
A bedsheet. A breeze from an open window. A hug from your grandchild. For most people, these are small, unremarkable moments of daily life.
For people living with allodynia, they can be excruciating.
Allodynia is one of the cruelest manifestations of nerve damage — the experience of pain from things that shouldn't hurt at all. A light touch that sends electric agony through the skin. A cool breeze that feels like a burn. The weight of fabric against the feet that makes simply getting dressed an ordeal.
What makes allodynia particularly hard to live with isn't just the pain itself. It's that it's so difficult to explain. When you tell someone that a light touch hurts you, that you can't bear the weight of a blanket at night, that you wince when the wind catches your sleeve — people who haven't experienced it struggle to understand. It sounds impossible. Dramatic, even.
It isn't. It's a real neurological phenomenon, it has a name, it has identifiable causes, and it has treatments that can genuinely help. Let me walk you through what's actually happening in your nervous system when allodynia strikes — and what you can do about it.
What Is Allodynia, Exactly?
Allodynia is defined as pain produced by a stimulus that doesn't normally cause pain. The word comes from the Greek: allos (other) and odynia (pain). Pain from something “other” — something that isn't supposed to hurt.
Key Takeaway
Allodynia isn't about the stimulus — it's about how the nervous system is processing it. The pain is real, the mechanism is neurological, and there are effective treatments. Understanding the “why” is the first step toward managing it better.
It's not the same as hyperalgesia, which is an exaggerated response to something that IS already painful. With hyperalgesia, a pinprick hurts much more than it should. With allodynia, a gentle touch that shouldn't hurt at all registers as pain. The distinction matters for treatment.
There are three main types of allodynia:
- Tactile allodynia (also called mechanical static allodynia) — pain from light touch or pressure. The pressure of clothing against the skin. A hand resting on your arm. A doctor's touch during examination.
- Dynamic mechanical allodynia — pain specifically from things moving across the skin. A brush of fabric. Running a finger across the forearm. Wind across exposed skin. Often more severe than static allodynia.
- Thermal allodynia — pain from temperatures that should be comfortable or neutral. A warm bath that feels like scalding. A cool glass held in the hand that produces burning pain.
Many people with neuropathic allodynia experience more than one type simultaneously, which compounds the difficulty of daily life considerably.
Why Does Touch Become Painful? The Neuroscience
To understand allodynia, it helps to understand something about how normal pain processing works — and what goes wrong in neuropathy.
The Three Types of Allodynia
Tactile Allodynia
Pain from light touch or pressure — clothing contact, a gentle handshake, a doctor's touch during examination.
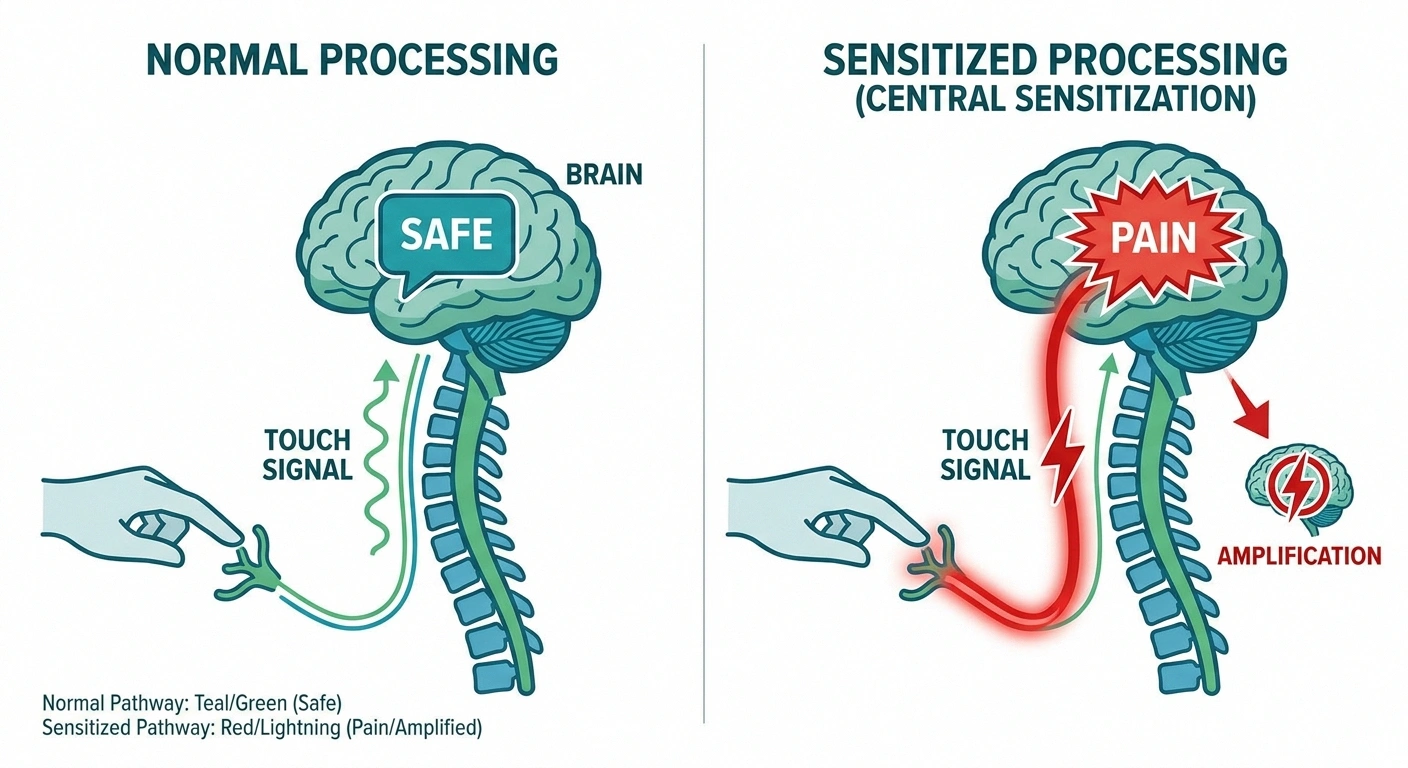
In a healthy nervous system, there's a clear separation between the signals that travel to your brain from light touch (carried by A-beta fibers) and the signals from pain stimuli (carried by A-delta and C fibers). Your brain knows the difference, and it processes them completely differently. Light touch registers as sensation. Pain stimuli register as pain.
In allodynia, something goes wrong with that processing. Damaged nerves can begin firing spontaneously and erratically. Signals get crossed. The spinal cord undergoes changes — a process called central sensitization — in which pain-processing neurons in the spinal cord become hyperexcitable. The “volume” of the pain system gets turned up.
The result is that signals from light touch, which were previously filtered and processed as “harmless,” now get amplified and misinterpreted as pain. The stimulus hasn't changed. The processing has.
Central sensitization also explains another phenomenon many people with allodynia experience: wind-up, where repeated stimulation makes the pain progressively worse during a single exposure, even if the intensity of the stimulus doesn't change. Your spinal cord neurons are essentially being primed to fire harder and harder.
This is important because it explains why allodynia isn't simply about the peripheral nerves. Even if you could repair the damaged nerve endings, the sensitization that's developed in the spinal cord and brain can persist and perpetuate the pain. Treatment often needs to address both peripheral nerve health and the central sensitization component.
What Causes Allodynia in Neuropathy?
Allodynia isn't a condition unto itself — it's a symptom that arises from underlying nerve damage. The conditions most commonly associated with allodynia include:
Allodynia vs. Hyperalgesia: Understanding the Difference
| Allodynia | Hyperalgesia | |
|---|---|---|
| Trigger | Non-painful stimulus (light touch, gentle warmth) | Painful stimulus (pinprick, heat) |
| Response | Pain where there should be none | Exaggerated pain response |
| Example | A blanket touching your feet hurts | A pinprick feels like a stab wound |
- Diabetic neuropathy — one of the most common causes of neuropathic allodynia; uncontrolled blood sugar damages the small nerve fibers responsible for sensory processing
- Post-herpetic neuralgia — allodynia after shingles can be among the most severe forms; the post-herpetic neuralgia article covers this in detail
- Chemotherapy-induced peripheral neuropathy (CIPN) — certain chemotherapy agents cause significant small fiber damage; allodynia is a hallmark complaint
- Fibromyalgia — widespread central sensitization makes touch painful throughout the body
- Complex Regional Pain Syndrome (CRPS) — allodynia is a core diagnostic feature of CRPS, often extreme
- Small fiber neuropathy — damage to the smallest sensory nerve fibers leads to burning and allodynia
- HIV-associated neuropathy
- Lyme disease neuropathy
- Idiopathic neuropathy — sometimes allodynia develops without a clear identifiable cause
In each case, the pathway is similar: nerve damage → disrupted sensory signaling → central sensitization → allodynia. But the specific type of nerve affected and the extent of central changes vary, which is why treatment response varies between individuals and conditions.
How Allodynia Affects Daily Life
I want to spend a moment on this, because medical resources often describe allodynia in clinical terms without capturing what it's actually like to live with it day to day.

Important
Allodynia is frequently misunderstood — even by healthcare providers. If touch causes you pain and others seem skeptical, know that this is a documented neurological phenomenon with measurable mechanisms. You are not imagining it, and you are not exaggerating. Advocate clearly for proper evaluation and treatment.
Clothing is one of the biggest challenges. Seams, elastic waistbands, sock cuffs, shoe uppers — all of these can become sources of constant irritation or outright pain. Many people with allodynia gravitate toward seamless socks (which are available specifically for this), tagless shirts, loose-fitting fabrics, and softer materials like bamboo and modal. Getting dressed stops being an automatic, mindless activity and becomes a careful, deliberate process.
Bedding is another major issue. The weight of even a light blanket over the feet and lower legs can make sleep nearly impossible. Foot cradles — wire frames that hold the covers up off the feet — can be genuinely helpful, and we mention them here for anyone who hasn't encountered them. Our article on why neuropathy gets worse at night touches on the sleep disruption this creates.
Bathing and temperature changes can be difficult. The transition from air to water, even water at a temperature that should feel comfortable, can trigger burning sensations. Warm baths are painful for some while soothing for others — there's no universal answer, and finding your own thermal sweet spot takes experimentation.
Physical affection — hugs, hand-holding, a reassuring touch — becomes complicated. This is one of the harder things to communicate to family members, who may feel confused or rejected when their touch causes pain. Explaining allodynia to loved ones, and finding ways to be close that don't trigger it, matters enormously for relationships and emotional wellbeing.
Medications That Help Allodynia
The pharmacological options for allodynia are largely the same medications used for neuropathic pain more broadly, but some have specific evidence for allodynia in particular.

Gabapentinoids
Gabapentin and pregabalin are often the first medications tried for allodynia. They work by modulating calcium channels in nerve cells, reducing the hyperexcitable signaling that underlies central sensitization. Many patients report that these medications reduce the intensity of allodynia — fabrics feel less agonizing, touch becomes tolerable — even if they don't eliminate the symptoms entirely.
Tricyclic Antidepressants
Amitriptyline and nortriptyline, at low doses much lower than their antidepressant doses, can be highly effective for neuropathic pain and allodynia. They work through multiple mechanisms including sodium channel blockade and serotonin/norepinephrine reuptake inhibition. The main drawbacks are sedation (which is why they're taken at night) and dry mouth.
SNRIs
Duloxetine (Cymbalta) enhances descending pain inhibition — essentially activating the brain's own pain-suppression circuits — and has FDA approval for diabetic neuropathic pain. It can be particularly helpful for the allodynia that accompanies diabetic neuropathy.
Topical Treatments
Lidocaine patches or gel applied directly to the allodynic area can provide meaningful local relief without systemic side effects — an advantage for people who are sensitive to oral medications. Capsaicin cream or high-concentration patches desensitize the nerve endings over time through a counterintuitive process: capsaicin initially activates pain fibers intensely, then depletes the chemical messengers that keep those fibers reactive, leaving them temporarily less sensitive. High-concentration capsaicin patches (8%, applied by a clinician) can provide weeks to months of relief from allodynia in post-herpetic neuralgia and HIV neuropathy.
Other Medications
Tramadol has some effectiveness for neuropathic pain, including allodynia, through opioid and norepinephrine/serotonin mechanisms. In cases of severe, refractory allodynia, a pain specialist may consider other approaches including low-dose naltrexone, ketamine infusions, or spinal cord stimulation.
Non-Medication Approaches That Make a Real Difference
Some of the most powerful interventions for allodynia work not through chemicals but through gradually recalibrating the nervous system's response to touch.

Research Says
Central sensitization — the nervous system “volume dial” turned up too high — is the primary driver of allodynia in neuropathy. Research shows that treatments targeting this central mechanism (CBT, mindfulness, desensitization) can reduce allodynia even when the peripheral nerve damage itself has not changed. The brain can be recalibrated.
Desensitization Therapy
This is a graded, systematic approach to re-exposing the skin to stimuli it's learned to fear. Working with an occupational therapist or physical therapist, you begin with textures that are well-tolerated (perhaps smooth silk or soft cotton) and very gradually introduce progressively rougher or more intense textures over weeks to months. The goal is to slowly recalibrate the nervous system's response — to teach the pain pathways that certain inputs are safe.
Desensitization takes patience and consistency. It often makes symptoms temporarily worse before they improve. But many people with chronic allodynia — particularly post-injury allodynia — find it genuinely transformative over time.
Cognitive Behavioral Therapy (CBT)
This isn't about convincing yourself the pain isn't real. CBT for pain works by modifying the psychological and behavioral responses to pain that amplify suffering and disability. Fear of pain leads to avoidance; avoidance leads to more sensitization; more sensitization leads to more pain. CBT breaks that cycle. There's solid evidence that it reduces pain intensity, improves function, and reduces the disability caused by chronic pain conditions including allodynia.
Mindfulness and Pain Neuroscience Education
Mindfulness practices can genuinely change how the brain processes pain signals — not just as coping tools, but through measurable neurological mechanisms. Mindfulness activates descending inhibitory pathways. Pain neuroscience education helps patients understand the central sensitization mechanisms behind their pain, which consistently reduces fear, catastrophizing, and disability even when the pain itself doesn't disappear entirely.
Graded Motor Imagery
Originally developed for complex regional pain syndrome, graded motor imagery involves progressively working through mental and visual exercises before attempting physical movement. By first imagining movement, then watching movement in a mirror, then attempting movement, the technique helps normalize the brain's motor and sensory representations. It can reduce allodynia in cases with strong central sensitization components.
Practical Strategies for Living with Allodynia
While you're working through treatment options, these practical strategies can make daily life more manageable:

Fabric & Bedding Guide for Allodynia
- Clothing: Seamless socks, tagless underwear and shirts, soft modal or bamboo fabrics, loose-fitting garments. Avoid elastic cuffs directly against affected skin.
- Bedding: Lightweight materials, foot cradles to lift covers off feet and lower legs, bamboo or tencel sheets (very soft against sensitive skin).
- Bathing: Lukewarm water (not hot or cold), gentle application of water rather than direct shower spray on affected areas, pat dry rather than rubbing.
- At the doctor: Tell your provider about allodynia before examination so they can modify their approach. Many patients find it helpful to say “please warn me before you touch me” and specify which areas are most sensitive.
- With family: Explain what allodynia is, that your pain response isn't voluntary or exaggerated, and brainstorm ways to be physically close that bypass the most sensitive areas.
- Temperature management: Avoid extreme temperature changes; dress in layers; test water temperature with a non-allodynic body part before immersing affected areas.
Frequently Asked Questions
Is allodynia permanent?
Not necessarily. In some cases, particularly when the underlying cause of nerve damage is treated effectively, allodynia can improve significantly or even resolve. In others — especially long-standing central sensitization — it becomes a chronic condition that requires ongoing management rather than expecting complete resolution. Early treatment generally produces better outcomes than waiting.
Why does allodynia seem worse at night?
Several factors contribute to nighttime worsening. Distractions that occupy your attention during the day are gone, so pain perception intensifies. The warmth of bed and increased blood flow to the skin can activate nerve endings. Inflammatory markers tend to peak at night. And the weight of bedding creates ongoing contact with sensitive skin. Many people find that managing the bedroom environment — cooler temperatures, lighter bedding, foot cradles — makes a meaningful difference.
Can exercise make allodynia worse?
It depends on the exercise and the individual. High-impact exercise that jars sensitive areas may transiently worsen symptoms. However, gentle, consistent exercise generally helps — it improves circulation, reduces inflammation, releases endorphins, and helps modulate central sensitization. Starting gently and building gradually is the key. Many people with allodynia find that water-based exercise is particularly comfortable because the water provides even, gentle pressure that can be somewhat desensitizing.
Is allodynia a sign that my neuropathy is getting worse?
Not necessarily, but it's worth discussing with your neurologist if allodynia suddenly develops or worsens significantly. Allodynia can develop or intensify even when underlying nerve damage is stable, because it partially reflects central sensitization changes rather than pure peripheral damage. A change in your pain pattern — new allodynia, significantly worsening allodynia — is worth noting and reporting.
What is the best fabric for allodynia?
Soft, smooth, natural fibers generally cause less irritation. Bamboo fabric, Tencel/lyocell, modal, and high-thread-count cotton tend to be the most tolerated. Silk works for some people. Avoid rough textures, synthetic blends that trap heat, and fabrics with prominent woven patterns that create tactile irregularity against the skin. Individual preference varies — what feels tolerable for one person may not for another, so trial and error is part of finding your fabric comfort zone.
Is allodynia the same thing as hyperesthesia?
Related but not identical. Hyperesthesia is an increased sensitivity to sensory stimulation generally — touch, temperature, and other inputs feel more intense than normal, even if not necessarily painful. Allodynia is specifically pain from non-painful stimuli. There's overlap, and the two often coexist in neuropathy patients, but allodynia specifically refers to the crossing of the non-painful into the painful.
Can allodynia affect areas other than the feet?
Absolutely. While neuropathic allodynia most commonly affects the feet and lower legs (reflecting the length-dependent nature of peripheral neuropathy), it can affect the hands, forearms, trunk, or anywhere that nerve damage is present. In conditions like fibromyalgia or widespread small fiber neuropathy, allodynia may be more generalized. In post-herpetic neuralgia, it typically corresponds to the skin area affected by the original shingles outbreak, which may be the trunk, face, or other body regions.


