
Leg Weakness: Neuropathy vs. Spinal Stenosis vs. MS vs. PAD — How to Tell the Difference
When your legs start feeling weak — when climbing stairs feels harder than it should, or your knees buckle unexpectedly — the uncertainty can be almost as distressing as the symptom itself. I remember that feeling well. Your mind races through possibilities, and Dr. Google isn't exactly reassuring.
Here's what I've learned after more than a decade navigating the neuropathy world: leg weakness has several possible causes, and getting the right diagnosis matters enormously because the treatments are completely different. The four most common culprits — peripheral neuropathy, spinal stenosis, multiple sclerosis (MS), and peripheral artery disease (PAD) — can all cause legs that feel heavy, tired, or unreliable. But each one does it for a fundamentally different reason.
This guide walks through each condition, how it causes weakness, the key differences that help doctors distinguish between them, and what tests can give you a definitive answer. My goal isn't to replace your neurologist — it's to help you walk into that appointment armed with better questions.
Understanding Why Legs Get Weak
Leg weakness isn't a diagnosis — it's a symptom. And the underlying mechanism matters because it determines whether the weakness is reversible, progressive, or manageable. At the most basic level, your legs need three things to function properly: healthy nerves to carry signals, an intact spinal cord and brain to coordinate those signals, and adequate blood flow to fuel the muscles.
Americans with peripheral neuropathy
adults affected by spinal stenosis
Americans with PAD over age 40
When any of these systems fail, the result can feel similar — your legs don't respond the way they should. But the pattern of failure, the timing, and the accompanying symptoms create a fingerprint that points toward the right diagnosis.
According to the National Institute of Neurological Disorders and Stroke (NINDS), peripheral neuropathy alone affects an estimated 20 million Americans. Add spinal stenosis (which impacts roughly 250,000 adults in the U.S.), MS (nearly one million Americans), and PAD (affecting 8-12 million people), and you begin to see why leg weakness is one of the most common complaints doctors encounter.
Peripheral Neuropathy: When Damaged Nerves Can't Carry the Signal
Peripheral neuropathy causes leg weakness by damaging the motor nerves that tell your leg muscles to contract. Think of it like frayed wiring — the signal from your brain may be perfectly clear, but by the time it reaches your leg muscles through damaged nerves, it's weak, garbled, or absent entirely.
🦶 Neuropathy
Gradual, symmetrical weakness starting in feet. Numbness and tingling. Balance problems. Doesn't improve with rest or position changes.
🦴 Stenosis
Position-dependent weakness. Worse standing/walking. Better sitting/leaning forward. May be one-sided. Often includes back pain.
🧠 MS
Episodic weakness that comes and goes. Often one-sided initially. Heat worsens symptoms. Spasticity and stiffness. Vision/bladder changes.
❤️ PAD
Exertion-dependent cramping/weakness. Predictable walking distance threshold. Improves by simply standing still. Cool skin, weak pulses.
Neuropathy Fingerprint
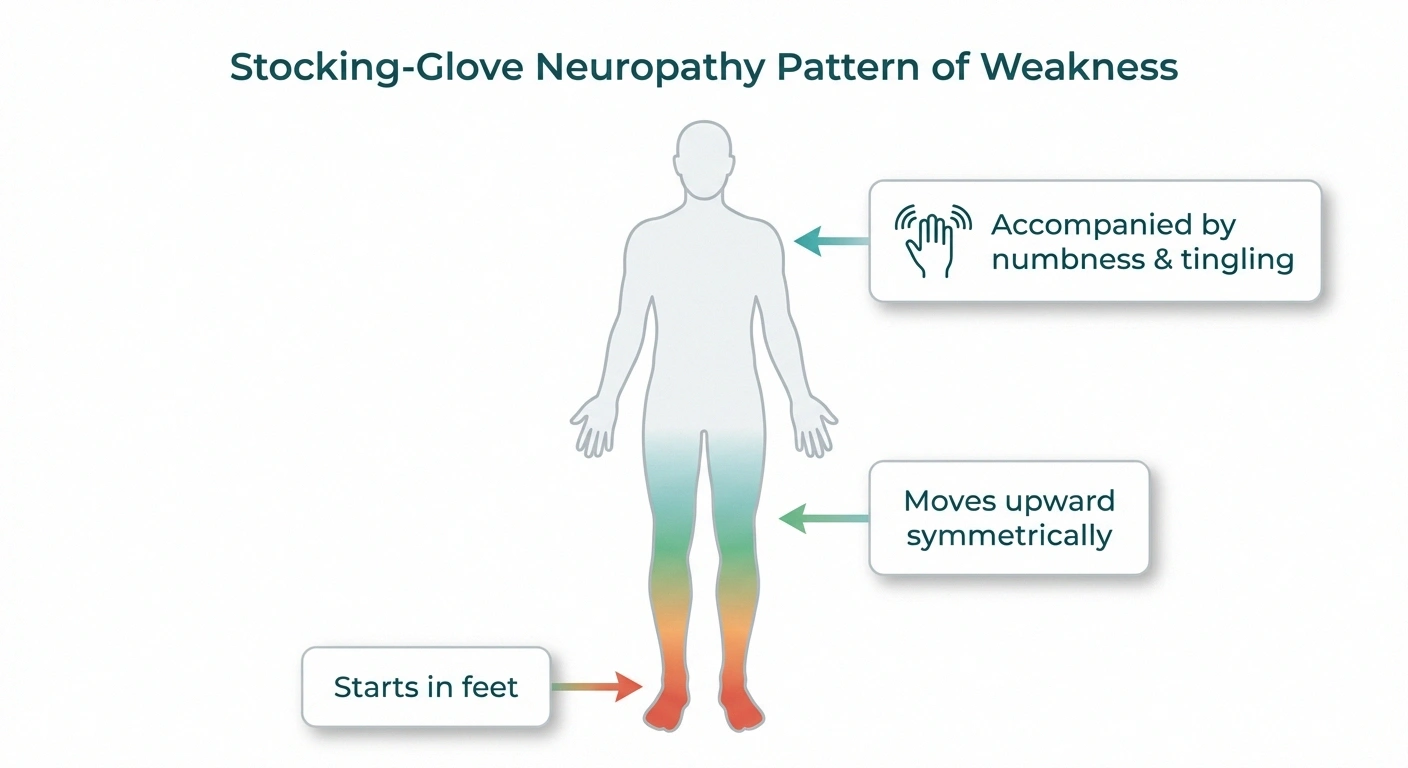
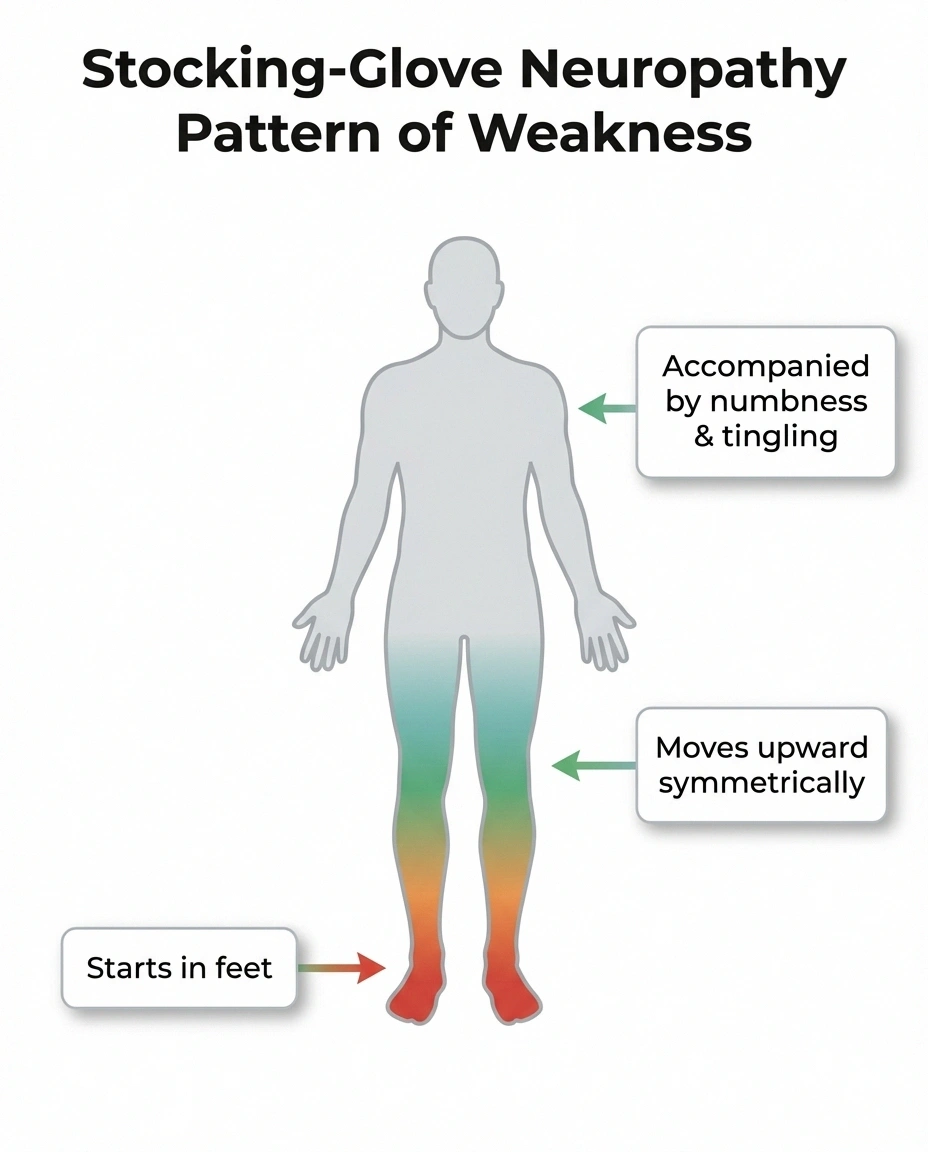
Weak legs + numb feet + symmetrical pattern = neuropathy is the leading suspect. The stocking-glove distribution — starting in the feet and moving upward equally on both sides — is the hallmark that separates neuropathy from the other three conditions.
What makes neuropathy-related weakness distinctive is its pattern. It almost always starts in the feet and works its way up — a pattern neurologists call “stocking-glove distribution.” You might notice difficulty lifting your toes first (called foot drop), then gradually experience weakness higher up in the calves and thighs as the condition progresses through its stages.
The weakness is typically symmetrical — affecting both legs roughly equally. And critically, it's accompanied by sensory symptoms: numbness, tingling, burning, or that strange pins-and-needles feeling that many of us know too well. If your legs are weak AND your feet are numb, neuropathy moves to the top of the suspect list.
Common causes include diabetes (which accounts for about 30% of all neuropathy cases), vitamin deficiencies (especially B12), alcohol-related nerve damage, chemotherapy, and idiopathic neuropathy where the cause remains unknown despite testing.
Key Neuropathy Weakness Patterns
Neuropathy weakness tends to be gradual and progressive over months to years. It doesn't come and go in episodes — once you lose strength in a muscle group, it generally stays weak unless the underlying cause is addressed. The weakness worsens with longer distances (you may feel fine at the start of a walk but struggle after a quarter mile), and it doesn't improve with rest in the way that PAD-related weakness does.
One hallmark: neuropathy weakness is often accompanied by balance problems because the sensory nerves in your feet that tell your brain where the ground is are also damaged. Many people describe feeling like they're walking on cotton or sand.
Spinal Stenosis: When the Spine Squeezes the Nerves
Spinal stenosis causes leg weakness through a completely different mechanism — physical compression. The spinal canal (the tunnel of bone that protects your spinal cord and nerve roots) narrows due to age-related changes like osteoarthritis, thickened ligaments, or bulging discs. When the canal gets too tight, it squeezes the nerves, and your legs pay the price.
The Shopping Cart Test
Can you walk farther leaning on a shopping cart than walking upright? Spinal stenosis weakness is position-dependent — it improves when you bend forward and worsens when you stand straight. Cycling is often easier than walking for the same reason.
The classic presentation of lumbar spinal stenosis is something doctors call neurogenic claudication: leg weakness, pain, and heaviness that come on with walking or standing and improve when you sit down or lean forward. The “shopping cart sign” is a real clinical observation — people with spinal stenosis often feel better leaning on a grocery cart because the forward lean opens up the spinal canal slightly.
A 2020 review in Current Reviews in Musculoskeletal Medicine noted that the overlapping symptoms between spinal stenosis, peripheral neuropathy, and PAD make clinical diagnosis particularly challenging — especially in older adults who may have more than one of these conditions simultaneously.
Key Spinal Stenosis Weakness Patterns
The signature difference: spinal stenosis weakness is positional. It worsens with standing and walking (especially walking downhill or on flat surfaces) and improves with sitting, bending forward, or lying down. Cycling is often easier than walking because the bent-forward position relieves pressure on the spine.

Unlike neuropathy, the weakness pattern may not be symmetrical. If a disc is compressing a nerve root on one side, you might have weakness predominantly in one leg. And the weakness often follows a specific nerve root pattern (called a dermatome) — for example, L4 stenosis causes weakness in knee extension, while L5 stenosis causes difficulty lifting your foot.
Back pain is common but not universal with spinal stenosis. Some people have significant leg symptoms with minimal back pain, which can lead to delayed diagnosis. The key diagnostic clue: if your leg weakness gets reliably better when you sit and reliably worse when you stand or walk, spinal stenosis belongs high on the differential.
Multiple Sclerosis: When the Brain's Signals Get Disrupted
Multiple sclerosis (MS) causes leg weakness through demyelination — the immune system mistakenly attacks the myelin sheath (the protective coating around nerve fibers in the brain and spinal cord). Without intact myelin, nerve signals slow down, become distorted, or stop entirely.

MS-related leg weakness has a fundamentally different character from neuropathy or stenosis. It's often described as a heavy, dragging feeling — as if your legs are weighted down. The weakness tends to be more prominent in one leg initially and may be accompanied by spasticity (increased muscle tone that makes legs feel stiff and hard to bend).
According to the National Multiple Sclerosis Society, weakness or numbness in one or more limbs is one of the most common initial symptoms of MS, typically occurring on one side of the body at a time or in the legs and trunk.
Key MS Weakness Patterns
The most distinctive feature of MS-related weakness is its episodic nature, particularly in relapsing-remitting MS (the most common form). Weakness may appear suddenly over days, persist for weeks, then partially or fully resolve — only to return later, possibly affecting different parts of the body. This relapsing pattern is quite different from the steady progression of neuropathy or the position-dependent pattern of stenosis.
Heat sensitivity is another hallmark. Many people with MS experience worsening weakness in hot weather, after a hot shower, or during exercise — a phenomenon called Uhthoff's phenomenon. If your legs feel dramatically weaker after a warm bath, this is a significant clinical clue.
MS weakness also tends to affect the hip flexors and knee extensors prominently (making it hard to lift your leg or straighten your knee), and it's often accompanied by other neurological symptoms like vision changes, difficulty with coordination, bladder problems, or cognitive fog. The age of onset is typically younger than neuropathy or stenosis — most MS diagnoses occur between ages 20 and 50.
Peripheral Artery Disease: When Blood Can't Reach the Muscles
PAD causes leg weakness through a vascular mechanism — narrowed or blocked arteries can't deliver enough blood (and therefore oxygen) to the leg muscles during activity. When muscles don't get enough oxygen, they fatigue rapidly and feel weak.

The weakness from PAD is called vascular claudication, and it has a very specific signature: the legs feel fine at rest, but walking triggers cramping, aching, and weakness — typically in the calves, though it can affect the thighs and buttocks depending on where the arterial blockage is located. The critical distinction from spinal stenosis claudication: PAD improves with simply standing still (because rest reduces oxygen demand), while spinal stenosis requires a change in position (sitting or bending forward).
Risk factors for PAD closely mirror those for heart disease: smoking, diabetes, high blood pressure, high cholesterol, and age over 50. According to the American Heart Association, PAD affects approximately 8.5 million Americans over age 40, and many cases go undiagnosed because people attribute the symptoms to aging.
Key PAD Weakness Patterns
PAD weakness follows a predictable exertion pattern. You may be able to walk a specific distance — say, two blocks — before the weakness and cramping force you to stop. After resting for a few minutes (without needing to sit), the symptoms resolve and you can walk the same distance again. This reproducible “walk-pain-rest-walk” pattern is a hallmark of vascular claudication.
Physical signs can also help: look for cool skin on the affected leg, reduced or absent pulses in the feet, slow-healing wounds or sores on the toes or feet, and changes in skin color (pale or bluish). Hair loss on the legs and poor toenail growth are also clues. These signs reflect the overall poor blood supply, not nerve damage.
PAD typically doesn't cause numbness or tingling in the stocking-glove pattern that neuropathy does. However, severe PAD can eventually damage peripheral nerves due to chronic oxygen deprivation, creating a frustrating overlap where both conditions coexist — particularly common in people with diabetes.
The Differential Comparison: How Each Condition Stacks Up
Understanding these four conditions becomes much clearer when you see them side by side. Here's how the key features compare across all four causes of leg weakness.
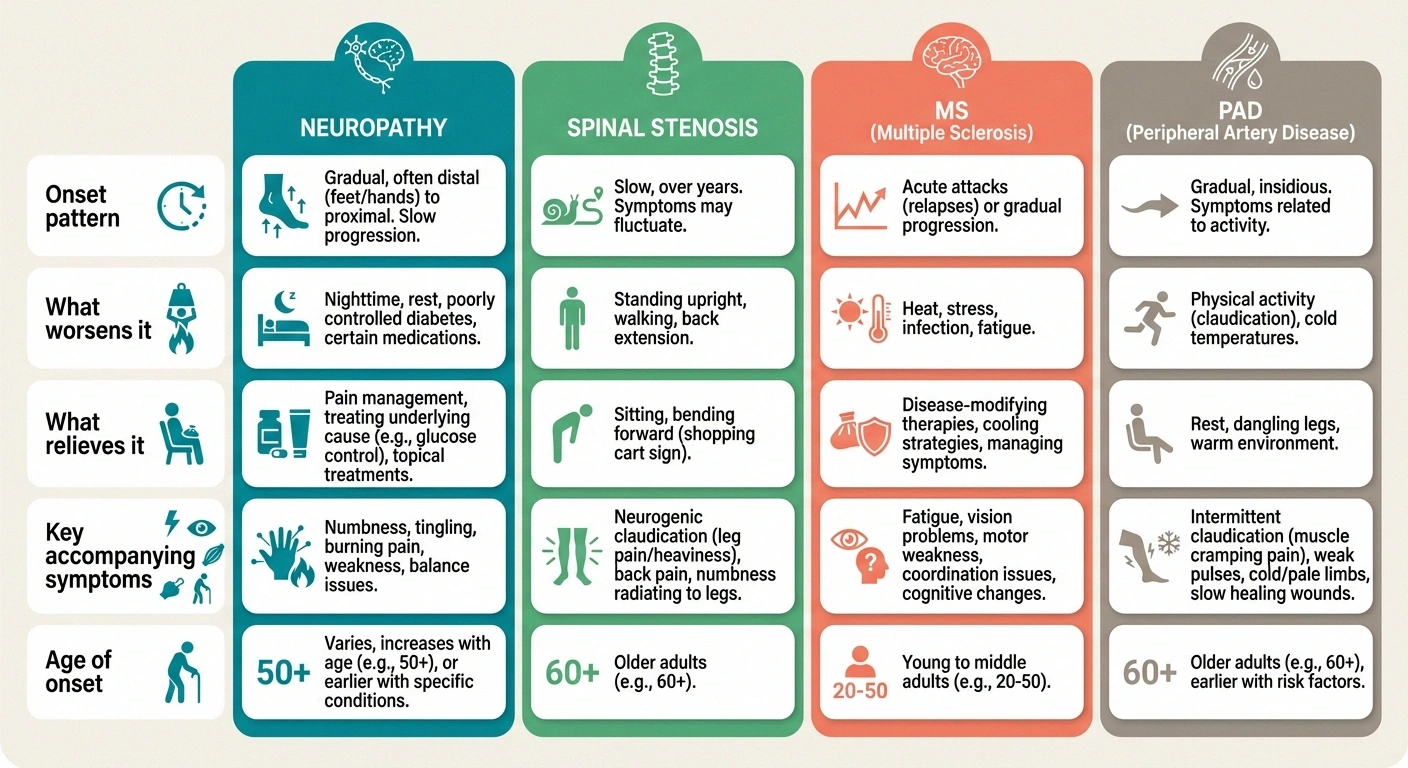
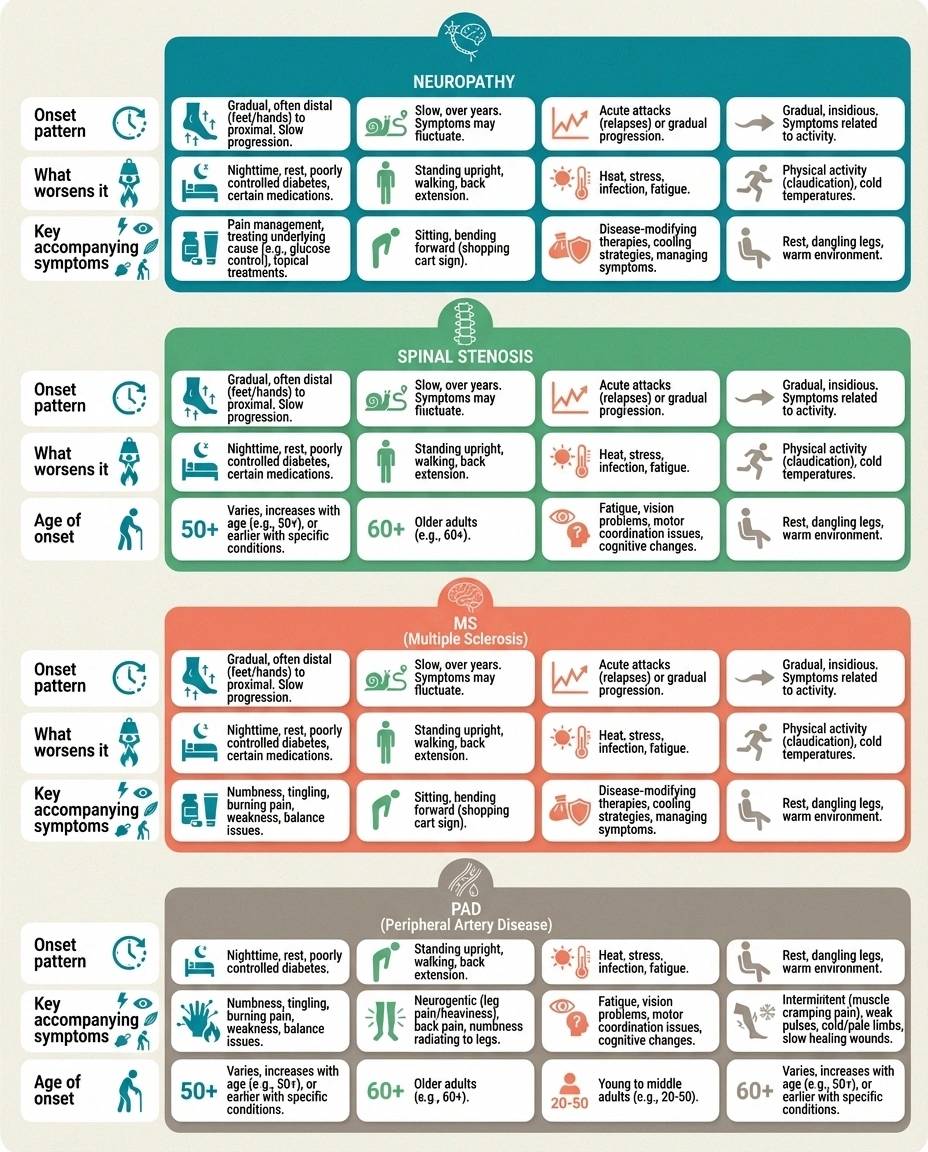
Onset and Progression
Neuropathy: Gradual onset over months to years. Steady progression unless the underlying cause is treated. Weakness starts in the feet and moves upward symmetrically.
Spinal Stenosis: Gradual onset, typically over months. Weakness is position-dependent — worse with standing and walking, better with sitting and bending forward. May be asymmetric.
MS: Can be sudden (over days) or gradual. Often episodic in the relapsing-remitting form — weakness comes and goes unpredictably. May affect one leg more than the other.
PAD: Gradual onset. Weakness is strictly activity-dependent — appears only during exertion and resolves with rest. Often affects the calves first.
What Makes Weakness Worse
Neuropathy: Prolonged walking or standing. Weakness doesn't significantly change with position changes.
Spinal Stenosis: Standing upright, walking (especially downhill), extending the spine backward.
MS: Heat exposure, fatigue, infection, and stress. Exercise may temporarily worsen weakness (Uhthoff's phenomenon).
PAD: Walking or any physical exertion. The weakness has a predictable “distance threshold” — it kicks in after a consistent amount of walking.
What Makes Weakness Better
Neuropathy: Addressing the underlying cause (blood sugar control, B12 supplementation). Physical weakness itself improves slowly if at all. Physical therapy can help maintain strength.
Spinal Stenosis: Sitting down, leaning forward, bending at the waist (opening the spinal canal). Cycling is often tolerated better than walking.
MS: Cooling the body, rest, and disease-modifying therapies. Episodes may resolve partially or fully over weeks.
PAD: Simply stopping and standing still for 2-5 minutes (unlike stenosis, which requires position change). Revascularization procedures can restore blood flow.
Accompanying Symptoms
Neuropathy: Numbness, tingling, burning in feet and hands (stocking-glove pattern). Balance problems. Sensitivity to touch. Foot sores that heal slowly.
Spinal Stenosis: Low back pain (though not always). Leg pain or cramping. Symptoms follow nerve root patterns. Numbness possible but usually follows a specific dermatome, not the stocking-glove pattern.
MS: Vision changes (optic neuritis), bladder dysfunction, fatigue, spasticity, coordination problems, cognitive changes. Symptoms typically affect multiple body systems.
PAD: Leg cramping during activity. Cool skin, weak pulses, skin color changes. Poor wound healing. Hair loss on legs. No numbness or tingling in the neuropathy pattern.
When Two Conditions Exist Together
Here's what makes this genuinely complicated: these conditions frequently coexist, especially in older adults. Someone with diabetes may have both peripheral neuropathy AND PAD. An older adult can have spinal stenosis AND neuropathy. The research literature calls this “diagnostic overlap,” and it's more common than you might think.
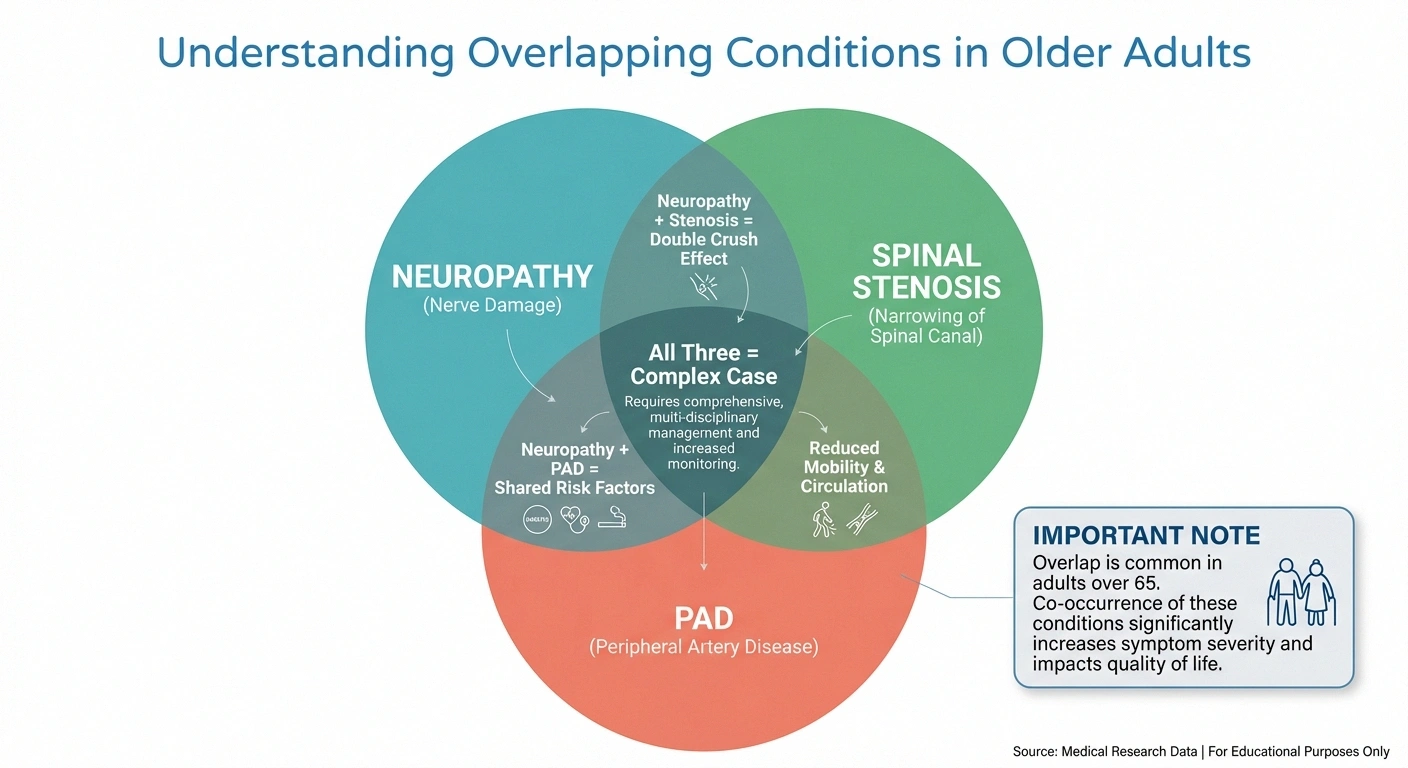
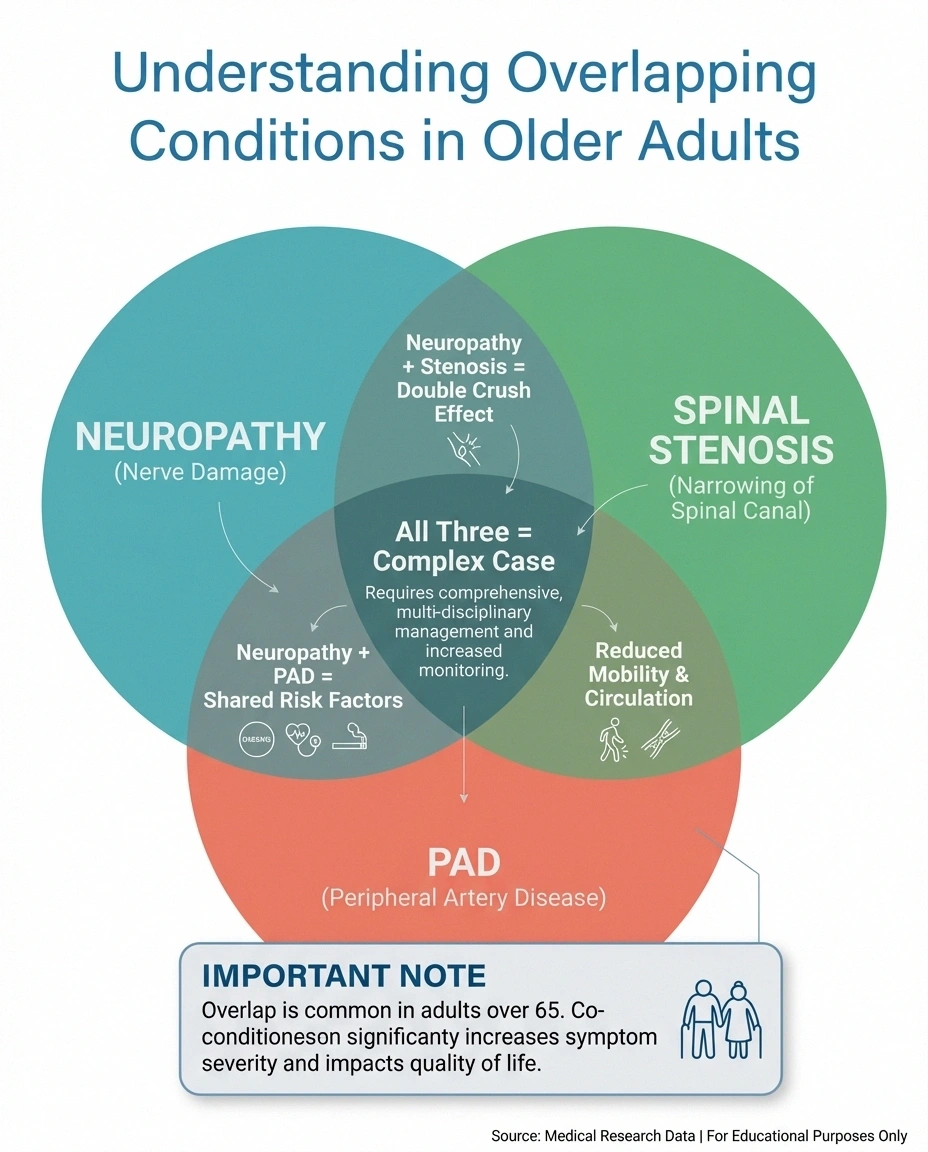
A study in the Journal of the American Podiatric Medical Association noted that spinal stenosis symptoms are “commonly misdiagnosed as peripheral neuropathy, especially in patients with diabetes.” When two conditions share the same risk factors and age group, they often show up together.
This is precisely why a thorough diagnostic workup matters. If your doctor treats only the most obvious condition and your symptoms don't fully resolve, it's worth asking whether a second condition might be contributing. The conversation with your doctor about these possibilities is one of the most valuable things you can do.
Diagnostic Tests: Getting a Definitive Answer
Each of these conditions has specific tests that can confirm or rule it out. Here's what your doctor may order.

Tests for Peripheral Neuropathy
Electromyography (EMG) and nerve conduction studies (NCS) are the gold standard. These tests measure how quickly and efficiently your nerves transmit electrical signals and whether your muscles respond normally. Blood tests can identify underlying causes — glucose levels for diabetes, B12 and folate levels, thyroid function, and inflammatory markers.
Tests for Spinal Stenosis
MRI of the lumbar spine is the primary imaging study. It shows the spinal canal dimensions, any disc herniations, bone spurs, or ligament thickening that might be compressing nerves. CT myelography is an alternative for patients who can't have an MRI. X-rays can show bony changes but don't visualize the soft tissue compression well.
Tests for MS
MRI of the brain and spinal cord is the cornerstone — MS lesions (areas of demyelination) appear as bright spots on specific MRI sequences. Cerebrospinal fluid analysis (obtained via lumbar puncture) may show oligoclonal bands that suggest immune system activity in the central nervous system. Visual evoked potentials can detect slowed nerve conduction in the optic nerve, even if vision seems normal.
Tests for PAD
The ankle-brachial index (ABI) is a simple, non-invasive office test that compares blood pressure in your ankle to blood pressure in your arm. A low ratio indicates reduced blood flow to the legs. Doppler ultrasound can visualize blood flow in the leg arteries. CT angiography or MR angiography provide detailed images of arterial blockages when surgery is being considered.
Red Flags: When Leg Weakness Needs Urgent Attention
Most leg weakness develops gradually and allows time for a proper diagnostic workup. However, certain patterns require immediate medical attention. Go to the emergency room if you experience sudden leg weakness that develops over minutes to hours, leg weakness accompanied by loss of bladder or bowel control (which may indicate cauda equina syndrome — a surgical emergency), weakness on one side of the body with facial drooping or speech changes (possible stroke), or rapidly progressive weakness ascending from the feet upward over days (possible Guillain-Barré syndrome).

Seek Emergency Care If
Sudden weakness over minutes/hours • Loss of bladder or bowel control • One-sided weakness with facial drooping or speech changes • Rapidly ascending weakness from feet upward over days. These are neurological emergencies — call 911 or go to the ER immediately.
These scenarios represent genuine neurological emergencies where rapid treatment can prevent permanent damage.
What to Tell Your Doctor
When you visit your doctor about leg weakness, the details you provide can significantly speed up the diagnostic process. Before your appointment, consider tracking these specifics in a symptom journal.
Prepare for Your Appointment
Track the Pattern
When did it start? Sudden or gradual? One leg or both?
Note Triggers & Relief
What makes it worse? Walking, standing, heat? What helps?
Document Other Symptoms
Numbness, tingling, back pain, vision changes, bladder issues?
List Medications & Conditions
Especially diabetes, high BP, high cholesterol, and all current meds.
Note when the weakness started and whether it came on suddenly or gradually. Track which activities make it worse and what makes it better. Pay attention to whether it affects one leg or both, and whether the weakness is constant or comes and goes. Document any other symptoms you've noticed — numbness, tingling, back pain, vision changes, bladder issues. List all your medications and medical conditions, especially diabetes, high blood pressure, or high cholesterol.
The more precise you can be, the faster your doctor can narrow the possibilities. “My left leg gets weak after walking about three blocks and gets better when I stop” gives your doctor a much clearer picture than “my legs feel weak.”
Treatment Approaches by Condition
Once you have a diagnosis, the treatment pathways diverge significantly — which is exactly why accurate diagnosis matters so much.
For neuropathy, treatment focuses on addressing the underlying cause (tight blood sugar control, B12 supplementation, eliminating toxin exposure) and managing symptoms. Physical therapy can help maintain muscle strength and improve balance. Medications like gabapentin or duloxetine may help with nerve pain but don't directly address weakness.
For spinal stenosis, conservative treatments include physical therapy (core strengthening and flexion-based exercises), epidural steroid injections, and activity modification. When conservative approaches fail, surgical decompression (laminectomy) can directly relieve the pressure on the nerves.
For MS, disease-modifying therapies (DMTs) aim to reduce relapses and slow disease progression. Physical therapy and rehabilitation help maintain function. Acute relapses may be treated with high-dose corticosteroids.
For PAD, lifestyle changes (smoking cessation, exercise, diet) are the foundation. Medications may include antiplatelet drugs, statins, and cilostazol for claudication symptoms. Severe cases may require angioplasty, stenting, or bypass surgery to restore blood flow.
Living with Leg Weakness: Practical Strategies
Regardless of the cause, there are practical steps that can help you manage leg weakness and maintain your independence. Exercise adapted to your condition is almost universally recommended — it maintains muscle mass, improves circulation, and can slow progression in several of these conditions.

Fall prevention is critical. leg weakness patterns that are not simple neuropathy significantly increases fall risk, and falls in older adults can have serious consequences. Simple home modifications — removing throw rugs, installing grab bars, ensuring good lighting, wearing supportive footwear — can make a meaningful difference. If you're experiencing significant balance issues, talk to your doctor about whether an assistive device like a cane or walker might be appropriate.
Don't underestimate the emotional impact of leg weakness. Losing physical capabilities you once took for granted is a genuine grief process. Support groups — whether for neuropathy, MS, or general chronic illness — can provide both practical advice and emotional connection with others who understand.
Frequently Asked Questions
Can neuropathy and spinal stenosis happen at the same time?
Yes, and this combination is particularly common in older adults with diabetes. The two conditions can coexist because they have different mechanisms — neuropathy damages the peripheral nerves themselves while stenosis compresses the nerve roots where they exit the spine. If treatment for one condition doesn't fully resolve your symptoms, ask your doctor about testing for the other.
How can I tell if my leg weakness is from neuropathy or PAD?
The rest test is a helpful clue. PAD weakness improves quickly when you stop walking and simply stand still for a few minutes, because the muscles no longer need as much oxygen. Neuropathy weakness does not improve with brief rest stops. Also, neuropathy usually includes numbness and tingling in the feet while PAD more commonly causes cramping and aching without the pins-and-needles sensation.
Does MS always cause leg weakness on both sides?
No. MS often affects one side of the body initially, which is actually one of its distinguishing features compared to neuropathy (which typically affects both sides symmetrically). However, as MS progresses, both sides may eventually be affected. The asymmetric onset is a clinical clue that helps differentiate MS from other causes.
What does the shopping cart sign mean for spinal stenosis?
The shopping cart sign refers to the observation that people with lumbar spinal stenosis feel better when leaning forward, such as when pushing a shopping cart. This posture opens up the spinal canal slightly, reducing pressure on the compressed nerves. If you notice you can walk further in the grocery store leaning on a cart than you can walking upright, this is a strong clue pointing toward spinal stenosis.
Is leg weakness always progressive?
Not necessarily. In MS, weakness may come and go in relapses, with partial or full recovery between episodes. Spinal stenosis weakness can remain stable for years or improve with treatment. Neuropathy progression depends heavily on the underlying cause — diabetic neuropathy may stabilize with good blood sugar control, while some toxic neuropathies may reverse once the toxin is removed. PAD weakness is progressive if the underlying vascular disease is not addressed.
Should I see a neurologist or a vascular specialist?
Start with your primary care doctor, who can perform initial screening tests and refer you appropriately. If numbness, tingling, or balance issues accompany the weakness, a neurologist is the right specialist. If the weakness is strictly exercise-related with no sensory symptoms and you have vascular risk factors, a vascular specialist may be more appropriate. In cases where the cause is unclear, your primary care doctor can coordinate between specialists.
The Bottom Line
Leg weakness is a symptom that demands investigation — not because every cause is dire, but because the four main culprits (neuropathy, spinal stenosis, MS, and PAD) each require fundamentally different treatment approaches. Getting the right diagnosis isn't just an academic exercise — it's the difference between treating the actual problem and chasing symptoms.

Pay attention to the pattern: does the weakness improve with rest or position changes? Is it symmetrical or one-sided? Does it come with numbness, back pain, or vision changes? These details are your diagnostic roadmap.
And please — don't wait for the weakness to become severe before seeking medical evaluation. Early diagnosis gives you the most treatment options and the best chance of maintaining your mobility and independence. Browse all our symptom guides for more help understanding what your body is telling you.


