Polyneuropathy vs. Mononeuropathy: Understanding the Difference
When a doctor tells you that you have neuropathy, one of the first things they need to figure out is what pattern the nerve damage follows. Is it affecting one specific nerve? Multiple nerves scattered throughout your body? Or many nerves simultaneously in a symmetrical pattern? The answer changes everything — from what's causing the damage to how it's treated to what you can expect going forward.
The two most fundamental categories are polyneuropathy (damage to many nerves) and mononeuropathy (damage to a single nerve). Understanding which type you're dealing with is one of the most important first steps in getting the right diagnosis and treatment. Let's break down exactly how they differ, what causes each one, and why it matters for your care.
What Is Polyneuropathy?
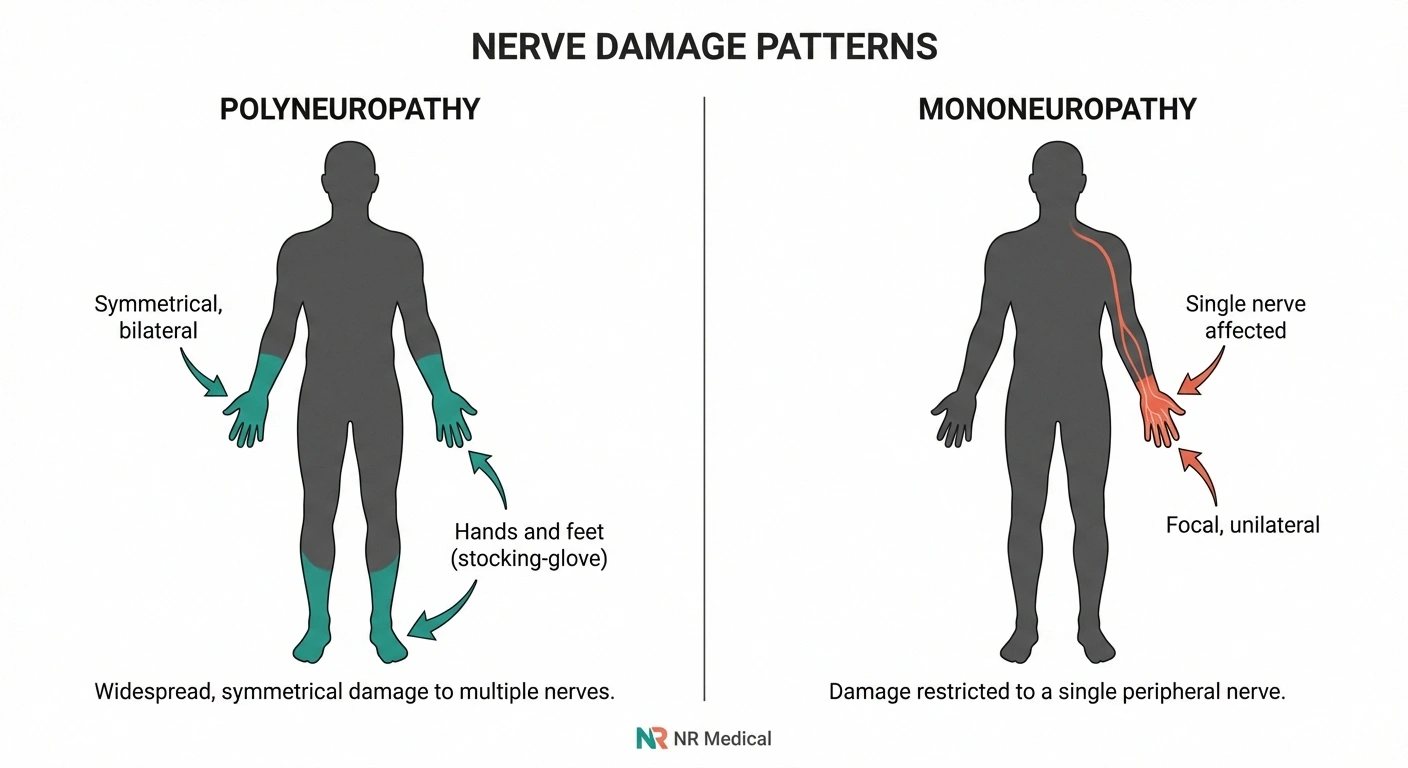
Polyneuropathy — sometimes called “peripheral polyneuropathy” — is a condition where many peripheral nerves throughout your body malfunction at the same time. The hallmark of polyneuropathy is its symmetrical, length-dependent pattern: it typically starts in the longest nerves first, which is why symptoms almost always begin in the feet and gradually move upward toward the legs, then later affect the hands and arms.
Doctors often describe this as a “stocking-glove” distribution because the affected areas mirror the pattern of wearing stockings and gloves. This pattern makes sense when you think about the underlying mechanism: because the longest nerve fibers are most vulnerable to metabolic, toxic, or inflammatory damage, the nerves running to your toes (the farthest point from your spinal cord) are the first to fail.
Polyneuropathy is, by far, the more common type. When most people say “neuropathy” without any other qualifier, they're usually referring to polyneuropathy. According to the National Institute of Neurological Disorders and Stroke (NINDS), an estimated 20 million Americans have some form of peripheral neuropathy, and the vast majority have polyneuropathy.
Common Symptoms of Polyneuropathy
- Numbness, tingling, or “pins and needles” starting in toes and fingertips
- Burning or freezing pain in feet and hands
- Gradual loss of sensation that moves upward from feet toward legs
- Balance problems and difficulty walking, especially in the dark
- Muscle weakness in the lower legs and feet (foot drop in advanced cases)
- Sensitivity to touch — even light contact like bedsheets can be painful
- Symptoms are typically symmetrical — both feet, both hands
Common Causes of Polyneuropathy
Polyneuropathy has a long list of potential causes, but a handful account for the vast majority of cases:
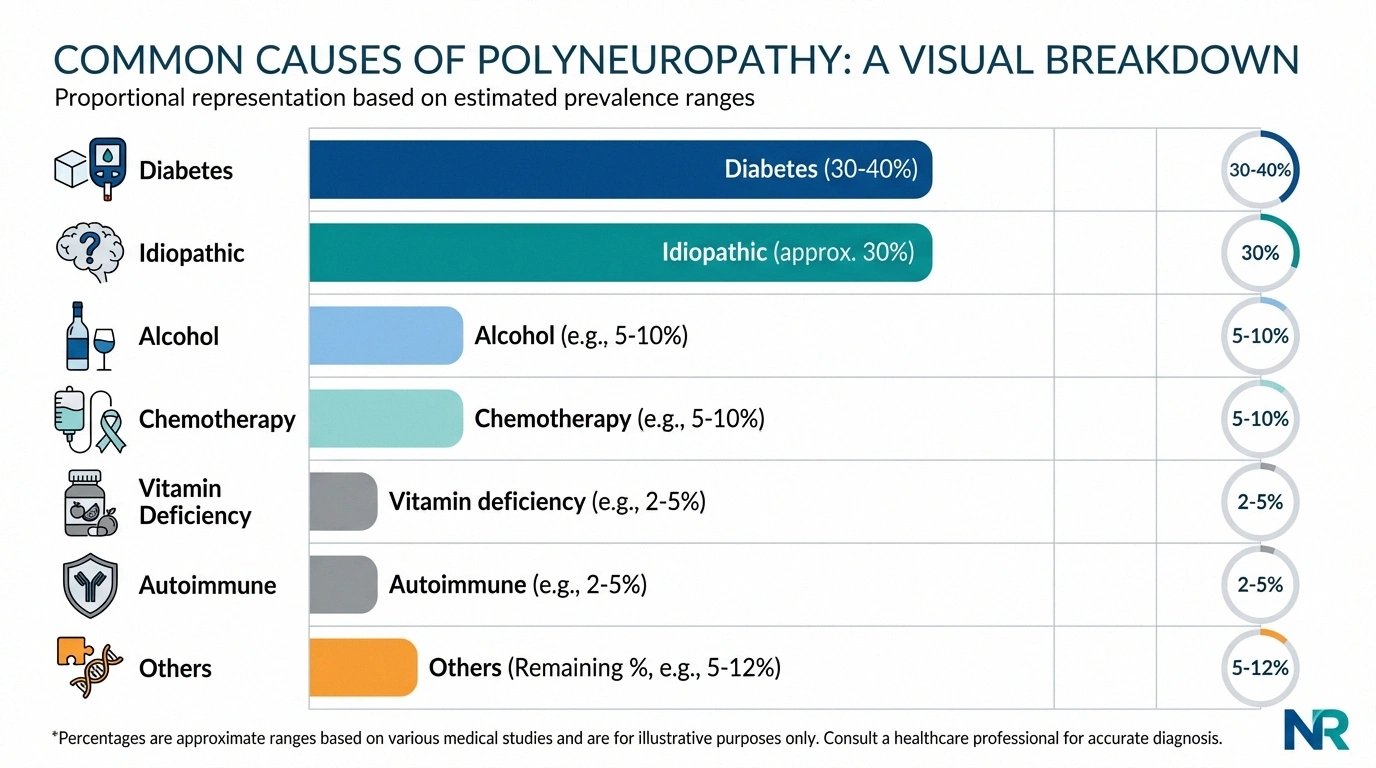
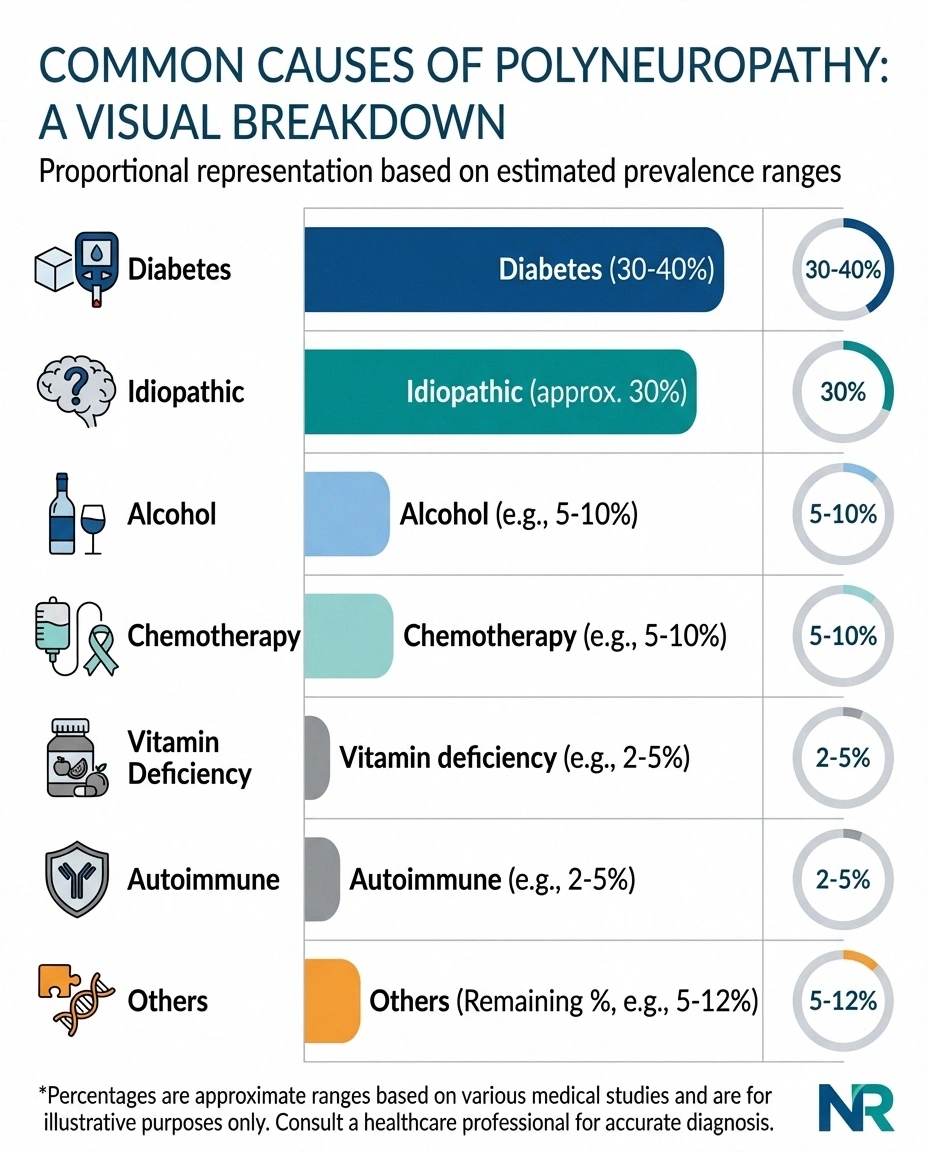
- Diabetes — the single most common cause, responsible for about 30-40% of all CIDP as a demyelinating polyneuropathy cases. Chronically elevated blood sugar damages nerve fibers over time.
- Idiopathic (unknown cause) — in approximately 30% of cases, no identifiable cause is found despite thorough testing
- Alcohol — chronic heavy drinking directly damages nerves and often causes nutritional deficiencies that compound the damage
- Chemotherapy — many chemotherapy drugs are neurotoxic and cause polyneuropathy as a side effect
- Vitamin deficiencies — particularly B12, B1 (thiamine), B6, and vitamin E
- Autoimmune conditions — including Guillain-Barré syndrome, chronic inflammatory demyelinating polyneuropathy (CIDP), and lupus
- Kidney disease — uremic toxins that accumulate in kidney failure damage peripheral nerves
- Thyroid disorders — particularly hypothyroidism
- Toxin exposure — heavy metals, industrial chemicals, and certain medications
What Is Mononeuropathy?
Mononeuropathy is damage to a single peripheral nerve. Unlike the diffuse, widespread pattern of polyneuropathy, mononeuropathy causes symptoms in the specific area that one nerve serves. The symptoms are localized and often one-sided — you might have numbness in just three fingers of one hand, weakness in one foot, or pain along one specific nerve pathway.
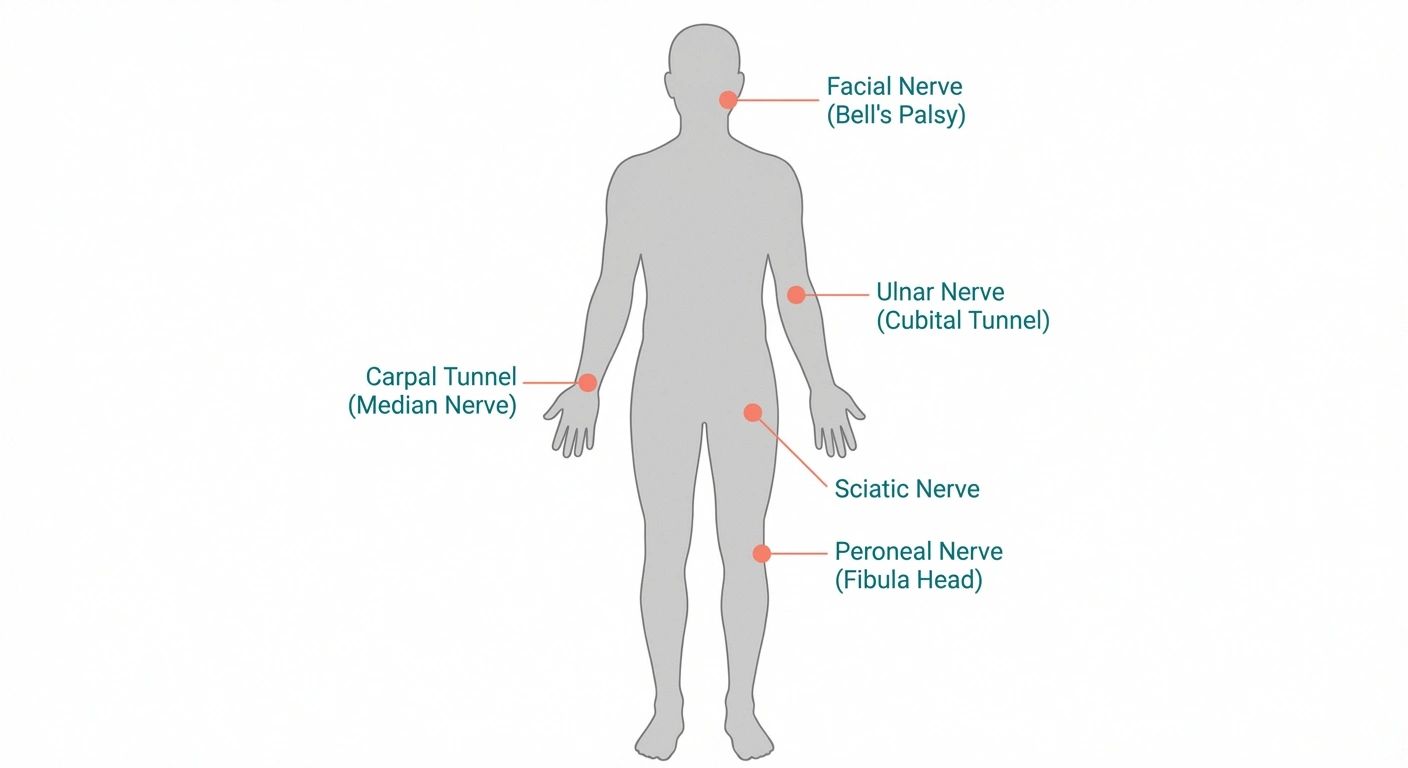
Mononeuropathies are extremely common. In fact, you've probably heard of several without realizing they were forms of neuropathy:
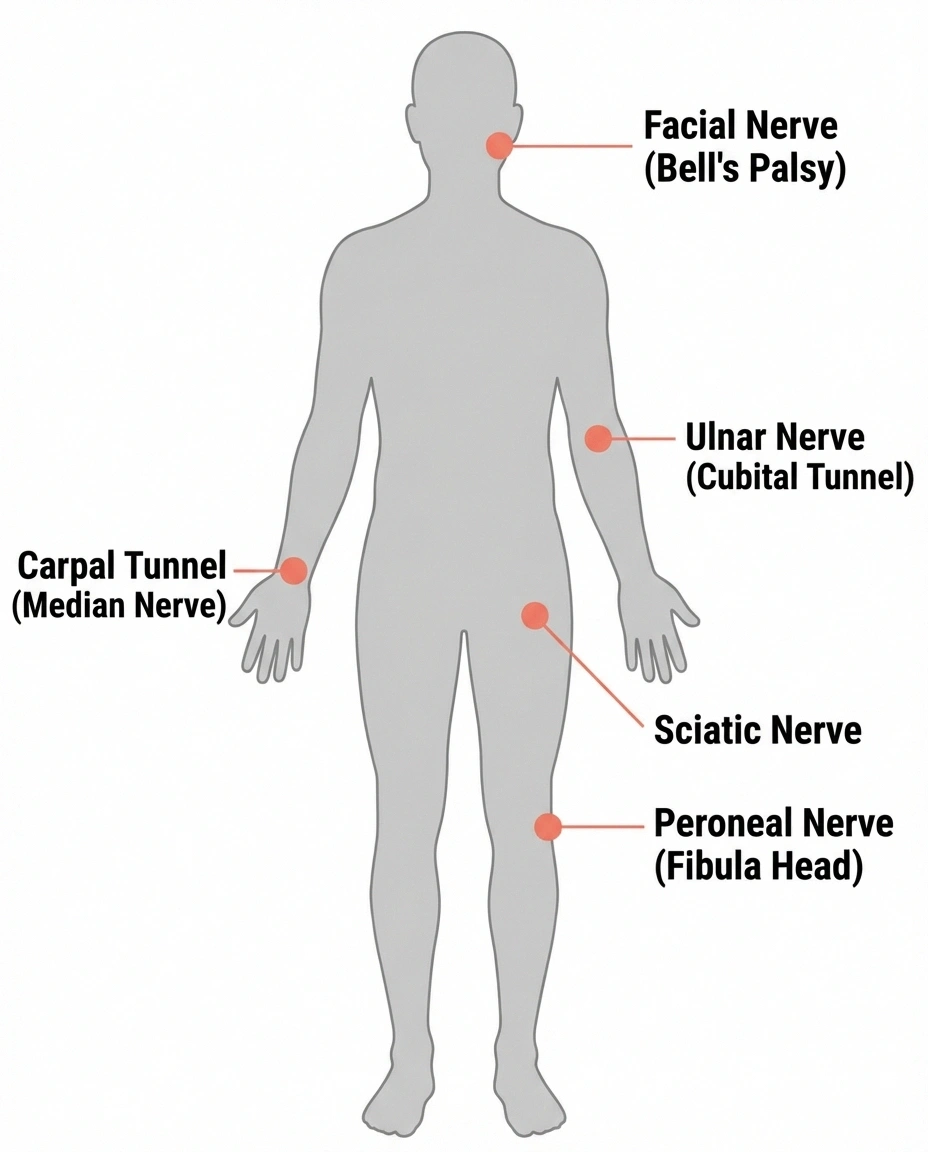
- Carpal tunnel syndrome — compression of the median nerve at the wrist (the most common mononeuropathy)
- Sciatica — compression or irritation of the sciatic nerve, causing pain down the back of one leg
- Ulnar neuropathy — compression of the ulnar nerve at the elbow (“funny bone” nerve), causing numbness in the ring and little finger
- Bell's palsy — damage to the facial nerve causing one-sided facial weakness
- Peroneal nerve palsy — compression of the peroneal nerve below the knee, causing foot drop
The key distinguishing feature of mononeuropathy is that it follows the distribution of one specific nerve. A doctor who understands nerve anatomy can often identify which nerve is affected based solely on the pattern of symptoms — a diagnostic skill called “neurological localization.”
Common Causes of Mononeuropathy
While polyneuropathy is usually caused by systemic conditions (diabetes, toxins, autoimmune disease), mononeuropathy typically has a local, mechanical cause:
- Nerve compression or entrapment — the most common cause. Nerves that pass through narrow anatomical tunnels (like the carpal tunnel in the wrist) are especially vulnerable to being squeezed by swollen tissue, bone spurs, or repetitive pressure.
- Direct trauma — fractures, lacerations, or crush injuries that damage a nerve at a specific location
- Prolonged pressure — sleeping in a position that compresses a nerve, leaning on elbows for extended periods, or wearing a tight cast
- Tumors or cysts — growths that press on a nearby nerve
- Inflammation — localized inflammatory conditions that damage a specific nerve
Key Differences Between Polyneuropathy and Mononeuropathy
Understanding the practical differences between these two types helps you and your doctor navigate diagnosis and treatment more effectively. Here's how they compare across the dimensions that matter most:
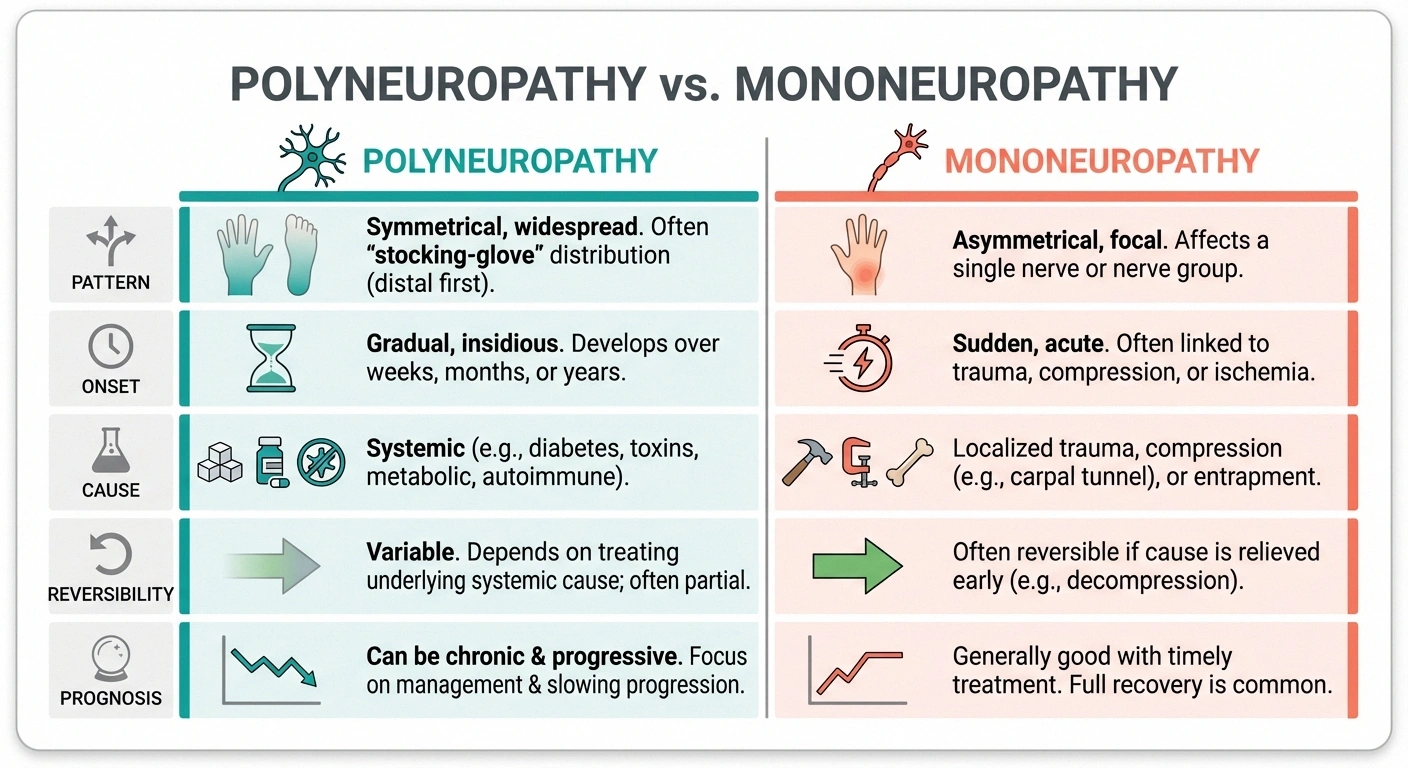
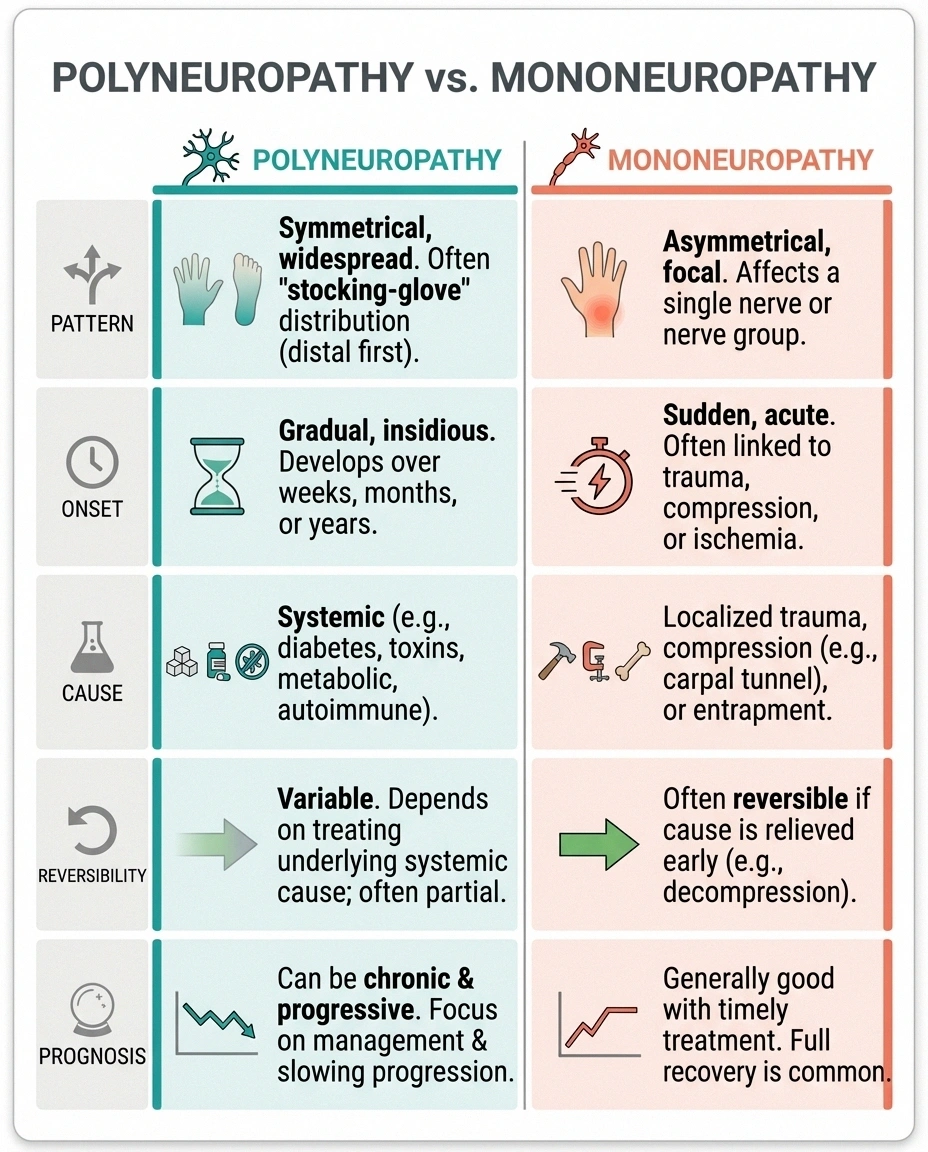
Pattern: Polyneuropathy is symmetrical and length-dependent — both sides of the body, starting at the extremities. Mononeuropathy is asymmetrical and localized — affecting one specific area on one side of the body, matching a single nerve's territory.
Onset: Polyneuropathy usually develops gradually over months to years. Mononeuropathy can develop suddenly (after an injury) or gradually (from repetitive compression).
Cause: Polyneuropathy is typically caused by systemic conditions — diseases or toxins that affect the whole body. Mononeuropathy is typically caused by local factors — compression, trauma, or inflammation at one specific site.
Reversibility: Mononeuropathy is often more treatable and potentially reversible. If you relieve the compression (through splinting, surgery, or lifestyle changes), the nerve can often recover. Polyneuropathy's reversibility depends entirely on the underlying cause — some causes are reversible (vitamin deficiency, early diabetic neuropathy) while others are not.
Prognosis: Mononeuropathy generally has a better long-term outlook because a single nerve can recover when the offending cause is removed. Polyneuropathy's prognosis is more variable and depends heavily on whether the underlying cause can be treated.
What About Mononeuritis Multiplex?
There's a third category that sits between polyneuropathy and mononeuropathy: mononeuritis multiplex (also called “multiple mononeuropathy”). This is when two or more individual nerves in different parts of your body are damaged — but in a patchy, asymmetrical pattern rather than the symmetrical stocking-glove pattern of polyneuropathy.
The distinction matters clinically because mononeuritis multiplex has a very different set of causes than either polyneuropathy or simple mononeuropathy. The Merck Manual notes that the most common causes include vasculitis (inflammation of blood vessels), diabetes, and certain autoimmune conditions like lupus and sarcoidosis.
If your doctor tells you that your nerve damage follows a “mononeuritis multiplex” pattern, it typically triggers a more urgent workup because several of the potential causes (particularly vasculitis) require prompt treatment to prevent further nerve damage.
How Doctors Tell Them Apart
The diagnostic process for distinguishing polyneuropathy from mononeuropathy starts with a careful clinical examination and often involves specialized testing:

Neurological exam: Your doctor tests sensation, reflexes, and strength in a systematic pattern across your body. The distribution of abnormal findings often reveals the pattern immediately — symmetrical deficits point toward polyneuropathy, while deficits confined to one nerve's territory suggest mononeuropathy.
Nerve conduction studies and EMG: These electrodiagnostic tests measure how fast electrical signals travel through your nerves and how well your muscles respond. They can pinpoint exactly which nerves are affected and whether the damage is to the nerve's myelin coating (demyelination) or the nerve fiber itself (axonal loss). This distinction further narrows the diagnostic possibilities.
Blood tests: Once the pattern is established, targeted blood work helps identify the underlying cause. For polyneuropathy, this might include blood sugar, vitamin levels, thyroid function, kidney function, and autoimmune markers. For mononeuropathy, blood tests may be less revealing since the cause is usually local and mechanical.
Imaging: MRI or ultrasound can visualize nerve compression in mononeuropathy — showing exactly where a nerve is being squeezed and what's causing the compression.
Treatment Approaches
The treatment strategy differs significantly depending on which type you have:

Treating Polyneuropathy
Treatment focuses on two goals: addressing the underlying cause (if treatable) and managing symptoms. For diabetic polyneuropathy, this means blood sugar control. For vitamin deficiency, it means supplementation. For autoimmune causes, it means immunotherapy. Symptom management typically involves medications like gabapentin, pregabalin, or duloxetine, alongside physical therapy, foot care, and lifestyle modifications.
Treating Mononeuropathy
Treatment targets the specific cause of the single nerve damage. For compression neuropathies, this might include splinting (wrist splint for carpal tunnel), ergonomic changes, corticosteroid injections to reduce inflammation, or surgery to relieve the compression (carpal tunnel release, cubital tunnel release). For trauma-related mononeuropathy, treatment focuses on nerve recovery through physical therapy and, in severe cases, nerve repair surgery.
Treating Mononeuritis Multiplex
Because mononeuritis multiplex often has a systemic inflammatory or autoimmune cause, treatment typically involves immunosuppressive medications, corticosteroids, or targeted therapy for the underlying condition. Early and aggressive treatment can prevent further nerve damage.
Can You Have Both?
Yes — and it's not uncommon. A person with diabetic polyneuropathy (symmetrical numbness in both feet) can also develop carpal tunnel syndrome (mononeuropathy of the median nerve in the wrist). In fact, diabetes makes mononeuropathies more likely because chronically elevated blood sugar makes nerves more vulnerable to compression injury.

This overlap is one reason that thorough diagnostic evaluation matters. If your doctor assumes all your symptoms are from one type, they might miss a treatable mononeuropathy sitting on top of your polyneuropathy — and that treatable component could be the source of your worst symptoms.
What This Means for Your Care
Understanding whether your neuropathy is a polyneuropathy or mononeuropathy isn't just academic — it directly impacts your treatment plan, your prognosis, and the urgency of your next steps.
If you have polyneuropathy, the priority is identifying and treating the underlying cause while managing symptoms and protecting your feet and hands from injury. Long-term management and monitoring are the norm.
If you have mononeuropathy, the priority is identifying what's causing the nerve compression or damage and relieving it. Many mononeuropathies are fully treatable, and catching them early gives the nerve the best chance of complete recovery.
Either way, the starting point is the same: a thorough evaluation by a neurologist who can map the pattern of your nerve damage and work backward to the cause. If you're experiencing new or worsening symptoms, don't wait — seeing a specialist sooner rather than later gives you more options and better outcomes.
Frequently Asked Questions
Is polyneuropathy worse than mononeuropathy?
Not necessarily, but polyneuropathy tends to be more widespread and progressive. Mononeuropathy affects a single nerve and is often treatable or reversible. Polyneuropathy affects many nerves and may be chronic, depending on the cause. The severity depends more on the underlying condition than on the category.
Can mononeuropathy turn into polyneuropathy?
A simple mononeuropathy from compression does not turn into polyneuropathy. However, if you have an underlying systemic condition like diabetes, you may develop polyneuropathy separately. In some cases, what initially appears to be mononeuropathy may eventually be recognized as mononeuritis multiplex as additional nerves become affected.
How do I know which type of neuropathy I have?
The pattern of your symptoms is the biggest clue. Symmetrical numbness and tingling in both feet and hands suggests polyneuropathy. Symptoms confined to one specific area, like three fingers on one hand or pain down one leg, suggests mononeuropathy. A neurological exam and nerve conduction studies can confirm the type definitively.
Is carpal tunnel syndrome a type of neuropathy?
Yes. Carpal tunnel syndrome is a mononeuropathy specifically affecting the median nerve at the wrist. It is the most common form of mononeuropathy and is caused by compression of the nerve as it passes through the carpal tunnel in the wrist.
Can polyneuropathy be cured?
It depends entirely on the cause. Polyneuropathy caused by vitamin deficiency can often be reversed with supplementation. Early diabetic polyneuropathy may improve significantly with strict blood sugar control. However, polyneuropathy from long-standing diabetes, chemotherapy damage, or inherited conditions is usually permanent, though symptoms can be managed effectively.
What is the most common type of peripheral neuropathy?
Polyneuropathy, specifically diabetic polyneuropathy, is the most common type of peripheral neuropathy overall. Among mononeuropathies, carpal tunnel syndrome is the most common. Together, these two conditions account for a large proportion of all neuropathy cases.


