
Every few months a new supplement gets passed around the support group like a hopeful little secret. Lately it has been quercetin — a plant flavonoid found in onions, apples, and capers that has shown some genuinely interesting results in nerve-pain research. I have been asked about it enough times that it deserves a careful, honest look.
I'm Janet Ellis, a community advocate who has lived with neuropathy for years — not a doctor or a researcher. What I can do is read the studies, sort the hype from what is actually known, and lay it out plainly. By the end of this you will know what the science says, what it does not, who tends to consider it, who probably should not, and how to talk to your own care team about it.
What Quercetin Actually Is
Quercetin is a flavonoid — a colorful plant compound that turns up in a long list of everyday foods. Onions (especially red and yellow), apples with the skin on, capers, kale, berries, broccoli, and black or green tea are the bigger sources. The body uses it as an antioxidant, and it has been studied for decades in the context of allergies, cardiovascular health, and inflammation. The neuropathy interest is newer, and it comes from a specific observation in lab studies: quercetin appears to calm several of the inflammatory and oxidative-stress pathways that damage nerves.
Quercetin is promising, not proven. The animal evidence on nerve inflammation is genuinely interesting; the human neuropathy trials are not yet there. Reasonable as a layered addition for the right person, with clinician oversight — not a foundation, and not a fast fix.
That is a meaningful thing to be calming, because chronic nerve pain is not just a wiring problem. It is a wiring problem held in place by ongoing inflammation in the nerves themselves and in the spinal cord pathways that carry their signals. A compound that genuinely interrupts that loop would matter. The question is whether quercetin does that in people, the way it appears to in lab animals.
What the Research Actually Shows
The honest answer is: the lab evidence is interesting, the human evidence for neuropathy specifically is thin. Here is what is actually published.
In animal models of diabetic neuropathy, quercetin has improved mechanical pain thresholds and nerve conduction velocity and reduced inflammatory markers (TNF-alpha, IL-1 beta) via the TLR4/MyD88/NF-kB pathway. A 2024 study extended this to axon-guidance factors and the Rho/ROCK pathway.
Human neuropathy trials remain limited — most current evidence is from rodent studies.
In animal models of diabetic peripheral neuropathy, quercetin has been shown to improve mechanical pain thresholds and nerve conduction velocity, and to reduce inflammatory markers like TNF-alpha and IL-1 beta in the sciatic nerve. One frequently cited 2021 study found it dampened the TLR4/MyD88/NF-kB inflammation signaling pathway in diabetic rats. A more recent 2024 paper extended that work, showing quercetin influenced axon-guidance factors and a separate pathway (Rho/ROCK) involved in how nerves regrow.
In chemotherapy models, quercetin has been studied against vincristine-induced nerve damage, where it appeared to protect nerves by suppressing the inflammatory and cell-death machinery and activating the body's own antioxidant defenses (the Nrf2 pathway).
What is missing — and this matters — are large, well-designed human trials. Most of what we have is rodent work. Smaller human studies of quercetin exist in adjacent areas (allergic rhinitis, prostatitis, exercise inflammation), but for neuropathy specifically, the human data is preliminary. So when you see headlines like “quercetin reverses nerve damage,” what they actually mean is “quercetin showed promising results in rats.” That is not nothing — most useful drugs started there — but it is not the same as “proven in people.”
Why Quercetin Is Harder to Use Than It Looks
There is a practical problem with quercetin that does not get talked about enough: it is famously badly absorbed. Ordinary quercetin powder in a capsule has very low bioavailability, meaning most of what you swallow never makes it into your bloodstream in a form your nerves could use. This is one of the real reasons trial results in people have been mixed even when lab results are striking.
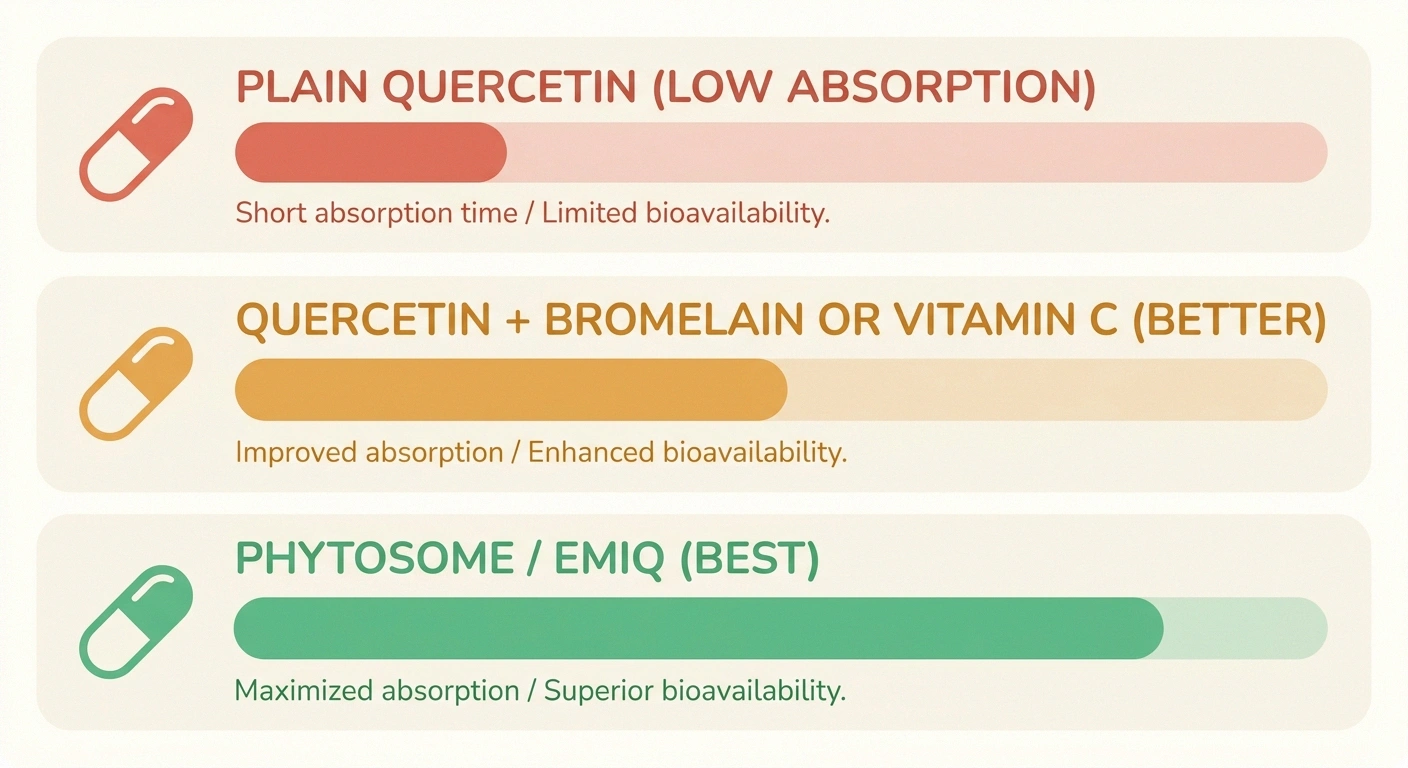
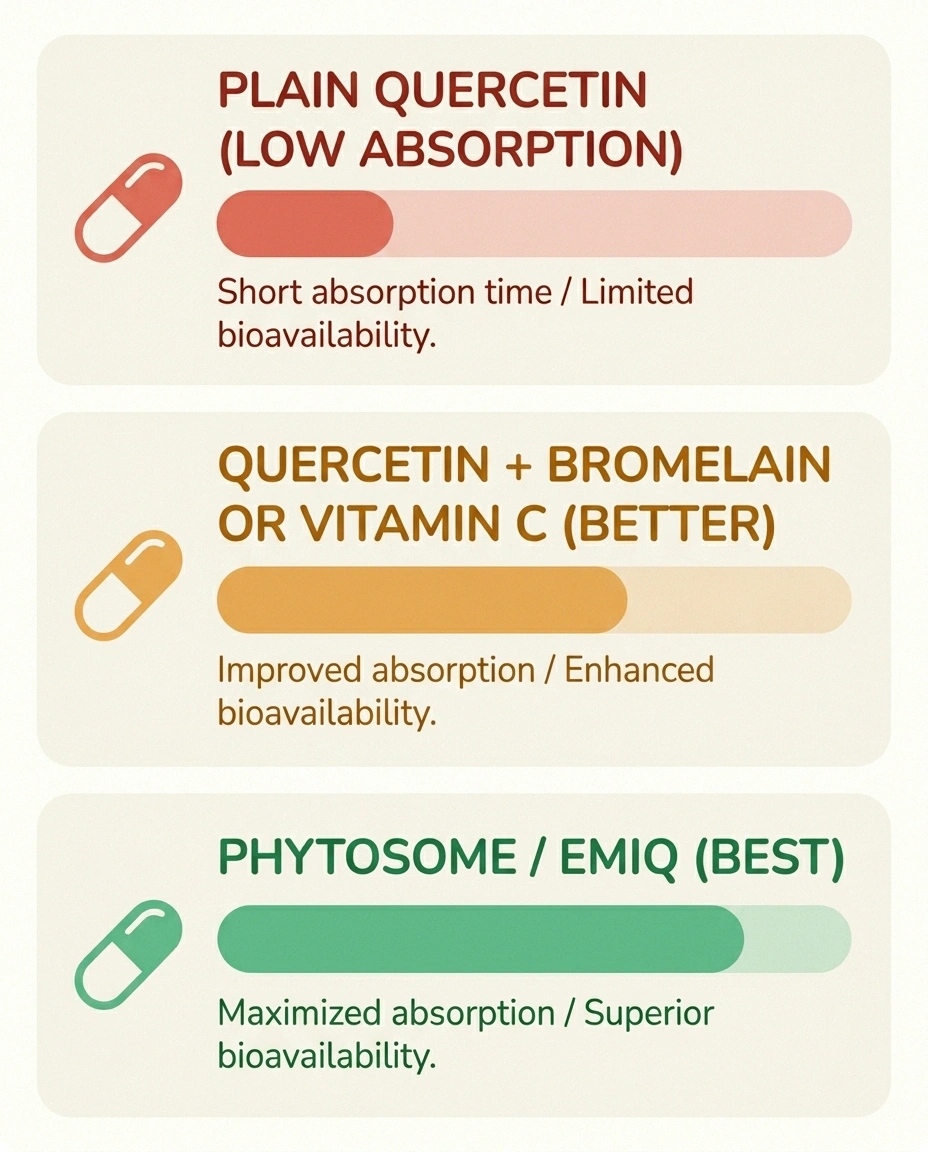
Quercetin Forms — Absorption at a Glance
Manufacturers have responded with several “enhanced” forms — quercetin phytosome (combined with a fat-soluble carrier), enzymatically modified quercetin (EMIQ), and quercetin combined with bromelain (an enzyme that may aid absorption). These forms appear to reach the bloodstream in meaningfully higher amounts. They also cost more, and the labels on enhanced products vary wildly in quality, so the brand and the form matter more than the dose number on the front of the bottle.
Realistic Dosing — and the Honest Caveat About It
Doses used in research and recommended by integrative practitioners generally fall in the range of 500 to 1,000 milligrams per day, often divided into two doses with food. Some protocols go higher; some pair quercetin with bromelain or with vitamin C, which may further support absorption. None of these numbers come from a definitive neuropathy trial — they come from related research and clinical experience.
What that means in practice is that “the right dose for nerve pain” is not really known. If you and your clinician decide to try it, start low, go slow, and give it real time. Like most supplements that work on inflammation rather than blocking pain signals directly, the realistic window for noticing anything is eight to twelve weeks, not days. Anyone selling you faster results is selling.
The Drug Interactions Nobody Mentions

This is the section I most wish someone had handed me earlier. Quercetin is not a quiet supplement. It interacts with several common medications, sometimes in ways that matter.
If you take blood thinners, fluoroquinolone antibiotics, cyclosporine, or any chemotherapy drug — clear quercetin with the prescriber before the first capsule. Quercetin is biologically active, which is exactly what makes it interesting and exactly why it interacts with other medications.
- Blood thinners. Quercetin can mildly inhibit platelets and may add to the effect of warfarin or other anticoagulants. If you are on any blood thinner, this needs a real conversation with the prescriber, not a guess.
- Fluoroquinolone antibiotics (ciprofloxacin, levofloxacin). Quercetin can compete with these antibiotics for the same cellular targets and theoretically reduce their effectiveness. If you have ever had a reaction to a fluoroquinolone — itself sometimes a cause of neuropathy — this is another reason to involve a clinician.
- Cyclosporine and certain other transplant or immune-modulating drugs. Quercetin can change how the liver processes them. If you take anything in this category, talk to your specialist before adding it.
- Some chemotherapy drugs. Quercetin's effects on cancer cells are an active research area and are not simple. If you are in active cancer treatment, do not add quercetin (or any antioxidant) without your oncology team's specific blessing.
None of this means quercetin is dangerous. It means it is biologically active, which is the same property that makes it interesting in the first place. Biologically active means “talk to whoever prescribes your other medications.”
Who Should Probably Skip It
A few groups should pause before adding quercetin at supplemental doses.
- People with significant kidney disease — high doses have raised concerns in animal studies, and the human safety margin in compromised kidneys is not well established.
- People who are pregnant or breastfeeding — there is not enough safety data, full stop.
- Anyone in active cancer treatment — for the reasons above.
- Anyone on the medications above without a clinician's review.
For most other adults, occasional dietary quercetin from foods is unquestionably safe (you have been eating it your whole life). It is the concentrated-supplement question that needs care.
The Food-First Option

Before reaching for a capsule, it is worth knowing that the largest concentrations of quercetin in everyday foods are in red and yellow onions (especially the outer layers), capers, apples with the skin on, kale, and elderberries. None of these are going to deliver the gram-level doses studied in research, but they come bundled with fiber, other flavonoids, and the broader anti-inflammatory benefits of a plant-forward eating pattern.
Where Quercetin Lives in Everyday Food
I am not anti-supplement — I take a few myself, with my doctor's input — but I am increasingly convinced that for chronic, inflammation-tinged conditions like neuropathy, the eating pattern around the supplements does more work than the supplements themselves. If your weekly meals already include onions, apples, leafy greens, and a few berries, you are doing more for the underlying biology than most pills will. We dig deeper into that thinking in our guide to the best neuropathy diet.
How Quercetin Fits Alongside the Better-Studied Supplements

If you are going to spend money on a nerve-supportive supplement, quercetin is probably not the first one I would suggest at the current state of evidence. The supplements with the strongest neuropathy-specific human research — alpha-lipoic acid for diabetic neuropathy and acetyl-L-carnitine in non-chemotherapy contexts — sit higher on the priority list. Curcumin from turmeric shares quercetin's broad anti-inflammatory profile and has more accumulated study time in people.
That does not make quercetin pointless. It makes it a reasonable third- or fourth-line addition for someone who has already tried the better-supported options, talked to their clinician, and wants to layer one more anti-inflammatory tool. It is not a foundation — it is, possibly, a finishing layer.
How to Talk to Your Clinician About It
A short, specific script tends to land better than a vague “what do you think of quercetin.” Try something like this:
Three Questions to Bring to Your Appointment
- “I have been reading about quercetin for nerve inflammation. I am taking [your current medications]. Is there any reason it would be a problem with what I am on?”
- “If it is safe to try, what form do you prefer — phytosome, EMIQ, or plain — and is there a starting dose you would suggest?”
- “How long should I give it before deciding whether it is helping, and what should I watch for that would tell me to stop?”
Three questions, written down, asked at an existing appointment. That is the entire ask. If your clinician is dismissive without a reason, it is fair to ask for the reason — but it is equally fair for them to say “I would rather you optimize the better-studied options first,” and that is a legitimate answer.
The Honest Bottom Line
Quercetin is a real flavonoid with a real anti-inflammatory profile and real, if early, lab evidence in neuropathy models. It is not snake oil. It is also not a proven treatment. It is poorly absorbed in its basic form, interacts with several common medications, and has not yet been tested in the kind of large human trials that would let anyone say with confidence “this works.”
For most people with neuropathy, the right place to start is somewhere else — the eating pattern, the better-supported supplements, the things your clinician already recommends. Quercetin can be a reasonable add-on later for the right person, with the right form, at the right dose, alongside a conversation with whoever prescribes everything else. Promising is not the same as proven, but for an option with relatively low downside in healthy people, that may be enough to consider.
Frequently Asked Questions
Is quercetin proven to treat neuropathy?
No. The lab evidence in animal models is genuinely promising — quercetin reduces inflammation in nerve tissue and has improved nerve function in diabetic and chemotherapy-induced models. But the human trials specific to neuropathy are not yet there. Calling it “proven” overstates what is known. Calling it “promising and reasonable for some people with clinician oversight” is closer to the truth.
How much quercetin should I take for nerve pain?
Common doses in research and integrative practice range from 500 to 1,000 milligrams per day, often divided into two doses with food. These numbers are extrapolated from related research, not from a definitive neuropathy trial. If you and your clinician decide to try it, start at the lower end and give it eight to twelve weeks before judging.
Which form of quercetin is best absorbed?
Plain quercetin powder is poorly absorbed. Enhanced forms — phytosome (combined with a fat-soluble carrier), enzymatically modified quercetin (EMIQ), or quercetin combined with bromelain — reach the bloodstream in higher amounts. Brand quality varies a lot in this category, so the form and the brand matter more than the milligram number on the front of the bottle.
Can I get enough quercetin from food?
Not at the gram-level doses used in research, but dietary quercetin from onions, apples with the skin, capers, kale, berries, and tea is unquestionably safe and contributes to the broader anti-inflammatory effect of a plant-forward eating pattern. For most people, the food version is a sensible foundation regardless of whether a supplement is added on top.
Does quercetin interact with other medications?
Yes — more than its mild reputation suggests. It can add to the effect of blood thinners like warfarin, reduce the effectiveness of fluoroquinolone antibiotics, change how the body processes cyclosporine and similar drugs, and may have unpredictable interactions with chemotherapy. Anyone on prescription medication should clear it with the prescriber before starting.
Who should not take quercetin supplements?
People with significant kidney disease, those who are pregnant or breastfeeding, anyone in active cancer treatment, and anyone on the interacting medications above without a clinician's review. For most other adults, supplemental quercetin appears to be well tolerated, but the safety conversation belongs with the clinician who knows the rest of your medication list.
How long does quercetin take to work for nerve pain?
If it helps, the realistic window is eight to twelve weeks of consistent use — not days. Quercetin works by gradually dampening inflammation, not by blocking pain signals like a medication. Anyone selling faster results is selling. Give it a fair trial and reassess with your clinician.
Should I take quercetin or alpha-lipoic acid?
If you are going to choose one and your neuropathy is diabetic in origin, alpha-lipoic acid has the stronger human evidence and would generally be the first pick. Quercetin sits better as a layered addition for someone who has already optimized the better-studied options.


