Suzetrigine (Journavx): The First New Non-Opioid Pain Drug for Neuropathy
For the first time in decades, there's a genuinely new approach to pain management — and it works in a way that's directly relevant to anyone living with neuropathy. Suzetrigine, sold under the brand name Journavx, was approved by the FDA in January 2025 as the first non-opioid medication for moderate-to-severe acute pain. But what's making waves in the neuropathy community isn't just its current approval — it's the clinical trials already underway testing whether it can treat chronic neuropathic pain.
Let me walk you through what this drug does, why it matters for neuropathy patients, and what the research shows so far.
What Is Suzetrigine and How Does It Work?
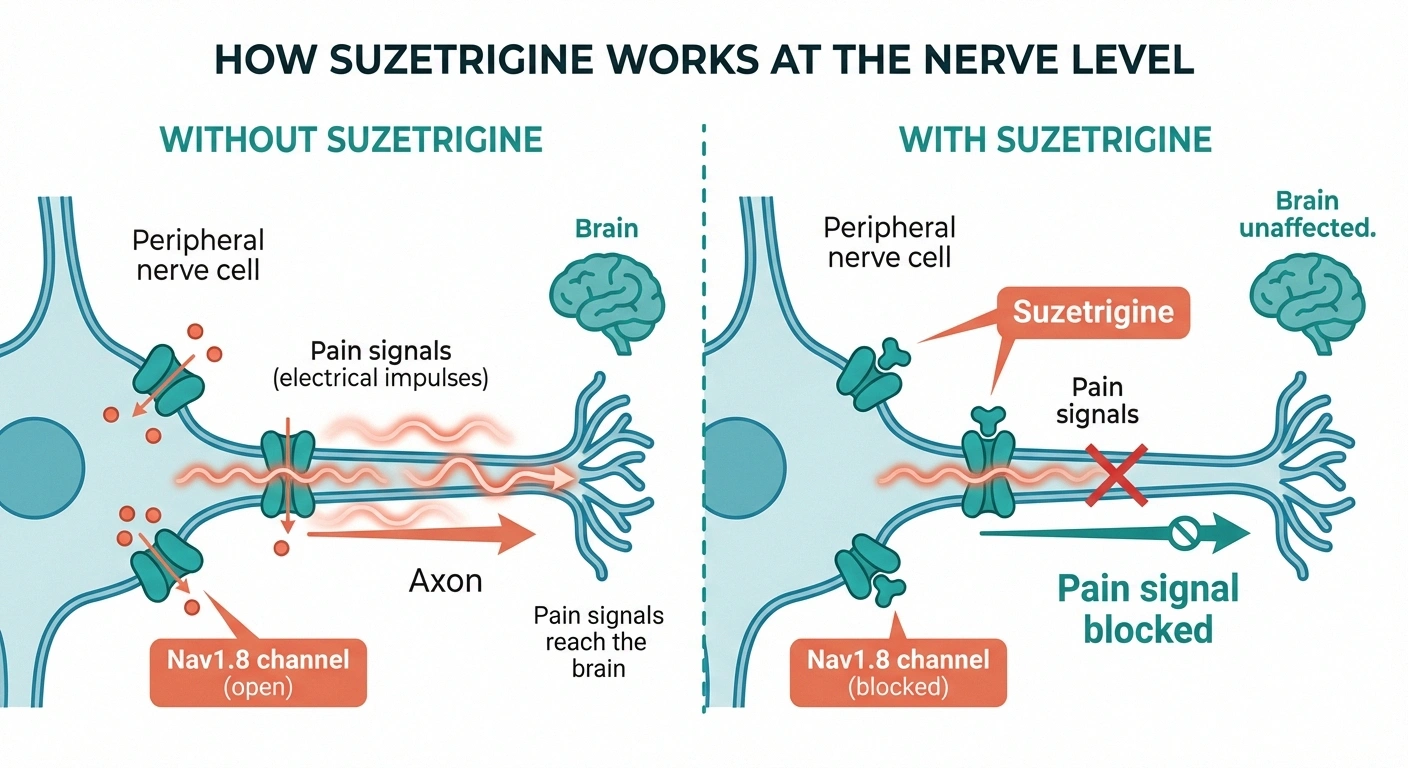
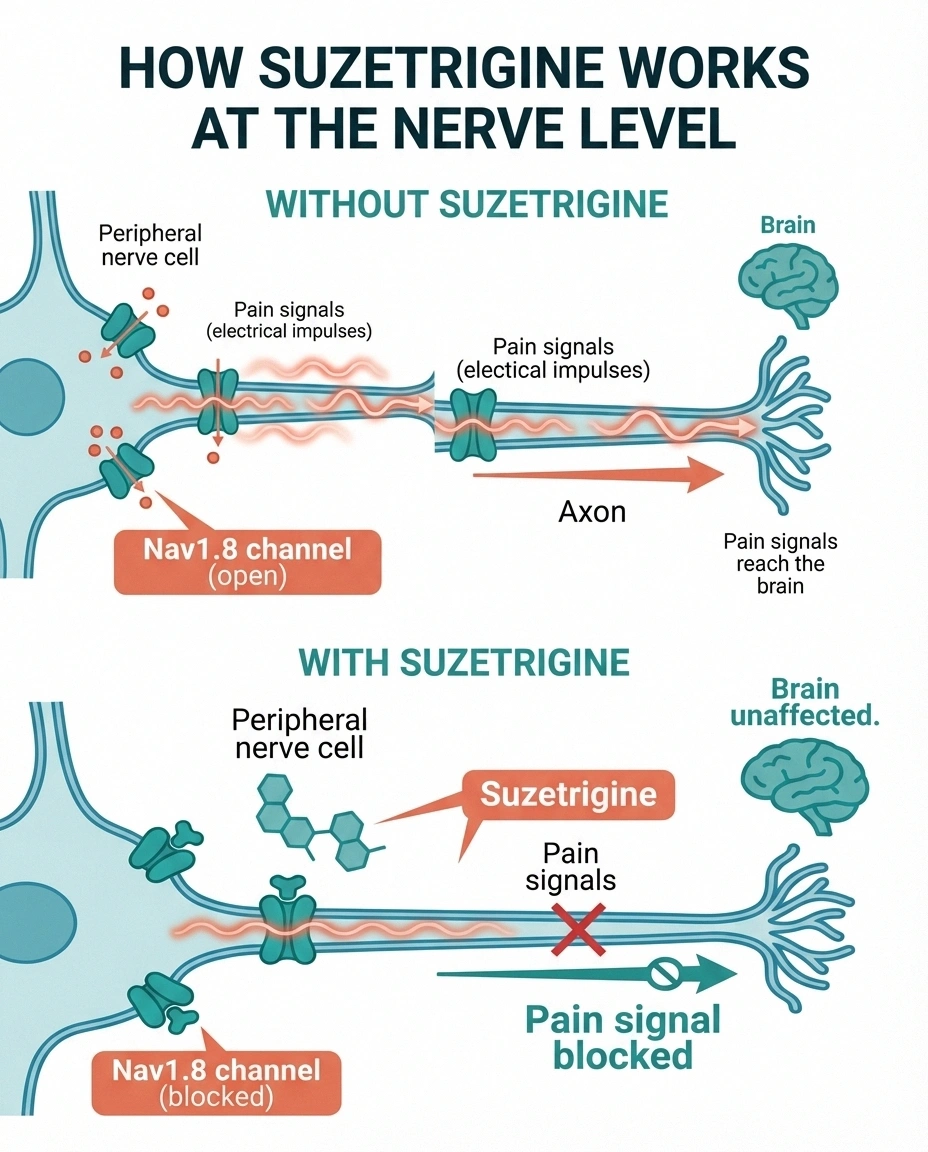
Suzetrigine is an oral, non-opioid painkiller developed by Vertex Pharmaceuticals. It works by selectively blocking a specific sodium channel called Nav1.8 — and understanding this mechanism is key to understanding why it matters for neuropathy.
When you feel pain, specialized nerve cells detect injury or damage and send electrical signals to your brain. These signals are generated by sodium channels — molecular gates in the nerve cell membrane that open and close to create electrical impulses. Different types of sodium channels serve different functions throughout the nervous system.
Nav1.8 is found almost exclusively in peripheral sensory neurons — the pain-sensing nerve cells in your skin, muscles, and organs. It's not present in the brain or central nervous system. This is what makes suzetrigine fundamentally different from opioids and most other painkillers: it blocks pain signals at the source, in the peripheral nerves, before they ever reach the brain.
Because suzetrigine doesn't act on the brain, it doesn't cause the euphoria, sedation, respiratory depression, or addiction potential that make opioids so dangerous. In clinical trials, the most common side effects were mild: itching, muscle spasms, and rash.
The Science Behind Nav1.8: Why It Matters for Neuropathy
The foundation for suzetrigine's development goes back more than 25 years to the work of Dr. Stephen Waxman at Yale School of Medicine. His research team discovered that Nav1.8 is essential for pain signaling in peripheral nerves but isn't needed for normal brain function. This insight made Nav1.8 an ideal drug target — block it, and you reduce pain without the cognitive and addictive effects of drugs that act on the brain.
For neuropathy patients specifically, Nav1.8 is particularly relevant because it plays a central role in the abnormal nerve signaling that causes neuropathic pain. In damaged nerves — whether from diabetes, chemotherapy, or other causes — sodium channels like Nav1.8 can become overactive, generating spontaneous pain signals even without any external stimulus. This is why neuropathy pain can feel like burning, stabbing, or electric shocks seemingly out of nowhere.
By selectively silencing Nav1.8, suzetrigine may be able to calm these misfiring nerves without shutting down normal sensation. That's the theory, and the early data suggests it's working.
Current FDA Approval: What Suzetrigine Can Do Now
As of its January 2025 approval, suzetrigine is indicated for moderate-to-severe acute pain in adults. “Acute” means short-term pain — typically from surgery, injuries, or trauma expected to last less than three months. The FDA's approval was based on two large clinical trials involving about 1,000 patients each:

- Abdominoplasty trial: Patients recovering from tummy tuck surgery — suzetrigine provided pain relief comparable to Vicodin (hydrocodone/acetaminophen) and significantly better than placebo
- Bunionectomy trial: Patients recovering from bunion removal surgery — similar results, with suzetrigine matching opioid-level pain relief without opioid side effects
The standard dose is 50mg tablets taken three times daily. Important practical details: the medication costs approximately $15.50 per pill (roughly $46.50/day), insurance coverage varies, and there are significant drug interactions to be aware of — patients should avoid the antibiotic erythromycin, the blood pressure medication verapamil, and grapefruit products.
The Neuropathy Trials: What the Data Shows So Far
The most exciting development for neuropathy patients isn't the current approval — it's the ongoing clinical trials testing suzetrigine for chronic neuropathic pain. Vertex Pharmaceuticals has multiple Phase III trials running for diabetic peripheral neuropathy and other chronic pain conditions.
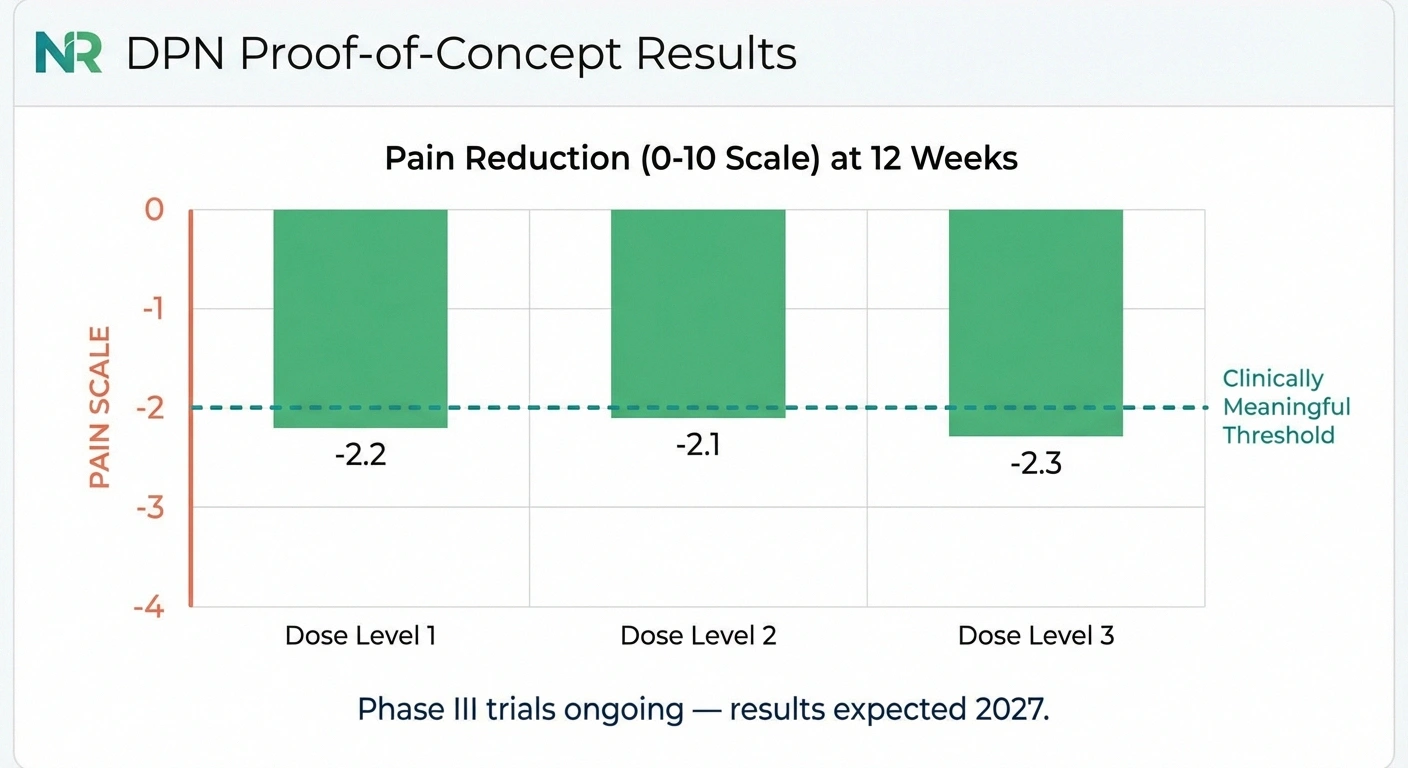
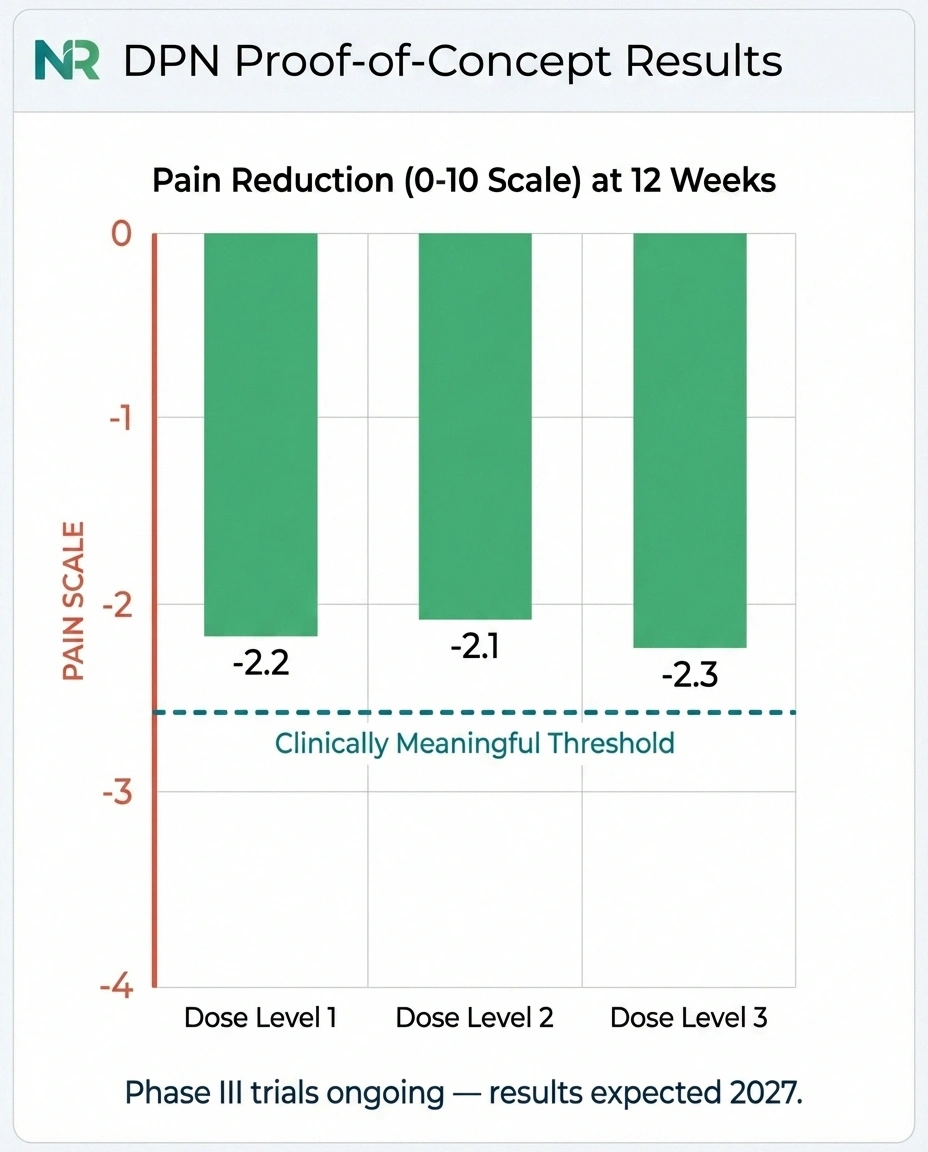
A proof-of-concept study presented at the American Academy of Neurology meeting in 2025 showed promising results for diabetic peripheral neuropathy:
- The study tested three dose levels of suzetrigine in patients with painful diabetic neuropathy
- All three doses met the primary endpoint — significant pain reduction at 12 weeks compared to baseline
- High-dose group: pain score reduction of -2.26 on a 0-10 scale (95% CI: -2.82 to -1.70, p<0.0001)
- Mid-dose group: -2.11 reduction (95% CI: -2.67 to -1.55, p<0.0001)
- Low-dose group: -2.18 reduction (95% CI: -2.94 to -1.41, p<0.0001)
To put these numbers in perspective: a 2-point reduction on a 10-point pain scale is considered clinically meaningful. If these results hold up in the larger Phase III trials, suzetrigine could become the first medication specifically designed to address the peripheral nerve mechanism of neuropathic pain, rather than dampening pain perception in the brain.
One important note from patient reports: in the Mayo Clinic Connect forums, a patient with idiopathic small fiber neuropathy who participated in a trial reported that suzetrigine provided a “wonderful week” with zero side effects — but pain returned when the medication was stopped. This suggests that suzetrigine manages pain rather than treating the underlying nerve damage, which aligns with its mechanism of action.
How Suzetrigine Compares to Current Neuropathy Medications
To understand why suzetrigine is generating so much interest, it helps to compare it with the current first-line medications for neuropathic pain:
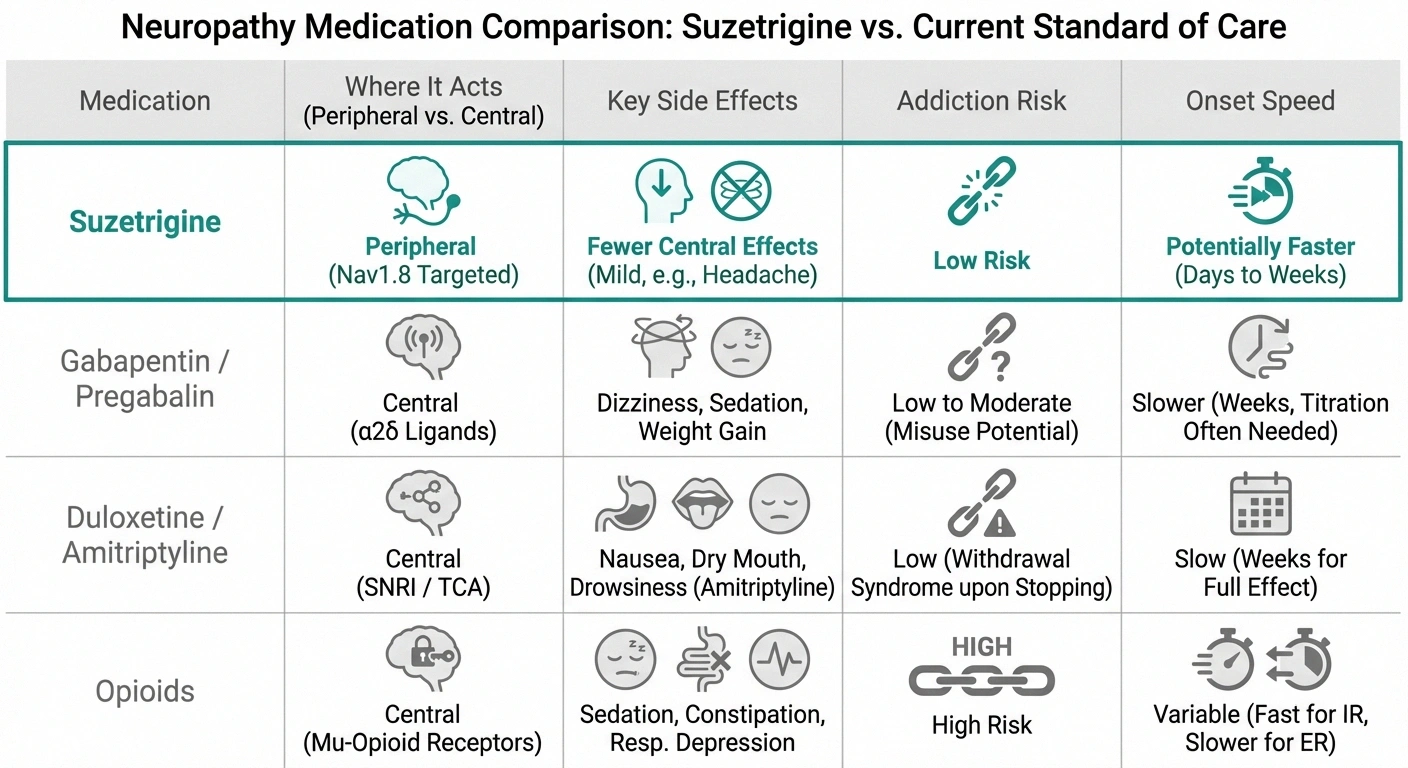
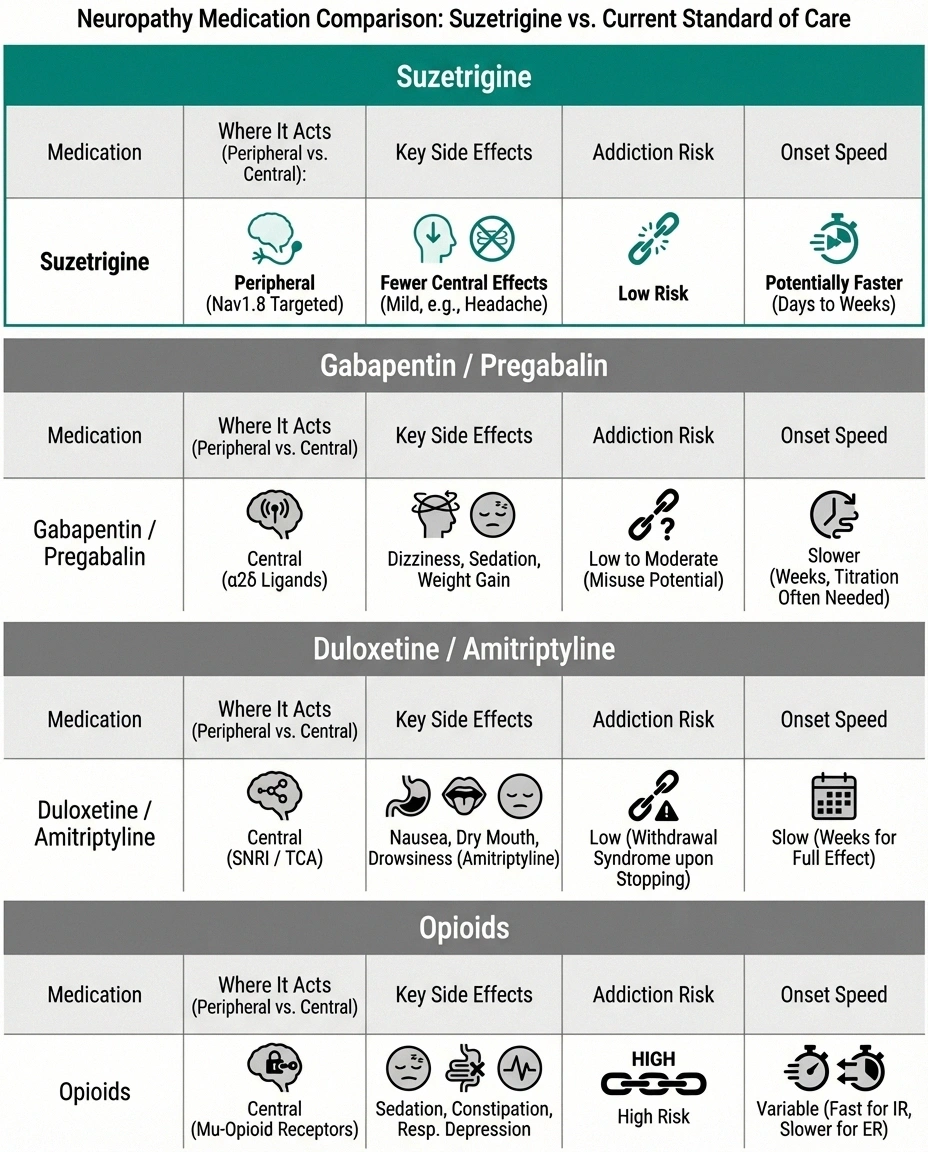
Gabapentin and pregabalin (Lyrica): These work by modifying calcium channel activity in the central nervous system. They're effective for many patients but cause drowsiness, dizziness, cognitive fog, and weight gain. They also require weeks of dose titration before reaching therapeutic levels.
Duloxetine (Cymbalta): An SNRI antidepressant that modulates pain signaling in the spinal cord. Effective but causes nausea, fatigue, and can be difficult to discontinue.
Amitriptyline: A tricyclic antidepressant used off-label. Effective for nerve pain but causes significant sedation, dry mouth, constipation, and cardiac concerns in older adults.
Opioids: Sometimes prescribed for severe neuropathic pain but carry addiction risk, tolerance development, and systemic side effects. The evidence for long-term opioid use in neuropathic pain is weak.
All of these medications work in the brain or spinal cord. Suzetrigine is the first to work at the actual site of nerve damage — the peripheral nervous system. If the neuropathy trials succeed, it would represent a fundamentally new approach to managing nerve pain.
Limitations and Open Questions
While the potential is real, important questions remain:
Does it work for chronic neuropathy long-term? The acute pain trials lasted days. The DPN proof-of-concept was 12 weeks. Neuropathy patients need pain management for months or years. Long-term safety and efficacy data are still being collected.
Which types of neuropathy will respond? The trials focus on diabetic peripheral neuropathy. Whether suzetrigine works equally well for chemotherapy-induced neuropathy, idiopathic neuropathy, or other types hasn't been established. Nav1.8 is involved in multiple neuropathy subtypes, so there's reason for cautious optimism — but the data needs to confirm it.
Cost and access: At $15.50 per pill, a daily regimen of suzetrigine would cost approximately $1,400 per month before insurance. For a chronic condition requiring long-term treatment, this is a significant barrier. Insurance coverage for the acute pain indication is still being established; coverage for a chronic neuropathy indication would need to be negotiated separately.
It manages pain, not the underlying damage. Suzetrigine blocks pain signals from damaged nerves; it doesn't repair the nerves themselves. Patients would still need to address the root cause of their neuropathy (blood sugar control, nutritional deficiencies, etc.) while using suzetrigine for symptom management.
What This Means for You Right Now
If you're living with neuropathic pain, here's the practical takeaway:

If you're managing with current medications: Don't change anything based on early trial data. Continue working with your doctor on your current regimen. Suzetrigine for chronic neuropathy isn't available yet — the Phase III trials are still underway, and FDA approval for neuropathic pain, if it comes, is likely still 1-2 years away.
If your current medications aren't working well enough: Ask your neurologist about clinical trials. Vertex has active trials for diabetic peripheral neuropathy at approximately 50 sites. Clinical trials give you access to the medication before it's commercially available, and all care is provided at no cost.
If you need surgery or have an injury: Suzetrigine is already available by prescription for acute pain. If you want to avoid opioids for post-surgical pain, discuss suzetrigine with your surgeon or anesthesiologist. The cost may be a factor — compare it to other non-opioid options and your insurance coverage.
Keep perspective: Suzetrigine is genuinely exciting because it represents a new mechanism of action — the first peripherally-targeted pain drug in decades. But it's not a miracle cure for neuropathy. Even if approved for neuropathic pain, it will likely be one tool in a comprehensive treatment plan, not a replacement for addressing the root cause of your nerve damage.
The Bigger Picture: Nav1.8 and the Future of Neuropathy Treatment
Suzetrigine is the first drug in this class to reach the market, but it's not the only one in development. Several other pharmaceutical companies are developing Nav1.8 inhibitors and related sodium channel blockers targeting peripheral neuropathic pain. This research pipeline suggests that even if suzetrigine itself has limitations, the Nav1.8 approach may yield multiple treatment options in the coming years.

The broader significance is that the pharmaceutical industry is finally investing seriously in peripheral nerve-targeted approaches to pain. For decades, neuropathy patients have been treated primarily with medications designed for other conditions — antidepressants, anticonvulsants, and opioids — repurposed for nerve pain. Suzetrigine represents the beginning of a new era where drugs are designed from the ground up to work where neuropathic pain actually originates: in the peripheral nerves.
That's worth being hopeful about — cautiously, scientifically, but genuinely hopeful.
Frequently Asked Questions
Is Journavx (suzetrigine) approved for neuropathy?
Not yet. As of early 2026, suzetrigine is FDA-approved only for moderate-to-severe acute pain in adults. Vertex Pharmaceuticals is running Phase III clinical trials testing suzetrigine specifically for painful diabetic peripheral neuropathy, with proof-of-concept data showing promising results. If the trials succeed, a neuropathy-specific approval could come within 1-2 years.
How is suzetrigine different from gabapentin or Lyrica?
Gabapentin and Lyrica work in the central nervous system — they modify nerve signaling in the brain and spinal cord. Suzetrigine works in the peripheral nervous system, blocking pain signals at the source by targeting Nav1.8 sodium channels on pain-sensing nerve cells. This peripheral mechanism means suzetrigine does not cause the drowsiness, cognitive fog, or dizziness associated with gabapentin and Lyrica.
Is suzetrigine addictive?
No. Suzetrigine does not act on the brain's reward pathways and has no addiction potential. Unlike opioids, it does not produce euphoria or sedation. It is not a controlled substance. This is one of its most important advantages over opioid painkillers.
Can I ask my doctor to prescribe Journavx for my neuropathy pain now?
Technically, a doctor could prescribe it off-label for neuropathic pain, but there are practical barriers. Insurance is unlikely to cover it for a non-approved indication, and the cost is approximately $46.50 per day out of pocket. Additionally, long-term safety and efficacy data for chronic neuropathic pain are still being collected. Discussing clinical trial enrollment with your neurologist may be a more practical route to accessing the medication.
What are the side effects of suzetrigine?
In clinical trials, the most common side effects were itching, muscle spasms, and rash. Suzetrigine does not cause nausea or drowsiness, which are common with opioids. However, it cannot be taken with certain medications including the antibiotic erythromycin and the blood pressure medication verapamil. Grapefruit should also be avoided as it interferes with the medication's metabolism.
Will suzetrigine cure neuropathy?
No. Suzetrigine manages neuropathic pain by blocking pain signals from damaged nerves. It does not repair damaged nerves or treat the underlying cause of neuropathy. Patients would still need to address root causes like blood sugar control, nutritional deficiencies, or other conditions alongside suzetrigine for pain management.