There's a moment many of us with neuropathy have experienced — reaching out in a dark room to flip the light switch, and suddenly feeling completely unmoored. Or stepping off a curb and almost going down because the foot didn't land quite the way the brain expected. Or standing in the shower with eyes closed and feeling a terrifying wobble that sends the hand scrambling for the wall.
This isn't clumsiness. It isn't inattention. It's a specific, explainable consequence of peripheral neuropathy called proprioception loss — and once you understand what's actually happening in your nervous system, it changes how you think about balance, safety, and recovery.
I've spent years talking with people who describe this feeling and don't have a name for it. They say things like, “I can't trust my feet anymore,” or “I feel like I'm walking on pillows,” or “I don't know where my legs are when I wake up at night.” What they're describing is proprioception — the body's internal positioning system — going dark.
Let's talk about what proprioception actually is, how neuropathy disrupts it, what the risks look like, and what you can actually do about it.
What Is Proprioception? Your Body's Hidden Sixth Sense
You've heard of five senses. But there's a sixth one that most people don't think about until it starts to fail: proprioception. It's your body's ability to sense its own position, movement, and force — constantly, automatically, without you having to look.
Key Takeaway
Proprioception is your body's internal GPS — the sense that tells your brain where every limb is without looking. It runs through large-diameter nerve fibers. When neuropathy damages those fibers, balance suffers even when you don't notice significant pain or numbness.
Right now, without looking at your hands, you know where they are. You could touch your nose with your eyes closed. You know whether you're sitting up straight or slouching. You can feel that your left foot is crossed over your right. None of this requires visual input. That's proprioception.
This sense comes from a dense network of specialized receptors embedded in your muscles, tendons, and joint capsules. These mechanoreceptors — with names like muscle spindles, Golgi tendon organs, and Ruffini endings — constantly fire signals up through the peripheral nerves to the spinal cord and brain, providing a real-time map of where every part of your body is in space.
The brain uses this information to coordinate movement, maintain balance, and make the thousands of micro-adjustments that keep you upright without conscious effort. Walking down a sidewalk, your brain is simultaneously processing ground texture from your feet, joint angles from your ankles and knees, and gravitational pull on your inner ear — all in milliseconds — to keep you balanced.
When this system works, it's invisible. When it starts to fail, you notice it in exactly the ways I described above: the wobble, the uncertainty, the feeling of walking on ground you can't quite trust.
How Neuropathy Damages Proprioception
Not all nerves do the same job, and not all neuropathy attacks the same nerve fibers. This is an important distinction that many people — and sometimes even their doctors — don't fully explain.
🔎 Research Says
People with peripheral neuropathy walk with shorter stride lengths, greater variability, and more caution than age-matched controls — measurable biomechanical signatures of unreliable proprioceptive feedback. Fall risk is 2-3x higher in neuropathy patients than in people without nerve damage.
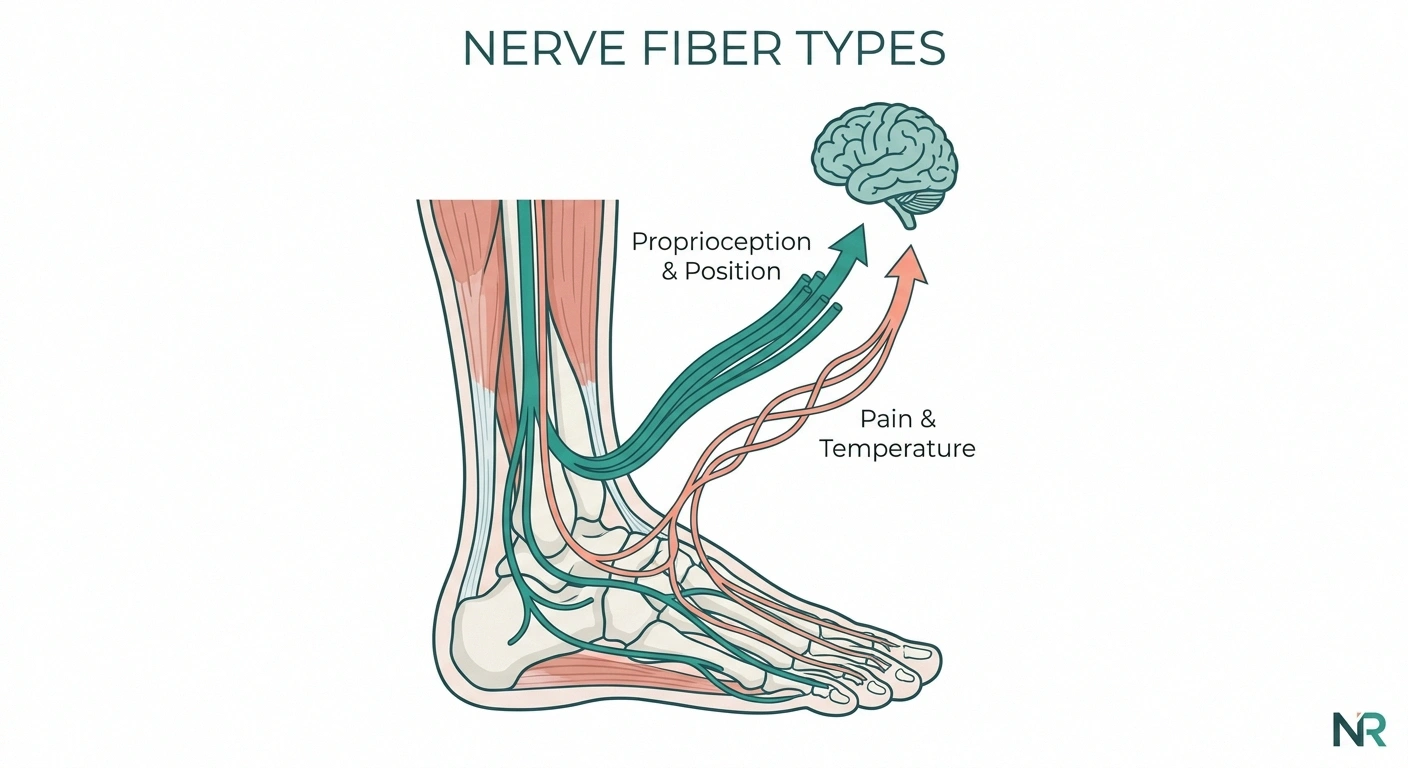
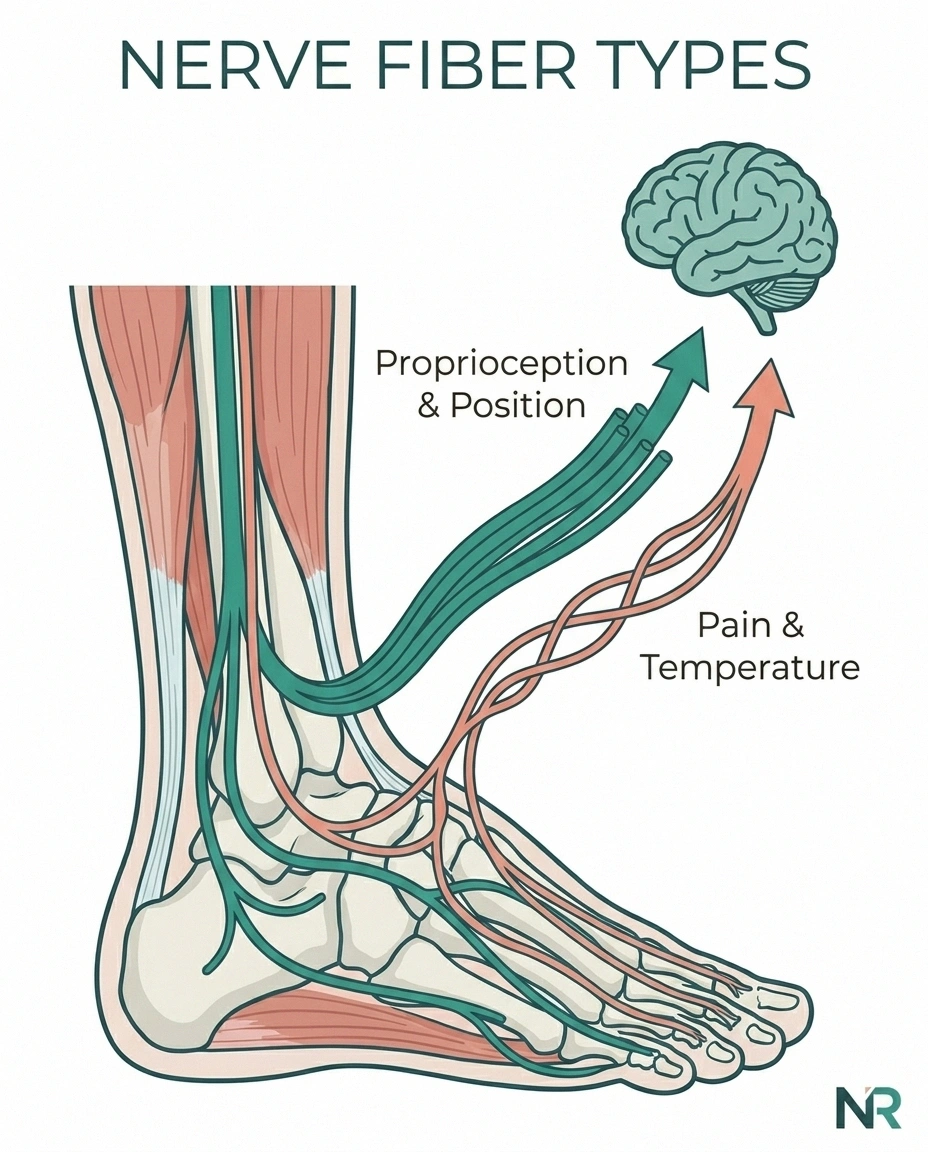
Peripheral nerves come in different sizes. Large-diameter fibers (called A-beta fibers) are thick, heavily insulated with myelin, and carry proprioceptive signals — the position and movement information from your mechanoreceptors. Small-diameter fibers (A-delta and C fibers) carry pain, temperature, and light touch.
When peripheral neuropathy damages the large fibers, proprioception suffers. This is why small fiber neuropathy — which spares the large fibers — tends to produce burning pain and temperature disturbance but doesn't typically destroy balance. Large-fiber or mixed-fiber neuropathy, on the other hand, directly attacks the proprioceptive pathway.
The damage follows a characteristic pattern: length-dependent. The longest nerves in the body — the ones running from your spinal cord to your feet — are affected first and most severely. This is why, almost universally, neuropathy starts in the feet and works upward. By the time the calves and knees are affected, the feet may have very little proprioceptive input remaining.
The brain doesn't receive silence from damaged nerves — it receives noise. Distorted, incomplete, or misfiring signals. The result is that your brain is working with bad data, trying to construct a body map that keeps changing and doesn't match reality. That's the root of the instability you feel.
Research published in the Journal of Orthopaedic & Sports Physical Therapy confirmed that foot and ankle sensory neuropathy directly impairs postural control, and that the degree of proprioceptive loss correlates with fall risk. Patients with peripheral neuropathy walk more cautiously, with shorter stride lengths and more variability — the body's instinctive compensation for unreliable ground feedback.
What Proprioception Loss Actually Feels Like

One of the most valuable things we can do is give language to experiences that are often hard to describe to doctors. Here's how proprioception loss tends to show up in daily life:
The Romberg Wobble
Stand with your feet together and close your eyes. Most people can hold this for 30 seconds without much difficulty. People with significant proprioceptive loss immediately feel themselves tipping and have to open their eyes or grab something. This is called a positive Romberg sign, and neurologists often test for it during exams. Your visual system is compensating for what your feet can't tell you — remove vision, and the instability becomes clear.
Nighttime Instability
Many people with neuropathy report that walking to the bathroom at 2 AM is genuinely frightening. In the dark, with reduced visual cues, the already-impaired proprioceptive system is working completely alone. Falls happen. This nighttime vulnerability isn't imagined — it's the physics of the problem.
Stair Uncertainty
Going down stairs requires your feet to land precisely and your ankles to make constant adjustments. With compromised proprioception, the foot doesn't “tell” the brain it has landed on a step, and the knee may buckle. This is why many people with neuropathy hold railings tightly and go one step at a time going down — even if they seem fine on flat ground.
Uneven Surface Difficulty
Grass, gravel, beach sand, cobblestones — any surface that requires constant ankle adjustment becomes disproportionately difficult. The brain can't get accurate feedback about what the foot is encountering, so the whole system becomes overwhelmed.
Not Knowing Your Foot Position
Some people with severe proprioceptive loss report that when they're lying in bed with eyes closed, they genuinely cannot tell whether their feet are dorsiflexed (toes up) or plantarflexed (toes pointed down). This is deeply disorienting and is a sign of significant large-fiber involvement.
If any of these sound familiar, you're not alone. And you're not “just getting old.” These are physiological signs of specific nerve damage, and they can be worked with.
The Fall Risk Reality — and Why It Matters So Much

Falls are not a minor concern. For older adults with neuropathy, a single fall can mean a hip fracture, hospitalization, loss of independence, and a cascade of health decline. Research consistently shows that people with peripheral neuropathy have two to three times the fall risk of age-matched controls without neuropathy.
Important Safety Note
Nighttime bathroom trips are the highest-risk moment for falls with proprioceptive loss. The combination of darkness (removing visual compensation) and grogginess (reducing alertness) is particularly dangerous. Install night lights in hallways and bathrooms as a medical priority, not a convenience.
Proprioceptive loss is a central — often underappreciated — contributor to this risk. Most people focus on the numbness (can't feel the ground) or the pain (distraction from movement), but the proprioceptive component adds another layer: the brain is not only receiving no sensation from the feet, it's also not receiving accurate body position data.
This is why the fall prevention strategies most relevant to neuropathy are specifically targeted at proprioceptive compensation — using vision, using walls and furniture, using wide stances and slower movement to give the brain more time to process the imperfect signals it's receiving.
Your neurologist or physical therapist may order a formal balance assessment, sometimes called a “balance test” or posturography. This objectively measures how much your balance depends on proprioception versus vision versus inner ear input. Understanding your specific profile helps target treatment more precisely.
What You Can Do: Evidence-Based Strategies
Here's where I want to be honest with you: proprioceptive loss from peripheral nerve damage doesn't fully reverse. But — and this matters enormously — you can train your brain and body to compensate in ways that dramatically reduce fall risk and restore functional confidence.
Physical Therapy: The Foundation

Working with a physical therapist who understands peripheral neuropathy is the single most evidence-supported intervention for proprioceptive loss. A good PT will assess your specific pattern of deficit and design a program around compensation strategies. Key elements include:
Physical Therapy Approach for Proprioceptive Loss
Balance Assessment — PT evaluates your specific deficit pattern (how much visual vs proprioceptive vs vestibular)
Progressive Balance Training — One-foot stands, heel-toe walking, foam surfaces; challenge stability safely
Sensory Re-education — Walking on textured surfaces, ankle drills to amplify residual nerve signals
Strengthening — Ankle, calf, and hip stabilizers to compensate mechanically for impaired joint position sense
Balance Training
Exercises that progressively challenge your balance in controlled settings. Standing on one foot (with a sturdy chair nearby), heel-to-toe walking, standing on foam surfaces — these challenge the vestibular and visual systems to compensate more fully for reduced proprioceptive input. The goal isn't to restore what's lost but to strengthen the systems that can pick up the slack.
Proprioceptive Cueing Exercises
Sensory re-education techniques that help the brain “pay more attention” to the weak signals that remain. Walking on different textured surfaces. Ankle circles and weight-shifting. These exercises, done consistently, have been shown to improve functional balance even when nerve function itself hasn't changed significantly.
Lower Extremity Strengthening
Strong muscles around the ankle and knee can partly compensate for impaired joint position sense. When proprioception can't tell the ankle where it is, a strong peroneal muscle can catch it. Calf raises, ankle strengthening, and hip stabilizer work all contribute.
The neuropathy exercise programs designed for seniors specifically address this through low-impact, targeted routines that can be done safely even with significant balance impairment.
Visual Compensation: Using Your Eyes Deliberately
Your visual system is your most powerful backup proprioceptor. When the feet can't report accurately, the eyes can help — but you have to be deliberate about it:
- Watch where you're stepping on unfamiliar terrain
- Look at your feet when stepping off curbs or down stairs
- Keep walking areas well-lit (especially at night)
- Avoid walking in situations where your visual field is restricted
The trap is relying on this entirely without working on other compensatory strategies. Vision alone — especially in dim light, fog, or situations where you're distracted — isn't enough to fully replace proprioception.
Home Safety Modifications

If your proprioception is compromised, your environment needs to work with you, not against you. The room-by-room guide to neuropathy home safety covers the specifics, but core modifications include:
2-3×
Higher fall risk for people with peripheral neuropathy compared to age-matched controls without nerve damage
- Grab bars in the bathroom (toilet, shower) — non-negotiable
- Night lights in hallways and bathrooms for those 2 AM walks
- Removal of throw rugs (they shift underfoot and worsen instability)
- Furniture arranged to provide touchpoints across rooms
- Textured, non-slip surfaces in key areas
- Stair railings on both sides if possible
Footwear and Orthotics
Footwear has a meaningful impact on proprioception for neuropathy. Thick-soled shoes actually reduce the already-limited feedback from the ground. For many people, a firmer sole (not cushioned to the point of sensory deprivation) with good ankle stability is preferable.
Vibrating insoles — devices that deliver a subtle vibration to the sole of the foot — have been studied as a form of stochastic resonance therapy. The theory: a small amount of background noise can paradoxically help the nervous system detect weak signals. Some clinical studies have shown improvement in balance with vibrating insoles. They're not widely prescribed yet but represent a promising area.
Ankle-foot orthoses (AFOs) may be appropriate when foot drop or significant ankle instability is present. These brace the foot in a neutral position and reduce the unpredictability of stepping.
Emerging Technologies
Virtual reality balance training is showing promise in research settings. By immersing patients in environments that progressively challenge balance while providing real-time visual feedback, VR allows for more intensive training with lower fall risk. Wearable sensors that vibrate when the body begins to tip are also being studied as real-time proprioceptive aids.
These aren't mainstream yet, but they represent the direction the field is heading. Worth asking your physical therapist about whether any of these are available in your area.
Managing the Emotional Reality

I want to acknowledge something that doesn't get discussed enough: the psychological weight of not trusting your own body.
On the Emotional Side
Not trusting your own body is exhausting. Many people in the neuropathy community describe physical therapy for proprioceptive loss not just as exercise, but as the experience of getting their confidence back. The physical and the psychological heal together.
When proprioception is compromised, there's a constant low-level vigilance required for ordinary movement. You can't zone out while walking. You can't talk and descend stairs simultaneously without risk. You can't close your eyes in the shower without bracing the wall. This vigilance is exhausting — physically and emotionally.
Many people pull back from activities they love because the unpredictability feels unmanageable. They stop going to events that involve standing or uneven ground. They avoid situations where a fall would be humiliating. The mental health impacts of neuropathy are real, and the loss of confidence in one's own body is a specific grief that deserves acknowledgment.
If this resonates, know that working with a physical therapist on balance — not just for the physical benefit but for the psychological experience of rebuilding trust in your body — can be genuinely life-changing. Many of my friends in the support community describe PT not as exercise, but as getting their confidence back.
The neuropathy and anxiety cycle is real: fear of falling makes people more tense and awkward in their movement, which actually increases fall risk. Breaking that cycle with gradual, supported balance challenges can shift the whole picture.
Talking to Your Doctor About Proprioception Loss
Many people experience significant proprioceptive loss before it's formally identified and addressed. Here's how to bring it into a clinical conversation:
Tell your neurologist or doctor specifically: “I'm having trouble knowing where my feet are when I can't see them. I wobble in the dark. I'm afraid of falling.” These specific descriptions — not just “numbness” or “balance problems” — point directly to large-fiber proprioceptive involvement.
Ask for a referral to a neurologist if you haven't seen one. The diagnostic workup for neuropathy should include an EMG/nerve conduction study that can characterize which fiber types are affected. Understanding whether you have predominantly large-fiber, small-fiber, or mixed-fiber involvement changes the conversation about what to expect and how to compensate.
Also ask for a physical therapy referral specifically for balance and fall prevention. Many doctors don't offer this proactively — you may need to ask for it directly.
Frequently Asked Questions
What is proprioception loss in neuropathy?
Proprioception loss in neuropathy occurs when peripheral nerve damage affects the large-diameter sensory fibers that carry body position information from muscles, joints, and tendons to the brain. When these fibers are damaged, the brain receives incomplete or distorted signals about where the body is in space, leading to balance problems, instability, and increased fall risk. It's distinct from pain or temperature loss, which involves smaller nerve fibers.
Can proprioception come back with neuropathy?
Full recovery of proprioception from nerve damage is not common, but the brain has significant capacity to compensate through a process called neuroplasticity. Physical therapy, balance training, and sensory re-education can train other systems — especially vision and the vestibular system — to pick up some of the proprioceptive slack. Many people achieve substantially improved functional balance even without full nerve recovery.
How do I know if I have proprioceptive loss from neuropathy?
Signs include wobbling when eyes are closed (positive Romberg sign), difficulty on stairs or uneven surfaces, nighttime instability, inability to identify your foot position without looking, and feeling unmoored when walking in reduced lighting. A neurologist can formally assess this with a physical exam and nerve conduction studies. A physical therapist can conduct a formal balance assessment.
What exercises help proprioception with neuropathy?
Balance training exercises are most effective: standing on one foot with support nearby, heel-to-toe walking, standing on foam surfaces, ankle circles and weight-shifting drills. These challenge the compensatory systems (vision and vestibular) to work harder in the absence of full proprioceptive input. A physical therapist should guide the program to ensure safety and appropriate progression.
Is proprioception loss dangerous with neuropathy?
Yes, proprioceptive loss significantly increases fall risk — research shows two to three times the fall rate compared to people without neuropathy. Falls in older adults can result in hip fractures, hospitalization, and loss of independence. This is why fall prevention — through PT, home modifications, appropriate footwear, and environmental adjustments — is a medical priority, not just a nice-to-have.
Why is neuropathy worse at night for balance?
During daylight hours, your visual system provides significant compensation for impaired proprioception — the brain uses what it sees to supplement the unreliable signals from the feet. In darkness, that compensation is removed, and proprioceptive loss becomes much more apparent. Nighttime bathroom trips are a high-risk time for falls. Night lights throughout the home, keeping a path clear, and moving slowly until fully awake can reduce this risk.
Does physical therapy help proprioception loss from neuropathy?
Yes, physical therapy is the most evidence-supported intervention for proprioceptive loss in neuropathy. While PT typically cannot restore the damaged nerve fibers themselves, it trains the brain and body to compensate through balance exercises, strengthening, and sensory re-education. Multiple studies have shown reduced fall risk and improved functional balance with consistent PT, even in patients with significant nerve damage.