sensations to Your Doctor
Getting accurate treatment depends heavily on giving your doctor a clear picture of what you're experiencing. Electric shock sensations can result from different types of nerve damage, and the distinction matters for treatment. Here's what to document:
- Location: Where exactly do the shocks occur? Feet only? Feet and legs? Hands? Do they follow a nerve distribution (e.g., traveling up the outside of the leg) or are they more diffuse?
- Pattern: Are they random throughout the day, or clustered at certain times (particularly at night or at rest)?
- Duration: How long does each shock last? True lancinating pain typically lasts milliseconds to a few seconds. Longer-lasting electric-type sensations might indicate something different.
- Triggers: Do they happen with movement? With cold? When you rest after activity?
- Frequency: How often per day or per week?
- Severity on a 0-10 scale: This helps track whether treatments are working.
A pain diary — even a simple notes app entry each time a significant episode occurs — can be invaluable. Patterns that aren't obvious in the moment become clear when you look at a week's worth of entries.
Medical Treatments for Electric Shock Sensations
The good news is that the same medications used to treat neuropathic pain generally work for electric shock sensations, and there are several options your doctor might consider.

Treatment Approach for Electric Shock Neuropathy Pain
Control blood sugar, correct B12 deficiency, treat autoimmune process — this is the most powerful long-term intervention.
Anticonvulsants: Gabapentin and Pregabalin
Gabapentin and pregabalin (Lyrica) work by blocking a specific calcium channel subunit in the nervous system (the alpha-2-delta subunit) that regulates the release of pain neurotransmitters. By dampening this signaling, they reduce the spontaneous nerve firing that causes electric shock sensations. Both drugs have solid evidence for neuropathic pain, and pregabalin is particularly effective for the intermittent, shock-like pain type.
Side effects include drowsiness, dizziness, and weight gain. Both medications require gradual dose titration to find the effective level while minimizing side effects. Don't judge efficacy until you've been on a therapeutic dose for at least 2-4 weeks.
SNRIs: Duloxetine and Venlafaxine
Duloxetine (Cymbalta) is FDA-approved specifically for diabetic peripheral neuropathy and works on both the serotonin and norepinephrine systems to enhance the body's own pain-suppressing pathways. It's particularly useful when anxiety or depression accompany neuropathy — which is common, given how much chronic pain affects mental health.
Tricyclic Antidepressants
Amitriptyline and nortriptyline, taken at low doses before bed, have decades of evidence for neuropathic pain. They work partly through sodium channel blockade (similar to the mechanism of nerve misfiring) and partly through enhancing descending pain inhibition. The bedtime timing is strategic — they help with nighttime pain and often improve sleep quality, which itself helps pain management.
Topical Treatments
For localized electric shock sensations — particularly those confined to the feet — topical treatments can provide relief without systemic side effects:
- Lidocaine patches (5%): Applied directly to painful areas, these provide local anesthesia by blocking sodium channels at the skin surface.
- Capsaicin cream or patches (8% prescription): Capsaicin depletes Substance P from nerve endings, reducing their ability to signal pain. The high-concentration patch (Qutenza) requires clinic application but can provide relief lasting months.
- Compounded creams: Some compounding pharmacies prepare topical formulations combining gabapentin, ketamine, and other agents specifically for neuropathic pain.
For Severe, Refractory Cases
When first-line treatments don't provide adequate relief, additional options include spinal cord stimulation (delivering mild electrical signals to modify pain processing at the spinal cord level), ketamine infusions, and — for specific conditions like CIDP — immunomodulatory treatments that address the underlying immune attack on nerves.
Non-Medical Approaches That Help
Medication isn't the only tool. A number of non-pharmacological approaches can meaningfully reduce the frequency and intensity of electric shock sensations.

Research Says
Pregabalin (Lyrica) has particular evidence for intermittent, lancinating (shock-like) neuropathic pain, in part because it reduces the abnormal calcium channel activity that drives spontaneous nerve firing. Multiple clinical trials support its use for this specific pain pattern.
Keep Moving (Gently)
Regular, gentle exercise improves blood flow to nerves, reduces inflammation, and — through mechanisms that aren't fully understood — seems to reduce neuropathic pain in many people. Walking, swimming, and cycling are particularly well-tolerated. The key is consistency and appropriate intensity: you're not trying to push through pain, but you are trying to maintain regular movement.
Warmth for Some, Cooling for Others
Many people find that warm foot soaks, heating pads, or warm water help reduce electric shock sensations by improving circulation and relaxing the surrounding tissues. Others find that cooling (cool water, gel packs) provides more relief by calming hypersensitive nerves. It's worth trying both — your response tells you something useful about what's driving your particular symptoms.
TENS (Transcutaneous Electrical Nerve Stimulation)
There's something almost counterintuitive about using gentle electrical stimulation to treat electrical shock sensations, but TENS can genuinely help. It works by activating large, non-pain nerve fibers that compete with and suppress the signals from damaged pain fibers — the “gate control” theory of pain. Many people find relief with regular TENS sessions, and the devices are available over the counter.
Sensory Grounding Techniques
When an electric shock hits, having something immediate to do helps break the cycle of alarm and anxiety that often amplifies the sensation. Some people find that gentle pressure (pressing hands on the affected area), cold or warm sensation (a washcloth, ice pack), or focused deep breathing helps them ride out the episode without the panic response that intensifies perceived pain.
Addressing the Underlying Cause
This is probably the most important point: treating the underlying cause of your neuropathy is the most powerful thing you can do for all your symptoms, including electric shock sensations. Tight blood sugar control in diabetic neuropathy can prevent further nerve damage and, over time, may reduce pain as nerves stabilize. Correcting B12 deficiency can allow nerves to begin repairing. Managing the immune response in autoimmune neuropathy can reduce ongoing damage. The stage of your neuropathy influences which approaches are most likely to help.
Living Day-to-Day with Electric Shock Sensations
Beyond treatments, there are practical adjustments that make daily life more manageable when you're dealing with unpredictable jolts of pain.

Common Triggers of Electric Shock Sensations
Nighttime & Rest
Create a predictable sleep environment. Since electric shocks often worsen at night, a bedtime routine that prepares your nervous system for rest can help. This might include a warm foot soak, gentle stretching, and a consistent medication timing so your evening dose is active at its peak when you're most vulnerable.
Wear soft, protective footwear. For shocks in the feet, even gentle pressure from clothing or bedding can act as a trigger. Non-binding socks, soft slippers, and seamless footwear reduce unnecessary stimulation. Some people find that wearing well-cushioned shoes even at home provides enough sensory normalization to reduce spontaneous firing.
Keep a trigger log. The patterns aren't always obvious until you record them. Even a week of noting when shocks occur and what preceded them often reveals actionable patterns — stress events, dietary choices, activity levels, weather changes.
Don't catastrophize — but do advocate. Electric shock sensations are frightening, especially when they first appear. Having them explained and named takes away some of their power. At the same time, if they're frequent and severe enough to disrupt your life, they deserve aggressive treatment attention. Don't accept “there's nothing more we can do” if your quality of life is significantly compromised. Combinations of treatments, different medication classes, and specialist referrals often open options that weren't apparent initially.
Reduce alcohol consumption. Alcohol is a known neurotoxin that can worsen peripheral neuropathy and amplify pain signaling. Even moderate consumption can intensify electric shock sensations in some people.
When to Seek Immediate Medical Attention
Most electric shock sensations in neuropathy, while deeply unpleasant, are not medical emergencies. However, certain situations warrant prompt evaluation:
- Sudden onset of new, severe electric sensations you've never experienced before, particularly if accompanied by weakness
- Electric sensations that travel up the spine when you bend your neck (Lhermitte's sign) — this warrants investigation of spinal cord involvement
- Electric sensations accompanied by new muscle weakness, bladder or bowel changes, or other neurological symptoms
- Rapid worsening of symptoms over days to weeks rather than months
- Electric sensations following any kind of trauma or fall
These patterns can indicate conditions beyond typical peripheral neuropathy — including spinal cord compression, Guillain-Barré syndrome, or other issues that need prompt attention.
The Emotional Weight of Unpredictable Pain
I want to acknowledge something that the medical literature often glosses over: the psychological impact of unpredictable, random pain. When you never know when the next jolt is coming, it creates a kind of hypervigilance — you're always waiting, always braced. This state of anticipatory anxiety can itself amplify pain perception and reduce quality of life in ways that go beyond the physical sensation itself.
You Are Not Alone
The anxiety that comes from not knowing when the next electric shock will hit is a real psychological burden — not an overreaction. Studies on chronic pain consistently show that unpredictability is more distressing than pain intensity. Talking to a therapist familiar with chronic illness, or connecting with a neuropathy community, can meaningfully reduce the anxiety load alongside your physical treatment plan.
This is one reason why psychological approaches — cognitive behavioral therapy, mindfulness, and acceptance-based therapies — are now considered legitimate parts of comprehensive neuropathy treatment. They don't eliminate the physical sensations, but they genuinely change the relationship between the sensations and your suffering.
If you're finding that fear of the next episode is governing your choices — avoiding activities, withdrawing from relationships, staying home because you don't want to have an episode in public — that's important information to share with your care team. The goal of treatment isn't just to reduce the shocks; it's to reclaim your life.
Frequently Asked Questions
Why do electric shock sensations happen in neuropathy?
Electric shock sensations occur because damaged nerve fibers begin firing spontaneously, generating false electrical signals that the brain interprets as intense, shock-like pain. This ectopic firing happens when nerve damage disrupts the ion channels and membrane stability that normally regulate nerve impulses.
Are electric shock sensations dangerous?
In most cases, electric shock sensations are a symptom rather than a danger in themselves. They indicate ongoing nerve irritation or damage, but the sensations themselves don't cause further harm. However, if they're accompanied by new weakness, changes in bladder or bowel function, or rapidly worsen, you should see a doctor promptly to rule out conditions that need urgent treatment.
What medications are most effective for electric shock pain in neuropathy?
Pregabalin and gabapentin (anticonvulsants) are often particularly effective for the intermittent, shock-like pain type because they reduce spontaneous nerve firing. Duloxetine, tricyclic antidepressants like amitriptyline, and topical treatments are also used. Most people require some trial and error to find the right medication or combination.
Why are electric shocks in neuropathy worse at night?
At night, there are fewer competing sensory inputs to distract from nerve misfiring, inflammation naturally increases, and the body's pain-modulating systems are less active. Blood flow patterns also change during rest, which can affect how much oxygen damaged nerves receive. Many people find their worst neuropathy symptoms, including electric shocks, occur between midnight and early morning.
Can electric shock sensations from neuropathy improve over time?
Yes, they can improve, particularly if the underlying cause is addressed. People with diabetic neuropathy who achieve excellent blood sugar control often report reduction in painful symptoms over time. Those with B12 deficiency often improve once deficiency is corrected. However, if nerve damage is severe, some degree of ongoing abnormal sensations may persist long-term.
Is there a connection between anxiety and electric shock sensations in neuropathy?
Yes, there is a real connection. Anxiety activates the sympathetic nervous system, which can amplify pain signals and lower the threshold for perceiving them. Additionally, anticipatory anxiety about the next shock can itself heighten nervous system activity. This is why stress management and psychological support are legitimate parts of comprehensive neuropathy treatment — they address a real physiological loop.
Should I be concerned if electric shocks start in a new location?
New locations for electric shocks can indicate that your neuropathy is progressing, affecting more nerve fibers or different areas. This warrants a conversation with your doctor about whether your underlying condition is being optimally managed and whether diagnostic updates are needed. Rapid progression, or new symptoms in atypical locations like the upper body or face, warrants prompt evaluation.
What is the difference between electric shocks from neuropathy versus from something else?
Neuropathic electric shocks are typically brief (milliseconds to seconds), occur in areas already affected by neuropathy symptoms, and often happen at rest or at night. They don't follow a consistent mechanical trigger like movement in a joint. Herniated discs or spinal stenosis can produce electric sensations too, but these typically follow nerve root distributions and are triggered by specific movements or positions. A neurological evaluation helps distinguish between these causes.


