
Neuropathy and Digestive Problems: The Gut-Nerve Connection
If you have neuropathy and also deal with bloating, constipation, nausea, or unpredictable digestion, these may not be separate problems. Your nervous system doesn't just control the feeling in your hands and feet — it runs the entire digestive tract. When neuropathy damages the nerves that manage digestion, your gut can become as unreliable as the tingling in your toes.
This is a connection that catches many people off guard. You might have been managing peripheral neuropathy symptoms for years without realizing that your chronic stomach issues are part of the same condition. Let's break down exactly how nerve damage affects digestion, what it looks like, and what you can do about it.
How Your Nervous System Controls Digestion
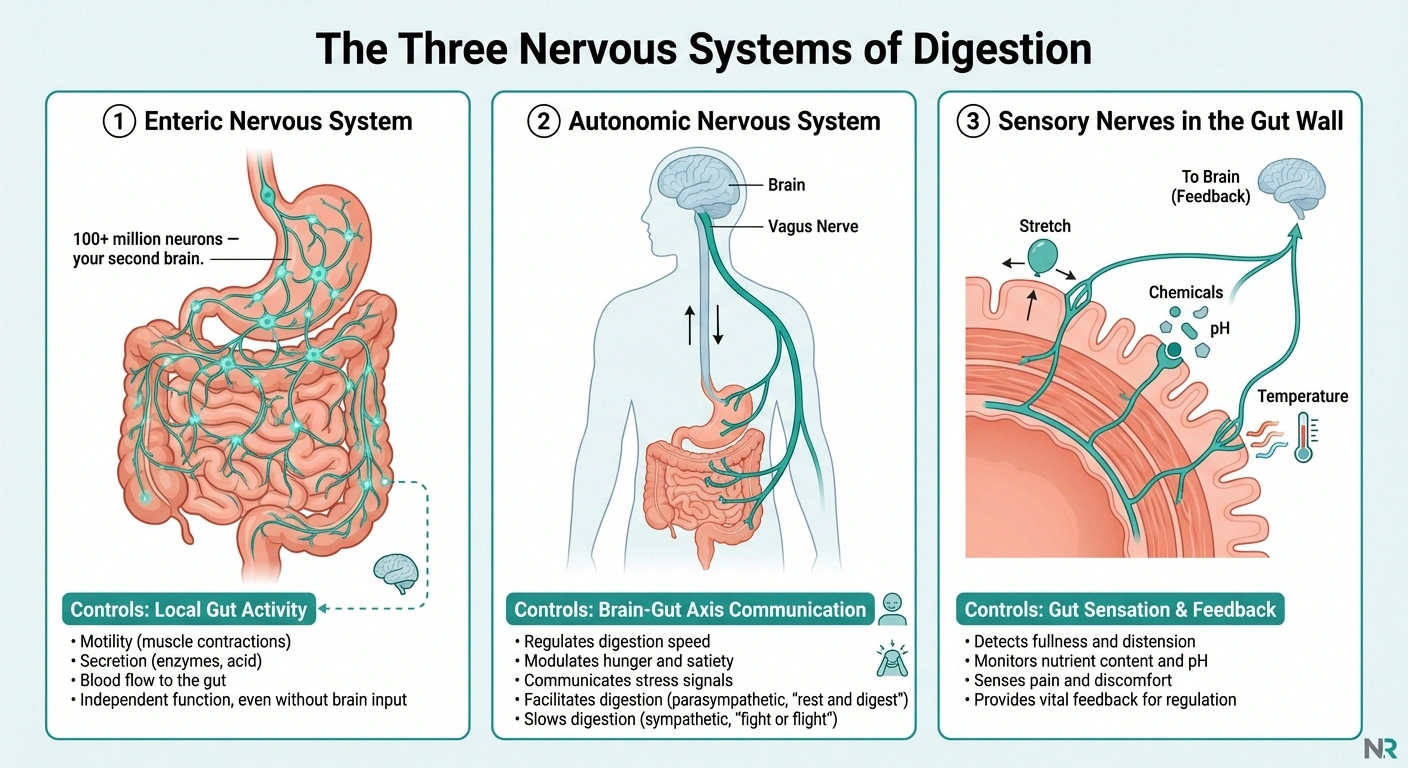
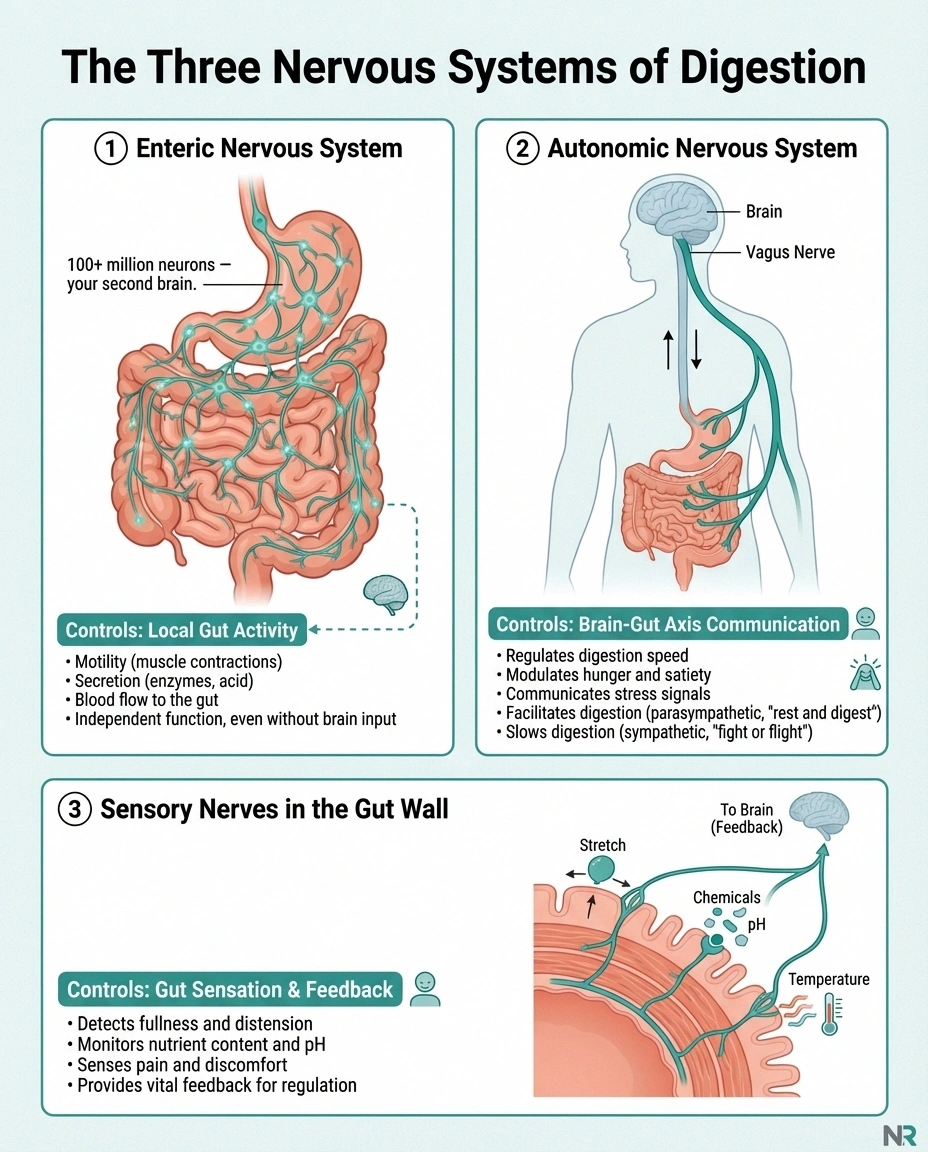
To understand why neuropathy causes digestive problems, you need to know about the three nervous systems involved in digestion:
The enteric nervous system (ENS) — sometimes called your “second brain” — is a vast network of over 100 million neurons embedded directly in the walls of your digestive tract. It controls the muscle contractions that move food through your gut (peristalsis), enzyme secretion, blood flow to the intestinal lining, and nutrient absorption. The ENS can operate independently of your brain, which is why it earned that “second brain” nickname.
The autonomic nervous system (ANS) — specifically the vagus nerve and sympathetic nerves — provides the communication bridge between your brain and your gut. The vagus nerve is the major highway: it carries signals from the brain to the digestive system and feedback from the gut back to the brain. It regulates stomach acid production, digestive enzyme release, gut motility, and the inflammatory response in the digestive tract.
Sensory nerves in the gut wall — these detect stretch (fullness), chemical changes, temperature, and pain. When they work properly, they tell you when you're full, when something you ate isn't agreeing with you, and when to stop eating. When they're damaged, these signals become unreliable or absent.
Neuropathy can damage any or all of these nerve networks, leading to a cascade of digestive dysfunction.
Types of Neuropathy That Affect Digestion
Three distinct types of neuropathy can cause digestive problems:
Autonomic Neuropathy
Autonomic neuropathy damages the nerves that control involuntary body functions, including digestion. When the vagus nerve and its branches are affected, the entire digestive system can slow down or become disorganized. This is the most common type of neuropathy responsible for gut symptoms, particularly in people with diabetes.
Diabetic autonomic neuropathy affects up to 75% of people with long-standing diabetes, though digestive symptoms are often attributed to other causes and go unrecognized as neuropathy-related for years.
Enteric Neuropathy
Enteric neuropathy involves damage to the neurons within the gut wall itself. Because the enteric nervous system has its own network of over 100 million neurons, damage here can cause severe digestive dysfunction even when the peripheral nerves in your hands and feet are functioning normally. Enteric neuropathy can be caused by diabetes, autoimmune conditions, infections, or aging.
Peripheral Neuropathy with Autonomic Overlap
Many people with peripheral neuropathy affecting their hands and feet also develop autonomic involvement without realizing it. The same disease process — whether diabetes, autoimmune disease, or nutritional deficiency — that damages sensory nerves can simultaneously damage autonomic nerves, including those serving the digestive system. If you have small fiber neuropathy, autonomic involvement is particularly common because the same small fibers that carry pain signals also control autonomic functions.
Common Digestive Symptoms Caused by Neuropathy
Nerve damage can affect every stage of digestion, from swallowing to elimination. Here's what to watch for:
Gastroparesis (Delayed Stomach Emptying)
Gastroparesis is perhaps the most well-known digestive complication of neuropathy. When the vagus nerve is damaged, the stomach muscles can't contract normally, and food sits in the stomach far longer than it should. Symptoms include:
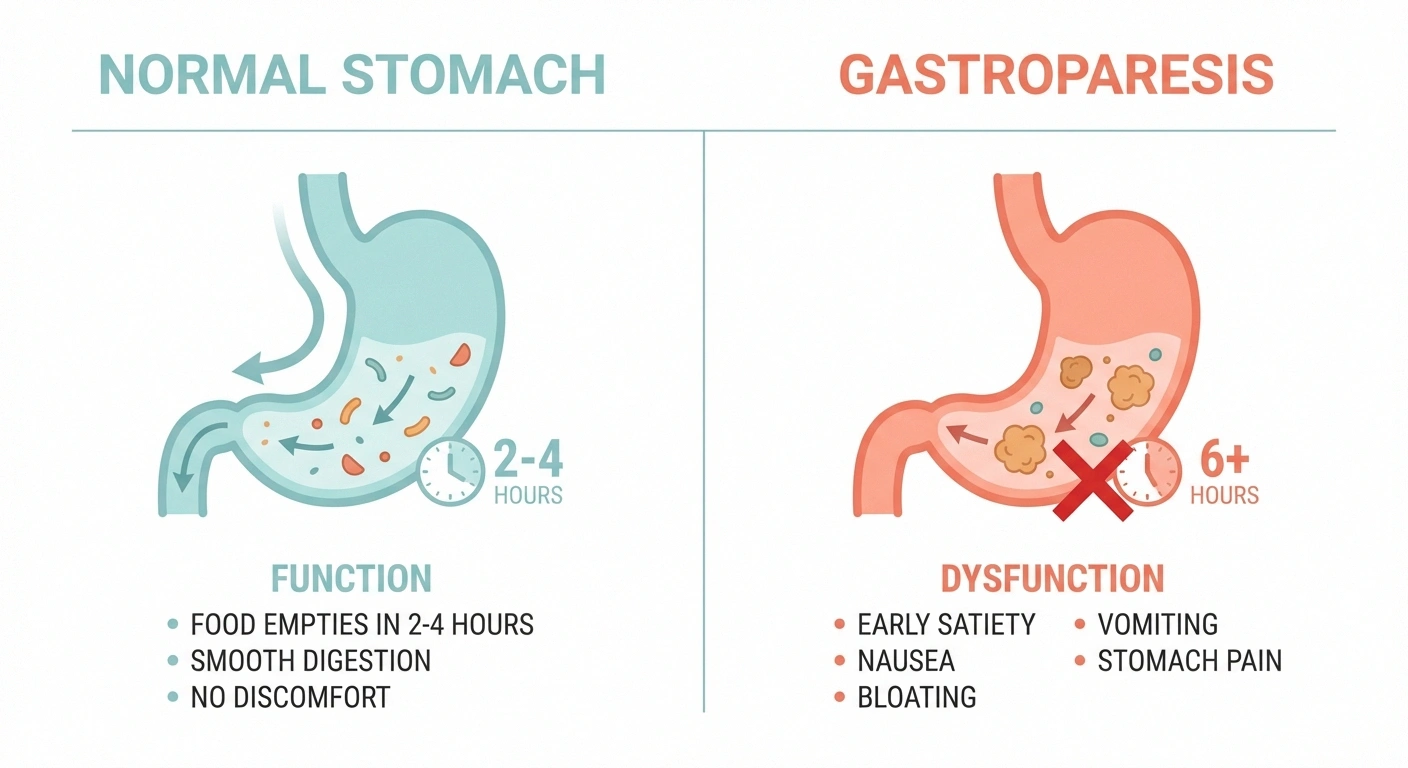
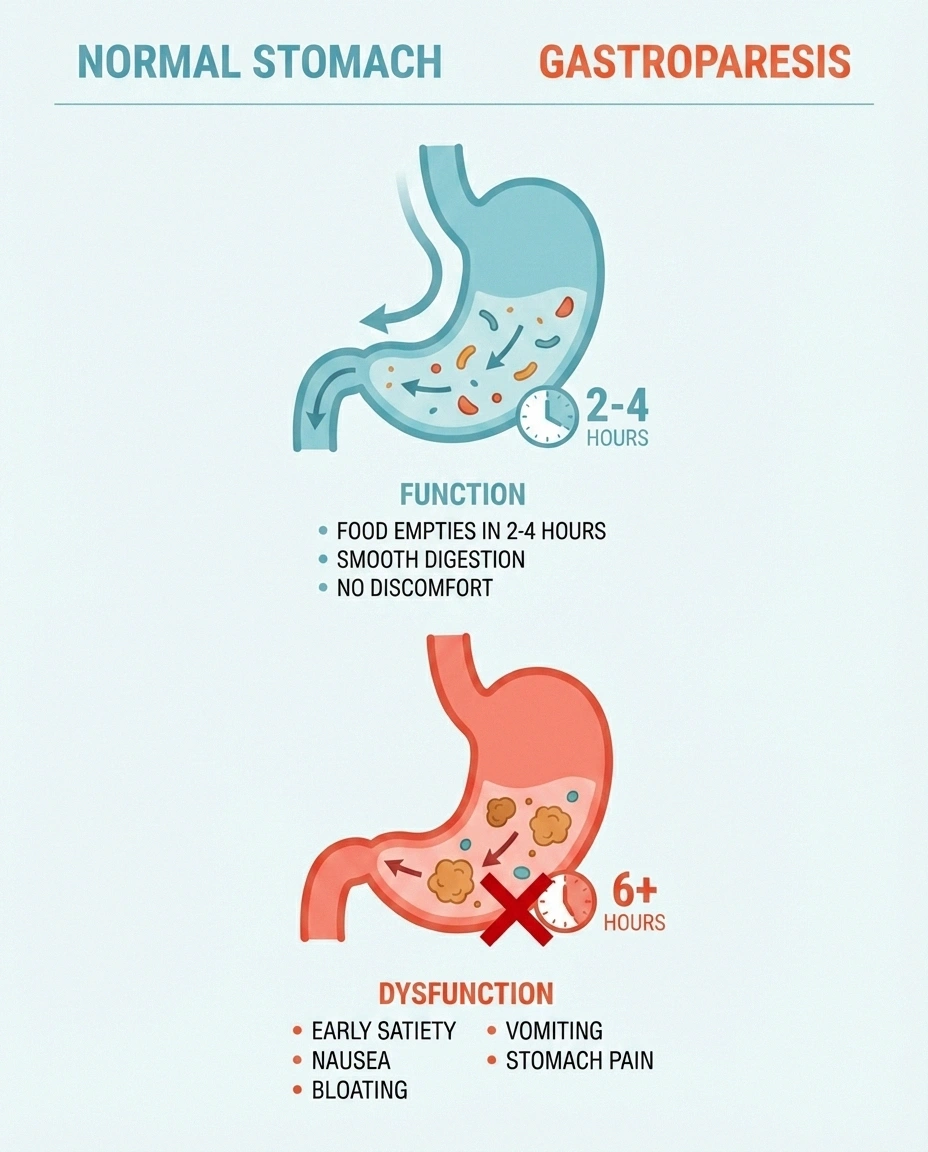
- Feeling full after just a few bites of food (early satiety)
- Nausea, especially after eating
- Vomiting undigested food hours after a meal
- Bloating and upper abdominal pain
- Acid reflux
- Unpredictable blood sugar levels (for people with diabetes)
Gastroparesis affects up to 40% of people with long-standing type 1 diabetes and up to 30% of people with type 2 diabetes who have other neuropathy complications.
Constipation
Neuropathy-related constipation happens when damaged nerves can't properly coordinate the muscle contractions that move food through the intestines. The colon may not contract forcefully enough, or the timing of contractions becomes disorganized. This leads to slow transit, hard stools, infrequent bowel movements, and a sense of incomplete evacuation. It's one of the most common digestive complaints in people with autonomic neuropathy.
Diarrhea
Paradoxically, neuropathy can also cause diarrhea — sometimes alternating with constipation. When the nerves controlling intestinal motility malfunction, the gut can alternate between periods of sluggishness and periods of overactivity. Neuropathic diarrhea is often nocturnal (worse at night), watery, and can come on suddenly with little warning. Bacterial overgrowth in a sluggish gut can also contribute to diarrhea episodes.
Difficulty Swallowing (Dysphagia)
The esophagus relies on coordinated nerve-controlled muscle contractions to push food from your throat to your stomach. When these nerves are damaged, you may notice food feeling like it's “sticking” in your throat or chest, difficulty swallowing pills, or a sensation of food going down slowly.
Bloating and Abdominal Distension
When the gut slows down, food ferments longer than it should, producing excess gas. The damaged nerves may also fail to coordinate the normal gas-moving contractions that distribute and expel gas. The result is persistent bloating that seems disproportionate to what you've eaten.
Bowel Urgency and Incontinence
Neuropathy can damage the nerves that control the anal sphincter and the sensory nerves that warn you when you need to have a bowel movement. This can lead to fecal urgency (sudden, intense need to go) or even fecal incontinence. These symptoms are often the most distressing and least discussed, but they're a direct consequence of autonomic nerve damage.
The Gut-Brain Axis: A Two-Way Street
The relationship between neuropathy and digestive problems runs in both directions. Not only can neuropathy cause digestive symptoms — gut problems can potentially worsen neuropathy:
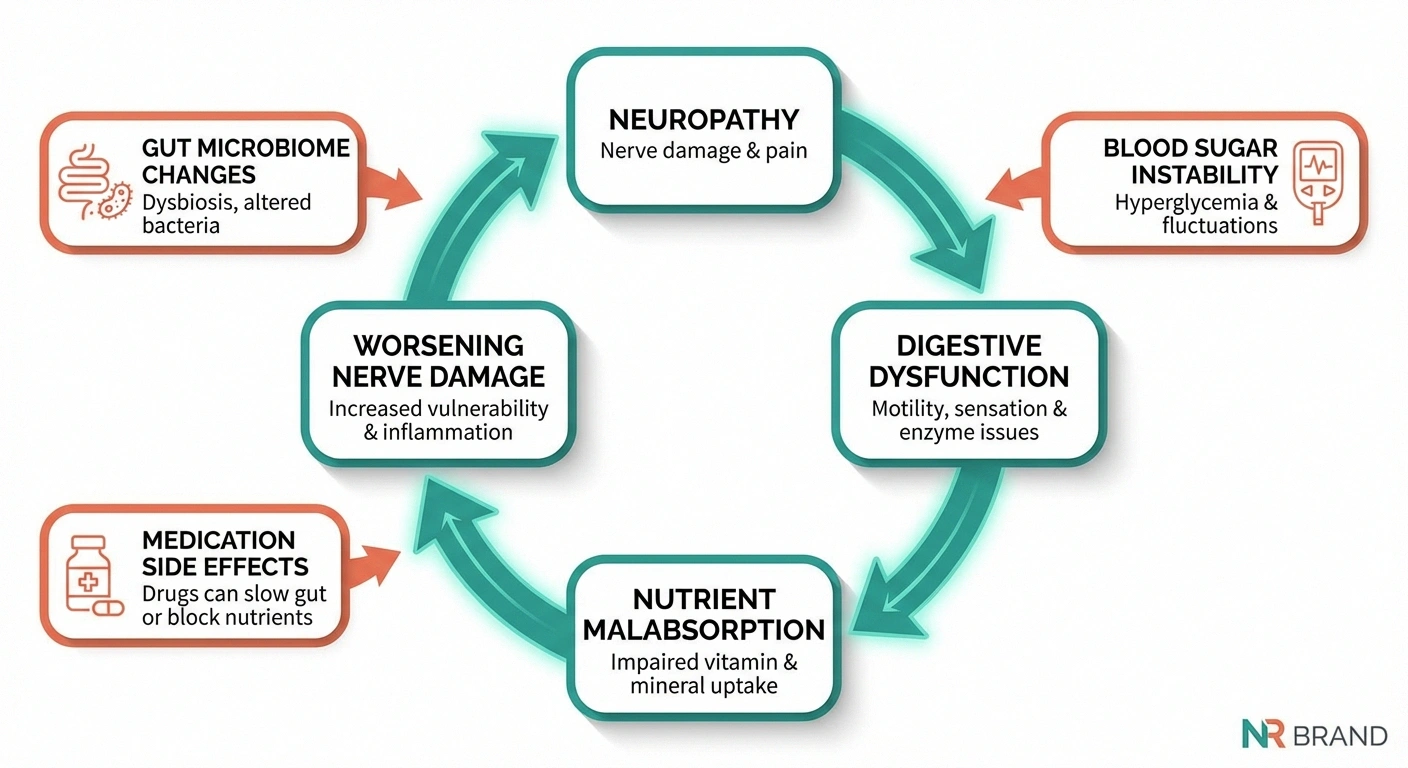
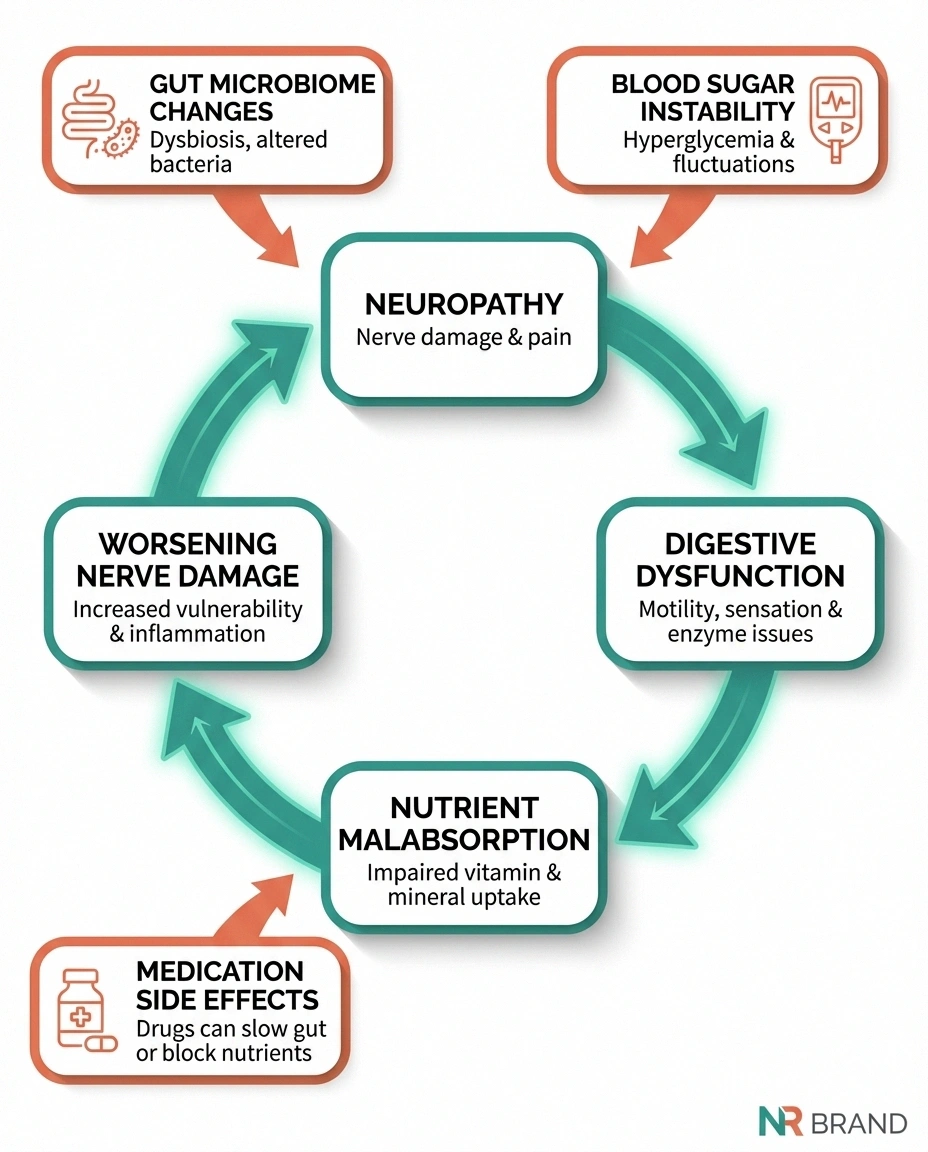
Nutrient malabsorption: When the gut isn't working properly, you may not absorb adequate B vitamins, key nutrients for nerve health, or minerals like magnesium and zinc. This creates a vicious cycle where digestive dysfunction worsens the nutritional deficiencies that drive further nerve damage.
Gut microbiome changes: Neuropathy-related gut dysfunction — slow transit, bacterial overgrowth, altered motility — changes the composition of your gut bacteria. Emerging research suggests that gut microbiome imbalances may promote systemic inflammation and directly influence peripheral nerve function through the gut-nerve axis.
Medication complications: Many neuropathy medications, including gabapentin, pregabalin, and tricyclic antidepressants, list constipation as a common side effect. If you already have neuropathy-related constipation, these medications can make it significantly worse.
Blood sugar instability: For people with diabetes, gastroparesis makes blood sugar control extremely difficult. Food absorbs unpredictably, causing blood sugar spikes and drops that don't match insulin timing. Poor blood sugar control, in turn, accelerates nerve damage — another vicious cycle.
Getting the Right Diagnosis
If you have neuropathy and digestive symptoms, getting the right diagnosis is important because it changes treatment. Tests your doctor may recommend:

Gastric emptying study: The gold standard for diagnosing gastroparesis. You eat a meal containing a small amount of radioactive tracer, and imaging shows how quickly food leaves your stomach. Delayed emptying confirms gastroparesis.
Autonomic function testing: A battery of tests that evaluate the autonomic nervous system, including heart rate variability, blood pressure response to standing, and sudomotor (sweat) testing. Abnormal results confirm autonomic neuropathy and help explain digestive symptoms.
Hydrogen breath test: Detects small intestinal bacterial overgrowth (SIBO), which commonly develops when neuropathy slows gut motility. SIBO causes bloating, gas, diarrhea, and malabsorption.
Esophageal manometry: If swallowing difficulty is prominent, this test measures the pressure and coordination of muscle contractions in the esophagus.
Colonoscopy or defecography: May be recommended if constipation or bowel dysfunction is severe, to rule out structural causes.
Treatment and Management Strategies
Managing neuropathy-related digestive problems typically involves a combination of dietary modifications, medications, and addressing the underlying neuropathy itself.
Dietary Adjustments
For gastroparesis: Eat smaller, more frequent meals (5-6 small meals instead of 3 large ones). Choose low-fat, low-fiber foods that are easier to digest. Cooked vegetables are better tolerated than raw. Avoid carbonated drinks and high-fat meals that slow emptying further. Some people find that liquid or pureed meals are better tolerated during flares.

For constipation: Increase water intake (aim for 8+ glasses daily). Add soluble fiber gradually — psyllium husk is often better tolerated than insoluble fiber. Prunes and prune juice contain natural sorbitol that can help. Establish a regular mealtime routine, as eating stimulates the gastrocolic reflex that triggers bowel movements.
For diarrhea: Avoid artificial sweeteners (especially sorbitol and mannitol), limit caffeine, and consider a low-FODMAP elimination diet to identify trigger foods. Small, frequent meals are generally better tolerated than large ones.
Medications
Prokinetic agents: Metoclopramide (Reglan) is the most commonly prescribed medication for gastroparesis. It helps the stomach muscles contract more effectively and moves food through faster. However, it has significant side effects with long-term use, including a risk of tardive dyskinesia (involuntary movements). Domperidone is an alternative used in some countries. Erythromycin at low doses also has prokinetic effects.
Anti-nausea medications: Ondansetron (Zofran) and promethazine can help manage the nausea associated with gastroparesis.
Laxatives for constipation: Osmotic laxatives like polyethylene glycol (MiraLAX) are generally safe for regular use. Stimulant laxatives should be used more cautiously. Linaclotide (Linzess) and prucalopride (Motegrity) are prescription options specifically designed for chronic constipation.
Antidiarrheals: Loperamide (Imodium) can help manage neuropathic diarrhea. Bile acid sequestrants like cholestyramine may help if bile acid malabsorption is a contributing factor.
Addressing the Root Cause
The most important step is treating the condition that's causing the neuropathy:
- Diabetes: Tight blood sugar control can slow the progression of autonomic neuropathy and may improve existing symptoms. For people with diabetic neuropathy, every point of HbA1c reduction matters.
- Autoimmune conditions: Treatment with immunosuppressive or immunomodulatory therapy may reduce the autoimmune attack on autonomic nerves.
- Nutritional deficiencies: Correcting B12, B1 (thiamine), and other nutritional deficiencies can improve autonomic nerve function. B12 injections may be necessary if oral absorption is impaired.
- Alcohol: Stopping alcohol consumption can halt further autonomic nerve damage and allow partial recovery.
Living with Neuropathy-Related Digestive Problems
Day-to-day management requires patience and adaptation. Some practical strategies that help:

- Keep a food and symptom diary — identify which foods consistently cause problems and which are well-tolerated. Patterns often emerge that aren't obvious without tracking.
- Stay upright after eating — gravity helps stomach emptying. Avoid lying down for at least 2-3 hours after meals.
- Walk after meals — even a gentle 10-15 minute walk stimulates gut motility and can reduce bloating.
- Manage stress — the gut-brain axis means that stress directly worsens digestive symptoms. Mindfulness and relaxation techniques can provide measurable improvement.
- Plan ahead for outings — know where bathrooms are located, carry emergency supplies if bowel urgency is an issue, and don't let embarrassment keep you from managing your condition proactively.
- Communicate with your doctor about medication side effects — if your neuropathy pain medications are worsening constipation, there may be alternatives with fewer GI side effects.
When to Seek Urgent Medical Attention
While most neuropathy-related digestive symptoms are manageable, certain situations require immediate medical attention:
• Significant unexplained weight loss
• Blood in stool or vomit
• Severe abdominal pain that doesn't resolve
• Signs of dehydration (dark urine, dizziness, dry mouth)
• No bowel movement for more than a week despite treatment
- Severe, persistent vomiting that prevents keeping any food or fluids down
- Significant unexplained weight loss
- Blood in your stool or vomit
- Severe abdominal pain that doesn't resolve
- Signs of dehydration (dark urine, dizziness, dry mouth)
- Inability to have a bowel movement for more than a week despite treatment
These could indicate complications that need more aggressive intervention, including hospitalization for rehydration, gastric decompression, or further diagnostic evaluation.
The Bottom Line
If you're living with neuropathy and struggling with digestive problems, know that these symptoms are likely connected — and treatable. Autonomic and enteric neuropathy are real, recognized conditions with established diagnostic pathways and management strategies. You don't have to simply accept chronic digestive distress as “just part of having neuropathy.”
Start by talking to your doctor about the connection between your nerve condition and your gut symptoms. Ask about autonomic testing, a gastric emptying study if gastroparesis is suspected, and a review of your current medications for GI side effects. With the right diagnosis and a targeted management plan, most people see meaningful improvement in their digestive symptoms.
Frequently Asked Questions
Can peripheral neuropathy cause stomach problems?
Yes. While peripheral neuropathy is most commonly associated with symptoms in the hands and feet, the same disease process often damages autonomic nerves that control digestion. Autonomic neuropathy can cause gastroparesis, constipation, diarrhea, bloating, nausea, and other digestive issues. This is especially common in people with diabetic neuropathy, where autonomic involvement affects up to 75% of long-standing cases.
What is gastroparesis and how is it related to neuropathy?
Gastroparesis is a condition where the stomach empties food too slowly due to damaged vagus nerve signals that normally coordinate stomach muscle contractions. It causes nausea, early fullness, vomiting, bloating, and unpredictable blood sugar levels. It affects up to 40% of people with long-standing type 1 diabetes and is one of the most common digestive complications of autonomic neuropathy.
Can gut problems make neuropathy worse?
Yes. Digestive dysfunction can impair absorption of B vitamins, magnesium, and other nutrients essential for nerve health, creating a vicious cycle where gut problems worsen nutritional deficiencies that drive further nerve damage. Gut microbiome imbalances from slow transit may also promote systemic inflammation that affects peripheral nerves. Managing digestive symptoms is important not just for comfort but for protecting remaining nerve function.
Should I change my neuropathy medication if it's causing constipation?
Talk to your doctor before making any changes. Many neuropathy medications, including gabapentin, pregabalin, and tricyclic antidepressants, can worsen constipation. Your doctor may adjust the dose, switch to an alternative with fewer GI side effects (duloxetine tends to cause less constipation), or add a targeted treatment for constipation alongside your pain medication. Do not stop neuropathy medications abruptly without medical guidance.
What diet is best for neuropathy-related digestive problems?
There is no single ideal diet, but general principles help. Eat smaller, more frequent meals to reduce the burden on a sluggish digestive system. Choose low-fat, moderate-fiber foods that are easier to digest. Cooked vegetables are better tolerated than raw. Stay well hydrated. Avoid carbonated beverages, artificial sweeteners, and very high-fat meals. A food and symptom diary is the best tool for identifying your personal trigger foods.
Is neuropathy-related bloating different from IBS?
They can look very similar, and some people with neuropathy are misdiagnosed with IBS for years. The key difference is the underlying cause: IBS involves a dysregulation of the gut-brain axis without structural nerve damage, while neuropathy-related bloating is caused by measurable nerve dysfunction. Autonomic testing and a gastric emptying study can help distinguish between the two. If you have peripheral neuropathy and IBS-like symptoms, ask your doctor about autonomic neuropathy testing.


