Does Neuropathy Spread? How Nerve Damage Progresses
It starts in your toes — tingling, numbness, maybe some burning. Then one day you notice it in your entire foot. A few months later, the other foot joins in. Now your calves are tingling too. The question that creeps into every neuropathy patient's mind eventually: “Is this going to keep spreading?”
It's a frightening question, and you deserve a straight answer. The short version: neuropathy doesn't “spread” in the way an infection spreads — it's not contagious, and one damaged nerve doesn't infect its neighbor. But it does progress, and understanding how and why that progression happens gives you the power to do something about it.
Why Neuropathy Seems to Spread
When people say their neuropathy is “spreading,” they're usually describing a real phenomenon — symptoms appearing in new body areas over time. But what's actually happening isn't nerve damage jumping from one nerve to the next. It's a systemic process affecting your entire peripheral nervous system, with the longest, most vulnerable nerves showing damage first.
Think of your peripheral nerves like a network of electrical cables running from your spinal cord to every part of your body. The cables running to your toes are the longest — some stretch over three feet. The cables running to your fingertips are the next longest. When something is damaging all the cables simultaneously (like high blood sugar or a toxin), the longest ones fail first, simply because they have more length to maintain and more surface area exposed to the damaging agent.
This is why the National Institute of Neurological Disorders and Stroke describes most neuropathies as “length-dependent” — symptoms develop first at the farthest points from the brain and, in severe cases, “spread upward toward the central parts of the body.” It's not one nerve infecting another. It's all your nerves being damaged by the same cause, with the longest ones reaching their breaking point first.
The Stocking-and-Glove Pattern: Neuropathy's Classic Progression
The most common progression pattern has a name: “stocking-and-glove distribution.” It's called that because the affected areas mirror where you'd wear stockings and gloves — the feet and hands, progressing up the legs and arms over time.
First symptoms — tingling, numbness, or burning. Often dismissed as “getting older.”
Symptoms become constant rather than intermittent. Both feet typically affected.
The “stocking-and-glove” pattern emerges. Hands affected because fingertip nerves are next-longest.
Advanced — not everyone reaches this stage. Abdomen may develop patchy numbness.
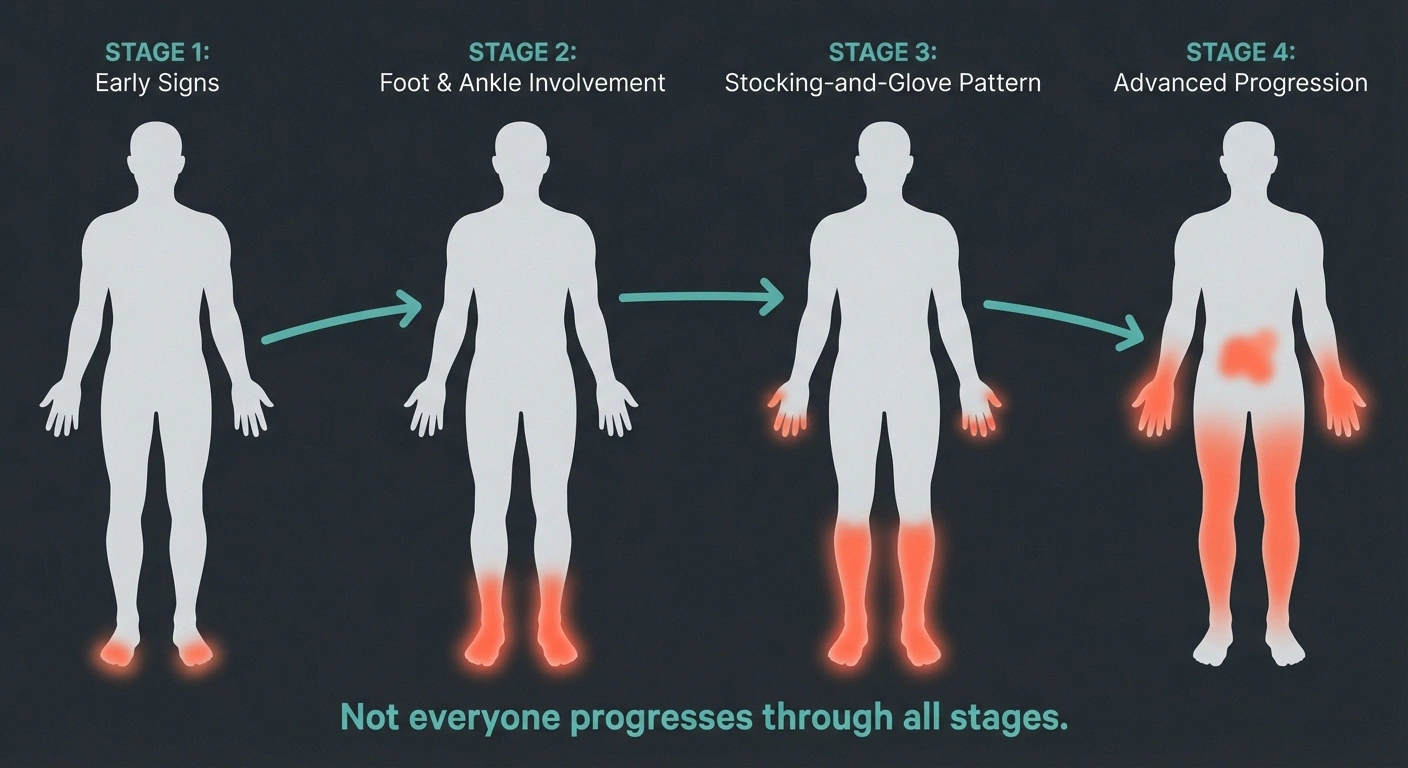
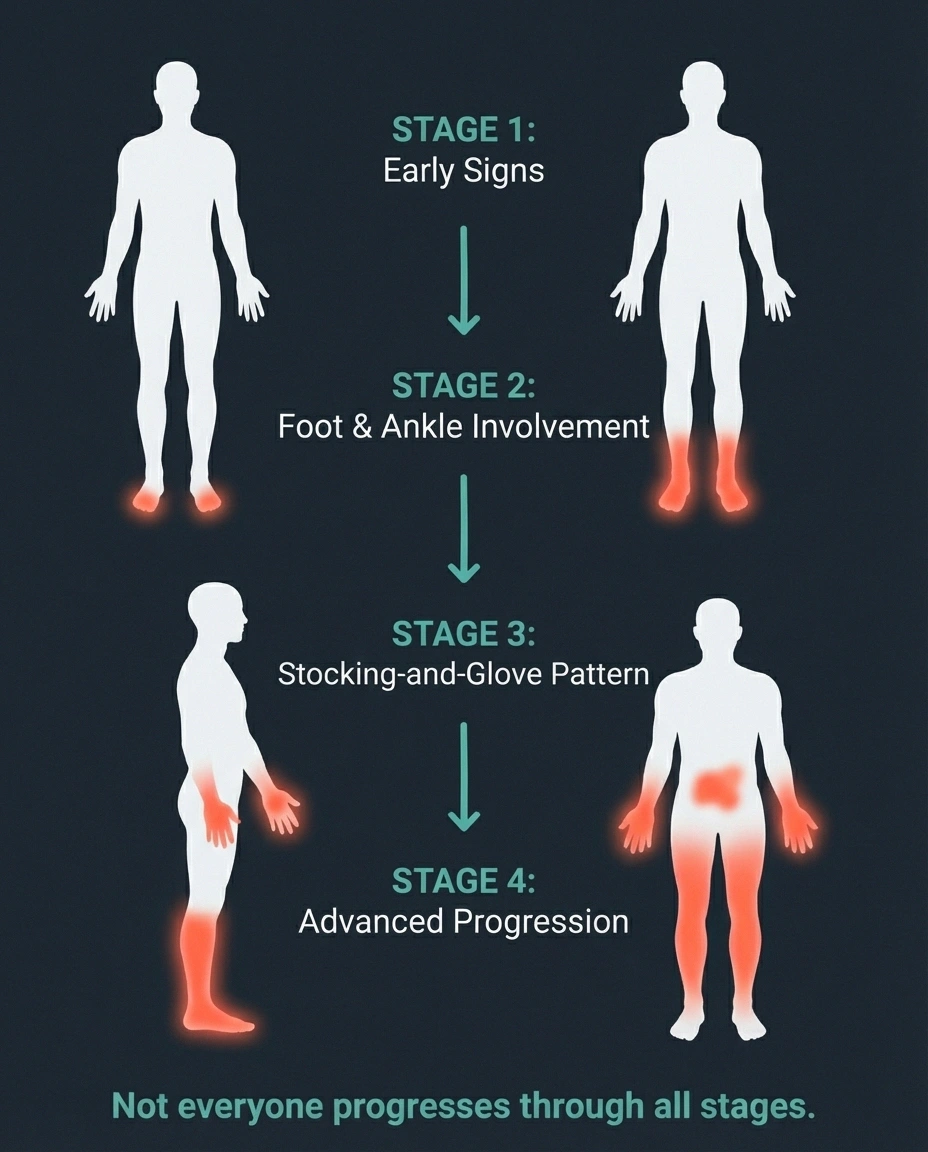
Here's how it typically unfolds:
Stage 1: Toes and balls of the feet. This is where most people first notice something wrong — numbness, tingling, or burning confined to the toes or the bottom of the foot. Many people dismiss this as “bad circulation” or “getting older.” At this point, only the very tips of the longest nerves have reached the damage threshold.
Stage 2: Entire foot and ankle. As the underlying cause continues, shorter nerve endings start failing. Symptoms extend from the toes to encompass the whole foot and ankle area. You might notice symptoms are now constant rather than intermittent. For a detailed look at staging, see our guide on the stages of neuropathy.
Stage 3: Lower legs and fingertips. When symptoms reach mid-calf level, the fingertips often start showing symptoms too — because the nerves to your fingertips are now the next-longest in the affected range. This is the “stocking-and-glove” pattern becoming visible.
Stage 4: Hands and upper limbs. In more advanced cases, symptoms climb further up the legs and extend into the hands and wrists. The front of the abdomen may develop a patch of numbness when the nerves from the trunk reach the same length threshold.
Not everyone progresses through all these stages. Many people's neuropathy stabilizes at Stage 1 or 2, especially if the underlying cause is identified and treated. The progression is not inevitable — it depends entirely on what's causing the damage and whether that cause can be controlled.
What Determines How Fast Neuropathy Progresses
The rate of progression varies enormously — from weeks to decades — depending on the cause. Understanding your specific situation helps predict what to expect.
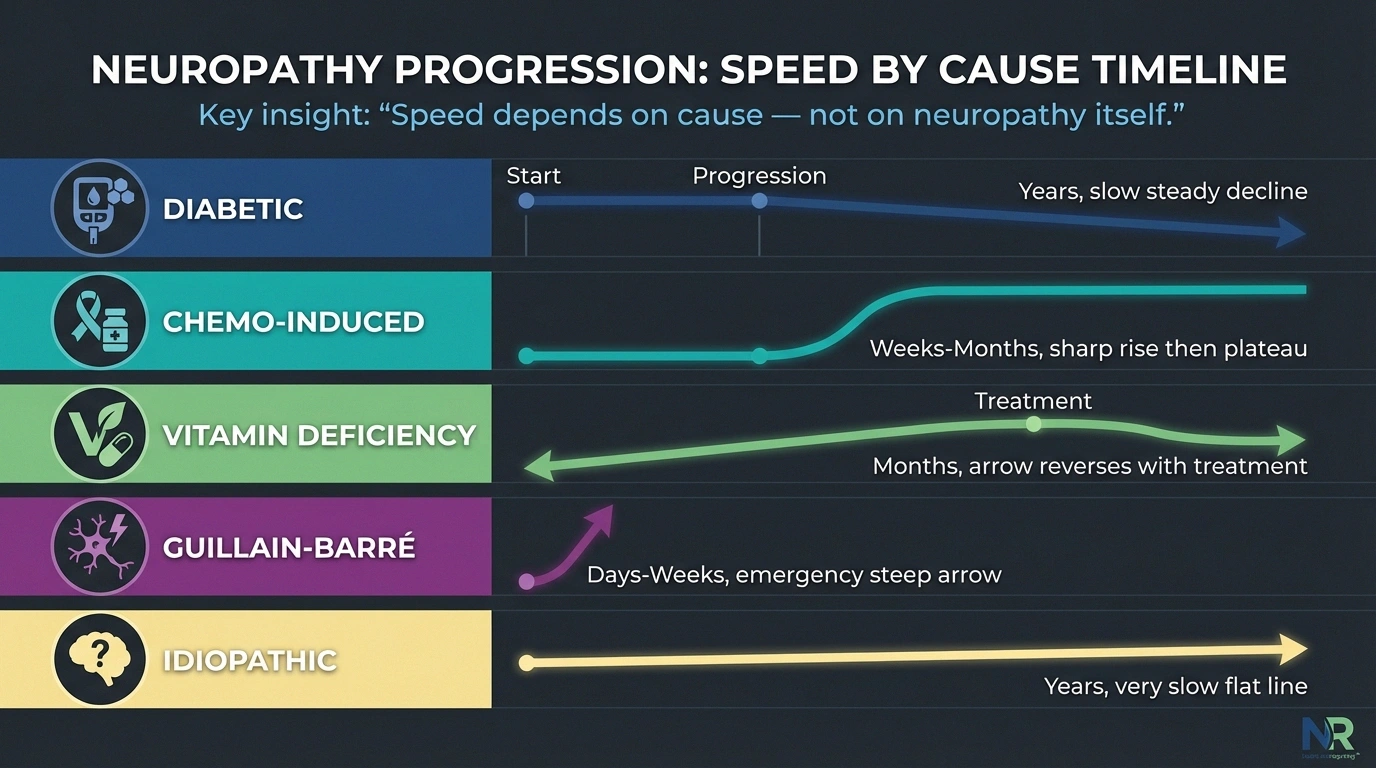
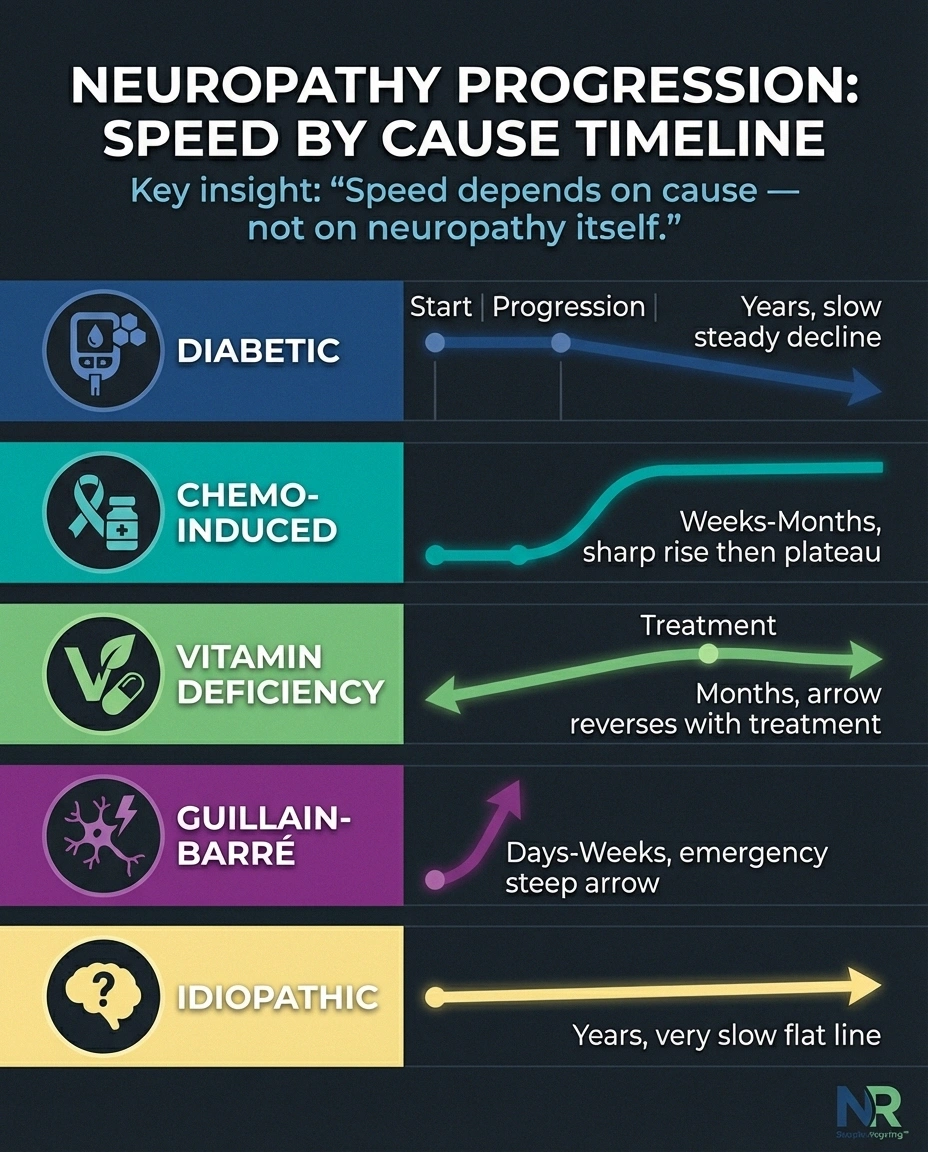
Diabetic neuropathy typically progresses slowly over years. Cleveland Clinic research indicates that peripheral neuropathy affects 15-50% of people with Type 2 diabetes who've had diabetes for at least 10 years. Better blood sugar control significantly slows this progression. Many people with well-managed diabetes maintain stable, mild neuropathy for decades.
Chemotherapy-induced neuropathy can develop rapidly — sometimes within weeks of starting treatment — and may stabilize or partially improve after chemotherapy ends. However, some people experience continued worsening for months after the last dose (a phenomenon called “coasting”).
Vitamin deficiency neuropathy progresses gradually as long as the deficiency persists, but can stabilize and often partially reverse once the vitamin is replenished. B12 deficiency neuropathy caught early has an excellent prognosis.
Autoimmune neuropathies like Guillain-Barré syndrome can progress extremely rapidly — over days to weeks — because the immune system is actively attacking nerve tissue. This is a medical emergency. Chronic autoimmune neuropathies (like CIDP) progress more gradually but can fluctuate with flares and remissions.
Idiopathic neuropathy (no known cause) tends to progress very slowly, and many people report years of stability. Research suggests that most idiopathic neuropathy follows a benign course, though the uncertainty can be emotionally difficult.
Non-Length-Dependent Neuropathy: When the Pattern Is Different
Not all neuropathy follows the neat stocking-and-glove pattern. Some forms affect nerves in patterns that can seem random.

Mononeuropathy affects a single nerve — carpal tunnel syndrome is the classic example, compressing the median nerve in the wrist. Ulnar neuropathy at the elbow is another common form. These don't “spread” to other nerves, though you can develop mononeuropathy in multiple separate nerves (called mononeuritis multiplex), which can look like spreading.
Proximal neuropathy starts in the hips, thighs, or buttocks rather than the feet. It's most common in Type 2 diabetes and typically affects one side of the body. While it rarely spreads to the other side, it can cause severe pain and significant muscle weakness in the affected area.
Small fiber neuropathy sometimes presents in non-length-dependent patterns — affecting the trunk, face, or scattered patches of skin. This can be confusing because it doesn't follow the classic progression from feet upward. If your symptoms don't fit the typical pattern, small fiber neuropathy is worth discussing with your neurologist.
Vasculitic neuropathy follows the pattern of blood vessel inflammation rather than nerve length, and can affect seemingly random nerves. This is a serious condition that requires aggressive immunosuppressive treatment.
Can You Stop Neuropathy from Progressing?
This is the question that really matters, and the answer is often yes — if you address the underlying cause. The concept is simple: stop what's damaging the nerves, and the damage stops accumulating.
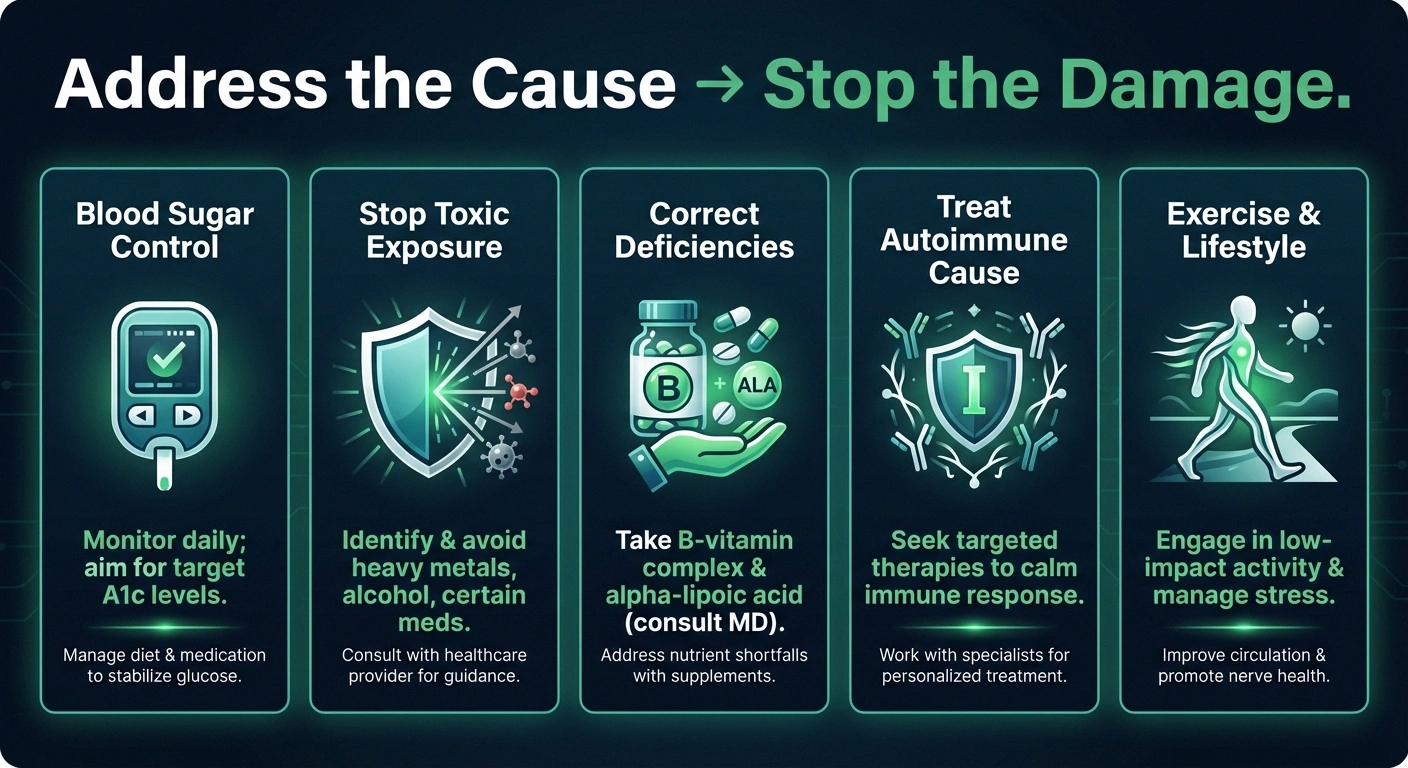
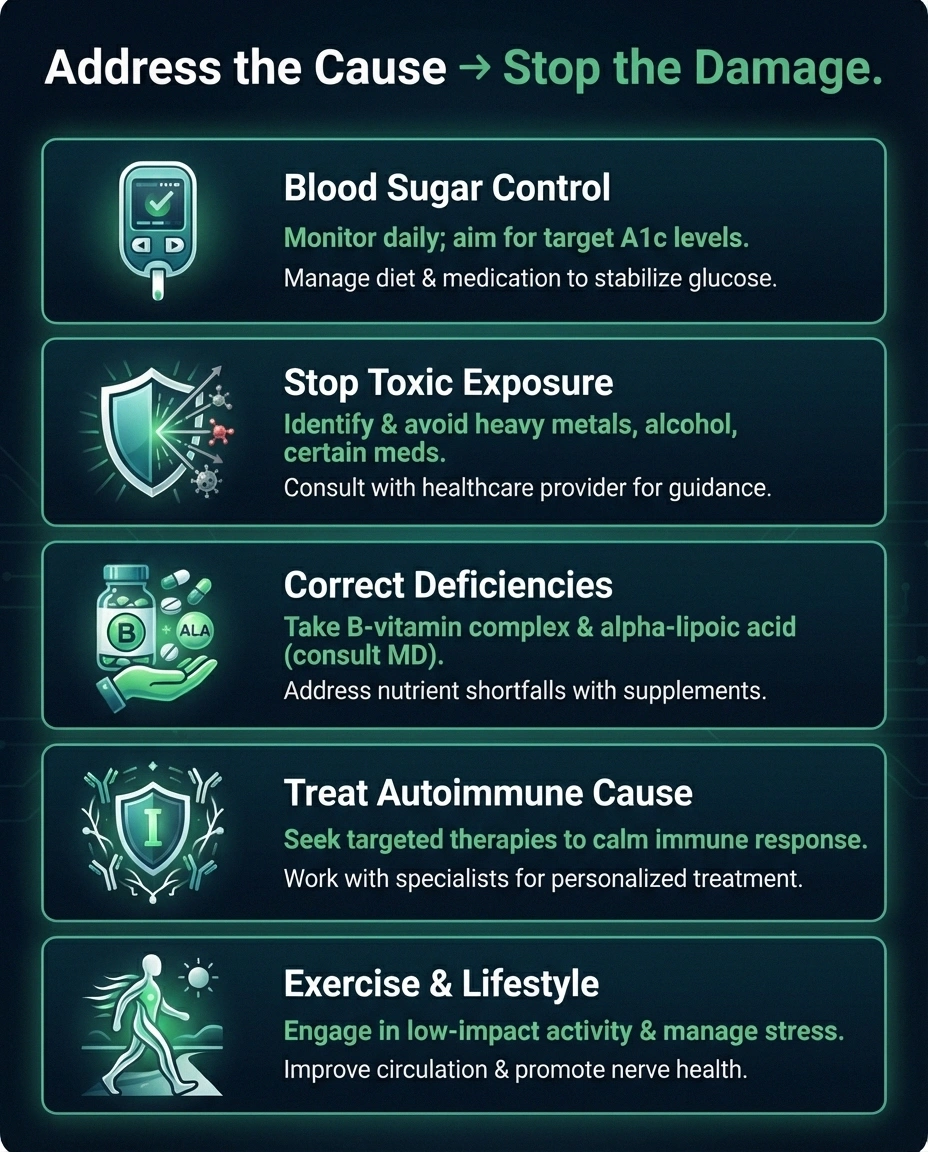
Blood sugar control is the most impactful intervention for diabetic neuropathy. The Diabetes Control and Complications Trial demonstrated that tight glycemic control reduced neuropathy risk by 60-70%. Even after neuropathy develops, improved blood sugar management slows progression significantly.
Stopping the toxic exposure — whether it's alcohol (understanding your alcohol limits), a medication causing nerve damage, or an environmental toxin — halts the progression in most cases.
Correcting nutritional deficiencies with B vitamins, alpha-lipoic acid, or other targeted supplements addresses nutritional neuropathies directly.
Treating autoimmune causes with immunotherapy (IVIg, plasma exchange, or immunosuppressive medications) can halt or reverse autoimmune neuropathies.
Even when the cause can't be fully eliminated, lifestyle interventions make a difference. Regular exercise has been shown to improve nerve function and may promote nerve regeneration. A nerve-healthy diet supports overall nerve maintenance and repair.
Signs That Your Neuropathy May Be Progressing
Monitoring your own neuropathy helps you catch progression early, when intervention is most effective. Watch for these indicators:

Geographic expansion: Symptoms appearing in new areas — toes to entire foot, feet to hands, lower legs to upper legs.
Symptom type changes: Moving from intermittent tingling to constant numbness, or from sensory symptoms to motor symptoms (weakness, muscle wasting). New motor symptoms are particularly significant because they indicate a different class of nerves is now affected.
Functional decline: Activities you could do 6 months ago that are now harder — opening jars, climbing stairs, maintaining balance on uneven surfaces.
Autonomic involvement: New symptoms like dizziness when standing, digestive changes, bladder difficulty, or sexual dysfunction suggest autonomic nerves are being affected.
Keeping a symptom journal is one of the most useful things you can do. Record what you feel, where, how intense it is, and what makes it better or worse. When you review entries from 3-6 months ago, you'll see trends that day-to-day living obscures. Bring this journal to your doctor — it's more valuable than any single snapshot appointment.
When to Seek Urgent Medical Attention
Most neuropathy progresses slowly enough that regular doctor visits are sufficient for monitoring. But certain progression patterns warrant urgent attention:
Ascending paralysis — weakness climbing from feet upward over hours to days
Sudden inability to lift your foot, grip objects, or maintain balance
Breathing difficulty with simultaneous limb weakness
Rapid onset: If significant weakness or numbness develops over days to weeks rather than months, this could indicate Guillain-Barré syndrome or another acute neuropathy requiring emergency treatment.
Sudden weakness: If you suddenly can't lift your foot (foot drop), grip objects, or maintain balance — especially if it affects one side — seek immediate medical evaluation. This could indicate a treatable cause like nerve compression or vasculitis.
Ascending paralysis: Weakness that starts in the feet and climbs upward over hours to days is a medical emergency. Go to the emergency room — this pattern is characteristic of Guillain-Barré syndrome, which can become life-threatening if it reaches the muscles that control breathing. Familiarize yourself with neuropathy emergency signs.
Bilateral symmetry breaking: If your neuropathy has been symmetric (both feet equally) and suddenly becomes dramatically worse on one side, this could indicate a new problem — nerve compression, vascular issue, or mononeuropathy — that requires separate investigation.
The Role of Nerve Regeneration
There's a reason for cautious optimism: unlike brain and spinal cord nerves, peripheral nerves can regenerate. The science of nerve regeneration is a source of genuine hope.
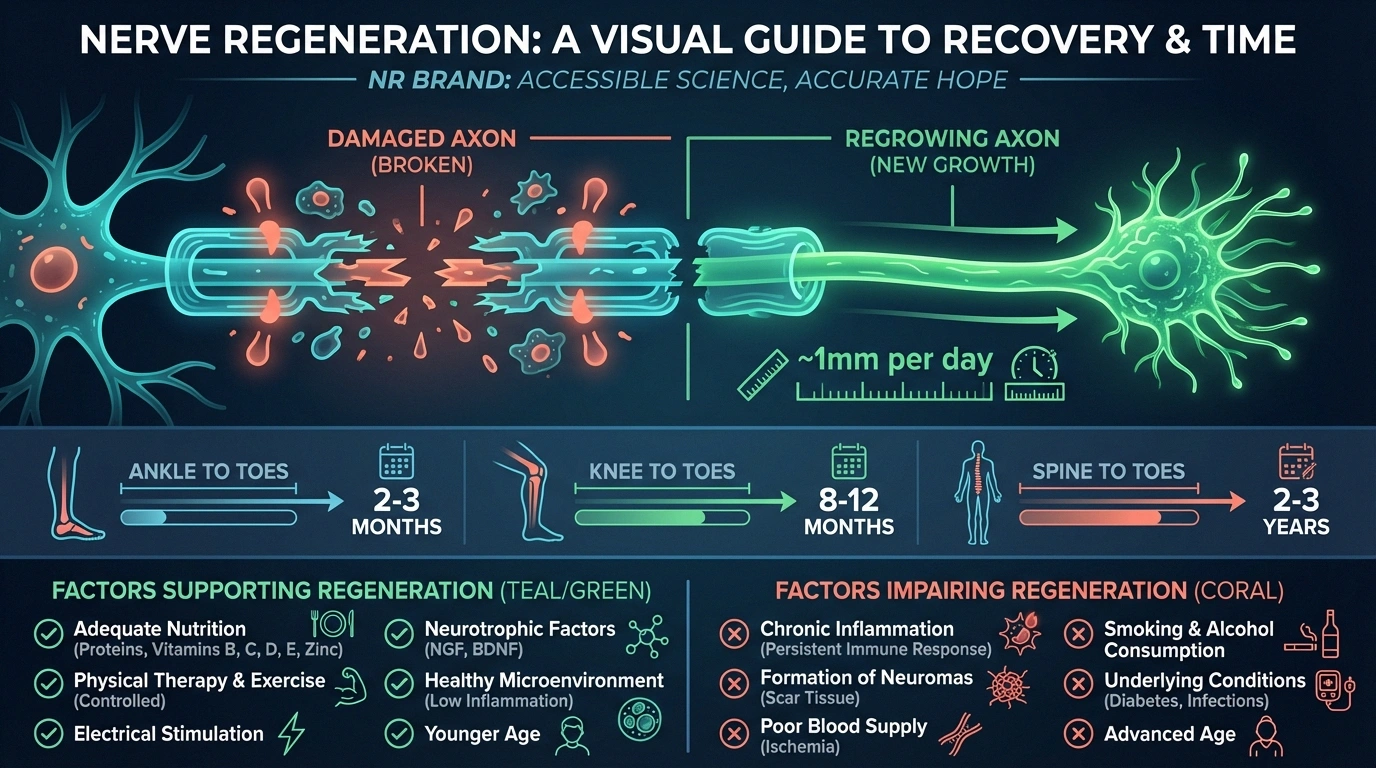
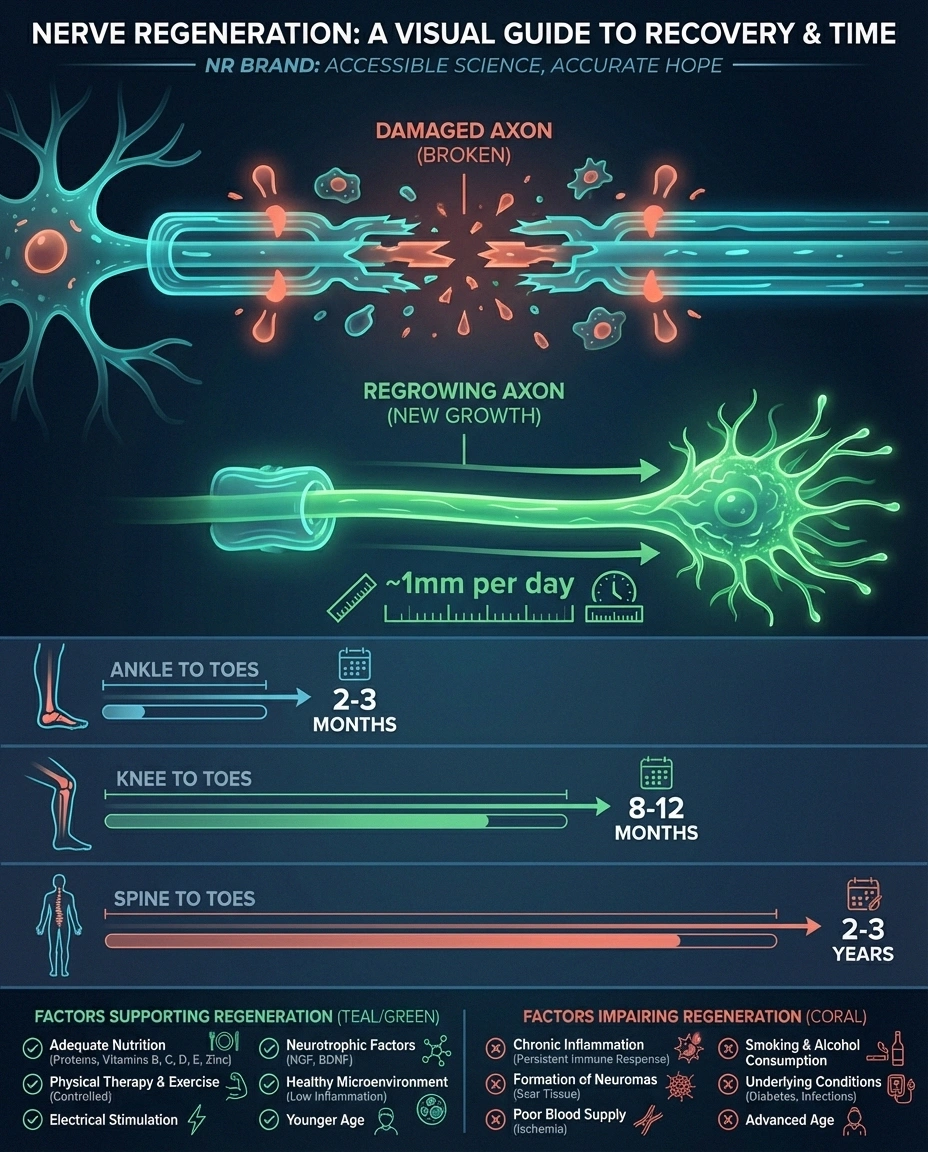
Peripheral nerves regrow at approximately 1 millimeter per day — about an inch per month. That means nerve recovery from the lower leg to the foot could take 6-12 months or more. Recovery from the spine to the toes might take years. This slow pace is why patience is essential and why monitoring progress through nerve conduction studies or skin biopsies is more reliable than subjective symptom assessment alone.
Factors that support nerve regeneration include: removing the damaging agent, correcting nutritional deficiencies (especially B12 and thiamine), regular exercise (shown to increase nerve fiber density in studies), adequate protein intake, and alpha-lipoic acid supplementation.
Factors that impair regeneration: continued toxic exposure, ongoing high blood sugar, smoking (which independently damages nerves), and advanced age (regeneration slows as we get older, though it doesn't stop entirely).
The key takeaway: progression is not a one-way street. Neuropathy reversal is possible in many situations, and even when complete reversal isn't achievable, stopping progression and allowing partial recovery is a realistic goal for most people.
Frequently Asked Questions
Does neuropathy always get worse over time?
No. Whether neuropathy gets worse depends on the underlying cause and whether it can be treated. Many people with well-managed diabetes maintain stable neuropathy for years. Neuropathy from vitamin deficiency often improves with supplementation. Even idiopathic neuropathy frequently follows a slow, stable course. Worsening is most common when the underlying cause remains unaddressed.
Can neuropathy spread from feet to hands?
Yes, this is the classic stocking-and-glove progression. It happens because the same systemic process damaging the nerves in your feet is also affecting the nerves in your hands — the hand nerves just reach their damage threshold later because they're shorter. When symptoms reach mid-calf level, hand symptoms often begin. This pattern doesn't mean the neuropathy is “jumping” — it's the same underlying process affecting nerves of progressively shorter length.
Is neuropathy a progressive disease?
Some forms are inherently progressive (like Charcot-Marie-Tooth disease), but most forms of neuropathy are progressive only if the underlying cause persists. Diabetic neuropathy progresses with uncontrolled blood sugar but stabilizes with good control. Toxic neuropathy progresses with continued exposure but stops when the toxin is removed. The critical message: progression is usually driven by the cause, not by the neuropathy itself.
Can neuropathy affect internal organs?
Yes, through autonomic neuropathy. The autonomic nerves control internal organ function — heart rate, digestion, bladder control, blood pressure regulation, and more. When these nerves are damaged, it can cause digestive problems, blood pressure drops when standing, bladder dysfunction, and other internal symptoms. Autonomic neuropathy is most common in diabetes and autoimmune conditions.
How do I know if my neuropathy is getting worse or just fluctuating?
Neuropathy symptoms naturally fluctuate day-to-day and week-to-week. Stress, sleep, weather, activity level, and even time of day all affect symptom intensity. True progression is measured over months, not days. A symptom journal helps distinguish fluctuation from actual progression. If symptoms are noticeably and consistently worse than they were 3-6 months ago — or if they've appeared in new body areas — that suggests genuine progression worth discussing with your doctor.
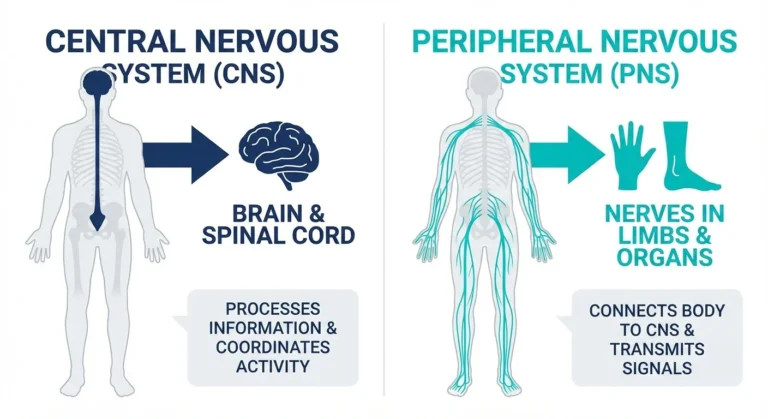
Will neuropathy spread to my brain or spinal cord?
Peripheral neuropathy, by definition, affects only the peripheral nerves — those outside the brain and spinal cord. The damage does not cross into the central nervous system. However, some conditions (like multiple sclerosis, Lyme disease, or B12 deficiency) can affect both peripheral and central nerves independently. If you're experiencing symptoms that suggest central nervous system involvement (vision changes, cognitive problems, coordination issues beyond what neuropathy explains), tell your doctor, as this may indicate a separate condition.