I remember the day a woman in my neuropathy support group came in looking frustrated and a little shaken. She'd been to three different doctors, and not one of them had explained why, over the past several months, she had started tripping over her own feet — dragging her left foot when she walked, unable to lift the front of it off the ground. She'd been told she had “foot drop,” but nobody had connected the dots back to her nerve damage.
That conversation sent me down a research rabbit hole on peroneal neuropathy — a condition I hadn't heard much about despite years of living with neuropathy myself. If you're experiencing weakness in one foot, trouble lifting the front of your foot, or an unexpected slapping gait, this article is for you.
What Is Peroneal Neuropathy?
Peroneal neuropathy — also called fibular neuropathy — is damage or dysfunction of the peroneal nerve, one of the major nerves in the leg. It's actually one of the most common forms of mononeuropathy (damage to a single nerve) affecting the lower limbs.
The common peroneal nerve branches off from the sciatic nerve just behind the knee, wraps around the outer side of the knee near the top of the fibula bone, and then travels down the lower leg. Because of this anatomy — the nerve runs close to the surface at the fibular head — it's uniquely vulnerable to compression and injury. There's barely any protective tissue between the nerve and the skin at that point.
When this nerve is damaged, it disrupts the muscles that lift the foot and toes upward (dorsiflexion). The result is what doctors call foot drop — an inability to raise the front of the foot, which causes the characteristic slapping or steppage gait where you have to raise your knee higher than normal to clear your foot from the ground.
It's worth knowing the difference between peroneal neuropathy and the broader condition of peripheral neuropathy. Peripheral neuropathy typically affects nerves throughout the body in a more generalized pattern, while peroneal neuropathy is localized to this single nerve — usually in one leg — which changes both the symptoms and treatment approach.
The Anatomy: Why the Peroneal Nerve Is So Vulnerable
Understanding the anatomy helps explain why this nerve gets injured so easily compared to others.
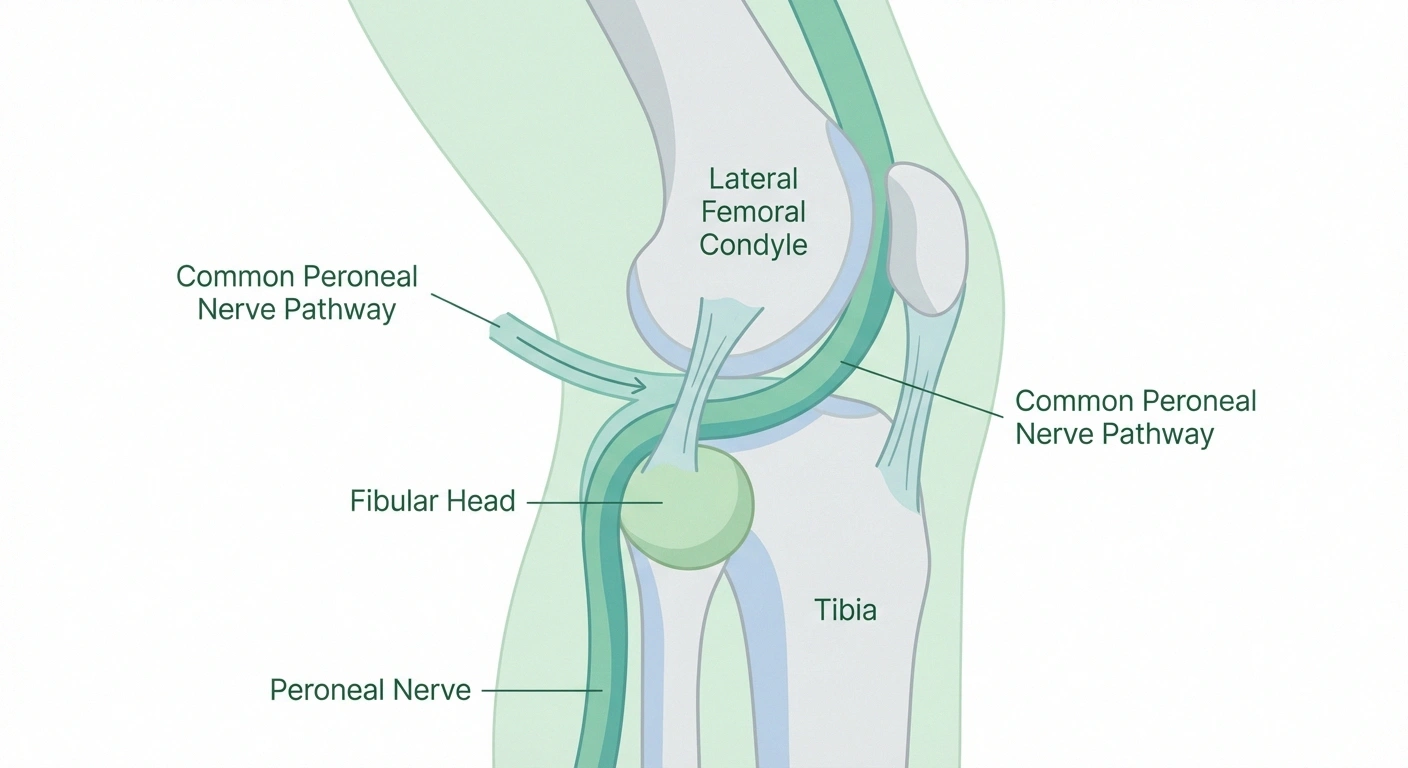
The common peroneal nerve originates from the L4-S1 nerve roots in the lumbar spine, traveling within the larger sciatic nerve before branching off behind the knee. From there, it winds around the fibular head — the bony bump on the outside of your knee — where it's covered only by skin and subcutaneous tissue. At this point, it splits into two branches:
- Superficial peroneal nerve — controls sensation along the outer leg and top of the foot, and the muscles that turn the foot outward
- Deep peroneal nerve — controls the muscles that pull the foot and toes upward, plus sensation between the first and second toes
The fibular head compression point is the critical vulnerability. Any sustained pressure at that spot — from crossing your legs, wearing a tight cast, prolonged squatting, or even sleeping in certain positions — can compress the nerve enough to cause damage.
Key Takeaway
Peroneal neuropathy is the most common mononeuropathy of the lower limb. It causes foot drop — the inability to lift the front of the foot — and is most often caused by compression at the fibular head (the bony bump on the outer knee). Early diagnosis and treatment significantly improve recovery chances.
Causes of Peroneal Neuropathy
There are more causes than most people realize. Here are the most common ones:
Direct Compression
The most frequent cause. The nerve gets compressed against the fibular head by external pressure. Specific compression causes include:
- Habitually crossing your legs
- Wearing a below-knee cast or brace
- Prolonged squatting (common in certain occupations)
- Extended time in certain positions during surgery or hospitalization
- Tight bandages or compression wraps
- Sitting for long periods with legs bent at the knee (especially in tight spaces)
Trauma and Injury
A blow to the outer knee, fractures near the fibular head, or knee ligament injuries can directly injure the peroneal nerve. Sports injuries, falls, and car accidents are common culprits. Knee replacement surgery is also a known cause — the positioning during surgery can compress the nerve, and this is actually one of the more common complications of that procedure.
Significant Weight Loss
This surprises many people, but rapid or significant weight loss can expose the peroneal nerve to compression. Fat pads that normally cushion and protect the nerve at the fibular head can disappear with major weight loss, leaving the nerve more vulnerable. Research has actually shown an 85% success rate for surgical decompression in people with foot drop following significant weight loss.
Underlying Neuropathy Conditions
People who already have diabetic neuropathy, alcoholic neuropathy, or hereditary conditions like Charcot-Marie-Tooth disease are at higher risk for peroneal neuropathy as well. Existing nerve damage makes nerves more susceptible to additional injury from compression.
Autoimmune and Inflammatory Conditions
Rheumatoid arthritis, lupus, vasculitis, and other inflammatory conditions can damage peripheral nerves including the peroneal nerve. Baker's cysts (fluid-filled swellings behind the knee) can also compress the nerve.
Tumors and Cysts
Ganglion cysts, lipomas, or other masses near the fibular head can impinge on the peroneal nerve. This is less common but important because it's a surgically treatable cause.
⚠ Important
Sudden onset foot drop — especially with no clear cause — requires prompt medical evaluation. Don't wait weeks to see a doctor. The earlier the underlying cause is identified and addressed, the better the chances of meaningful recovery. Some causes (like nerve compression) are reversible if caught early.
Symptoms: What Peroneal Neuropathy Feels Like
Symptoms vary depending on whether it's the superficial branch, deep branch, or the common peroneal nerve itself that's affected — but typical signs include:
- Foot drop — the inability to raise the front of your foot, causing it to drag or slap with each step
- Weakness in ankle/foot movements — difficulty lifting the foot upward or turning it outward
- Numbness or tingling — along the outer lower leg, top of the foot, and sometimes between the first and second toes
- Pain — may or may not be present; some people have significant pain in the outer knee or leg, others have no pain at all
- Steppage gait — an abnormal walking pattern where you must lift the knee higher to avoid dragging the foot
- Weakness turning the foot outward (eversion)
It's important to distinguish peroneal neuropathy from other causes of foot drop or leg weakness. L5 nerve root compression from a herniated disc, for example, can cause very similar symptoms — this is why proper diagnosis with nerve testing is essential. The distinction matters because treatment is completely different.
The balance problems caused by foot drop can significantly increase fall risk — something anyone dealing with this condition needs to address proactively.
Diagnosis: How Doctors Identify Peroneal Neuropathy
Getting the right diagnosis requires more than just a physical exam. Here's what to expect:
Clinical Examination
Your doctor will test the strength of specific foot and ankle movements, check sensation along the outer leg and top of the foot, and look for other neurological signs. The pattern of weakness and sensory loss points toward the peroneal nerve — but a clinical exam alone can't definitively localize the injury or determine its severity.
EMG and Nerve Conduction Studies
Electrodiagnostic testing — EMG and nerve conduction studies — is the gold standard for diagnosing peroneal neuropathy. The nerve conduction study measures how fast electrical signals travel through the nerve, and the EMG assesses the muscles the nerve supplies. For peroneal neuropathy, testing is done with electrodes at the ankle, fibular head, and back of the knee to find where the conduction slows down or blocks — which localizes the injury site.
This testing also helps determine whether the injury is primarily to the myelin sheath (demyelinating) or to the nerve fibers themselves (axonal) — which has major implications for how well and how quickly you might recover.
Research Says
A retrospective review found clinical improvement in 28 of 30 patients who underwent neuroplasty and decompression for common peroneal nerve palsy. A separate study found an 85% success rate for external neurolysis at the fibular head in patients with foot drop secondary to weight loss. (Source: PMC/Orthopedic Reviews)
Ultrasound
Nerve ultrasound has become increasingly useful in peroneal neuropathy evaluation. Unlike nerve conduction studies, ultrasound can directly visualize the nerve and identify structural causes — ganglion cysts, scarring, bone fragments, or tumors pressing on the nerve. It can also show nerve enlargement or changes in nerve appearance that indicate damage.
MRI
MRI may be ordered when a mass lesion is suspected, or to evaluate the spine if there's any possibility the symptoms originate from the lumbar nerve roots rather than the peripheral nerve.
If you haven't had a formal neuropathy diagnosis workup yet, the tests above are standard — your doctor should also review what other conditions might be contributing.
Treatment Options for Peroneal Neuropathy
Treatment depends on the underlying cause, the severity of nerve damage, and how long the condition has been present. Here's a rundown from conservative to surgical:
Addressing the Cause First
The most important first step is identifying and eliminating the compression source. If you've been crossing your legs habitually, that has to stop. If a cast or brace was the culprit, it may need to be modified or padded. If prolonged bedrest or a recent surgery is the cause, repositioning strategies become important.
Ankle-Foot Orthosis (AFO)
For foot drop, an ankle-foot orthosis — a brace that holds the foot at 90 degrees — is typically the first practical intervention. The AFO doesn't treat the nerve damage, but it allows you to walk safely while the nerve heals (if healing is possible) and dramatically reduces fall risk. Choosing the right footwear with an AFO matters — specially designed shoes for neuropathy are often needed.

Physical Therapy
Physical therapy plays a critical role in peroneal neuropathy management. A therapist can work on strengthening the remaining functional muscles in the foot and leg, improving proprioception (balance and position sense), gait training with the AFO, and preventing contractures — the stiffening that can develop when muscles aren't used normally. Balance training is particularly important given the elevated fall risk.

~1mm/day
Rate of peripheral nerve regeneration. A nerve injured at the knee may take 12–18 months to fully regenerate to the foot if the nerve fibers themselves were damaged.
Medications for Pain
If pain is a component, standard neuropathic pain medications may be used. Gabapentin, pregabalin, and duloxetine are common options — the same medications used for peripheral neuropathy in general. Anti-inflammatory medications may also be helpful in cases involving inflammatory causes.
TENS and Electrical Stimulation
TENS units and other electrical stimulation modalities can help with pain management and may support nerve function during recovery. Some research supports functional electrical stimulation specifically for foot drop.
Surgical Options
Surgery is considered when conservative measures fail or when a structural cause (like a cyst or scar tissue) is identified. The main surgical options are:
- Nerve decompression/neurolysis — releasing the peroneal nerve at the fibular head by cutting through the tight fascial tissue. Research shows 28 of 30 patients improved after this procedure in one study series.
- Tendon transfer — when the nerve cannot recover, a tendon transfer procedure (typically moving the tibialis posterior tendon) can restore active foot lifting. This bypasses the damaged nerve entirely.
- Nerve repair or grafting — in cases of complete nerve transection from trauma, surgical repair may be attempted.
Timing matters significantly for surgical intervention. Research suggests better outcomes when decompression surgery is performed earlier rather than after months or years of waiting. There is a trend toward better recovery when surgery happens within 48 hours for acute injuries, though this isn't always practically possible.
Recovery: What to Realistically Expect
This is the question everyone asks — and the honest answer is: it depends.
Recovery from peroneal neuropathy is highly variable and depends on:
Peroneal Neuropathy: Diagnosis Pathway
Clinical exam — test dorsiflexion strength, sensory loss pattern, reflexes
- Cause — Compression-related injuries generally have better prognosis than trauma or severe axonal damage
- Severity — Demyelinating injuries (myelin sheath damage) typically recover better and faster than axonal injuries (nerve fiber damage)
- Duration — The longer the nerve has been injured without treatment, the harder recovery becomes
- Underlying health conditions — Diabetes, vascular disease, and other conditions that impair nerve healing affect the outcome
- Age — Nerve regeneration slows with age
For mild to moderate compression injuries, good recovery is possible over weeks to months. The peroneal nerve regenerates at roughly 1mm per day — so a nerve injured at the knee may take 12-18 months to fully regenerate down to the foot if the nerve fibers themselves were damaged.
For chronic injuries or severe damage, full recovery is less certain. Understanding how nerve damage progresses can help set realistic expectations for your own situation.
Key markers of recovery include return of sensation, gradual strengthening of ankle dorsiflexion, and eventually less reliance on the AFO. Some people never recover full function but achieve significant improvement. Others make a complete recovery.
Living With Peroneal Neuropathy and Foot Drop
If you're managing foot drop day-to-day, there are practical strategies beyond medical treatment:

Fall Prevention Is Non-Negotiable
Foot drop dramatically increases fall risk. Always wearing your AFO (even for short trips to the bathroom at night), removing tripping hazards at home, using handrails on stairs, and installing grab bars in the bathroom are all essential. This connects directly to broader neuropathy balance and fall prevention strategies.
Footwear Matters
With an AFO, you'll need shoes with a wider toe box and removable insoles to accommodate the brace. Deep-toe box shoes designed for neuropathy patients are often a good starting point. Avoid backless shoes, sandals, or anything without a secure heel strap.
Exercise Within Your Capability
Staying active is important even with foot drop. Swimming, stationary cycling, and seated exercises can maintain fitness without the fall risk of walking on uneven terrain. Low-impact exercises keep circulation moving and muscles engaged.
Did You Know?
Habitually crossing your legs is one of the most common causes of peroneal neuropathy. Each time you cross legs at the knee, you compress the peroneal nerve against the fibular head. Repeated or prolonged compression over time can cause lasting nerve damage. If you have neuropathy, this habit should stop completely.
Ongoing Foot Care
Because sensation may be reduced, meticulous neuropathy foot care is essential. Inspect your feet daily for pressure sores, blisters, or injuries you might not feel. The combination of reduced sensation and abnormal gait creates real foot health risks.

When to See a Specialist
Don't wait on this one. If you develop sudden foot drop or rapidly progressing weakness and numbness in one leg, that warrants prompt medical evaluation — not watchful waiting. The earlier the cause is identified and addressed, the better the recovery chances.
You'll want to see a neurologist for electrodiagnostic testing and a clear diagnosis, and potentially a neurosurgeon or orthopedic surgeon if structural causes are identified or if decompression surgery is being considered. If you're managing pain alongside this, a pain specialist may also be helpful.
Frequently Asked Questions About Peroneal Neuropathy and Foot Drop
What is the most common cause of peroneal neuropathy?
External compression at the fibular head is the most common cause. This includes crossing the legs habitually, wearing tight casts or splints, prolonged squatting, and positioning during surgery. The nerve is extremely vulnerable at this anatomical location because it runs close to the surface with minimal protective tissue.
Can peroneal neuropathy heal on its own?
Yes, in many cases — especially when caused by temporary compression. Once the compression source is removed, mild to moderate injuries often recover gradually over weeks to months. Severe injuries with significant axonal damage have a much less predictable recovery timeline and may not fully heal.
Is foot drop the same as peroneal neuropathy?
No. Foot drop is a symptom — the inability to lift the front of the foot — and peroneal neuropathy is one cause of foot drop. Other causes include L5 nerve root compression from a herniated disc, stroke, brain tumors, multiple sclerosis, and other conditions. That's why proper diagnosis with nerve conduction studies is essential before assuming the cause.
How long does recovery from peroneal neuropathy take?
Recovery time varies enormously. Mild compression injuries may improve in weeks to a few months. Severe injuries where nerve fibers (axons) are damaged may take 12-18 months or longer, since nerves regenerate at roughly 1mm per day. Some people never achieve full recovery, while others return to essentially normal function.
Practical Tip
Wear your AFO brace even for short trips — including to the bathroom at night. Falls with foot drop happen most often during those unguarded moments. Keep the AFO where you can put it on immediately when getting out of bed.
Will I always need to wear a brace with foot drop?
Not necessarily. If the underlying nerve heals, foot drop often improves and the brace may no longer be needed. For people with permanent foot drop, modern AFOs are lightweight and can be worn inside regular shoes, making them manageable for daily life. Tendon transfer surgery is also an option for permanent foot drop if walking mechanics are a significant problem.
Can exercises help foot drop?
Yes. Physical therapy exercises to strengthen ankle dorsiflexors, improve proprioception and balance, and maintain range of motion in the ankle and foot are valuable. Electrical stimulation exercises may also support nerve recovery. However, exercises do not replace the need to address the underlying cause of the nerve damage.
Does peroneal neuropathy cause pain?
Pain varies by person and by which branch of the nerve is affected. Some people with peroneal neuropathy have significant pain along the outer knee and leg. Others have primarily numbness and weakness with little or no pain. Pain, when present, can often be managed with neuropathic pain medications.
What's the difference between peroneal neuropathy and sciatica?
Sciatica refers to pain and symptoms originating from compression of the sciatic nerve roots in the lower back — typically from a herniated disc or spinal stenosis. Peroneal neuropathy is damage to the peroneal nerve branch further down the leg. Both can cause foot and leg symptoms, but sciatica usually involves pain radiating from the lower back through the buttock and down the leg, while peroneal neuropathy typically has a more localized pattern focused on the outer knee, lower leg, and top of the foot without back pain.
A Final Note on Getting the Right Care
Peroneal neuropathy is one of those conditions that can go months or even years without a proper diagnosis — especially when doctors focus only on the foot drop without investigating the nerve carefully. If you're managing foot drop or outer-leg symptoms and haven't had electrodiagnostic testing, that's the most important next step.
The good news is that for many people with peroneal neuropathy — especially those where compression is the cause — meaningful recovery is possible with the right diagnosis, treatment, and rehab. It takes patience, consistent physical therapy, and often a good AFO, but people do get better from this.
I've seen it happen in our support group. That woman who came in frustrated and confused about her foot drop? She eventually found a neurologist who did the proper workup, identified she had nerve compression from years of leg-crossing, got fitted for a proper AFO, and committed to PT. Six months later, she was walking without the brace most of the time. Not a miracle — just good diagnosis and consistent care.
If you're dealing with broader questions about how your neuropathy is progressing and what your long-term outlook looks like, this resource on neuropathy prognosis may help give you a framework for what to expect.