
One of the most common things I hear in our support group is “I don't know if this is my neuropathy or restless legs — but it's keeping me awake every night.” For many people the two conditions sit so close together in symptoms and in shared causes that even careful clinicians struggle to draw a clean line between them. And yet the distinction matters, because the treatments diverge in ways that can make the difference between sleeping through the night and not.
I'm Janet Ellis. I am a community advocate who has lived with neuropathy for years; I am not a doctor or a sleep specialist. What I can do is translate what the medical literature actually says about the overlap between restless legs syndrome (RLS) and peripheral neuropathy, and help you frame the conversation you might have with your own clinician. If you have been told you have one, neither, or both, this is meant to give you a clearer map.
What Restless Legs Syndrome Actually Is
Restless legs syndrome — now sometimes called Willis-Ekbom disease in the medical literature — is a sleep-related sensory-motor disorder. People with RLS describe an uncomfortable urge to move their legs, usually accompanied by sensations that are hard to put words to: creepy-crawly, fizzy, buzzing, deep, “like ginger ale in my bones.” The sensations come on at rest, especially in the evening or at night, and movement temporarily relieves them. It is the relief-from-movement piece that defines RLS more than any other feature.
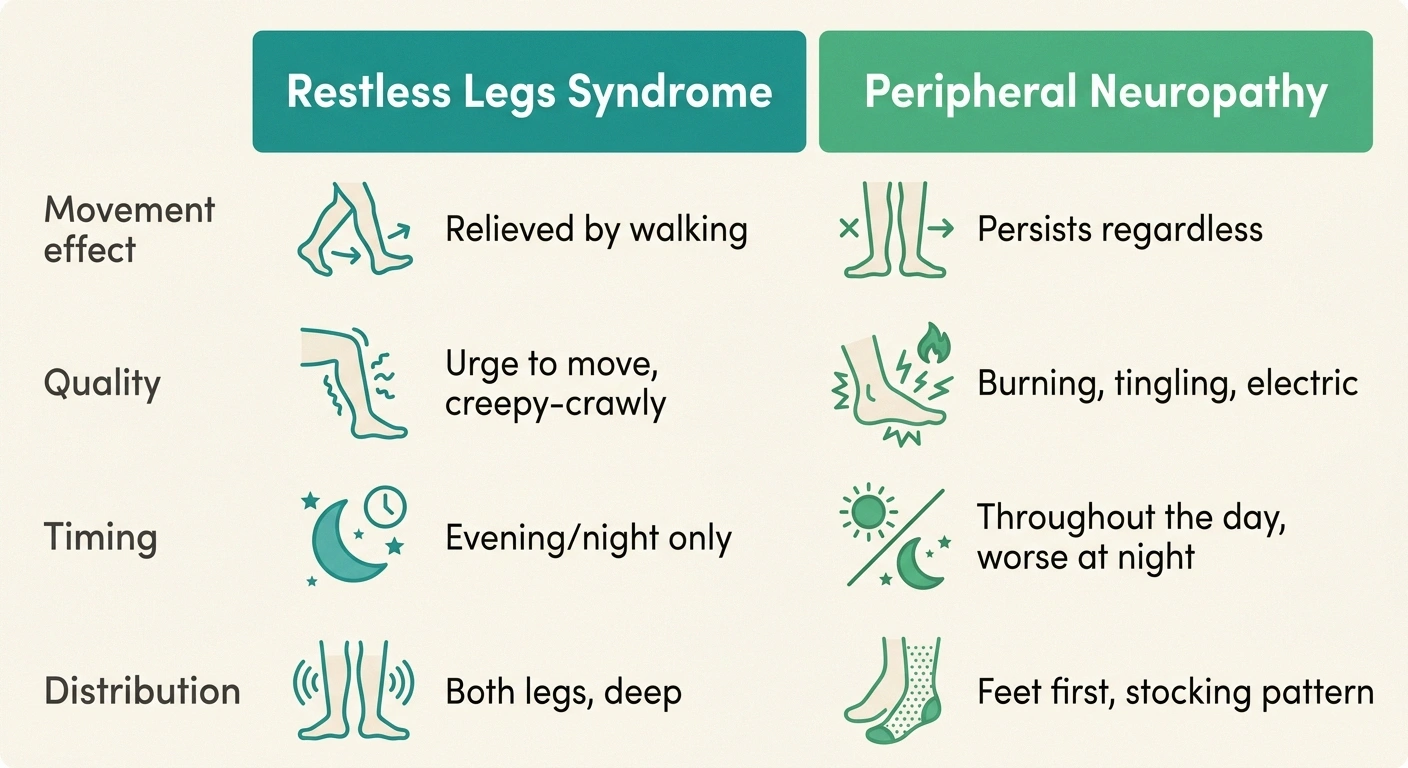
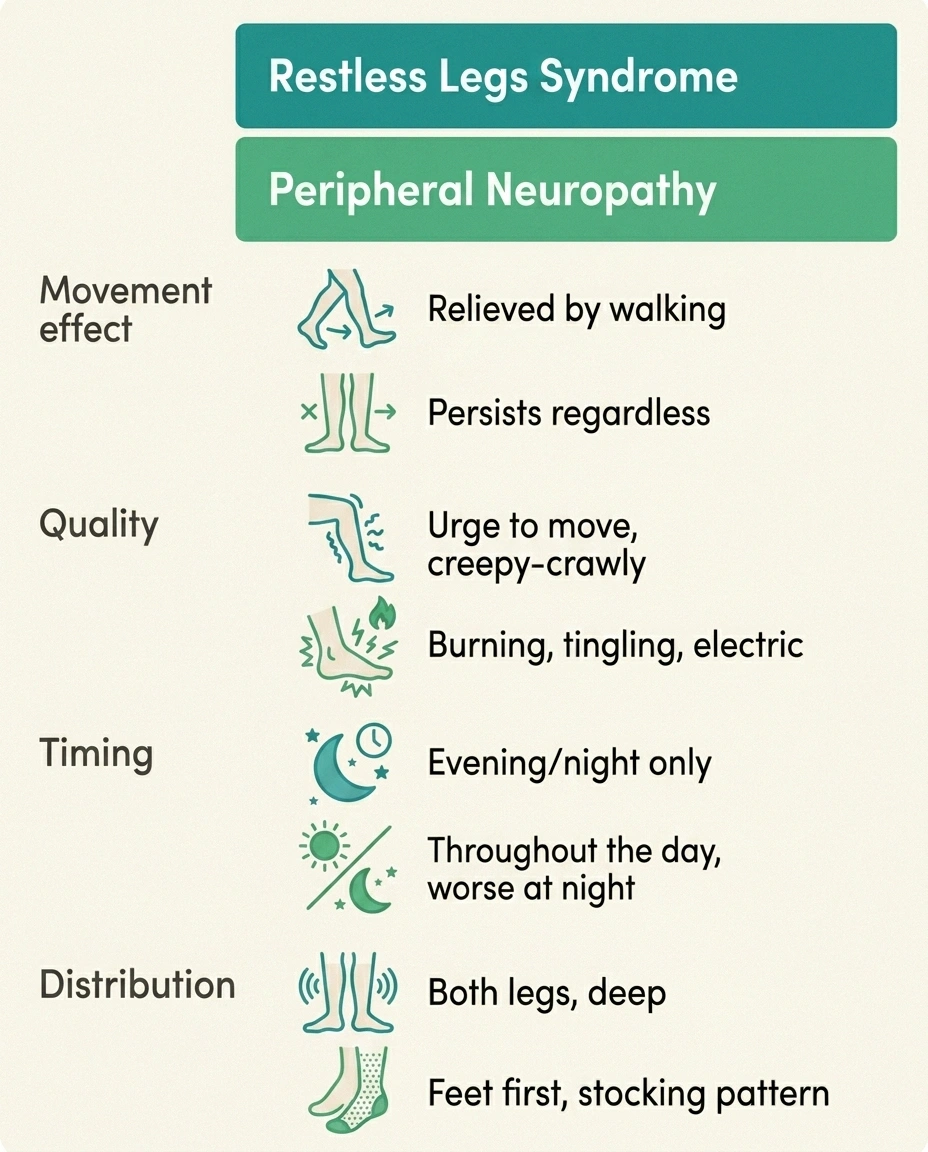
The single most useful test for telling RLS apart from neuropathy is the movement effect. RLS sensations are relieved by walking, stretching, or moving the legs. Neuropathy sensations are not. The two conditions can also coexist — and when they do, one well-chosen medication and an iron-status check often address both.
The International Restless Legs Syndrome Study Group has formal diagnostic criteria — all five must be met:
- An urge to move the legs, usually accompanied by uncomfortable sensations
- Symptoms begin or worsen during rest or inactivity
- Symptoms are partially or completely relieved by movement
- Symptoms are worse in the evening or at night
- The symptoms are not solely explained by another medical or behavioral condition
Notice the fifth point. It is built into the diagnostic criteria precisely because conditions like neuropathy can mimic RLS, and a proper diagnosis requires ruling out (or carefully accounting for) the lookalikes.
How Neuropathy Symptoms Differ From RLS

Peripheral neuropathy, especially the small-fiber type, can produce sensations that overlap with RLS — burning, tingling, “pins and needles,” a vague discomfort in the feet and lower legs that often gets worse at night. The reason neuropathy gets worse at night is its own topic, but it sets up the practical confusion. Both conditions are at their worst when you finally lie down.
RLS Diagnostic Criteria (IRLSSG — All 5 Must Be Met)
RLS vs Peripheral Neuropathy — Practical Discriminators
Timing: Evening/night, often absent by day
Feel: Urge to move, “creepy-crawly,” buzzy
Location: Deep in legs, both sides
Workup: Clinical only; no nerve-study finding
Timing: Often constant; night-time worse
Feel: Burning, tingling, pins/needles, numb
Location: Distal feet first (“stocking-glove”)
Workup: EMG/NCS often abnormal; reflexes reduced
Here are the practical features that help separate them:
- Movement effect. This is the most useful single discriminator. RLS sensations get better when you walk, stretch, or move your legs. Neuropathy sensations don't — they often persist regardless of position, and walking on a flare can make burning worse. If standing up and pacing the kitchen reliably brings relief, that is RLS leaning. If it doesn't help at all, that points away.
- Quality of the sensation. RLS is typically described as an “urge to move” with a deep, restless, crawling quality — patients reach for verbs like “creep” and “shimmer” and metaphors like fizzy water. Neuropathy is more often described with adjectives — burning, tingling, electric, numb. Both can be uncomfortable in their own ways, but the words people choose differ.
- Timing. RLS has a strong circadian pattern: nearly absent during the day, worse in the evening, worst at night. Neuropathy can be present throughout the day with night-time worsening, but it rarely disappears completely during waking hours. If symptoms are essentially absent at noon and unbearable at midnight, that is RLS.
- Location. RLS is usually deep in the legs (often the calves or thighs) and almost always involves both legs, though one side may be worse. Neuropathy is more often distal — feet first, then toward the ankles, in the classic “stocking” pattern. A symmetric distal pattern points to neuropathy; a more diffuse, deeper, both-legs pattern points to RLS.
- Objective testing. Neuropathy often has measurable nerve conduction abnormalities or small-fiber findings on skin biopsy. RLS has no diagnostic blood test or nerve study — it is a clinical diagnosis based on the criteria above and on the response to treatment.
- Reflexes and sensation on exam. Long-standing neuropathy often shows reduced reflexes (especially the Achilles) and a measurable sensory deficit. RLS does not change these exam findings on its own.
Our guide to what neuropathy actually feels like walks through the broader sensory vocabulary that patients use; reading both descriptions side by side often clarifies which fits.
The Overlap Problem — They Can Coexist
Here is what makes the conversation messier: RLS and peripheral neuropathy are not mutually exclusive. The published literature shows RLS prevalence in people with peripheral neuropathy ranging anywhere from about 5 percent to 37 percent depending on how the conditions are defined and how the studies are done. The plain-language version: a meaningful minority of people with neuropathy also have RLS, and the symptoms can stack on top of each other.
Several mechanisms might explain the connection. Damaged small nerve fibers can themselves generate restless sensations that meet RLS criteria. Both conditions share underlying risk factors — diabetes, chronic kidney disease, B-vitamin deficiencies, low iron stores, and some autoimmune conditions all raise the risk of both. And the same dorsal-horn and central-nervous-system circuits that go awry in one condition can be affected in the other.
This is why a careful evaluation matters. Calling something “neuropathy” when it is actually RLS — or vice versa — leads to wasted time on treatments that target the wrong condition. Treating only one when both are present leaves the patient half-better and confused about why.
The Iron Question

One of the clearest mechanistic findings in RLS research is the role of iron. Specifically, low brain iron — which may exist even when blood ferritin levels look acceptable by general standards — is strongly associated with RLS and often drives the condition. The treatment threshold for RLS purposes is higher than for general health: many sleep specialists target a serum ferritin above 75 to 100 ng/mL (and transferrin saturation above 20 percent) for RLS patients, not the “above 30” range that's considered normal for most labs.
For RLS, many sleep specialists target serum ferritin above 75-100 ng/mL (and transferrin saturation >20%) — much higher than the >30 ng/mL “normal” cutoff most labs use.
Iron repletion resolves RLS in a meaningful percentage of cases without further medication — making this the cheapest, highest-leverage first step.
If you are working through a possible RLS diagnosis and your ferritin has not been checked recently, it is one of the first things to ask about. Iron repletion — oral if tolerated, intravenous for those who can't absorb oral iron — resolves RLS in a meaningful percentage of cases without needing other medications. Our guide to interpreting neuropathy blood test results covers what these labs actually mean.
Iron is also relevant to certain types of neuropathy, but in a different way. Iron-deficiency anemia per se doesn't typically cause peripheral neuropathy, but the broader nutritional context — particularly B12 status — overlaps with neuropathy risk. Bringing both lab pictures together is part of a thorough workup when symptoms are unclear.
Treatments That Target RLS Specifically

If you have been diagnosed with RLS (with or without coexisting neuropathy), several treatment categories exist. None should be chosen lightly — each has a real trade-off — and the decision belongs with a clinician who knows your full picture.
Long-term dopamine agonists (pramipexole, ropinirole) can paradoxically worsen RLS over months to years — pushing symptoms earlier in the day and intensifying them. This is now well documented enough that most specialists have moved alpha-2-delta ligands (gabapentin enacarbil, gabapentin, pregabalin) to first-line.
If your dopamine agonist seems to be working less well over time — talk to your prescriber. Don't stop abruptly.
When Both Are Present — The Joint Playbook
Iron Repletion
For RLS patients with ferritin below the RLS-specific threshold (75-100 ng/mL), oral iron supplementation taken every other day with vitamin C (which improves absorption), or intravenous iron for those who can't tolerate or absorb oral, is now considered first-line by many sleep specialists. This is non-controversial and often produces durable benefit if iron stores were truly low.
Alpha-2-Delta Ligands (Gabapentin, Pregabalin, Gabapentin Enacarbil)
These medications — sometimes called “gabapentinoids” — have become the preferred first-line drug class for RLS in many guidelines, particularly because they don't carry the augmentation risk that the dopamine agonists carry. Gabapentin enacarbil (Horizant) is specifically FDA-approved for RLS. Plain gabapentin and pregabalin are often used off-label with similar effect.
There is an obvious convenience here for people with both RLS and neuropathy: these are the same medications used for neuropathic pain. One prescription can target both conditions if the dose is set thoughtfully.
Dopamine Agonists (Pramipexole, Ropinirole, Rotigotine)
For many years, dopamine agonists were first-line for RLS, and they still work well for many people in the short term. The major concern is “augmentation” — a paradoxical worsening of symptoms over months to years of use, where the medication that initially helped starts to make the condition more severe and to push symptoms earlier in the day. Augmentation is now well documented enough that many sleep specialists have moved dopamine agonists to second-line for new patients, reserving them for cases where alpha-2-delta ligands haven't worked.
If you are currently on a dopamine agonist and find your symptoms are worsening or appearing earlier than they used to, augmentation is the first thing to discuss with your prescribing clinician — not to stop the medication abruptly, but to plan a careful taper and transition to an alternative.
Other Options
Low-dose opioids (such as oxycodone or methadone) are used in severe refractory RLS, with appropriate caution. Benzodiazepines are occasionally added for sleep but do not treat the underlying RLS. Lifestyle measures — avoiding caffeine and alcohol in the evening, regular gentle exercise, stretching before bed, magnesium (in some cases), and managing sleep hygiene — help on the margins.
When Both Conditions Are Present — The Joint Approach
If a careful evaluation confirms both peripheral neuropathy and RLS, the practical approach often involves a few coordinated moves:
- Check and correct iron status with the RLS-specific ferritin threshold in mind. This is the cheapest intervention with the highest potential return.
- Address any underlying drivers shared by both conditions — diabetes management, B12 repletion if low, alcohol moderation, kidney function follow-up if relevant.
- Choose a medication that works for both when possible. Gabapentin or pregabalin at an appropriate dose can address both conditions; this avoids stacking multiple prescriptions.
- Sleep hygiene as a true intervention. Both conditions punish poor sleep. A consistent bedtime, a cool dark room, no caffeine after lunch, and a deliberate wind-down routine matter more here than in many other settings. Our guide to setting up a neuropathy-friendly bedroom applies directly.
- Symptom diary to track which symptoms respond to which interventions. When two conditions overlap, it is genuinely hard to attribute improvement (or worsening) without a written log. Our guide to keeping a neuropathy symptom diary covers a simple template.
Things That Worsen Both Conditions

A small number of lifestyle and medication factors can flare either or both:
- Most SSRI and SNRI antidepressants (duloxetine is more nuanced)
- Antihistamines, especially diphenhydramine (Benadryl, OTC sleep aids, PM pain formulas)
- Dopamine-blocking anti-nausea drugs (metoclopramide, prochlorperazine)
- Certain antipsychotics
- Alcohol in the evening
- Caffeine after lunch
If you're starting RLS treatment, review your full medication list for these contributors first.
- Caffeine, especially in the afternoon and evening. The half-life is long enough that an afternoon coffee can affect midnight sleep onset and RLS severity.
- Alcohol. Both conditions are sensitive to alcohol; for RLS, even modest evening drinking can intensify symptoms.
- Certain antidepressants, particularly the SSRIs and many SNRIs, can worsen RLS. The notable exception is duloxetine, which is more nuanced — useful for neuropathic pain but capable of aggravating RLS in some patients. Bupropion is one antidepressant that does not typically worsen RLS and is sometimes preferred when both conditions are present.
- Antihistamines, especially the older diphenhydramine-based products often found in over-the-counter sleep aids and PM-formulation pain relievers. These can dramatically worsen RLS.
- Some anti-nausea medications (especially the dopamine-blocking ones like metoclopramide and prochlorperazine).
- Magnesium-poor diets for some people; magnesium may help both conditions modestly, though evidence is mixed.
- Sleep deprivation itself, which is a vicious feedback loop — bad sleep worsens both conditions, which worsens sleep further.
How to Frame the Conversation With Your Clinician
If you suspect you have one or both conditions, a few practical pieces help the appointment go better:
- Bring a one-week symptom log recording when the symptoms appear, what they feel like, what makes them better or worse, and how they affect sleep.
- Try the movement test honestly in the week before your appointment. Does standing up and walking around for two or three minutes reliably relieve the sensations, or not? The answer is one of the most useful pieces of information you can bring.
- List all medications and supplements, including over-the-counter sleep aids and PM-formulation pain relievers. Many people don't realize their nightly Benadryl or Tylenol-PM may be making things worse.
- Recent lab work if you have it — particularly ferritin, transferrin saturation, B12, folate, fasting glucose, kidney function, and TSH (low thyroid contributes to neuropathy).
- Ask specifically: “Could this be RLS, neuropathy, or both? What testing or trial would help us figure that out?” That phrasing keeps the conversation open instead of pre-committing to one diagnosis.
The Honest Truth About Living With Both
For people who have both conditions, the most useful insight is that you do not have to figure out which sensation belongs to which condition every time. The goal is functional — sleep better, walk safely, get through the day with less suffering — and the same handful of tools serve both. Iron when it's low. A medication that helps both, dosed thoughtfully. Sleep hygiene treated like a real intervention. Avoidance of the things that worsen both. A movement habit that helps RLS and supports nerve health. Our guide to building a pain management toolkit at home applies directly here, and most of the tools work for both conditions.
The frustrating thing about overlap conditions is that simple stories rarely fit them. The hopeful thing is that the same patience, observation, and willingness to iterate that you bring to one of them tends to pay off for both.
Frequently Asked Questions
What is the difference between RLS and peripheral neuropathy?
The single most useful distinguishing feature is the response to movement. RLS sensations are relieved by walking, stretching, or moving the legs; neuropathy sensations are not. RLS is also typically a deep, evening-and-night phenomenon with an urge to move; neuropathy is often a more persistent burning or tingling that tends to be worst distally in the feet. Both can worsen at night, both can disrupt sleep, and the two conditions often coexist in the same person.
Can peripheral neuropathy cause restless legs syndrome?
The two conditions are linked, but the exact relationship is not fully settled. RLS occurs more commonly in people with peripheral neuropathy than in the general population, and they share several underlying causes — diabetes, kidney disease, B12 deficiency, and low iron among them. Damaged small nerve fibers may also produce sensations that meet RLS criteria. Whether neuropathy directly causes RLS or whether the two are parallel consequences of shared risk factors is debated.
What is the first-line treatment for restless legs syndrome?
For most patients, current guidelines favor checking and correcting iron stores first, and then using an alpha-2-delta ligand (gabapentin enacarbil, gabapentin, or pregabalin) if medication is needed. Dopamine agonists, which were first-line for many years, have been moved to second-line by many specialists because of the risk of augmentation over time. The specific choice depends on individual factors and should be made with a clinician familiar with your case.
What should my ferritin level be if I have RLS?
Many sleep specialists target a serum ferritin above 75 to 100 ng/mL for RLS patients, which is higher than the general “above 30” cutoff considered normal by most labs. Transferrin saturation above 20 percent is also typical. If your ferritin is below the RLS-specific threshold, iron repletion is often the first intervention tried, and it resolves the condition for a meaningful percentage of patients without further medication.
Does gabapentin treat both neuropathy and RLS?
Yes, in many cases. Gabapentin and related medications (pregabalin, gabapentin enacarbil) are used for both peripheral neuropathic pain and restless legs syndrome. For patients with both conditions, this overlap can mean one well-dosed medication addresses both — a real practical advantage. The dose and timing may need adjustment depending on which condition is more dominant.
What medications make restless legs syndrome worse?
Several common medications can worsen RLS: most SSRI and SNRI antidepressants, antihistamines (especially diphenhydramine, the active ingredient in many over-the-counter sleep aids and PM pain formulas), some anti-nausea medications (metoclopramide, prochlorperazine), and certain anti-psychotics. If you are starting RLS treatment, reviewing your full medication list for these contributors is a productive step.
Can RLS go away on its own?
Secondary RLS — RLS caused by an identifiable, correctable factor like iron deficiency, pregnancy, kidney disease, or a triggering medication — can resolve completely when the underlying cause is addressed. Primary RLS, which often runs in families and has no identifiable trigger, tends to be a long-term condition that is managed rather than cured. Even primary RLS can wax and wane over years, sometimes improving for stretches without explanation.
How is RLS diagnosed if there is no blood test for it?
RLS is a clinical diagnosis based on the five International Restless Legs Syndrome Study Group criteria — urge to move the legs, worse at rest, relieved by movement, worse in the evening or at night, and not solely explained by another condition. A careful history is the diagnostic test. Blood work is used to identify underlying contributors (iron, B12, kidney function), and a sleep study may be done in some cases, but neither establishes the diagnosis on its own.


