I sat in my Medicare counselor's office last winter with a stack of denial letters in my lap and a question I'd been avoiding for months: What does Medicare actually pay for when you have neuropathy?
Two hours later, I walked out with a clearer answer than three years of guessing had given me. Medicare covers far more than most patients realize — and it also denies, refuses, or quietly leaves out specific services in ways that catch people off guard at the worst possible moment. The difference between a covered claim and an unexpected $1,800 bill often comes down to a single CPT code, the exact wording on your doctor's note, or whether you knew to ask for a particular benefit by name.
This article is the plain-English version of what I learned. It's not legal advice, and it isn't a substitute for talking to your own State Health Insurance Assistance Program (SHIP) counselor. But after watching readers in my support group hit the same dead ends over and over, I wanted to write down what's covered, what's not, and how to push back when a claim gets denied unfairly.
The Medicare Map: A Five-Minute Overview
Medicare isn't one program. It's four parts that fit together, plus a private supplemental layer. For neuropathy specifically, what gets covered depends on which part picks up the bill. Here's the version I wish someone had drawn for me on a napkin three years ago.
Key Takeaway
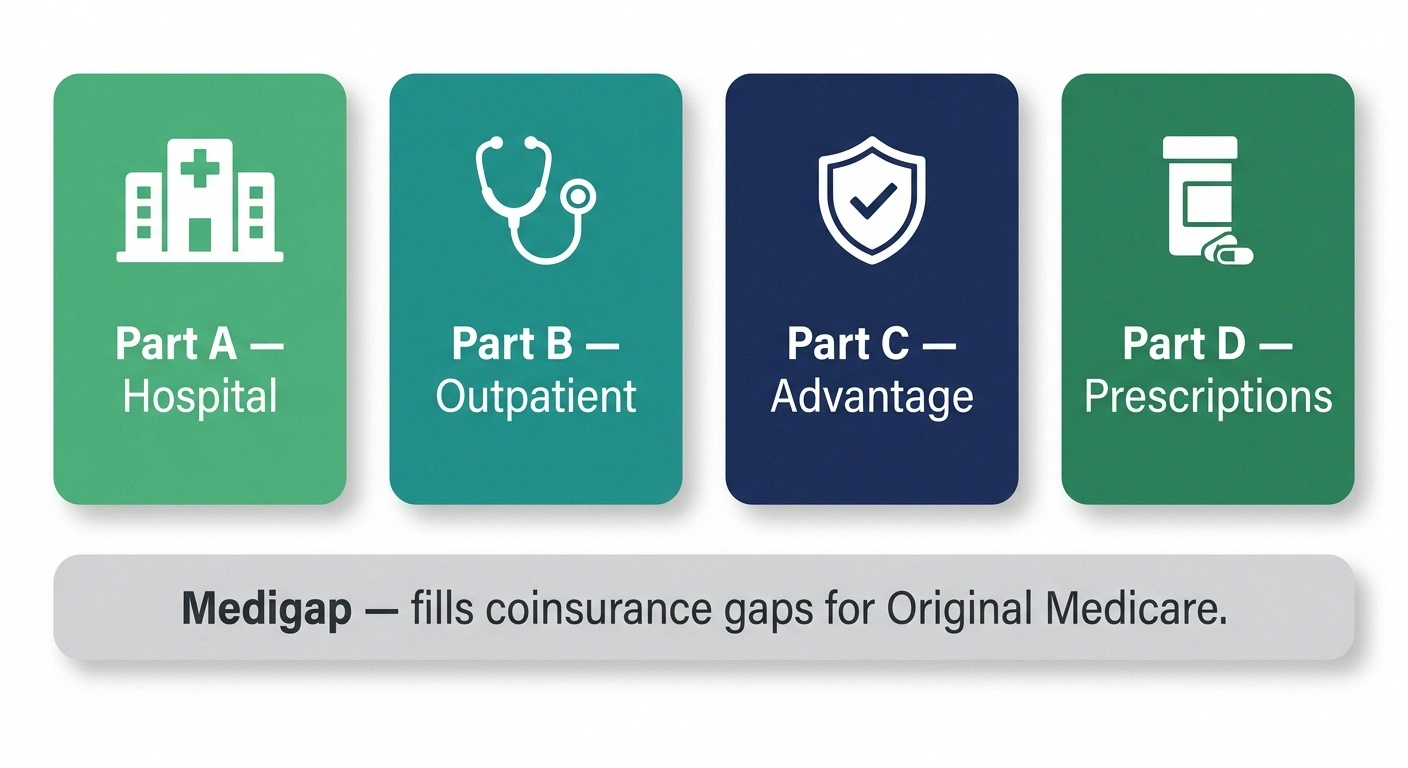
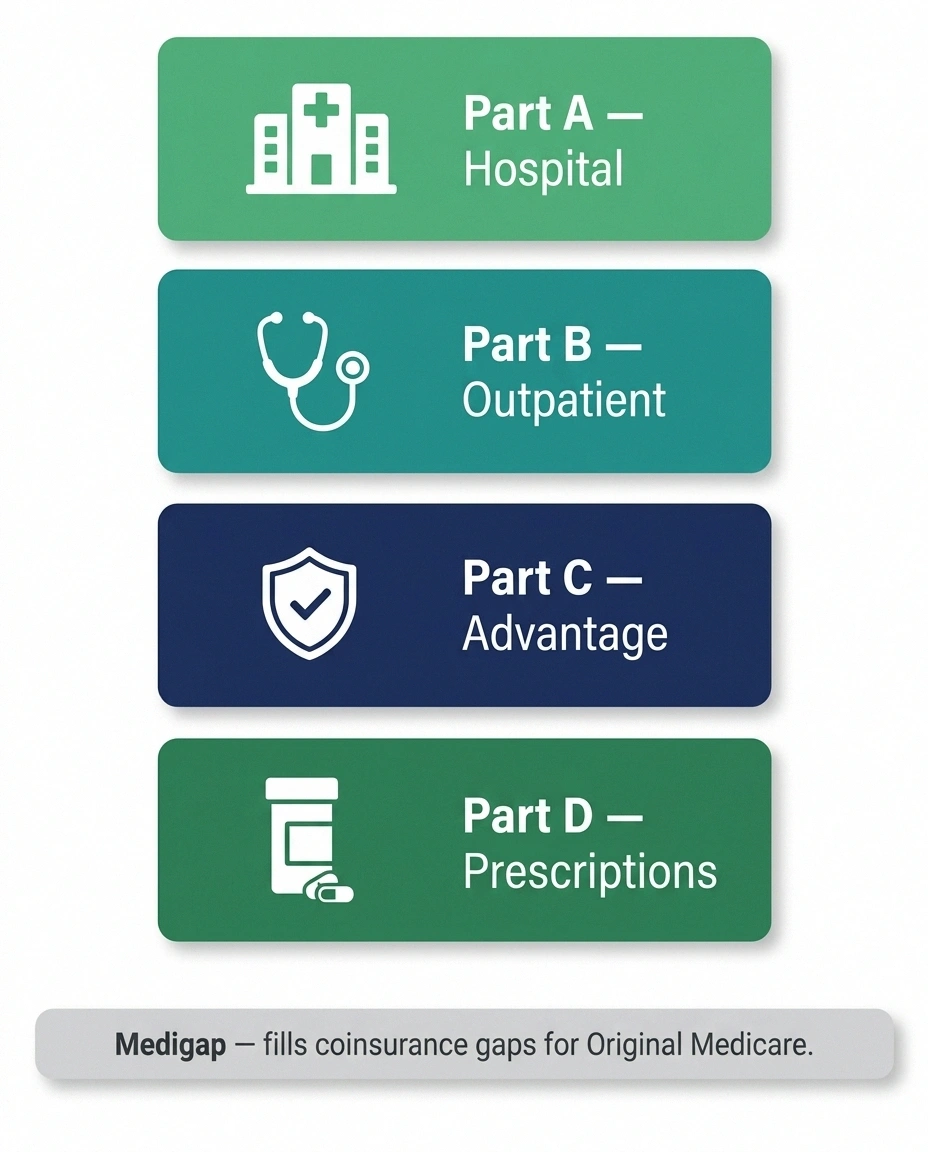
Medicare covers most neuropathy care across four parts: Part A for hospitalization, Part B for doctor visits and outpatient testing, Part D for prescriptions, and Medicare Advantage as a private bundled alternative. The 2025 $2,000 Part D out-of-pocket cap is the single biggest change for neuropathy patients in years.
Part A — Hospital Insurance. Inpatient hospital stays, skilled nursing facility (briefly), home health when you have a skilled need, hospice. Most retirees pay no premium for Part A because they paid in through payroll taxes during their working years.
For neuropathy, Part A comes into play only if you're hospitalized — for example, after a serious fall, for IV antibiotic treatment of an infected diabetic foot ulcer, or for a complication like Guillain-Barré syndrome that requires inpatient care.
Part B — Medical Insurance. This is the workhorse for chronic conditions. Part B pays for outpatient services: doctor visits, neurologist consultations, EMG and nerve conduction studies, physical and occupational therapy, durable medical equipment, B12 injections, IVIG administered in a clinic, lab work, and most office-based procedures. The 2026 Part B annual deductible is $268, and you typically pay 20% of the Medicare-approved amount after the deductible.
Part C — Medicare Advantage. A private alternative to Original Medicare that bundles Parts A, B, and usually D into one plan. Many Advantage plans add extras Original Medicare doesn't cover — limited acupuncture, chiropractic visits, dental, vision, gym memberships, sometimes over-the-counter allowances. The catch: you're locked into a network of doctors, and prior authorization is far more aggressive than under Original Medicare. For neuropathy, the network restriction matters because the best neurologist in your area may not be in-network for your plan.
Part D — Prescription Drug Coverage. Where almost all of your neuropathy medications are paid for. Gabapentin, pregabalin (Lyrica), duloxetine (Cymbalta), amitriptyline, lidocaine patches, and most other neuropathy prescriptions live here. The single biggest change in years for neuropathy patients took effect in 2025: Part D now caps your annual out-of-pocket prescription costs at $2,000. If you've been spending hundreds of dollars a month on Lyrica or capsaicin patches, this cap alone may save you thousands per year.
Medigap (Medicare Supplement). Private insurance you can buy to pay your Part B coinsurance and deductible if you stay in Original Medicare. Different lettered plans cover different things; Plan G is the most comprehensive available to people who turned 65 after 2019.
What Medicare Does Cover for Neuropathy

Let me start with the good news, because there's more here than most patients assume.
Doctor visits and specialist consultations
Your primary care visits, neurologist consultations, podiatrist visits for diabetic neuropathy with loss of protective sensation, endocrinologist visits to manage underlying diabetes, and follow-ups are all covered under Part B. You pay 20% coinsurance after meeting the deductible, or your Medigap plan or Medicare Advantage plan pays it depending on what you have.
Diagnostic testing
EMG (electromyography) and nerve conduction studies — the two tests neurologists use to confirm and characterize neuropathy — are covered under Part B when ordered by a physician. So are blood tests for the underlying causes (B12, folate, thyroid panel, A1c, autoimmune workup, heavy metals when indicated), MRI when there's suspected structural cause, and skin biopsy for small fiber neuropathy at most academic centers. Our article on neuropathy diagnosis walks through what each test does and when it's ordered.
Physical therapy and occupational therapy
Both are covered under Part B when prescribed and medically necessary. There used to be a hard annual cap; that's been replaced by a “threshold” — once your therapy spending crosses $2,410 in 2026, your therapist has to add a modifier to the claim documenting why continued therapy is medically necessary. As long as your progress notes support continuing care, therapy keeps getting covered. Our overview of physical therapy for neuropathy explains what to expect from a course of treatment.
Prescription neuropathy medications
Under Part D, the standard neuropathy drug formulary is well-covered. Generic gabapentin is almost always Tier 1 with copays of $0–$15 per month on most plans. Generic duloxetine is typically Tier 1 or Tier 2. Amitriptyline and nortriptyline (older tricyclic antidepressants used off-label for nerve pain) are generic Tier 1. Pregabalin (Lyrica) is more often Tier 3 and may require prior authorization, but the patent has expired so generic pregabalin is now widely available at lower copays. Lidocaine patches are usually covered with prior authorization. See our deep-dives on gabapentin, pregabalin, and duloxetine for what each medication does and how it's typically dosed.
$2,000
Annual Part D out-of-pocket cap
Effective 2025 for all Medicare beneficiaries. Caps total prescription spending. Spread it across the year via the Medicare Prescription Payment Plan if monthly costs are tight.
The 2025 Part D out-of-pocket cap
This deserves its own paragraph because it's the most significant Medicare change for neuropathy patients in a decade. Before 2025, there was no annual cap on Part D out-of-pocket costs — patients on expensive medications could spend $4,000, $5,000, $7,000 a year on prescriptions. Starting January 2025, that's done. The maximum any Medicare beneficiary now pays out-of-pocket for prescription drugs in a calendar year is $2,000. There's also a smoothing program (the Medicare Prescription Payment Plan) that lets you spread that $2,000 across the year in monthly installments instead of paying it in big lumps at the start of the year.
B12 injections
If you have documented B12 deficiency — and many neuropathy patients do, especially those on metformin or with absorption issues — Part B covers B12 injections administered in your doctor's office. Self-administered home injections are typically covered under Part D. We've written separately about B12 injections versus oral supplements for neuropathy.
Diabetic neuropathy: the special category
Medicare treats diabetic neuropathy more generously than other types because diabetes is a covered chronic condition under specific National Coverage Determinations. If you have diabetic peripheral neuropathy with documented loss of protective sensation:
Diabetic Neuropathy: Extra Medicare Benefits
Therapeutic shoes + 3 inserts/year
Covered annually under Part B for diabetic neuropathy with documented loss of protective sensation.
Routine foot care every 6 months
Toenail/callus care normally excluded — covered when LOPS is documented.
Annual comprehensive foot exam
By primary care doctor or podiatrist. Documented in your record.
Diabetes self-management training
10 initial hours + 2 hours/year ongoing. Make sure your doctor refers you.
All require diagnosis code E11.42 (or equivalent) with LOPS documentation.
- Therapeutic shoes. Medicare Part B covers one pair of therapeutic shoes plus three pairs of inserts each calendar year, when prescribed by your podiatrist or doctor managing your diabetes. The shoes must be billed by a Medicare-enrolled supplier. This benefit alone can save $200–$400 per year.
- Routine foot care every six months. Normally Medicare excludes “routine” foot care (toenail cutting, callus removal). For diabetic neuropathy with loss of protective sensation, those services become medically necessary and are covered every six months when performed by a podiatrist or qualified provider.
- Comprehensive foot exam annually. A documented annual foot exam by your primary care doctor or podiatrist is covered.
- Diabetes self-management training. Up to 10 hours of initial training and 2 hours per year ongoing.
If you have diabetes and any neuropathy symptoms, ask explicitly for a documented diagnosis of “diabetic peripheral neuropathy with loss of protective sensation” using ICD-10 code E11.42 (or the equivalent for your diabetes type). That diagnosis unlocks all the foot-care benefits above. Without it, those same services get denied as routine.
IVIG for CIDP and other immune neuropathies
Intravenous immunoglobulin is expensive — often $80,000–$150,000 per year — but Medicare Part B covers IVIG infusions when administered in a doctor's office or outpatient clinic for FDA-approved diagnoses, including CIDP (chronic inflammatory demyelinating polyneuropathy) and multifocal motor neuropathy. Home infusion is covered under Part D and may require prior authorization. Our article on CIDP covers when this treatment is appropriate.
What Medicare Does NOT Cover (Or Covers Inconsistently)

This is where the surprises live. Some of these gaps are explicit policy; some are gray-area items that get denied by some plans and covered by others. Knowing which is which helps you decide whether to fight a denial or just plan around the gap.
Acupuncture for neuropathy
Medicare added acupuncture coverage in 2020 — but only for chronic low back pain. Acupuncture for neuropathy specifically remains uncovered under Original Medicare. Some Medicare Advantage plans add limited acupuncture as a supplemental benefit, usually 12–20 visits per year, sometimes with a per-visit copay of $20–$40. If you want acupuncture as part of your neuropathy treatment plan and you're choosing between Original Medicare and Advantage, this is one factor to weigh. Our piece on acupuncture for neuropathy covers what the research actually shows.
Chiropractic care beyond manual spinal manipulation
Medicare covers chiropractic spinal manipulation (CPT 98940/98941/98942) when there's a documented subluxation. It does not cover other chiropractic services — no exam fees, no x-rays ordered by the chiropractor, no therapeutic exercise, no massage. If you see a chiropractor for neuropathy, expect to pay out of pocket for everything except the spinal adjustment itself.
Most stem cell therapy and PRP injections
Stem cell injections and platelet-rich plasma therapy for neuropathy are categorized as experimental or investigational by Medicare and are not covered. Plan to pay out of pocket — typically $2,500–$8,000 per session. We've written about both: stem cell therapy for neuropathy and PRP therapy for neuropathy. Read those before you consider paying out of pocket.
Watch Out For
Clinics that advertise stem cell or PRP “neuropathy reversal” rarely disclose that Medicare classifies these as experimental. Patients commonly pay $2,500–$8,000 per session out of pocket with no insurance reimbursement and limited evidence of benefit. Get a second opinion from a board-certified neurologist before committing.
Compounded pain creams
Custom-mixed topical formulations from compounding pharmacies (often containing combinations of gabapentin, ketamine, lidocaine, and other ingredients) are usually not covered by Part D because the formulations aren't FDA-approved. A few specialty plans cover certain compounds with prior authorization, but expect to pay $40–$120 out of pocket per tube as a default.
TENS units for diabetic neuropathy
Here's a frustrating one. Medicare has a National Coverage Determination that covers TENS units for chronic low back pain. For neuropathy specifically, the picture is more complicated. Some local Medicare contractors will cover a TENS unit as durable medical equipment when prescribed for diabetic neuropathy; others deny these claims as “not medically necessary.” Medicare Advantage plans vary widely. If you want one, your doctor's office should call your specific plan to ask about coverage before you order. Our article on TENS units for neuropathy covers what the units do and what to expect.
Massage therapy and most “alternative” treatments
Therapeutic massage, reflexology, reiki, and most other complementary therapies aren't covered, even when prescribed. The exception is when massage is part of a covered physical therapy or occupational therapy session billed by a licensed therapist; in that case, what you're really paying for is PT/OT, and the manual therapy is one component.
Most over-the-counter supplements
Alpha-lipoic acid, acetyl-L-carnitine, B-complex (over-the-counter), magnesium, turmeric, and other supplements are generally not covered, even when recommended by your doctor. Medicare Advantage plans sometimes include an over-the-counter allowance ($25–$100 per quarter) you can spend on covered items at participating pharmacies. Check your plan's OTC catalog. If you're researching supplements, our hub article on the best neuropathy supplements for nerve health covers what the evidence supports and at what doses.
Routine foot care for non-diabetic neuropathy
If your neuropathy is idiopathic, chemo-induced, alcohol-related, or any non-diabetic cause, Medicare generally does not cover routine podiatry — no covered toenail trimming, no routine callus care, no covered “comfort” foot maintenance. Some podiatrists will appeal individual cases when the patient has documented severe neuropathy and is at high risk of injury; these appeals succeed sometimes and fail other times.
Medicare Advantage vs. Original Medicare: Which Is Better for Neuropathy?

I get this question constantly, and the honest answer is: it depends, and the calculation is harder for neuropathy patients than for the average retiree.
Original Medicare + Medigap + Part D often wins for neuropathy patients who:
- See specialists at academic medical centers or large neurology practices
- May need IVIG, plasma exchange, specialized infusion treatments, or referrals to out-of-state experts
- Want maximum freedom to choose providers without referrals or prior authorization
- Have or expect to have multiple comorbidities requiring coordinated specialist care
Medicare Advantage often wins for neuropathy patients who:
- Live in markets with strong local plan networks that include the specialists they use
- Value the bundled extras (limited acupuncture, dental, vision, OTC allowance, gym membership)
- Are healthy enough that out-of-pocket maximums and co-pays will outweigh the Medigap premium savings
- Don't anticipate needing high-cost specialty drugs delivered by infusion (those can land patients in step-therapy and prior-auth gauntlets in Advantage plans)
The single most important rule: look at the specific plans available in your zip code, not generic comparisons. Two Advantage plans with the same name in different states often have completely different formularies, networks, and out-of-pocket maximums. Medicare's plan finder at Medicare.gov is the one tool I'd insist every patient use during open enrollment.
Appealing a Denied Claim
If Medicare denies a service you believe should be covered, you have the right to appeal — and a meaningful percentage of appeals succeed, especially at the first two levels. Here's how the process works under Original Medicare.
The 5 Levels of Medicare Appeals
Redetermination — 120-day deadline
Same Medicare contractor reviews again. ~30% succeed.
Reconsideration — 180-day deadline
Independent contractor reviews. Strong cases often win here.
ALJ Hearing — 60-day deadline
Administrative Law Judge. You can have a phone or video hearing.
Medicare Appeals Council
Last administrative level before federal court.
Federal District Court
Rare. Usually only for very high-dollar denials.
Level 1: Redetermination
You have 120 days from the date on your Medicare Summary Notice to file a redetermination request. The Medicare Administrative Contractor that processed the original claim reviews it again, ideally with new supporting documentation from your doctor. Roughly 30% of redeterminations succeed in part or in full. The form is on the back of your MSN, or you can use CMS-20027.
Level 2: Reconsideration
If redetermination fails, you have 180 days to request reconsideration by a Qualified Independent Contractor. This is a separate review by a different organization. Reconsideration is where the strongest cases — those with clear medical necessity documentation — often succeed.
Levels 3–5: ALJ, Council, Federal Court
Subsequent levels go to an Administrative Law Judge (where you can have a hearing), the Medicare Appeals Council, and ultimately federal district court. Most patients don't go past Level 2 because the dollar amounts at issue rarely justify the complexity. But for high-cost denied items — IVIG, infusion therapies, specialized DME — Level 3 ALJ hearings have a strong success rate when supported by detailed medical necessity letters from your treating physician.
Appeals Data
Roughly 30% of Level 1 redetermination appeals succeed in part or in full. Level 2 reconsideration success rates are higher when supported by a strong letter of medical necessity. Level 3 ALJ hearings have an even higher success rate for high-cost denied items like IVIG and specialized DME — but they take 6-12+ months to schedule.
Practical appeal tips
- Get a letter of medical necessity. Have your doctor explicitly state the diagnosis, the failed alternatives, and why the requested service is medically necessary in your specific case. This single document drives more successful appeals than anything else.
- Cite the relevant National Coverage Determination or Local Coverage Determination. If you're appealing a TENS denial for diabetic neuropathy, citing the LCD that covers it in your jurisdiction shifts the burden back to the contractor.
- Ask your SHIP counselor for help. Every state has a free State Health Insurance Assistance Program. SHIP counselors are trained to help with Medicare appeals and they don't charge.
- Don't miss the deadlines. 120 days for Level 1, 180 days for Level 2. A late appeal is almost always rejected without review.
If You're Under 65 with Neuropathy
Medicare isn't only for people 65 and older. If you've been on Social Security Disability Insurance for 24 months, you become Medicare-eligible regardless of age. People with end-stage renal disease and ALS have shorter waiting periods. Many patients with severe neuropathy from CIDP, advanced diabetic neuropathy, or other disabling forms of nerve damage qualify for SSDI and eventually Medicare on this basis. Our article on neuropathy disability benefits walks through the SSDI application process specifically for neuropathy.
Getting Help Navigating Medicare

The system is genuinely complicated, and you don't have to figure it out alone. Two free resources that I recommend to every patient:
1. Your State Health Insurance Assistance Program (SHIP). Free, unbiased, one-on-one Medicare counseling in every state. They'll help you compare plans, file appeals, and understand denials. Find your local SHIP at shiphelp.org or by calling 1-877-839-2675.
2. Medicare.gov plan finder. The official tool for comparing Part D and Advantage plans. You can enter your specific medications and pharmacies to see actual estimated annual costs under each available plan. Use it during open enrollment (October 15 – December 7 each year).
I'd avoid getting Medicare advice from insurance brokers who sell only one plan or one type of plan; their incentives don't always line up with yours. SHIP counselors don't sell anything.
Quick-Reference: What to Ask Your Doctor
If you're dealing with neuropathy and want to maximize what Medicare covers, these are the questions worth asking at your next appointment:
Free Help: Find Your SHIP Counselor
Every state has free, unbiased Medicare counselors through the State Health Insurance Assistance Program. They'll help you compare plans, file appeals, and understand denials. No sales pitch. Find yours at shiphelp.org or call 1-877-839-2675.
- What ICD-10 code are you using for my neuropathy? The diagnosis code drives almost everything Medicare pays for. For diabetic neuropathy, you want E11.42 (or equivalent) with documentation of loss of protective sensation.
- Am I eligible for therapeutic shoes through Medicare? If you have diabetic neuropathy, you almost certainly are.
- Can my routine foot care be coded as medically necessary because of my neuropathy? For diabetic patients with LOPS, yes. For others, probably not, but ask.
- Can we try a generic before a brand-name drug? Almost every neuropathy medication has a generic; generics are almost always cheaper under Part D.
- Could I qualify for the Medicare Prescription Payment Plan? If you have high prescription costs, spreading your $2,000 cap across the year may help with cash flow.
- Are any of my treatments billable as part of a covered service? Some “uncovered” services (like manual therapy) become covered when delivered as part of a covered PT visit.
The Bottom Line
Medicare covers more for neuropathy than most patients realize, but the system requires you to know the rules — what diagnosis codes unlock benefits, what to ask for by name, when to appeal, and which plan structure fits your specific situation. The 2025 Part D out-of-pocket cap is genuinely transformative for patients on expensive medications. Diabetic neuropathy patients have access to therapeutic shoes and routine foot care that many never claim. And for almost every gap in coverage, there's either a workaround or an appeal path worth trying.
The investment of one afternoon with a SHIP counselor pays for itself many times over for almost every patient I've worked with. If you've been navigating Medicare alone, that's the single best step you can take.
Frequently Asked Questions
Does Medicare cover gabapentin for neuropathy?
Yes. Gabapentin is covered under Medicare Part D and is almost always on Tier 1 of plan formularies, meaning it has the lowest copay. Most patients pay between $0 and $15 per month for generic gabapentin under standard Part D plans.
Will Medicare pay for nerve conduction studies?
Yes, when ordered by a physician. Nerve conduction studies and EMG (electromyography) are covered under Medicare Part B as medically necessary diagnostic tests when there's a clinical indication of neuropathy. You pay 20% coinsurance after the Part B deductible unless you have Medigap or Medicare Advantage covering that portion.
Does Medicare cover acupuncture for neuropathy?
No, not under Original Medicare. Medicare added acupuncture coverage in 2020, but only for chronic low back pain. Some Medicare Advantage plans add acupuncture as a supplemental benefit, but coverage varies by plan and is usually limited to 12 to 20 visits per year.
What's the 2026 Medicare Part B deductible?
The Part B deductible for 2026 is $268. After you meet that, Medicare typically pays 80% of the approved amount for covered services and you (or your Medigap plan) pay the remaining 20% coinsurance.
How does the new Part D out-of-pocket cap work?
Beginning in 2025, Medicare Part D caps your annual out-of-pocket prescription drug costs at $2,000 per calendar year. Once you hit that amount, you pay nothing for covered prescriptions for the rest of the year. Medicare also offers a smoothing program called the Medicare Prescription Payment Plan that lets you spread costs into monthly installments instead of paying them in lumps.
Does Medicare cover therapeutic shoes for neuropathy?
Yes, but only for diabetic neuropathy with documented loss of protective sensation. Medicare Part B covers one pair of therapeutic shoes plus three pairs of inserts each calendar year for qualifying patients, when prescribed by your podiatrist or the doctor managing your diabetes. The shoes must be supplied by a Medicare-enrolled supplier.
How do I appeal a Medicare denial?
You have 120 days from the date on your Medicare Summary Notice to file a Level 1 redetermination. If denied at Level 1, you have 180 days to request a Level 2 reconsideration by an independent contractor. Get a detailed letter of medical necessity from your doctor, and contact your free State Health Insurance Assistance Program (SHIP) for help. Many appeals succeed at Levels 1 or 2, especially with strong documentation.
Are stem cell injections for neuropathy covered by Medicare?
No. Stem cell therapy and platelet-rich plasma injections for neuropathy are categorized as experimental or investigational by Medicare and are not covered. Patients pursuing these treatments typically pay $2,500 to $8,000 per session out of pocket. Talk to your doctor about evidence-based alternatives that are covered before considering experimental treatments.


