
The first time my calf muscle seized up at three in the morning, I thought I'd torn something. The pain was startling — sharp, gripping, the muscle so hard it felt like a rock under the skin. I limped to the bathroom thinking I'd done damage. By morning the pain had eased, the muscle was tender but functional, and I had no explanation. Then it happened again the next week. And the next. By the time I had been diagnosed with peripheral neuropathy, I had been quietly cataloguing what I now know are nighttime calf cramps for almost a year.
If you have neuropathy and you cramp, you are not imagining a connection between the two. Damaged nerves cause cramps. The mechanism is well-described in the research literature, and there are real things you can do about it. The cramps are not a sign you're getting worse; they're a recognized symptom of an already-known condition. That alone is a relief most patients have never been told.
I'm Janet Ellis, and this is what I've learned about why neuropathy makes muscles cramp, what to do in the moment, and what actually prevents the next one.
Yes, Neuropathy Causes Muscle Cramps
Cramps are a recognized symptom of peripheral neuropathy. They appear in the symptom lists of every major neurology reference, and they show up in patient surveys at high rates — meaningfully higher than in the general population.
Cramps are a recognized symptom of peripheral neuropathy, not a separate problem. The cramping is not a sign you're getting worse — it's a known feature of damaged nerves misfiring. There are real, immediate things that help, both in the moment and to prevent the next one.
The pattern is consistent. Most patients describe nighttime calf cramps, foot or arch cramps where the toes curl involuntarily, and sometimes hand cramps where the fingers fold tight. The cramp may last seconds or minutes. The muscle stays tender for hours afterward. The cramp can be mild and shake-out-able, or severe enough that you can't put weight on the leg until it eases.
Many patients also experience related symptoms that look similar but are not identical: muscle twitches under the skin (called fasciculations), broader muscle spasms, and sudden brief jerks (myoclonus). These all sit on the spectrum of what damaged nerves do to the muscles they connect to. We'll come back to the differences.
What surprised me when I started researching was how many patients had never connected their cramping to their neuropathy. Their doctors hadn't mentioned it. They'd been told it was dehydration, or aging, or potassium, or “just one of those things.” Sometimes that's true. Often, in a neuropathy patient, the underlying driver is the nerve damage itself.
Why Damaged Nerves Cause Cramping
The mechanism is not mystical. It's a misfiring electrical system, and once you understand it, the rest of this article makes more sense.
5 Reasons Neuropathy Causes Cramps
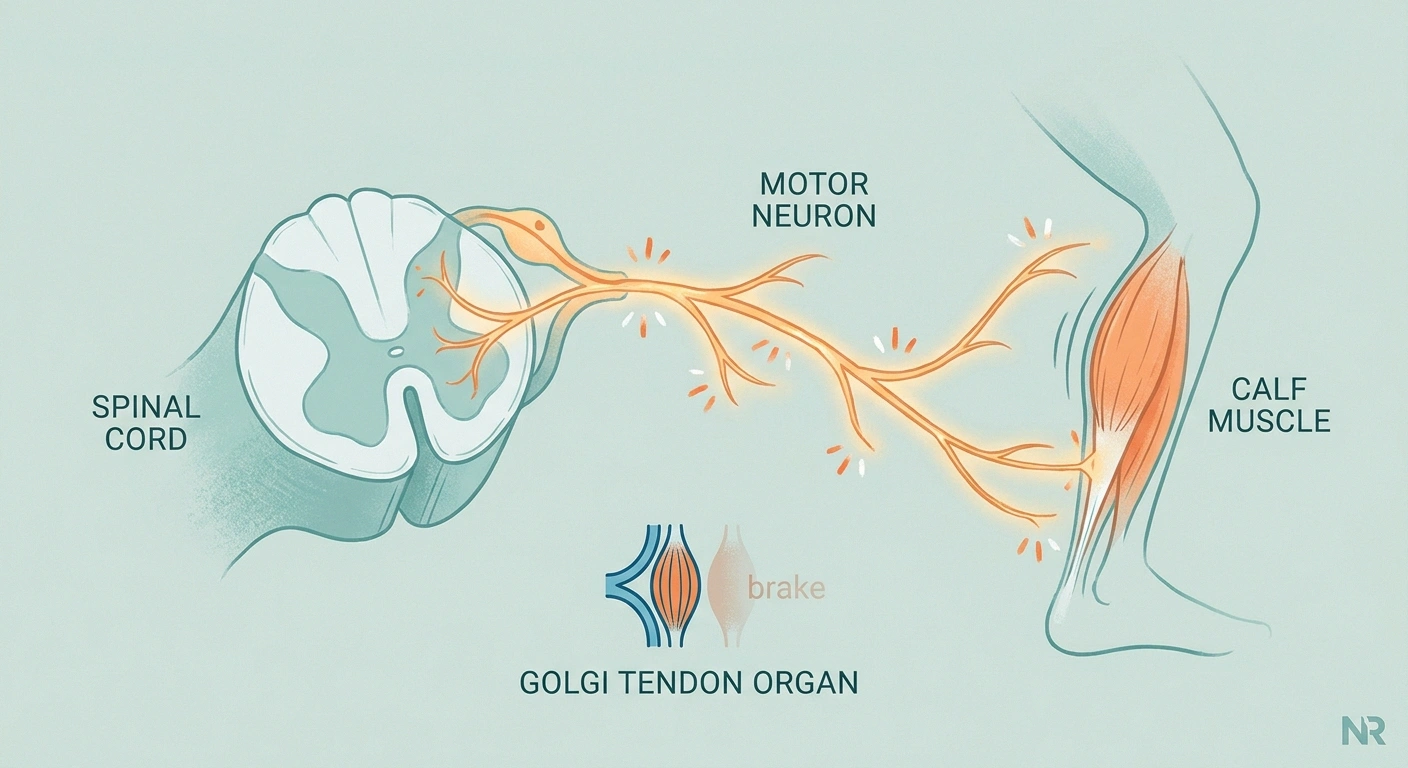
Muscles contract when motor nerves tell them to. Each motor nerve has its cell body in the spinal cord and a long fiber that runs out to the muscle, where it forms connections (called neuromuscular junctions) with individual muscle fibers. When the nerve fires, the muscle contracts. When the nerve quiets down, the muscle relaxes. That's the basic loop.
Several things go wrong in neuropathy:
Damaged motor neurons fire spontaneously. When a motor nerve is injured or stressed, the cell body in the spinal cord can become hyperexcitable. It fires when it shouldn't. Each spontaneous discharge causes a contraction in the muscle fibers it controls. Multiple discharges produce a sustained contraction — a cramp.
Inhibitory signals weaken. Normally, when a muscle starts to over-contract, sensory feedback through the Golgi tendon organs tells the spinal cord to back off. That brake gets weaker when sensory nerves are damaged. The cramp loses its built-in stop signal.
Muscle spindles drive too much. Spindles are sensors inside muscles that report stretch. When they fire excessively, they push the muscle to contract more. Damaged sensory feedback throws this calibration off.
Local inflammation excites intramuscular nerves. Damaged small nerves release inflammatory mediators that lower the threshold for cramp generation in surrounding tissue.
Electrolyte imbalances make all of this worse. Magnesium, potassium, and calcium each play a role in muscle excitability. When they're low or out of balance, a muscle that was already prone to cramp now cramps more readily and more severely.
The combined picture: hyperexcitable motor neurons fire when they shouldn't, the brakes that would normally stop the cramp are weakened, and any electrolyte stress pushes the system over the edge. That's why neuropathy patients cramp more than the general population, and why simple “drink more water and eat a banana” advice often falls short.
Cramp, Spasm, Twitch — What's the Difference?
Patients use these words interchangeably, but they describe distinct things. Telling them apart helps you describe what's happening to your doctor and helps you target treatment correctly.
Cramp vs Spasm vs Twitch vs Jerk
Cramp. A sustained, painful, involuntary muscle contraction. Lasts seconds to minutes. The muscle visibly tightens and may form a hard knot under the skin. You usually cannot voluntarily relax it. This is what most neuropathy patients are describing when they say “cramp.”
Spasm. A broader term that overlaps with cramp. Some clinicians use it for any involuntary contraction; others reserve it for jerky, repetitive contractions rather than sustained ones. In conversation, “muscle spasm” usually means the same thing as “cramp.”
Fasciculation. A small, visible twitch of a muscle bundle just under the skin. Brief, usually painless, often described as “the muscle moving on its own.” Not a cramp. Common in neuropathy and not in itself dangerous, though new or persistent fasciculations should be discussed with a doctor.
Myoclonus. A sudden, jerk-like contraction. Often happens at the edge of sleep (the “hypnic jerk” most people experience occasionally), but can be more frequent in neurologic conditions. Brief and not painful in the way a cramp is.
If you're keeping a symptom diary — and I think most neuropathy patients should — distinguishing among these four helps. A pattern of nighttime sustained cramps is a different problem than a pattern of frequent fasciculations.
What to Do in the Moment

When a cramp hits, the first goal is to stop it. There are real, immediate things that work.
When a Cramp Hits — In Order
- Stretch the cramping muscle. Lengthen it — don't shorten it. Calf cramp: dorsiflex foot. Foot cramp: pull toes back. Hand: extend fingers.
- Apply heat. Warm compress, heating pad, or warm bath. Increases blood flow and helps the muscle release.
- Massage gently. Long strokes toward the heart. Don't dig hard into the cramping fibers.
- Hydrate after. Glass of water with a pinch of salt or an electrolyte mix.
- Don't force-relax. Lengthen the muscle into the cramp. Don't try to power-relax a shortened muscle.
Stretch the cramping muscle. This is the most reliable acute intervention. For a calf cramp, stand up and put weight on the cramping leg, or sit and pull your toes upward toward your shin (dorsiflexion). For a foot cramp, push the toes back. For a hand cramp, gently extend the fingers with the other hand. The stretch interrupts the cramp signal and forces the muscle to lengthen.
Apply heat. A warm compress, heating pad, or warm bath helps the muscle relax and increases blood flow. Cold packs can also help some patients, but heat is the more common first move.
Massage gently. Knead the muscle in long strokes toward the heart. Don't dig hard into the cramping fibers — gentle, sustained pressure works better than aggressive work.
Hydrate. A glass of water won't stop a cramp in progress, but if you've been losing fluids and not replacing them, the next cramp comes faster than the last. After the cramp eases, drink water with a pinch of salt or an electrolyte mix.
Don't fight the muscle. Trying to forcibly relax a cramping muscle while keeping it shortened often makes it worse. Lengthen it. Stretch into the cramp, not away from it.
What Actually Prevents the Next One

Acute relief is one thing. The harder problem is reducing how often cramps happen. Prevention is where neuropathy patients can make real progress.
Magnesium status is one of the most common reversible contributors to nighttime cramping in neuropathy patients. Glycinate or citrate forms (350–400 mg evening dose) are well-absorbed; magnesium oxide is poorly absorbed.
Talk to your doctor before starting any supplement, especially with kidney disease or interacting medications.
Check your magnesium status. Low magnesium is one of the most common reversible contributors to cramping, and it's also low in many neuropathy patients independent of the cramps. A typical preventive dose is 350 to 400 milligrams of magnesium glycinate or magnesium citrate in the evening. Magnesium oxide is poorly absorbed; the glycinate or citrate forms work better. Talk to your doctor before adding any supplement, especially if you have kidney problems.
Stretch before bed. Five minutes of calf stretches, foot rolls, and gentle hand stretches before sleep meaningfully reduces nighttime cramping. The mechanism: pre-stretched muscles have a higher threshold for cramping. The standing wall stretch (calves), the toe-to-heel rocks (feet), and finger fans (hands) cover the most common cramp zones.
Stay hydrated. Most patients are slightly underhydrated most of the time. Aim for clear or pale-yellow urine. Add a pinch of salt and a squeeze of lemon to one or two glasses of water during the day if you're losing more fluids than usual.
Pay attention to the medication list. Certain medications increase cramping risk in neuropathy patients. Diuretics deplete electrolytes. Statins can directly affect muscles. Some inhalers, antidepressants, and chemotherapy agents are known cramp drivers. If your cramping suddenly worsened after a medication change, that's worth a conversation with your prescriber.
Consider compression socks. Light compression (15 to 20 mmHg) helps some patients with nighttime calf cramps by improving venous return and reducing muscle fatigue. Aggressive compression isn't necessary and can be uncomfortable.
Time your activity. Many patients notice cramps more after specific activities — long days on their feet, unusual exercise, or extended sitting. Once you find your patterns, modest pacing and pre-stretching around those activities helps.
What About Medications for Cramps?

If lifestyle measures aren't enough, several prescription options exist. None of them is a perfect answer.
The FDA warned in 2010 against quinine for cramps due to risks of low platelets, heart rhythm disturbances, and other serious problems. If a relative or older clinician suggests it, this is no longer accepted practice for routine cramp prevention.
Quinine is off the table. Decades ago, quinine was the standard prescription for muscle cramps. The FDA issued a warning in 2010 against using quinine for cramps because of a serious risk of low platelets, heart rhythm disturbances, and other problems. It's no longer recommended for routine cramp prevention. Patients sometimes ask about quinine because they remember it being prescribed, but the safety profile is no longer acceptable.
Gabapentin and pregabalin. These medications are first-line for neuropathic pain and often help with cramping as a side benefit. If you're already on one for nerve pain, the cramp reduction is a bonus. Starting one specifically for cramps is reasonable if cramps are severe and not responding to lifestyle measures.
Mexiletine. A sodium channel blocker used off-label for neuropathic pain and for cramps. Effective in some patients, but requires cardiac evaluation before starting because of the rhythm-disturbance risk. Specialty prescribing.
Baclofen. A muscle relaxant that can help when cramps are severe and frequent. Causes drowsiness and should not be stopped abruptly.
Phenytoin. An older anti-seizure medication occasionally used for cramps in specialized cases.
The honest hierarchy: lifestyle and electrolyte optimization first, then a discussion with your doctor about whether any medication you're already on (gabapentin, pregabalin) might be adjusted to also address cramps, then specialty options if needed.
Why Cramps Are Worse at Night

Most neuropathy cramps happen at night. There are several reasons.
5-Minute Pre-Bed Anti-Cramp Routine
Pre-stretched muscles have a higher cramp threshold.
The first is positional. When you sleep, your feet often point downward (plantar flexion), shortening the calf muscle. A shortened muscle is more prone to cramping than a lengthened one. The longer you stay in that position, the more the cramp threshold drops.
The second is circulatory. Lying still reduces venous return and lets minor electrolyte gradients build up.
The third is neurological. Many neuropathy symptoms — pain, tingling, restless legs, cramps — are worse at night because daytime sensory input that distracts from nerve symptoms goes quiet. The same hyperexcitable motor neurons that misfire during the day get more attention from your brain at night.
The pre-bed stretch routine I mentioned earlier addresses the first cause. Hydration earlier in the evening (not right before bed, which disrupts sleep) addresses the second. Magnesium addresses the third indirectly.
When to Tell Your Doctor

Most neuropathy cramps are uncomfortable but not dangerous. There are situations where they warrant a real medical conversation.
5 Cramp Patterns Worth a Doctor Visit
- New cramping after a medication change — statins, diuretics, antidepressants
- Cramping plus new weakness — possible progression or separate process
- Cramps lasting longer than 10 minutes — most release in seconds to minutes
- Cramps plus rapid muscle wasting or speech/swallow changes — different conditions to rule out
- Sudden severe increase in frequency — something has shifted
New cramping after a medication change. If you started a new prescription and the cramping started or got worse, the connection is worth investigating. Statins, diuretics, and certain antidepressants are common drivers.
Cramping with new weakness. Cramps in a muscle that is also getting weaker over time may indicate progression of the neuropathy or a separate process. This is one of the more important “tell the doctor” patterns.
Cramps lasting longer than 10 minutes. Most cramps resolve within seconds to minutes. A cramp that won't release for ten or more minutes, or one that leaves the muscle severely tender or bruised afterward, deserves attention.
Cramping plus other red flag symptoms. Cramping with rapid muscle wasting, persistent severe weakness, or speech and swallowing changes can point to other conditions, including some that are not neuropathy. Most patients reading this don't have these — but if you do, the symptom combination is the key.
Sudden severe increase in frequency. If your cramping pattern changes dramatically — going from one or two a week to multiple every night — something has shifted. Dehydration, a new medication, electrolyte disturbance, or worsening neuropathy are the usual suspects, and a quick visit can sort it out.
Cramping in Specific Neuropathy Types
Different causes of neuropathy have somewhat different cramp patterns.
Diabetic neuropathy. Calf and foot cramps are very common. Blood-sugar swings make cramping worse. Patients with the most chronic and severe diabetic neuropathy often have the most cramping.
Chemotherapy-induced neuropathy. Hand and foot cramps are common during and after treatment. Cramping can persist for months or longer after chemotherapy ends.
Small-fiber neuropathy. Cramping is sometimes the first symptom that brings patients in. Foot cramps and toe cramps are particularly common. The mechanism is partly inflammation-driven, which is why some patients respond to anti-inflammatory approaches.
Idiopathic neuropathy. The mechanism is the same as in any other neuropathy — hyperexcitable motor neurons, weakened inhibition. Treatment is the same.
Inherited neuropathies (Charcot-Marie-Tooth and others). Cramping is common and tends to be a long-running feature. Patients are often more familiar with their pattern and have a working set of personal strategies.
What I Wish I Had Known Earlier
Three things would have saved me a lot of nights.
The first: I would have started magnesium five years sooner. It's a low-cost, low-risk supplement that helps a real percentage of cramping patients meaningfully. The downside is loose stools at high doses, but at the 350-to-400-milligram dose most patients tolerate it fine.
The second: I would have stretched before bed. Five minutes. I resisted because it felt fussy. The reduction in nighttime cramping was disproportionate to the effort.
The third: I would have asked my prescribers earlier whether any of my medications were contributing. One of them was. Adjusting it didn't eliminate cramps, but it cut the frequency in half.
None of these is a cure. They reduce frequency and severity. For a neuropathy patient, that combination — fewer cramps, milder when they happen, better sleep, better mobility — adds up to a meaningfully better life.
Frequently Asked Questions
Why do people with neuropathy get muscle cramps?
Damaged nerves cause spontaneous, abnormal firing of motor neurons, which makes muscles contract when they shouldn't. The normal feedback loops that would stop a cramp are also weakened by sensory nerve damage. Add common electrolyte imbalances on top and the cramping threshold drops further. The combined picture is why neuropathy patients cramp more than the general population.
What helps muscle cramps from neuropathy?
For an acute cramp: stretch the cramping muscle in the lengthening direction, apply gentle heat, massage long strokes toward the heart, and rehydrate afterward. For prevention: 350 to 400 milligrams of magnesium glycinate or citrate in the evening, a five-minute pre-bed stretch routine, consistent hydration, and a check of your medication list for known cramp drivers like diuretics and statins.
Are cramps a symptom of neuropathy?
Yes. Cramps are listed as a symptom of peripheral neuropathy in major neurology references and appear at high rates in patient surveys. They are particularly common in diabetic, chemotherapy-induced, and small-fiber neuropathies. Many patients are not told this connection, which is why so many describe years of cramping without ever connecting it to their neuropathy diagnosis.
Is gabapentin good for muscle cramps?
Gabapentin is approved for neuropathic pain, not specifically for cramps, but it does reduce cramping in many neuropathy patients as a side benefit. If you're already on gabapentin or pregabalin for nerve pain and you cramp, you may be cramping less than you would otherwise. Starting it specifically for cramps is reasonable when lifestyle measures are insufficient and your doctor agrees.
What deficiency causes nerve cramps?
The deficiencies most commonly linked to cramping are magnesium, potassium, calcium, and sometimes vitamin D. Magnesium is the most common in clinical practice and the easiest to address. In neuropathy patients, the cramping is rarely caused by a deficiency alone — it's the combination of nerve damage plus a borderline electrolyte status that produces the most severe pattern. Testing levels and supplementing strategically is more useful than guessing.
Why do my feet cramp so badly at night?
The combination of plantar flexion (toes pointing down) during sleep, reduced circulation in a still position, and the natural tendency for nerve symptoms to be louder at night when other sensory input is quiet. Pre-bed foot rolls and toe stretches address the first; staying gently active during the day and adequately hydrated addresses the second; magnesium and treating the underlying neuropathy address the third.
Can I prevent cramps without medication?
For many patients, yes — at least to a meaningful degree. The combination of magnesium supplementation, evening stretching, consistent hydration, and avoiding known dietary triggers reduces cramp frequency substantially in most patients who try it for at least four to six weeks. If lifestyle measures are not enough, prescription options exist, but most patients see real improvement before getting to that step.
Is muscle cramping in neuropathy a sign it's getting worse?
Not usually. Cramping is a recognized symptom of established neuropathy, not necessarily a sign of progression. Cramping that is suddenly much worse, that comes with new weakness, or that shifts to muscles that didn't cramp before is more notable and worth telling your doctor. A stable pattern of cramping at roughly the same frequency over months is normal background for neuropathy and does not, by itself, mean things are getting worse.


