
I want to talk about berberine the way I wish someone had talked to me when I first found it on a supplement shelf next to the magnesium and the alpha-lipoic acid. Because here's what nobody told me at the time: berberine has a genuinely interesting story for nerve health, but the part the bottle wants you to believe and the part the studies actually show are two different conversations.
If you've been searching “berberine for neuropathy,” you've probably seen claims that range from cautious to wildly enthusiastic. Some sites treat it like a miracle. Others lump it in with snake oil. Both are wrong. The truth sits in between, and once you understand the difference between direct evidence (does berberine help nerve pain in humans?) and indirect evidence (does berberine help the things that cause nerve pain?), you can decide whether it belongs in your toolkit — and whether it's safe to put there given everything else you're already taking.
That's what we're going to do today. The honest version.
What Berberine Actually Is
Berberine is a bright yellow plant compound — an alkaloid — extracted mostly from Berberis species (barberry, Oregon grape) and Chinese goldthread (Coptis chinensis). Traditional Chinese medicine has used the root and bark for centuries, originally for digestive complaints and infections. The yellow color is so vivid it was used as a dye long before anyone studied its biochemistry.
Berberine is a plant-derived AMPK activator with the same metabolic lever as metformin. The supplement aisle sells it as a nerve-pain fix; the studies sell it as a blood-sugar helper. Both can be true — but only one is supported by human trials.
What put berberine on the modern supplement map wasn't its history, though. It was a discovery in the 2000s that berberine activates an enzyme called AMP-activated protein kinase, or AMPK. AMPK is the same metabolic switch that metformin activates — the one that helps cells become more sensitive to insulin and that nudges blood sugar down. Once researchers realized berberine and metformin were tugging on the same lever, the floodgates opened. Studies poured out. Most of them were about diabetes and cholesterol, not nerves. But a smaller branch of that research started asking a different question: if berberine helps the metabolic problems that cause diabetic neuropathy, can it also help the nerve damage itself?
That question turned out to have a more complicated answer than anyone expected.
The Two Evidence Buckets You Need to Separate
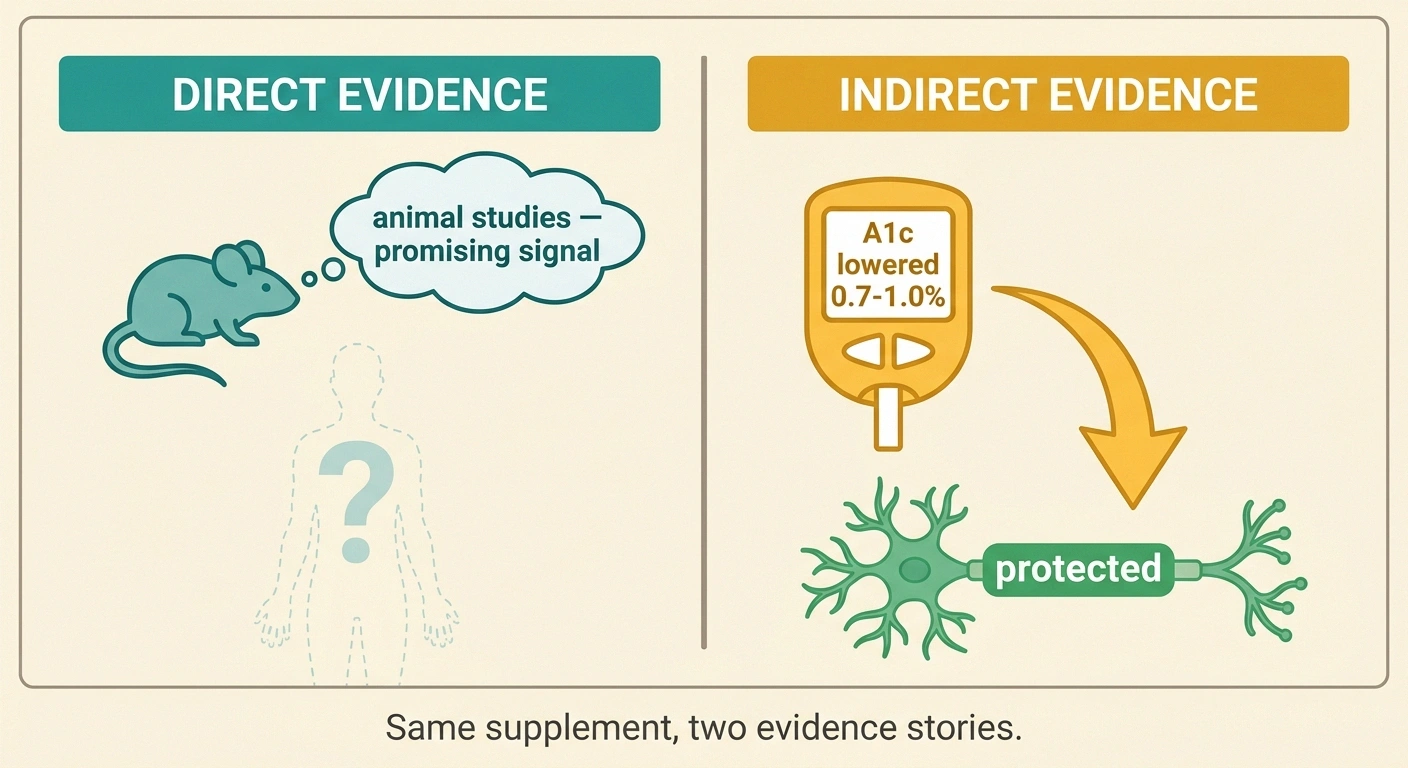
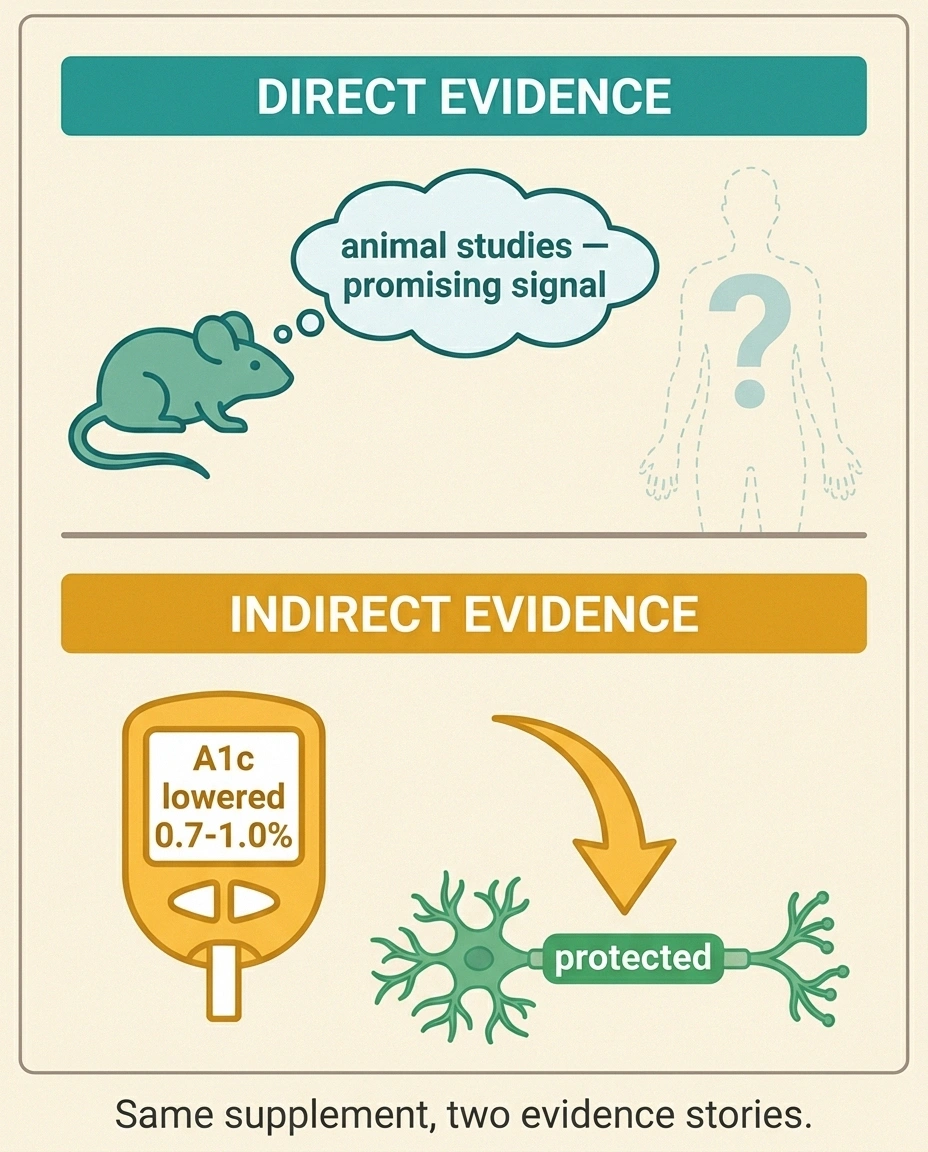
Whenever I evaluate a supplement for my own use or for the support group, I split the evidence into two buckets. Direct evidence means human studies that measured the thing I care about — in this case, nerve pain, numbness, or nerve function. Indirect evidence means studies that measured something upstream that we already know affects the thing I care about.
for berberine as a nerve treatment
(the indirect nerve benefit)
Both buckets matter. But you have to know which one a claim is drawing from before you decide how much weight to give it.
The Direct Evidence (Mostly Animal)
Here's the part that has me cautiously curious. In laboratory rats with diabetic neuropathy, berberine at moderate doses meaningfully reduced pain behaviors, hyperalgesia (exaggerated pain response), and even improved sensory nerve conduction velocity — the speed at which nerves carry signals. That's a real result, repeated by multiple research groups. The mechanism appears to involve several pathways at once: berberine quiets a key inflammation signal called TNF-α, modulates a pain channel called TRPV1 (the same channel that capsaicin acts on), and engages the body's own opioid receptors in animal models. There's similar evidence in rats with chemotherapy-induced neuropathy from cisplatin.
Here's what's missing. As of this writing in 2026, I cannot find a completed randomized controlled trial in humans that tested berberine specifically for neuropathy and measured nerve-related endpoints like pain scores, nerve conduction, or small-fiber density. Not one. The supplement is everywhere, the animal data is genuinely interesting, and yet the human neuropathy trial that would settle the question hasn't been done — or at least hasn't been published.
This is the gap between a real signal and a proven treatment. Animals are not people. Doses scale strangely. And rat hyperalgesia tests are useful but they're not the same as a 65-year-old in Maplewood asking whether her feet are going to stop burning at 2 a.m.
Anyone telling you berberine is “proven for neuropathy” is, at best, citing rats. At worst, citing nothing at all.
The Indirect Evidence (Much Stronger)
And yet — here's the twist — the indirect evidence for berberine is genuinely solid. Multiple human meta-analyses now show that berberine, at typical supplement doses, lowers hemoglobin A1c by somewhere between 0.7 and 1.0 percentage points in people with type 2 diabetes. That's in the same neighborhood as metformin in head-to-head studies. Berberine also reliably lowers LDL cholesterol and triglycerides, often by meaningful margins.
Why does that matter for your nerves? Because the single biggest driver of progressive nerve damage in the largest neuropathy population — people with diabetes or prediabetes — is sustained high blood sugar. Anything that brings that number down protects the nerves you still have. The same logic applies to lifestyle changes, to weight loss, to the right medications. It's why doctors say “tight glycemic control” until you're sick of hearing it. The control IS the nerve treatment, indirectly.
So when a neuropathy patient with elevated A1c takes berberine and feels their feet improve over six months, what likely helped wasn't berberine flipping a magical nerve switch. It was the upstream metabolic work — and that's still meaningful. It just changes the conversation. Berberine doesn't replace nerve treatment. It might support the metabolic conditions that nerves need to heal.
This is the framing I wish more supplement sites would use. Berberine sits in the same conceptual space as tight blood sugar control or weight loss — an upstream intervention with downstream nerve benefits, not a nerve drug.
How Berberine Works in the Body
If you like understanding the mechanism, here's the short tour. If you don't, you can skip to the next section without missing anything practical.

Berberine activates the same AMPK metabolic switch as metformin and additionally calms TNF-α inflammation and TRPV1 pain channels in animal models — three biochemically reasonable mechanisms running simultaneously. Whether they translate into clinical nerve benefit in humans is the open question.
Berberine's main lever is that AMPK activation I mentioned. AMPK is a kind of cellular “low fuel” sensor. When AMPK turns on, cells stop storing energy and start using it — they pull glucose out of the bloodstream more efficiently, they burn fatty acids, they slow down inflammatory signaling. That's why berberine looks like a metabolic helper: it tilts cells toward the same fuel-burning state that exercise produces.
Beyond that, berberine appears to do several other useful things. It calms down the inflammatory chemicals (cytokines like TNF-α and IL-6) that climb when blood sugar is chronically high. It reduces oxidative stress, the cellular rust that damages nerve fibers in diabetic neuropathy. And it appears to interact with pain channels and pain receptors — at least in animals — in ways that could plausibly affect how the nervous system processes signals.
The honest summary: berberine is doing several biochemically reasonable things at once. Whether those things add up to clinical benefit in a real person with neuropathy is the question we don't yet have a human answer for.
The Bioavailability Problem Nobody Mentions
Now we have to talk about the asterisk on every berberine bottle: the absorption is terrible. Plain berberine has a bioavailability of about 5 percent. That means if you swallow 500 mg, only about 25 mg actually reaches your bloodstream. The rest gets metabolized in the gut and liver or simply passes through. That's why berberine has to be taken in divided doses, often three times a day with food, just to keep blood levels measurable.
Some newer formulations try to fix this. Dihydroberberine (DHB) is a metabolic precursor that the gut converts to berberine, and it has roughly five times the bioavailability of plain berberine. Liposomal berberine wraps the molecule in fat bubbles to slip past first-pass metabolism. Berberine HCl with milk thistle or silymarin is another combo aimed at improving absorption. These products cost more — sometimes substantially more — and the studies comparing them to plain berberine for clinical outcomes are sparse.
For most people starting out, plain berberine HCl at the standard split dose is fine. If you don't see metabolic improvement after 8-12 weeks, that's when I'd talk to your pharmacist about whether a higher-bioavailability form is worth the cost.
The Drug Interaction Section You Should Not Skip
I'm going to be a little forceful here because this is the part that worries me most when I see neuropathy patients reach for berberine without checking with anyone.

Bring the berberine bottle to your pharmacist before you start — especially if you take any of these:
- Statins (atorvastatin, simvastatin) — rhabdomyolysis risk reported
- Duloxetine, tramadol, codeine — CYP2D6 interaction raises blood levels
- Cyclosporine, tacrolimus — transplant medications
- Digoxin, warfarin — heart and blood-thinner safety
- Metformin, insulin, sulfonylureas — additive hypoglycemia risk
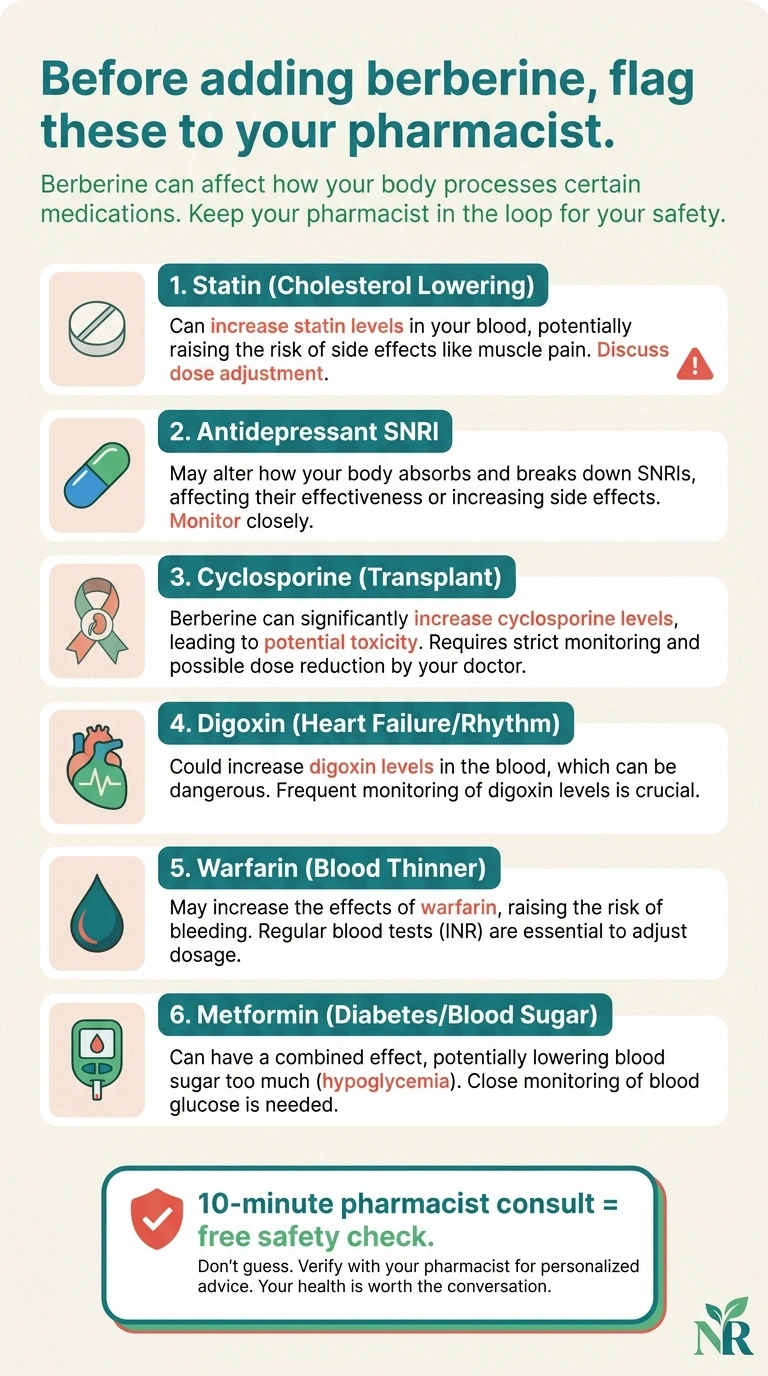
Berberine inhibits several of the same liver enzymes that metabolize many common medications. That means it can raise blood levels of those medications, sometimes dangerously. The big ones to know about:
- Statins (atorvastatin, simvastatin, lovastatin). Higher statin levels can cause muscle breakdown (rhabdomyolysis). This combination shows up in published case reports.
- Duloxetine (Cymbalta), nortriptyline, amitriptyline, tramadol, codeine. Berberine inhibits the CYP2D6 enzyme that processes these. If you take duloxetine for neuropathy, adding berberine could raise its level — and the side effects.
- Cyclosporine, tacrolimus (transplant patients). Berberine can push these into toxic ranges.
- Digoxin (heart). Berberine interferes with the transporter that clears digoxin, raising levels.
- Warfarin and other blood thinners. Berberine can amplify bleeding risk.
- Other diabetes medications (metformin, sulfonylureas, insulin). Additive blood sugar lowering can cause hypoglycemia. This is fixable but only if everyone knows it's happening.
- Antibiotics and antifungals processed through CYP3A4 (some macrolides, azoles).
This is not a complete list. It's the highlight reel. If you take a daily medication for anything — heart, mood, pain, thyroid, transplant, infection — please, please bring the berberine bottle to your pharmacist before you start. Pharmacists love this question. They will not roll their eyes. They will pull up your full med list and check it in the way that prescribers sometimes don't have time for. It's the single most underused free safety check in the American healthcare system.
Who Should Not Take Berberine At All
A few absolutes worth knowing:
- Pregnancy and breastfeeding. Berberine crosses the placenta and can displace bilirubin from albumin in newborns, which is a serious problem for jaundice. Don't take it.
- Newborns and infants. Same reason. Berberine has historically been linked to kernicterus risk in jaundiced babies. It is not a children's supplement.
- Before surgery. Stop berberine at least two weeks before any planned surgery because of the blood sugar effect and the bleeding-risk combination with anticoagulants.
- If you have low blood pressure or take blood pressure medications. Berberine can lower blood pressure further; if you're already on the edge of feeling dizzy when you stand, this could push you over.
- Active GI conditions (IBD flare, severe IBS, recent gut surgery). Berberine reliably stirs up the gut. Wait until you're stable.
How People Actually Take It
If you and your healthcare team decide berberine is reasonable to try for the metabolic angle, here's the typical playbook I see in the support group:

Bring your full medication list. This is the single most useful free safety review in healthcare.
A1c, fasting glucose, lipid panel. You need before-numbers to judge after-numbers.
Start at 500 mg once daily for a week. If tolerated, increase to 500 mg twice, then three times daily.
Burning, tingling, numbness scores 0–10. GI side effects. Blood pressure if you take cardiac meds.
A1c shift tells you whether the upstream benefit is happening. Decide to continue based on numbers, not hope.
- Dose: 500 mg three times daily with meals (1,500 mg/day total) is the most-studied dose. Some people start at 500 mg once daily for a week to test for GI tolerance, then ramp up.
- With food. Always. Empty stomach amplifies GI side effects.
- Tracking: Keep a symptom diary for the first 8-12 weeks. Note GI changes, energy, blood sugar readings if you have a meter, and your neuropathy symptoms on a 0-10 scale. This is how you know whether anything is actually happening.
- Lab work: If you're using berberine for metabolic effect, getting an A1c at 12 weeks tells you whether you're getting the upstream benefit. Without that number, you're guessing.
- Patience: Metabolic changes take 8-12 weeks to show up in A1c. If you expect immediate nerve relief, you'll be disappointed and stop too early.
Berberine vs. Other Supplements People Ask About
One question I hear constantly: “Should I take berberine, or alpha-lipoic acid, or both?” Here's how I think about it:
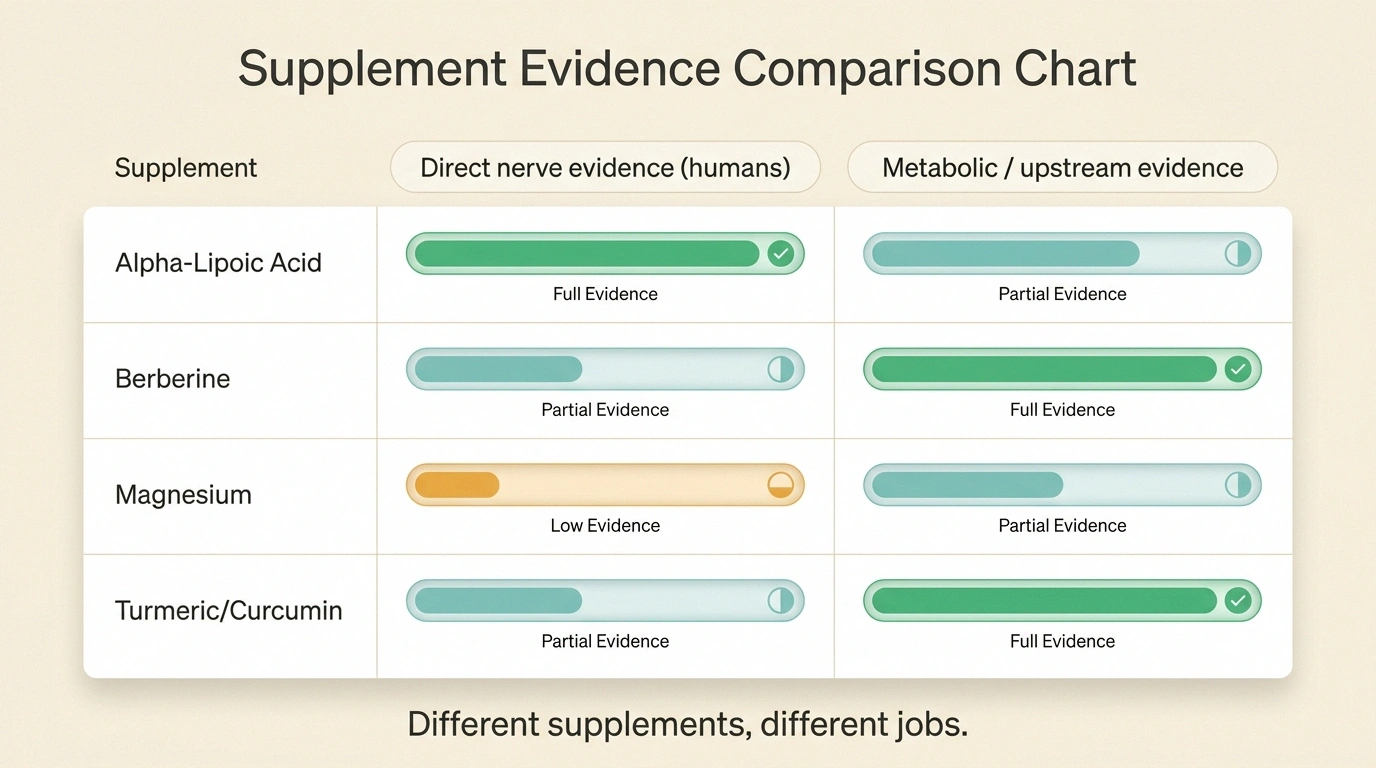
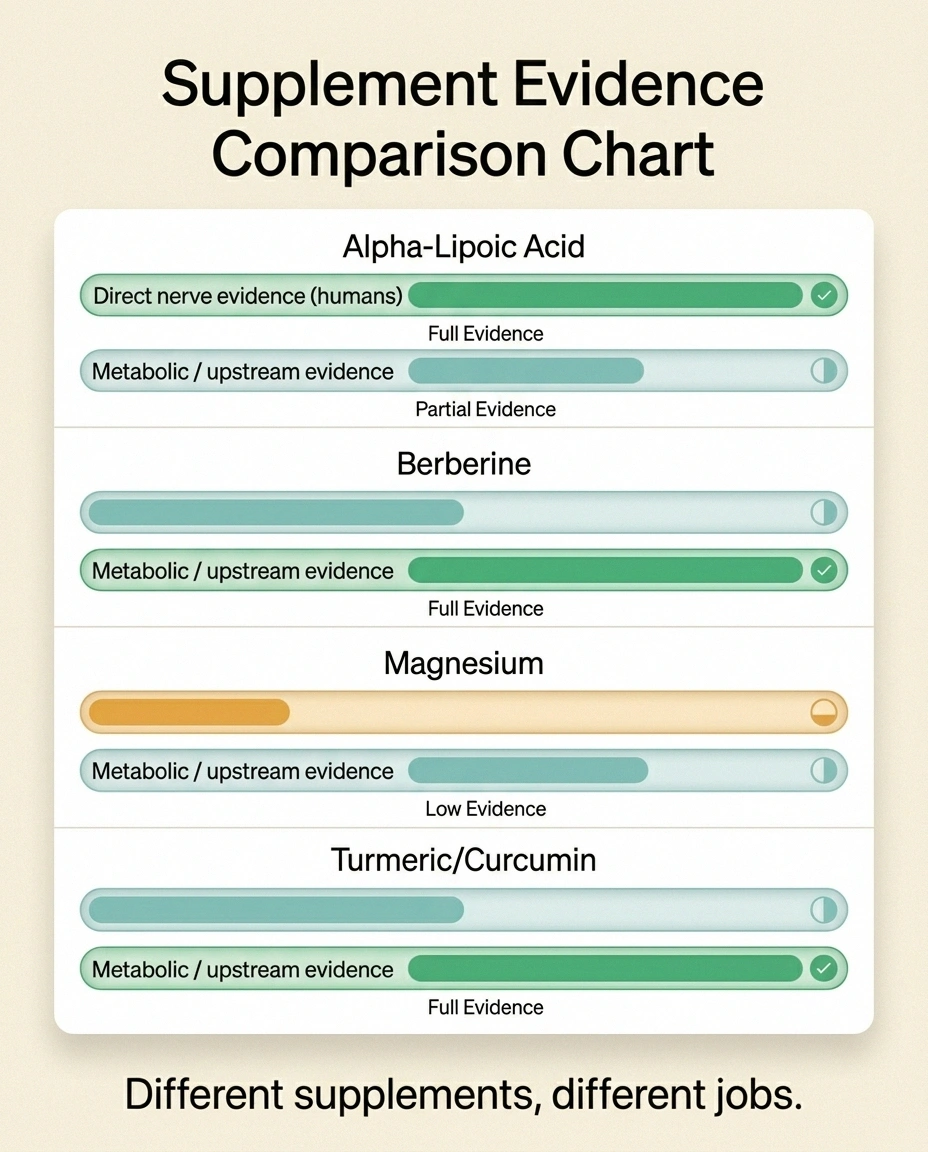
Alpha-lipoic acid has the most direct human evidence for diabetic neuropathy symptoms — meaningful pain reduction in multiple randomized trials, especially the European IV studies and the oral ALADIN and SYDNEY trials. If you want a supplement with actual direct neuropathy data, ALA is the one to start with. Berberine isn't competing with ALA on direct nerve evidence — ALA wins.
Berberine wins on the metabolic axis. If your A1c is uncomfortably high and you're trying to bring it down without adding another prescription, berberine has real evidence there. So the honest answer to “ALA or berberine” is often: they do different jobs. ALA targets the nerves more directly. Berberine targets the metabolic environment that surrounds the nerves.
For comparison, magnesium is more about cramping and sleep than nerve regeneration. Turmeric and curcumin are anti-inflammatory like berberine but with weaker metabolic effects and even weaker direct-nerve evidence. The fuller picture lives in our neuropathy supplements guide.
None of these are replacements for the prescription medications your neurologist or primary care doctor has put you on. They sit alongside, not instead.
Realistic Expectations
Here's what I tell people who are considering berberine after they've weighed the interactions and gotten the green light from their pharmacist:

- Don't expect a dramatic change in burning, tingling, or numbness in the first month. The nerves don't work on that timeline.
- If your A1c drops by half a point or more over 12 weeks, that's a meaningful win — and that win will, over a longer arc, protect the nerves you still have.
- If you feel no metabolic change by 12 weeks (no A1c improvement, no fasting glucose change, no fewer post-meal crashes), berberine may not be the right tool for you.
- The supplements that get blamed for “not working” are often the ones being asked to do a job they don't do. Berberine is a metabolic tool with possible nerve-adjacent benefits. Judge it on that, not on whether your feet stopped hurting in two weeks.
- Any supplement you add should make the rest of your natural remedies plan stronger, not crowd it out. A 12-pill supplement stack isn't a treatment plan, it's an expense.
What I'd Do If I Were Starting Over
If I were sitting at my kitchen table tonight, brand new to all of this, with a fresh neuropathy diagnosis and a row of supplement bottles I'd been told to try, here's how I'd think about berberine specifically:
Berberine is a peripheral player in a neuropathy plan, not the centerpiece. Use it as a metabolic helper when blood sugar or cholesterol is the upstream problem you're trying to fix. Judge it on lab numbers at 12 weeks, not on whether your feet stopped hurting in two weeks.
First, I'd ask: do I have a metabolic problem I'm trying to fix? If my A1c is sitting at 7.5 percent, my LDL is 140, my triglycerides are pushing 200, and my doctor and I are circling the conversation about adding another medication — berberine is at least worth a discussion. Not as a nerve treatment, but as a metabolic helper that has plausible downstream nerve benefit.
Second, I'd ask: am I taking anything else that's going to interact? My pharmacist would be my first call. Not Google. Not the supplement store clerk. The pharmacist who has my whole med list pulled up on a screen and gets paid to flag things like CYP2D6 inhibition.
Third, I'd give it a real 12-week trial with proper tracking — A1c before and after, a symptom diary, blood pressure checks if I'm taking anything that affects blood pressure. Then I'd judge it on the numbers, not on hope.
And fourth, I'd make sure berberine wasn't crowding out the things with stronger direct evidence — alpha-lipoic acid for nerve symptoms, walking for circulation and balance, B12 if I had any reason to think I was low, and the prescription pain treatments my neurologist had picked. Berberine is a peripheral player, not a centerpiece. Treating it like a peripheral player is how it earns its place.
Neuropathy taught me to ask harder questions about everything that gets sold to people like us. Berberine deserves the same scrutiny — neither dismissed nor oversold. The animal data is interesting. The metabolic data is real. The human nerve data is missing. That's the honest picture. Now you can make your own call.
Frequently Asked Questions
Does berberine actually help neuropathy?
There is real evidence in animal studies that berberine reduces neuropathic pain behaviors and improves nerve conduction in diabetic and chemotherapy-induced rat models. There are no completed randomized human trials that tested berberine specifically for neuropathy as of 2026. The strongest argument for berberine in nerve health is indirect: it lowers blood sugar and cholesterol in humans, and those metabolic improvements protect nerves over time. Anyone promising direct neuropathy benefit in humans is going beyond what the published evidence shows.
How much berberine should I take for nerve pain?
The most-studied dose is 500 milligrams three times daily with meals, for a total of 1,500 milligrams a day. This dose was developed for blood sugar and cholesterol outcomes, not nerve outcomes specifically. Most people start lower for a week or two to test gastrointestinal tolerance, then ramp up. Always take with food and split the dose because berberine has very low bioavailability of about 5 percent. Talk to your pharmacist before starting if you take any prescription medication.
Can I take berberine with gabapentin or duloxetine?
Gabapentin and berberine have not been reported to have a direct major interaction, but the combination has not been thoroughly studied either. Duloxetine is processed by the CYP2D6 liver enzyme, which berberine inhibits, so adding berberine could theoretically raise duloxetine blood levels and increase side effects like nausea, dizziness, or drowsiness. Do not combine these without checking with your pharmacist or prescriber first. This is exactly the conversation a 10-minute pharmacist consult is built for.
Is berberine safe to take with metformin?
Berberine and metformin both lower blood sugar through overlapping pathways including AMPK activation. The combination is not dangerous in itself, but it can produce additive blood sugar lowering that may push you into hypoglycemia (low blood sugar) if your dose is not adjusted. People who combine them often need to reduce their metformin dose, monitor with a meter or continuous glucose monitor, and stay in close touch with their prescriber. Do not stack them quietly without telling your medical team.
What are the most common side effects of berberine?
The most common side effects are gastrointestinal: diarrhea, constipation, abdominal cramping, gas, and nausea. These affect roughly a third of people, especially during the first few weeks. Splitting the dose, taking it with food, and starting low usually helps. Less common but more serious risks include low blood sugar (especially when combined with diabetes medications), low blood pressure, and rare elevations in liver enzymes. Stop berberine and contact your doctor if you develop dark urine, yellowing of the skin, severe abdominal pain, or symptoms of low blood sugar like shakiness, sweating, or confusion.
How long until berberine works?
For blood sugar and cholesterol effects, meaningful changes typically show up after 8 to 12 weeks of consistent dosing. Hemoglobin A1c, which is a 3-month average of blood sugar, takes at least that long to shift in any direction. If you are taking berberine in hopes of nerve symptom improvement, you should expect even longer timelines because nerves recover slowly, and you may not see direct symptom change at all. A 12-week trial with before-and-after A1c testing is the most informative way to evaluate whether it is doing anything for you.
Can berberine reverse neuropathy?
Berberine cannot reverse nerve damage in the way the word “reverse” is sometimes used in marketing. What is more accurate to say: in people with high blood sugar, lowering blood sugar gives the body a better environment in which nerves can stabilize and, in some cases, regrow small fibers slowly over time. Berberine is one tool among many for that metabolic work. The structural recovery that follows belongs to good blood sugar control, time, B vitamins where there is a deficiency, and the prescription treatments your doctor recommends. Read more in our article on whether neuropathy can be reversed.
Should I take berberine or alpha-lipoic acid for neuropathy?
Alpha-lipoic acid has substantially more direct human evidence for reducing diabetic neuropathy symptoms, including pain, burning, and tingling. If your goal is symptom relief, alpha-lipoic acid is the better-supported choice. Berberine is better supported for metabolic outcomes (blood sugar, cholesterol) than for direct nerve symptoms. Many people use both if their pharmacist confirms no interactions with their prescription medications, since the two supplements target different parts of the problem. Neither replaces prescription neuropathy treatment.


