
Proximal Neuropathy: Nerve Damage in Hips, Thighs, and Buttocks
When most people think of neuropathy, they picture tingling toes and numb feet. But there's a form of nerve damage that strikes much higher—in your hips, thighs, and buttocks—and it can be one of the most painful and disabling types of neuropathy you'll encounter.
Proximal neuropathy hit a friend of mine without warning. He woke up one morning with searing pain in his left thigh, and within a few weeks, his leg had weakened to the point where he struggled to get out of a chair. His doctor initially thought it might be a hip problem or sciatica. It took nearly two months before he got the correct diagnosis. That delay—and the fear that came with it—is something I hear about again and again from people with this condition.
If you or someone you love is dealing with sudden, severe pain in the hips or thighs along with muscle weakness, this article will explain what proximal neuropathy is, why it happens, and what the road to recovery actually looks like.
What Is Proximal Neuropathy?
Proximal neuropathy is a rare and disabling form of nerve damage that affects the nerves serving your hips, buttocks, thighs, and sometimes your lower legs. Unlike peripheral neuropathy, which typically starts in the hands and feet and works its way inward, proximal neuropathy targets the large nerves closer to the center of your body—the “proximal” nerves.
of people with type 2 diabetes develop proximal neuropathy — rare but often recoverable
This condition goes by many names in the medical literature, which can add to the confusion:
- Diabetic amyotrophy (the most common clinical term)
- Diabetic lumbosacral radiculoplexopathy (the formal neurological name)
- Diabetic polyradiculopathy
- Femoral neuropathy (when the femoral nerve is primarily affected)
- Bruns-Garland syndrome
Regardless of what your doctor calls it, the condition involves damage to the nerve roots and nerve plexus in the lumbosacral area—the network of nerves that controls sensation and movement in your lower body.
According to Johns Hopkins Medicine, proximal neuropathy is a relatively rare type of diabetic neuropathy, occurring in approximately one percent of people with type 2 diabetes. It's more common in men, in people over age fifty, and almost exclusively occurs in people with diabetes—though rare cases have been documented without diabetes.
How Proximal Neuropathy Differs From Other Types
Understanding what makes proximal neuropathy different from other types of neuropathy is important, because the differences affect diagnosis, treatment, and prognosis.
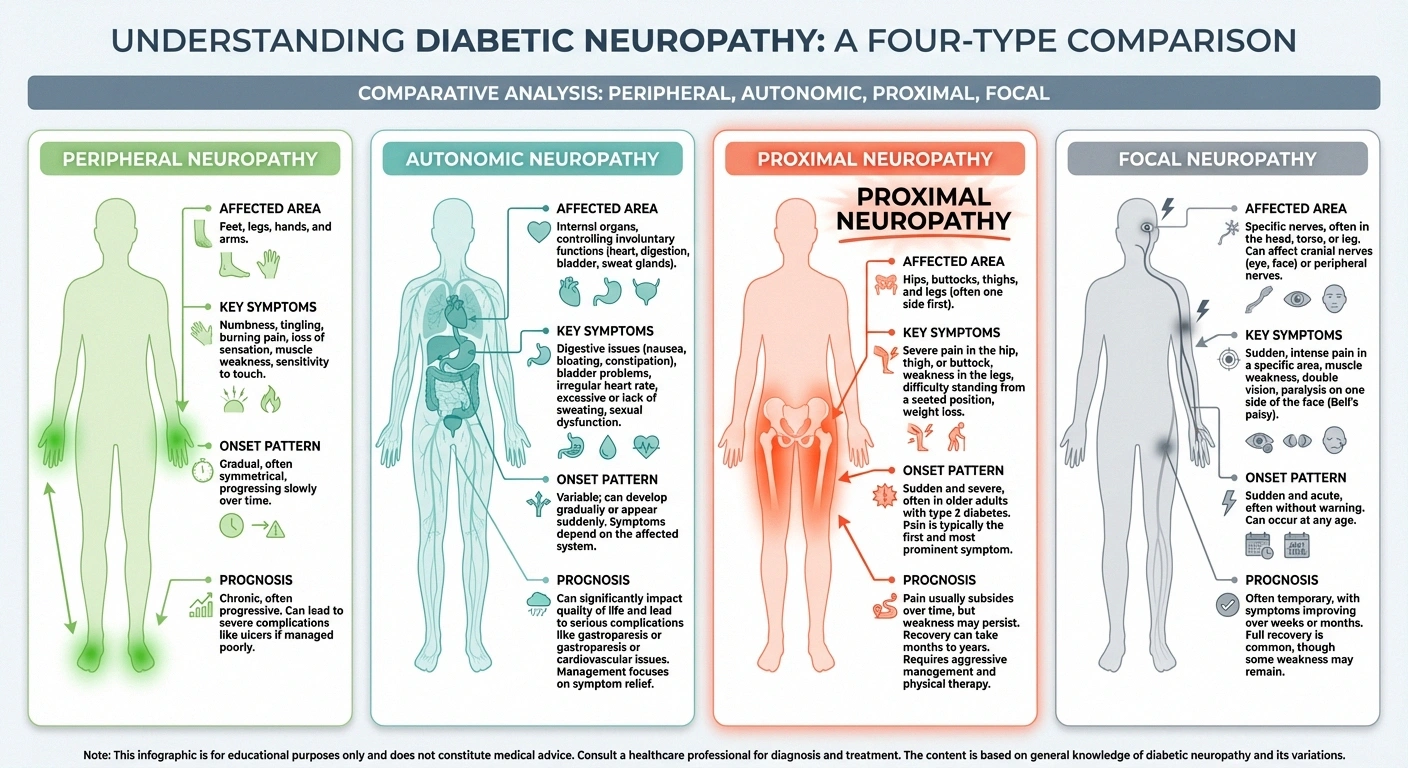
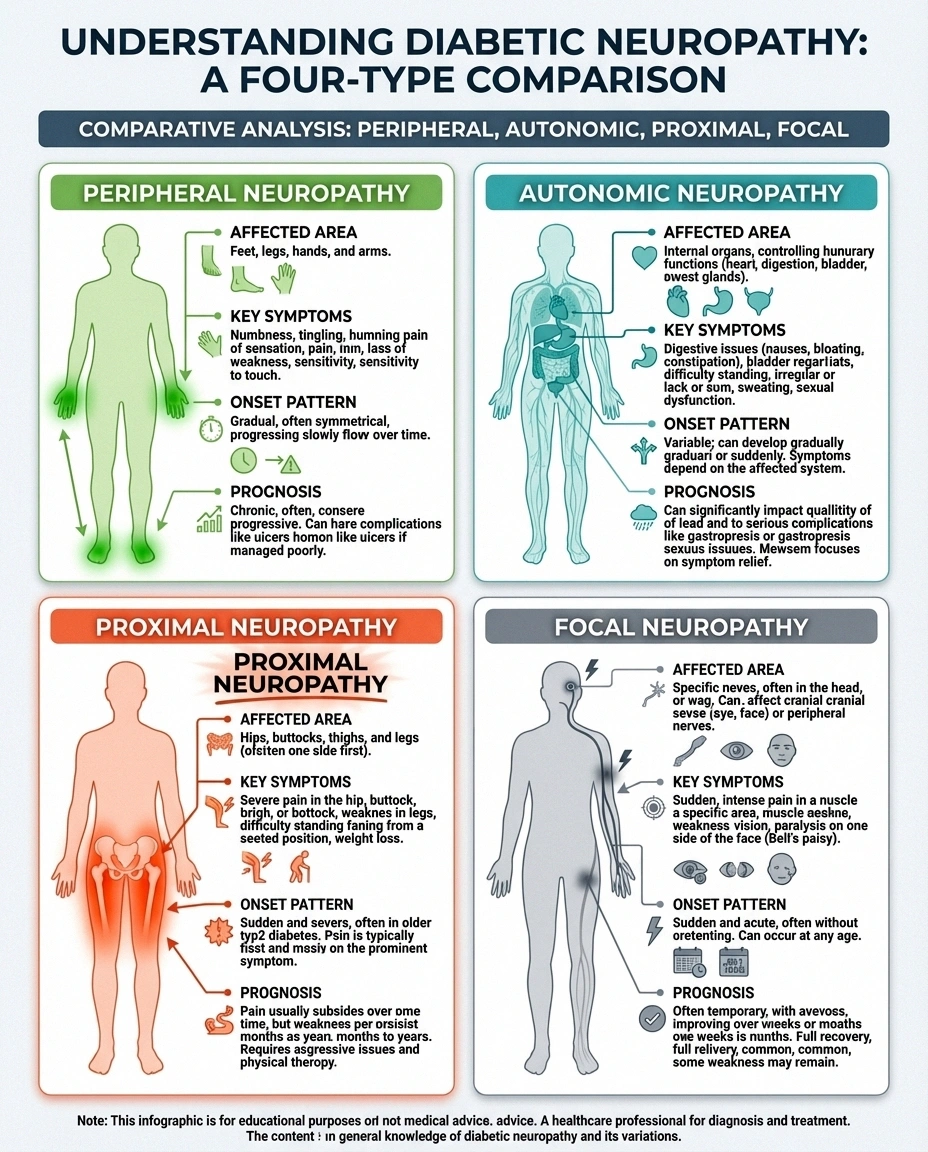
🦶 Peripheral Neuropathy
Where: Feet and hands
Onset: Gradual (months/years)
Main symptoms: Numbness, tingling, burning
Prognosis: Often progressive
🦵 Proximal Neuropathy
Where: Hips, thighs, buttocks
Onset: Sudden (days/weeks)
Main symptoms: Severe pain, weakness, wasting
Prognosis: Usually self-limiting
Location: While diabetic peripheral neuropathy affects the feet and hands (the most distant nerves), proximal neuropathy hits the hips, thighs, and buttocks. Autonomic neuropathy affects internal organs. Proximal neuropathy is the only common form that causes significant muscle weakness in the legs.
Onset: Peripheral neuropathy develops gradually over months or years. Proximal neuropathy typically strikes suddenly, with severe pain appearing over days to weeks. This abrupt onset is one of its defining characteristics—and one of the reasons it's initially misdiagnosed.
Symmetry: Peripheral neuropathy usually affects both sides equally (both feet, both hands). Proximal neuropathy most often starts on one side only—one hip, one thigh—though it may rarely spread to the other side over time.
Prognosis: Here's the most important difference—and the one that offers hope. While peripheral neuropathy is generally a progressive, long-term condition, most people with proximal neuropathy experience significant recovery within months to a few years. According to the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), most people recover from proximal neuropathy even without specific treatment—though the recovery period can be long and difficult.
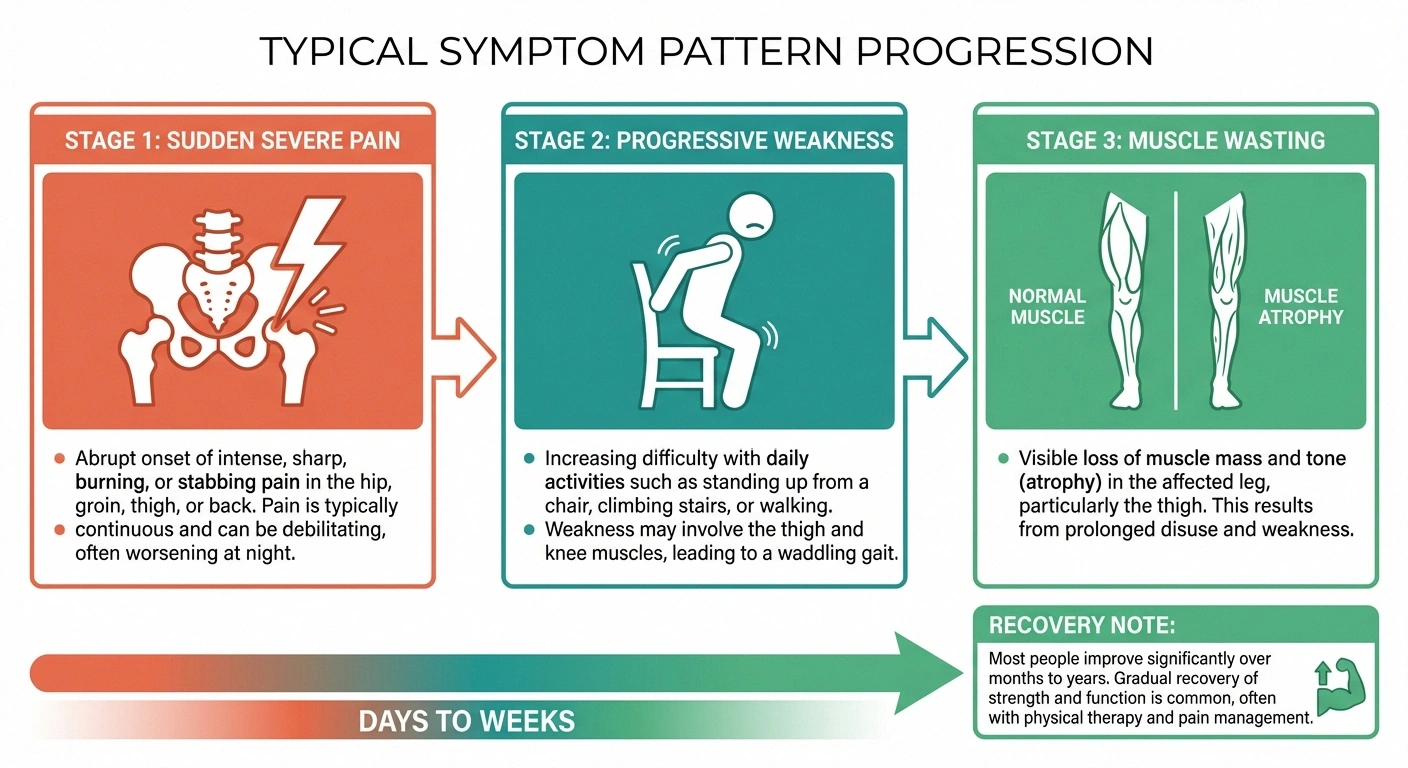
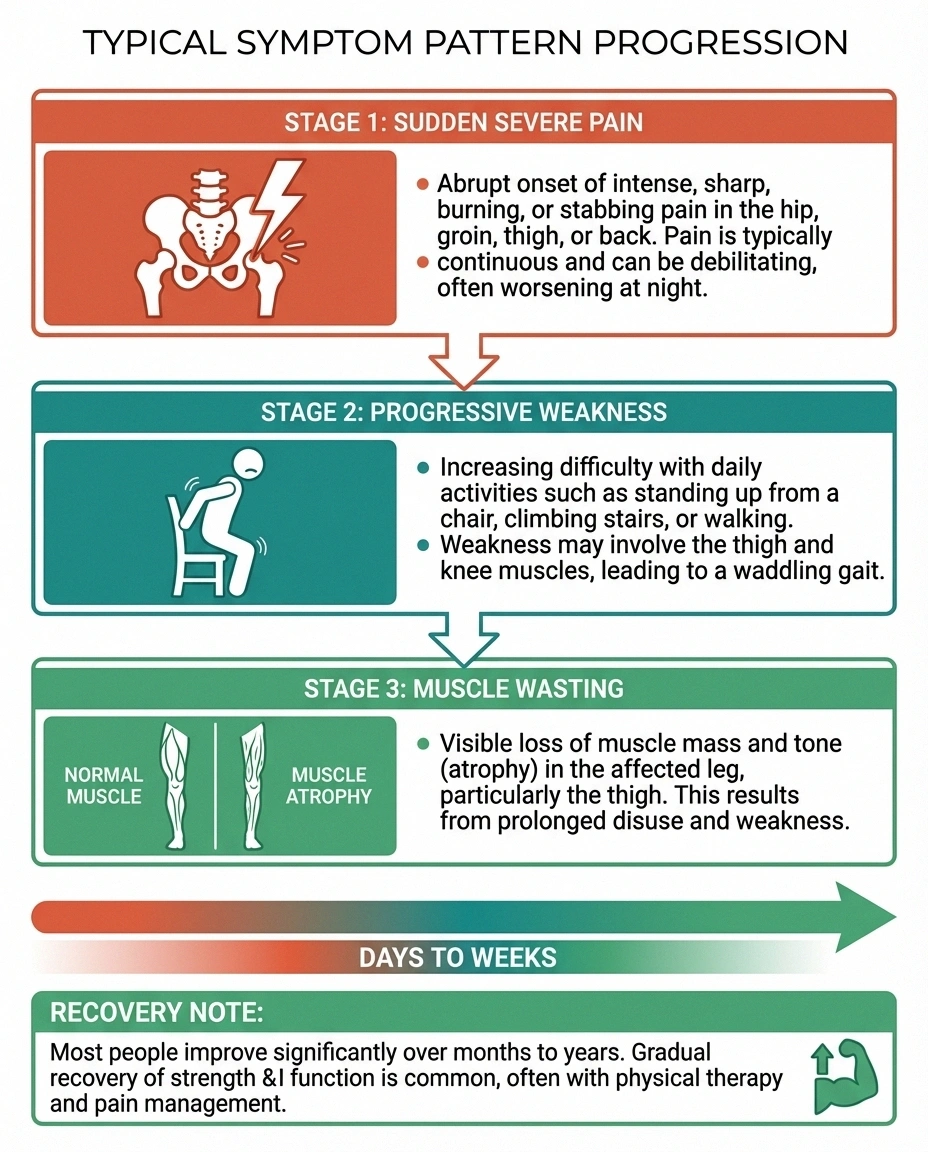
Symptoms of Proximal Neuropathy
The symptoms of proximal neuropathy tend to develop in a recognizable pattern. Understanding this pattern can help you recognize the condition earlier and seek appropriate medical care:
Warning Signs of Proximal Neuropathy
Sudden, severe pain in one hip, buttock, or thigh
Difficulty standing up from a seated position
Leg weakness or a feeling of instability
One thigh looking thinner than the other
Unexplained weight loss alongside leg pain
If you have diabetes and recognize these symptoms, contact your doctor promptly — early treatment improves outcomes.
Stage 1: Sudden, severe pain. The first symptom is usually intense pain in one hip, buttock, or thigh. Many people describe it as a deep, aching, burning, or stabbing pain that can be severe enough to prevent sleep and limit mobility. The pain often comes on within days and can be among the worst pain people have experienced.
Stage 2: Progressive weakness. Following the onset of pain—typically within days to weeks—the muscles in the affected area begin to weaken. You may notice:
- Difficulty standing up from a seated position
- Trouble climbing stairs
- The leg feeling unstable or “giving way”
- Difficulty getting in and out of cars
- A noticeable change in your walking pattern
Stage 3: Muscle wasting. As the nerve damage progresses, the muscles in the affected thigh may visibly shrink—a process called atrophy. You may notice one thigh looking noticeably thinner than the other. This can be alarming, but it's a characteristic feature of the condition.
Other associated symptoms:
- Loss of the knee-jerk reflex on the affected side
- Unintentional weight loss (which can be significant)
- Occasionally, pain and weakness spreading to the other leg
- Numbness or tingling in the affected areas (though pain and weakness are usually more prominent than sensory changes)
What Causes Proximal Neuropathy?
Proximal neuropathy is overwhelmingly associated with diabetes—particularly type 2 diabetes. The exact mechanism is still being studied, but researchers believe it involves a combination of factors:
Metabolic damage: Chronic high blood sugar damages the small blood vessels that supply the lumbosacral nerve plexus. High levels of triglycerides—common in type 2 diabetes—compound this vascular damage. Over time, the nerves are starved of oxygen and nutrients.
Immune-mediated inflammation: Growing evidence suggests that proximal neuropathy may have an autoimmune component. Research indicates that the condition involves inflammatory changes in the nerve tissue—the body's immune system may be attacking the nerves themselves. This autoimmune theory helps explain why the condition can sometimes respond to immunotherapy treatments.
Vascular factors: Damage to the tiny blood vessels (vasa nervorum) that supply blood to the nerves is a consistent finding in studies of proximal neuropathy. This vascular damage reduces blood flow to the nerve plexus, contributing to nerve injury.
One important misconception to address: proximal neuropathy doesn't only affect people who have had diabetes for many years. According to research published in Diabetes Care, the condition can develop relatively early in the course of diabetes—sometimes even in people who were only recently diagnosed. This makes regular monitoring for neurological symptoms important regardless of how long you've had diabetes.
Getting an Accurate Diagnosis
Diagnosing proximal neuropathy can be challenging because its symptoms overlap with several other conditions. The sudden hip or thigh pain is often initially attributed to:

Don't Assume It's Sciatica
Proximal neuropathy is frequently misdiagnosed as sciatica, hip arthritis, or a muscle strain. If you have diabetes and develop sudden hip or thigh pain with progressive leg weakness, specifically ask your doctor about proximal neuropathy. EMG testing can help distinguish it from other conditions.
- Hip arthritis or bursitis
- Sciatica or herniated disc
- Spinal stenosis
- Blood clots in the leg
- Muscle strains or injuries
The combination of sudden severe pain plus progressive leg weakness plus diabetes should raise a red flag for proximal neuropathy. If you have diabetes and develop these symptoms, mention the possibility of proximal neuropathy to your doctor.
Diagnostic testing typically includes:
Electromyography (EMG) and nerve conduction studies: These tests measure how electrical signals move through your nerves and how your muscles respond. EMG is particularly useful for proximal neuropathy because it can show the pattern and extent of nerve damage in the lumbosacral plexus—helping distinguish it from simpler conditions like a pinched nerve.
MRI: Imaging of the lumbar spine and pelvis can help rule out structural causes (herniated discs, tumors, spinal stenosis) and may show inflammation or swelling in the nerve plexus itself.
Blood tests: Blood glucose levels, HbA1c (to assess long-term blood sugar control), and sometimes inflammatory markers are checked to evaluate the underlying cause and guide treatment.
Lumbar puncture (in some cases): If autoimmune causes are suspected, a spinal fluid analysis may be performed to look for elevated protein levels or inflammatory markers.
Treatment and Management
There is no single treatment that “fixes” proximal neuropathy, but a multi-pronged approach can manage the pain, maintain function, and support recovery. Treatment generally focuses on three areas:
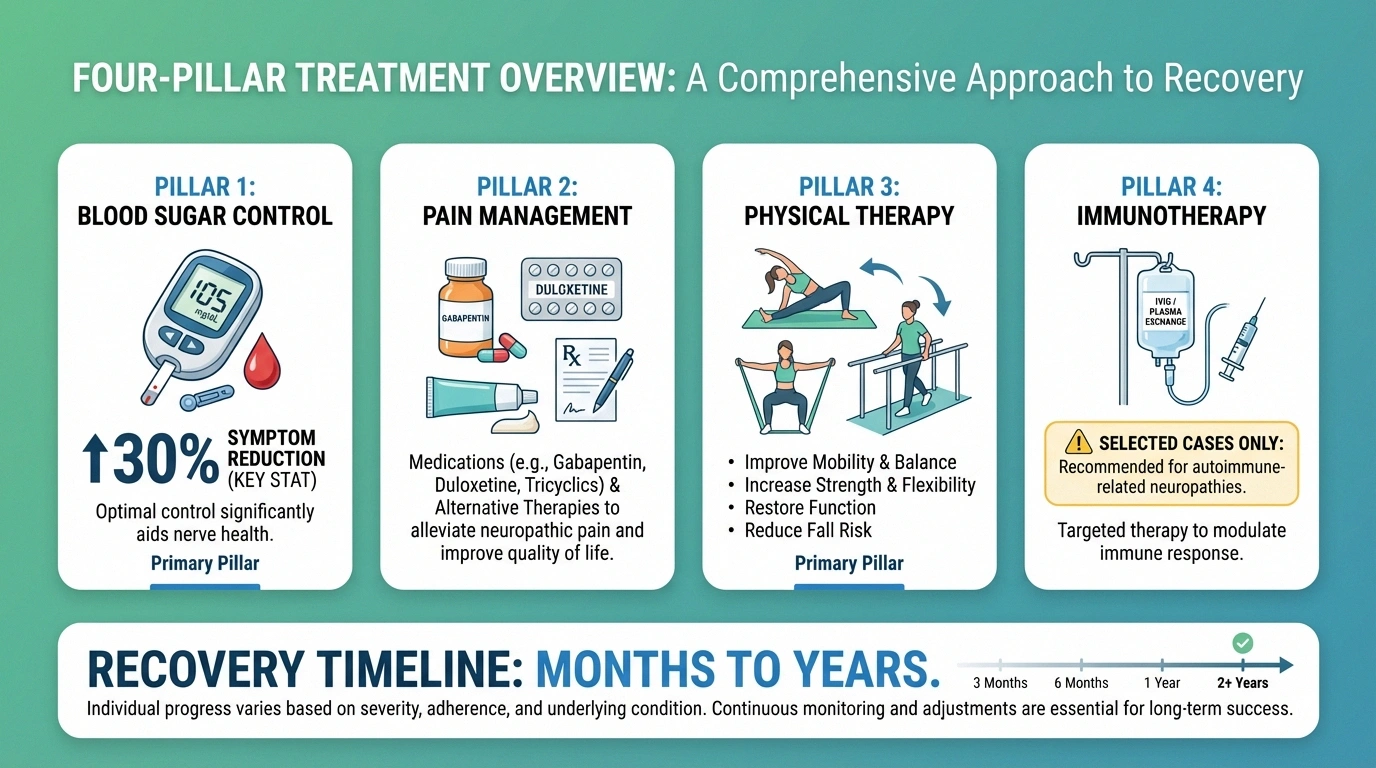
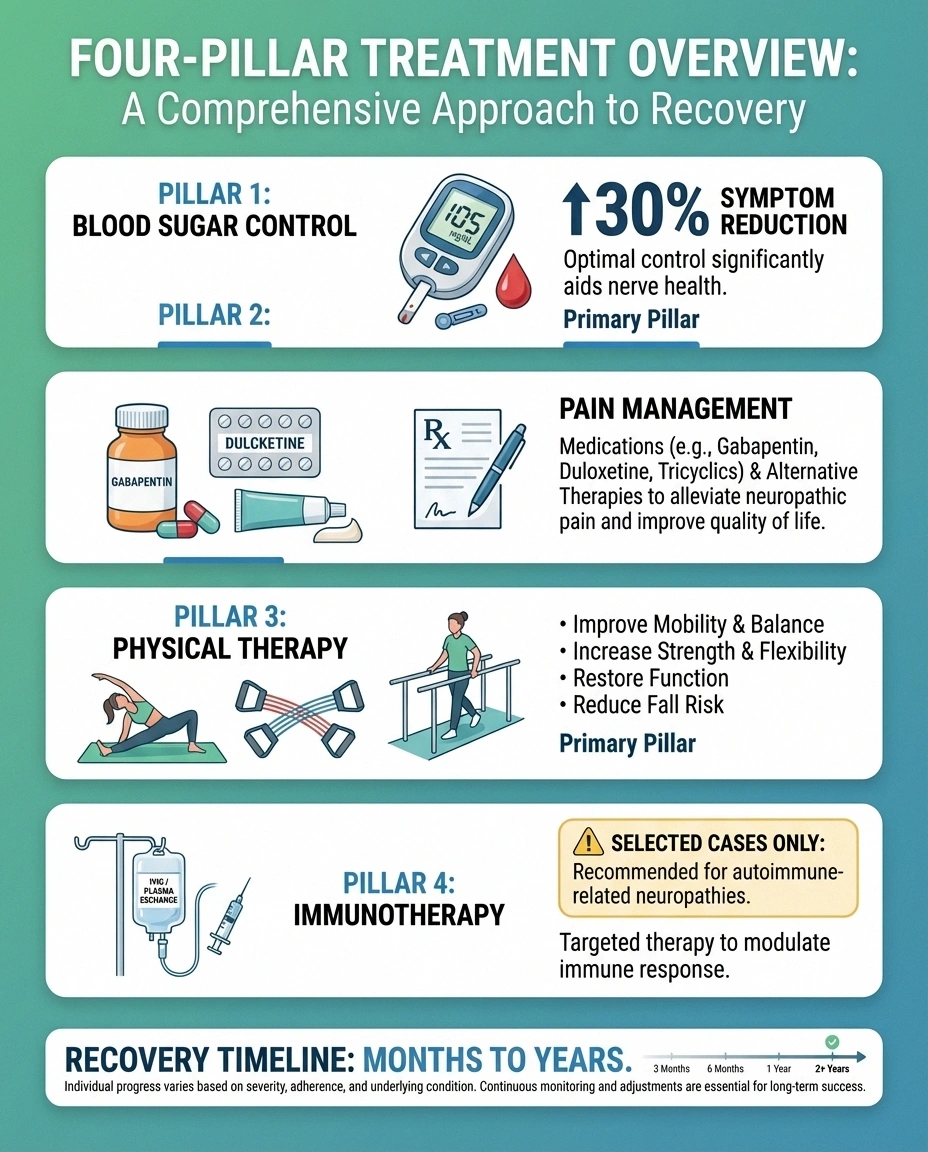
Blood Sugar Control
This is the foundation of treatment. Tight blood sugar management can help slow nerve damage and create the best environment for nerve recovery. A 2022 study published in the Journal of Diabetes Research found that intensive glycemic control reduced symptom progression by thirty percent over a two-year period.
Work closely with your endocrinologist or primary care doctor to optimize your diabetes management. This may involve adjusting medications, modifying your diet, increasing physical activity (as tolerated), and monitoring blood sugar more frequently during the acute phase.
Pain Management
The pain of proximal neuropathy can be severe—sometimes the most challenging aspect of the condition. Your doctor may recommend:
- Gabapentin or pregabalin: First-line medications for neuropathic pain that work by calming overactive nerve signals
- Duloxetine: An antidepressant that's also effective for neuropathic pain
- Tricyclic antidepressants (like amitriptyline): Older but still effective medications for nerve pain
- NSAIDs or acetaminophen: May provide some relief for milder pain, though they're generally less effective for neuropathic pain
- Short-term opioids: In cases of severe, acute pain, your doctor may prescribe opioids for a limited period—though this is approached cautiously due to dependency risks
Physical Therapy and Rehabilitation
physical therapy for neuropathy is critically important for proximal neuropathy—arguably more important than for any other type of neuropathy. Because this condition causes significant muscle weakness and wasting, rehabilitation focuses on:

- Maintaining and rebuilding strength in the affected muscles
- Preventing further muscle atrophy during the acute phase
- Improving balance and reducing fall risk (since leg weakness significantly increases your risk of falls)
- Restoring functional mobility—getting in and out of chairs, climbing stairs, walking safely
Your physical therapist will design a program that progresses as your strength improves. In the early stages, when pain and weakness are most severe, exercises may be gentle and focused on maintaining range of motion. As recovery progresses, the program intensifies to rebuild muscle strength and endurance.
Occupational therapy may also be helpful for adapting daily activities while you recover—learning new ways to get dressed, navigate stairs, or manage household tasks with reduced leg strength.
Immunotherapy (In Selected Cases)
Because of the suspected autoimmune component, some neurologists treat proximal neuropathy with immunomodulatory therapies—particularly in severe cases or when standard treatments haven't provided adequate relief. Options may include intravenous immunoglobulin (IVIG) or corticosteroids. These treatments are not standard first-line therapy and are typically reserved for cases where inflammation is clearly contributing to the nerve damage.
Recovery and Prognosis
Here's the news that most people with proximal neuropathy need to hear: this condition is generally self-limiting, and most people experience significant recovery.
The Good News
Unlike most forms of neuropathy, proximal neuropathy is generally self-limiting. Most people experience significant recovery within months to a few years. Approximately 50% of patients show meaningful improvement within the first year with proper treatment — especially physical therapy and blood sugar control.
According to the NIDDK and Mayo Clinic, symptoms typically follow this pattern:
- Acute phase (weeks to months): Pain is most severe. Weakness progresses. This is the hardest period.
- Plateau (months): Symptoms stabilize. Pain begins to ease for many people.
- Recovery phase (months to years): Gradual improvement in strength and function. Pain continues to decrease. Most people recover substantially within two to three years.
However, recovery is not always complete. Some residual weakness or mild pain may persist, and the condition can rarely recur—sometimes on the opposite side. Early intervention with physical therapy and optimal blood sugar control gives you the best chance of a fuller recovery.
Research suggests that approximately fifty percent of patients show significant improvement within one year with proper treatment, including physical therapy and glycemic control.
Living With Proximal Neuropathy Day to Day
While you're in the midst of recovery—which can take months to years—these practical strategies can help you manage daily life:

Fall prevention is priority one. With weakened leg muscles, your fall risk is significantly increased. Remove tripping hazards from your home, install grab bars in the bathroom, use handrails on stairs, and consider a cane or walker during the acute phase. There's no shame in using assistive devices—they keep you safe while your nerves heal.
Adapt how you move. Learn techniques for getting out of chairs using your arms for support. Take stairs one at a time. When possible, choose seating with armrests. These adaptations reduce the demand on weakened muscles and lower your injury risk.
Manage your weight. Excess weight places additional stress on weakened leg muscles and can worsen pain. If you're overweight, even modest weight loss can improve mobility and comfort. Our article on neuropathy and weight explores this connection in detail.
Prioritize sleep. Pain often disrupts sleep, and poor sleep worsens pain perception—a vicious cycle. Talk to your doctor about sleep-specific pain management strategies, and see our guide on why neuropathy gets worse at night for practical tips.
Stay engaged. The limitations imposed by proximal neuropathy can lead to isolation and depression. Stay connected with family and friends, pursue activities you can do comfortably, and consider joining a neuropathy support group where others understand what you're going through.
Frequently Asked Questions
Is proximal neuropathy the same as peripheral neuropathy?
No, they are distinct conditions that affect different nerves. Peripheral neuropathy damages the nerves farthest from the center of the body, typically causing numbness, tingling, and pain in the feet and hands. Proximal neuropathy damages nerves closer to the trunk, affecting the hips, thighs, and buttocks, and is characterized by severe pain and muscle weakness. A person can have both conditions simultaneously, as they share diabetes as a common underlying cause.
Can proximal neuropathy occur without diabetes?
Rarely. The vast majority of proximal neuropathy cases occur in people with type 2 diabetes. However, similar presentations can occasionally occur with other conditions, including certain autoimmune disorders, infections, and vascular diseases. If you develop symptoms of proximal neuropathy without a diabetes diagnosis, your doctor may need to investigate other potential causes.
Will I fully recover from proximal neuropathy?
Most people experience significant improvement over months to years, with many recovering most of their strength and experiencing substantial pain reduction. However, complete recovery to the pre-condition baseline does not occur in every case. Some people retain mild residual weakness or discomfort. Early treatment with physical therapy and optimal blood sugar control improves the chances of fuller recovery.
How is proximal neuropathy different from sciatica?
While both cause pain in the hip and thigh area, they have different causes and patterns. Sciatica is caused by compression of the sciatic nerve, usually from a herniated disc, and pain typically radiates down the back of the leg. Proximal neuropathy involves broader nerve damage from diabetes and affects multiple nerves in the lumbosacral plexus. It causes significant muscle weakness and wasting, which sciatica generally does not. EMG and imaging studies can help distinguish between the two.

Can proximal neuropathy affect both legs?
Proximal neuropathy most commonly starts on one side of the body only. In some cases, it may spread to affect the other leg, though this is relatively uncommon. When it does occur on both sides, it typically begins on one side first and then involves the other side weeks to months later. Bilateral involvement may suggest a more severe or inflammatory course.
What exercises are safe with proximal neuropathy?
Exercise is important for recovery, but it should be guided by a physical therapist, especially in the early stages when pain and weakness are most severe. Generally safe activities include gentle range-of-motion exercises, seated exercises, upper body workouts, and swimming or water therapy once pain allows. Avoid high-impact activities and heavy leg exercises until your physical therapist gives the green light. Water-based exercises are often recommended because the buoyancy reduces stress on weakened muscles.
Moving Forward With Hope
Proximal neuropathy is frightening—there's no way around that. The sudden onset of severe pain and the progressive loss of leg strength can shake your confidence and your independence. But unlike many forms of neuropathy, this one comes with a genuinely encouraging prognosis.
Most people recover significantly. Physical therapy works. Blood sugar management makes a real difference. And while the road to recovery is measured in months and years rather than days and weeks, recovery does happen for the majority of people.
If you or someone you know is dealing with proximal neuropathy, the most important steps are getting an accurate diagnosis, working closely with your healthcare team, starting physical therapy as soon as possible, and maintaining tight blood sugar control. These aren't magic solutions—they're steady, proven strategies that give your nerves the best possible chance to heal.
For more information on managing neuropathy, explore our guides to the stages of neuropathy, whether neuropathy can be reversed, physical therapy for neuropathy, and safe neuropathy exercises for seniors.


