If you're taking tirzepatide — sold as Mounjaro for type 2 diabetes or Zepbound for weight management — and you've noticed a change in your nerve symptoms, you're not alone. The internet is full of stories. Some patients say their long-standing diabetic neuropathy is getting better since they started the drug. Others say they developed new tingling, burning, or numbness after starting it. Both groups are searching for answers, and the conversation deserves more honesty than most of the existing online content offers.
I want to give you the two-sided truth — based on what the clinical trial data shows, what's reported in case-series literature, and what real patients describe in support communities. Tirzepatide can plausibly help diabetic neuropathy by dramatically improving the very metabolic conditions that cause it. But it has also been associated, in rare cases, with new or worsening neuropathy symptoms — primarily at higher doses.
By the end of this, you'll have a clearer framework for thinking about your own situation and a better set of questions to bring to your prescribing doctor.
What Tirzepatide Is — the Quick Background
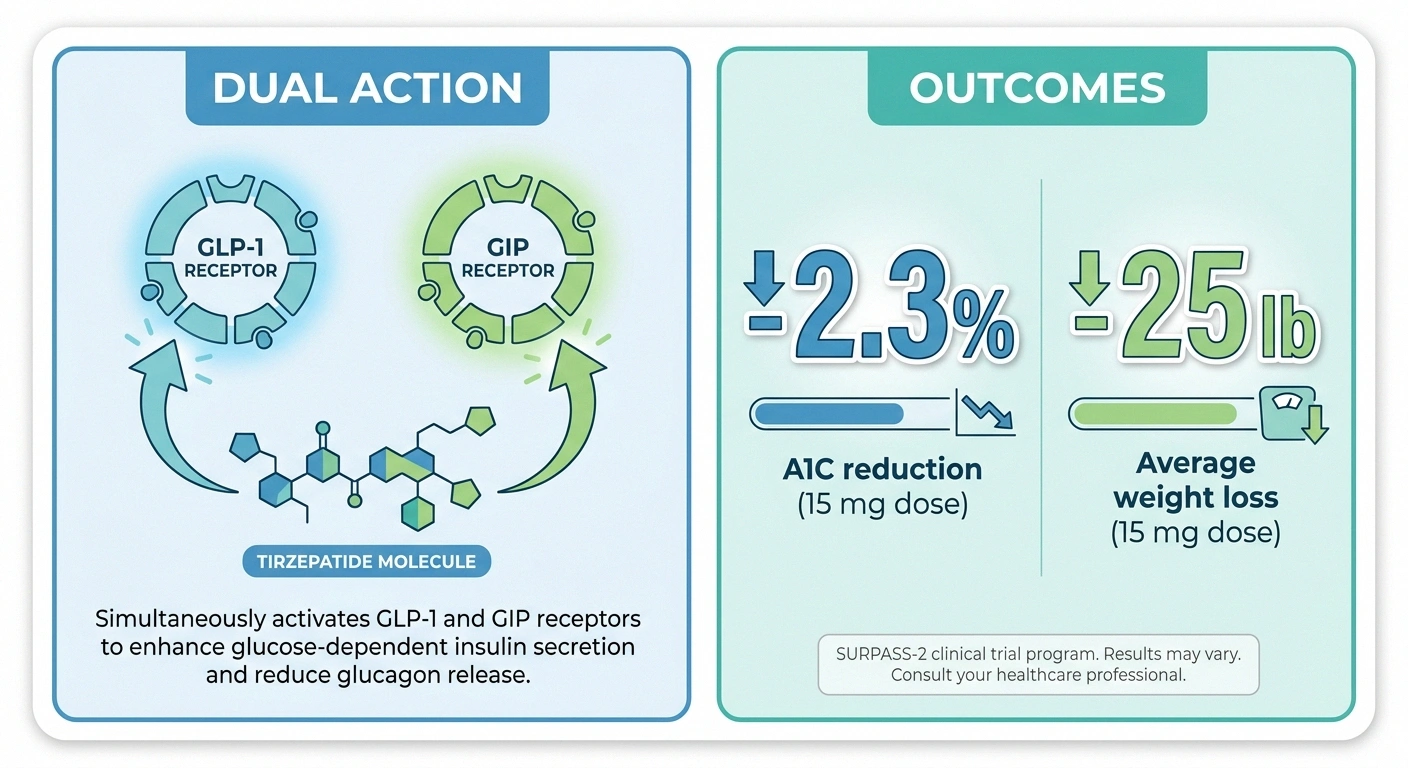
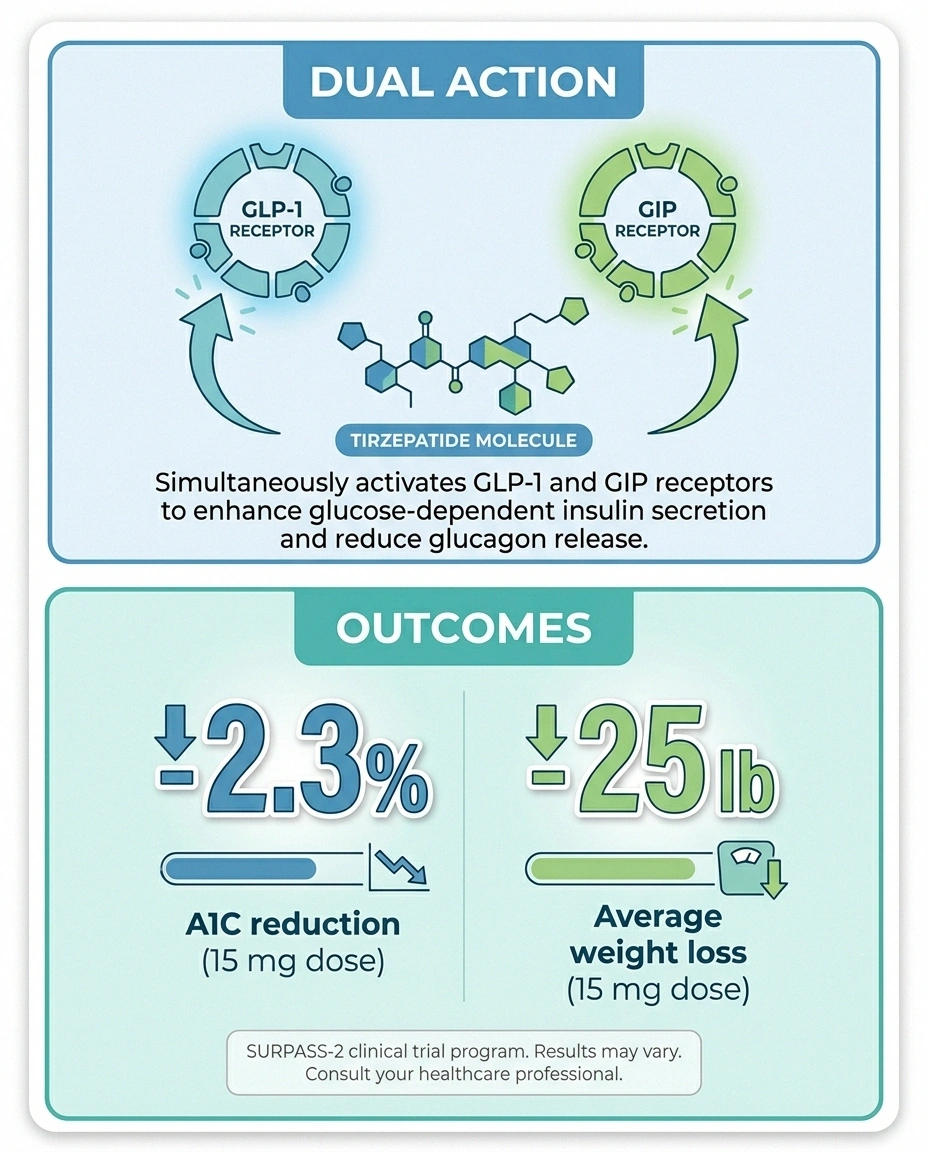
Tirzepatide is the first member of a new drug class called dual GIP/GLP-1 receptor agonists — also informally called “twincretins.” Most people are familiar with single GLP-1 drugs like semaglutide (Ozempic, Wegovy). Tirzepatide hits both incretin receptors at once — the GLP-1 receptor and the GIP receptor — which produces stronger effects on blood sugar and weight than GLP-1 alone.
It's made by Eli Lilly. It comes as a weekly subcutaneous injection. Doses start at 2.5 mg and titrate up over months to a maximum of 15 mg. Branded names:
- Mounjaro — FDA-approved for type 2 diabetes (May 2022)
- Zepbound — FDA-approved for chronic weight management in adults with obesity or overweight with comorbidities (November 2023)
The numbers from the SURPASS trial program are striking. In SURPASS-2, patients on the highest dose (15 mg) lowered their A1C by an average of 2.30 percentage points — putting up to 92% of participants below the ADA's 7% target, and up to 52% all the way to non-diabetic A1C levels under 5.7%. Weight loss averaged 19 to 28 pounds at the highest dose across the SURPASS arms. These are bigger effects than any prior diabetes drug class has produced.
Why Tirzepatide Might Help Diabetic Neuropathy

Let's start with the upside argument, because it's the more biologically plausible one.
The single most important determinant of diabetic neuropathy progression is glycemic control. The landmark Diabetes Control and Complications Trial (DCCT) — and decades of follow-up data since — established that intensive blood-sugar control delays the onset and slows the progression of diabetic neuropathy. The effect is stronger in type 1 diabetes (about 60–70% reduction in neuropathy progression with tight control) but real in type 2 as well, typically in the 35–50% range. Tight blood-sugar control is the foundation underneath every other neuropathy treatment.
Now think about what tirzepatide does:
- Drops A1C by an average of 2 percentage points — a magnitude of reduction you simply don't see with most other diabetes drugs.
- Causes 10–14% body weight loss at higher doses — and obesity is an independent risk factor for neuropathy, separate from blood sugar.
- Improves insulin sensitivity and reduces inflammation broadly throughout the body.
If a patient has poorly controlled diabetes plus excess weight plus diabetic neuropathy, tirzepatide can remove or substantially reduce all three of the metabolic drivers at once. From a biology-of-nerve-damage perspective, that's a real shot at slowing — or in some cases partially reversing — the underlying problem. Many patient anecdotes describing improved sensation, reduced tingling, or fewer burning episodes after months on tirzepatide line up exactly with what you'd predict from getting metabolic control under control.
To be clear: tirzepatide is not FDA-approved as a neuropathy treatment. No pivotal trial has been run with neuropathy progression as a primary endpoint. The biology and the broad clinical-trial improvements in glycemic control make benefit plausible, but plausible isn't the same as proven for this specific outcome.
For the broader picture of how blood sugar damages nerves, our piece on sugar, blood sugar, and neuropathy covers the mechanism more fully. And our piece on whether neuropathy can be reversed sets realistic expectations for any approach that targets the underlying cause.
The Other Side — When Tirzepatide May Cause Neuropathy
This is where the honest framing matters most, because almost no marketing-page treatment of tirzepatide acknowledges it.
Peripheral neuropathy is listed as a rare adverse event in tirzepatide post-marketing reports — at frequencies below 1% based on FDA Adverse Event Reporting System data and case-series literature. That's rare in statistical terms but not zero. And in the world of patient experience, “rare but possible” is very different from “not a concern.”
What's been reported:
- New peripheral neuropathy after starting tirzepatide, often appearing during titration to 10 mg or 15 mg.
- Worsening of pre-existing neuropathy symptoms after dose increases.
- Symptoms most commonly described as tingling in fingers and toes, burning sensations, allodynia (pain to normal touch), and in some cases small-fiber-type symptoms.
- Partial improvement on discontinuation. Most case reports describe patients who stopped the drug and saw meaningful symptom improvement — but not always complete resolution. Some cases involve persistent residual symptoms even after stopping.
Two important caveats:
First, this signal appears to be specific to tirzepatide, not the entire GLP-1 class. Semaglutide (Ozempic, Wegovy) has not produced the same reports. Why tirzepatide specifically would have this signal — and not its GLP-1-only cousin — isn't yet understood. Hypotheses involve the GIP receptor agonism, rapid metabolic shifts, or pharmacologic effects at higher doses, but none are confirmed.
Second, the mechanism by which any of this happens is unclear. Some researchers wonder whether rapid normalization of blood sugar in long-term diabetics can paradoxically produce treatment-induced neuropathy of diabetes (TIND) — a known phenomenon where extremely rapid A1C drops trigger transient nerve symptoms. Others wonder whether rapid weight loss itself plays a role (a phenomenon documented after bariatric surgery — see our piece on neuropathy after rapid weight loss). Others suspect a direct neurotoxic or autoimmune mechanism specific to tirzepatide. The honest answer right now: we don't know.
Which Story Applies to You? A Decision Framework
If you're already on tirzepatide and have noticed nerve symptoms, the question is which side of the coin you're on. Here are clues that point in each direction.
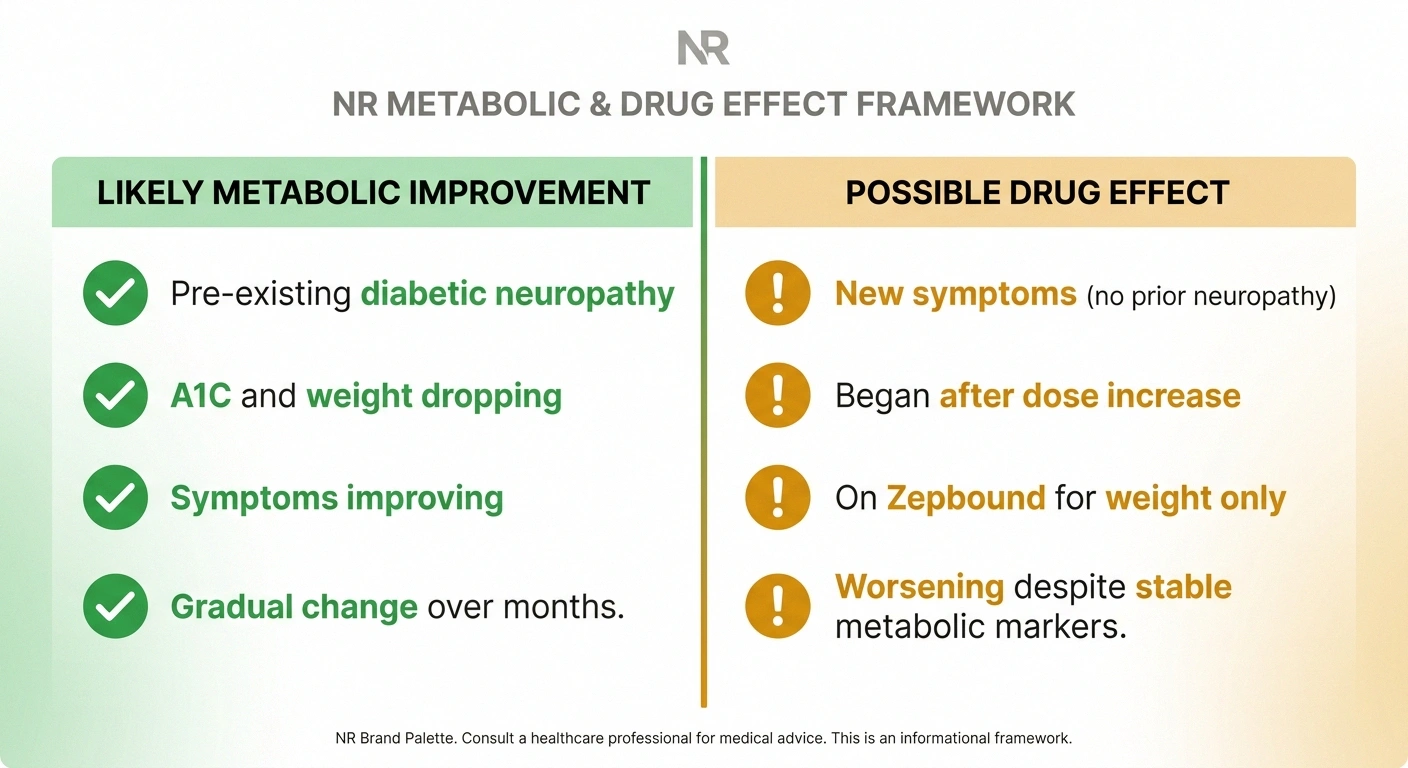
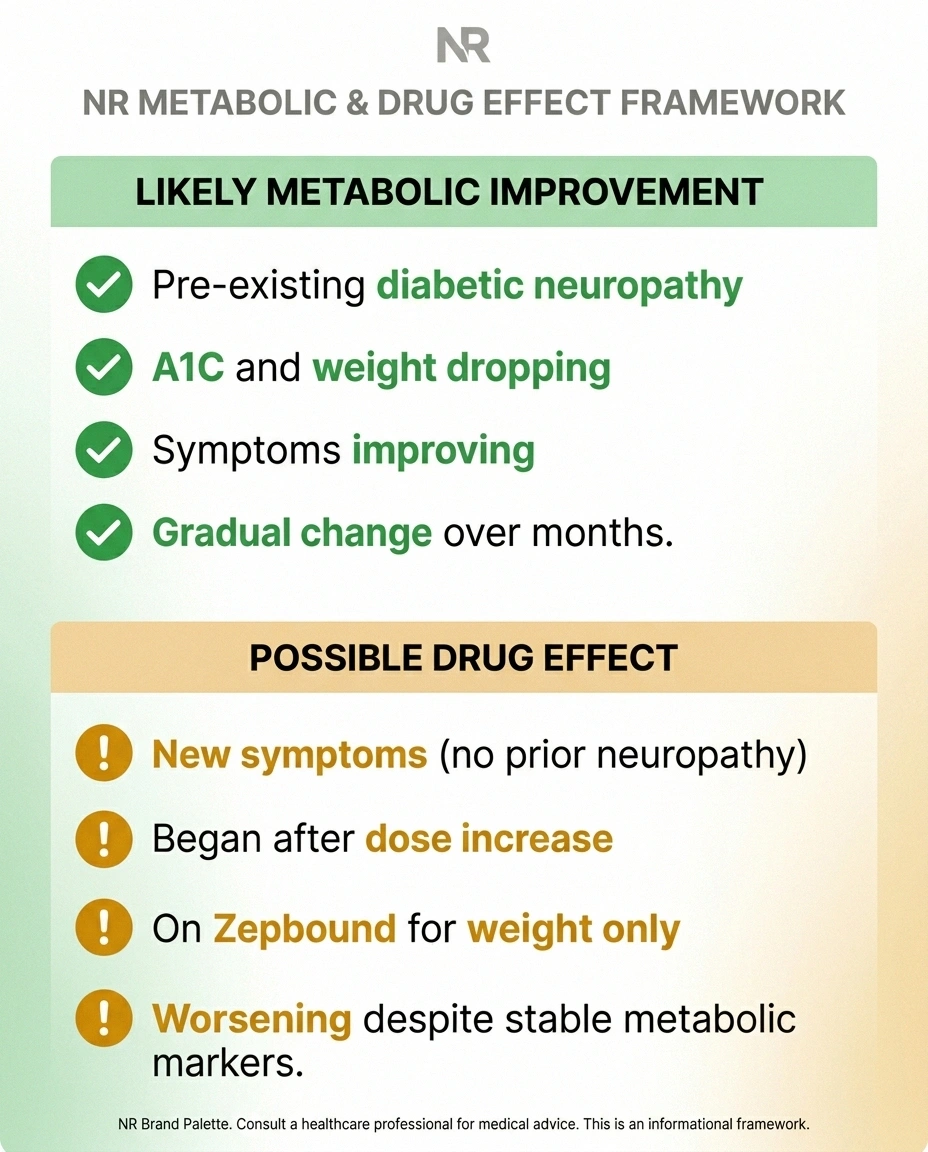
- Pre-existing diabetic neuropathy before starting
- A1C and weight dropping substantially
- Symptoms improving — less burning, returning sensation
- Gradual change over weeks to months
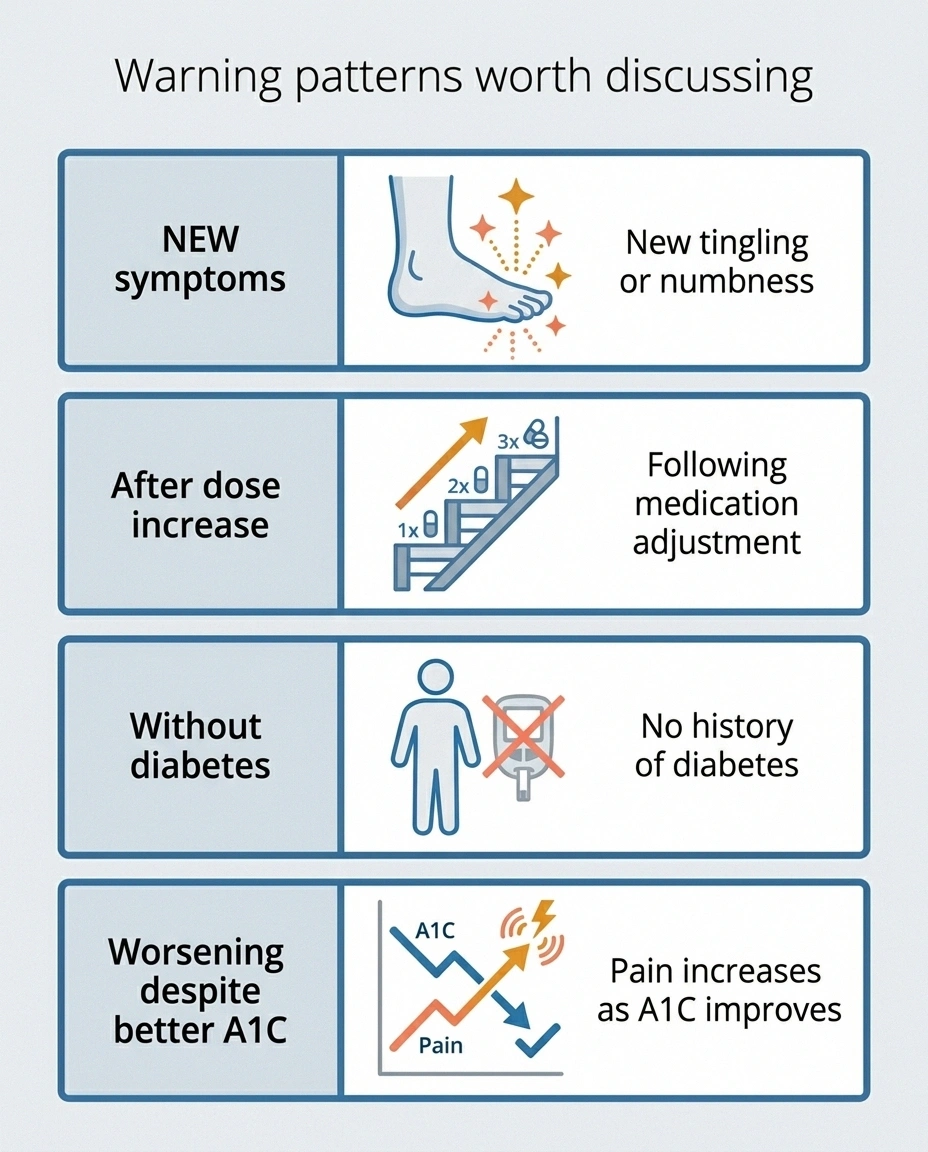
- NEW symptoms — no prior neuropathy
- Began or worsened after dose increase (10 mg or 15 mg)
- On Zepbound for weight only (no diabetes)
- Worsening despite improving metabolic markers
Pattern suggesting metabolic improvement (likely good news):
- You had pre-existing diabetic neuropathy before starting tirzepatide.
- Your A1C and weight have dropped substantially since starting.
- You're noticing improvement in symptoms — less burning, returning sensation, fewer night-time flares — not worsening.
- The change has been gradual, over weeks to months, paralleling your metabolic improvement.
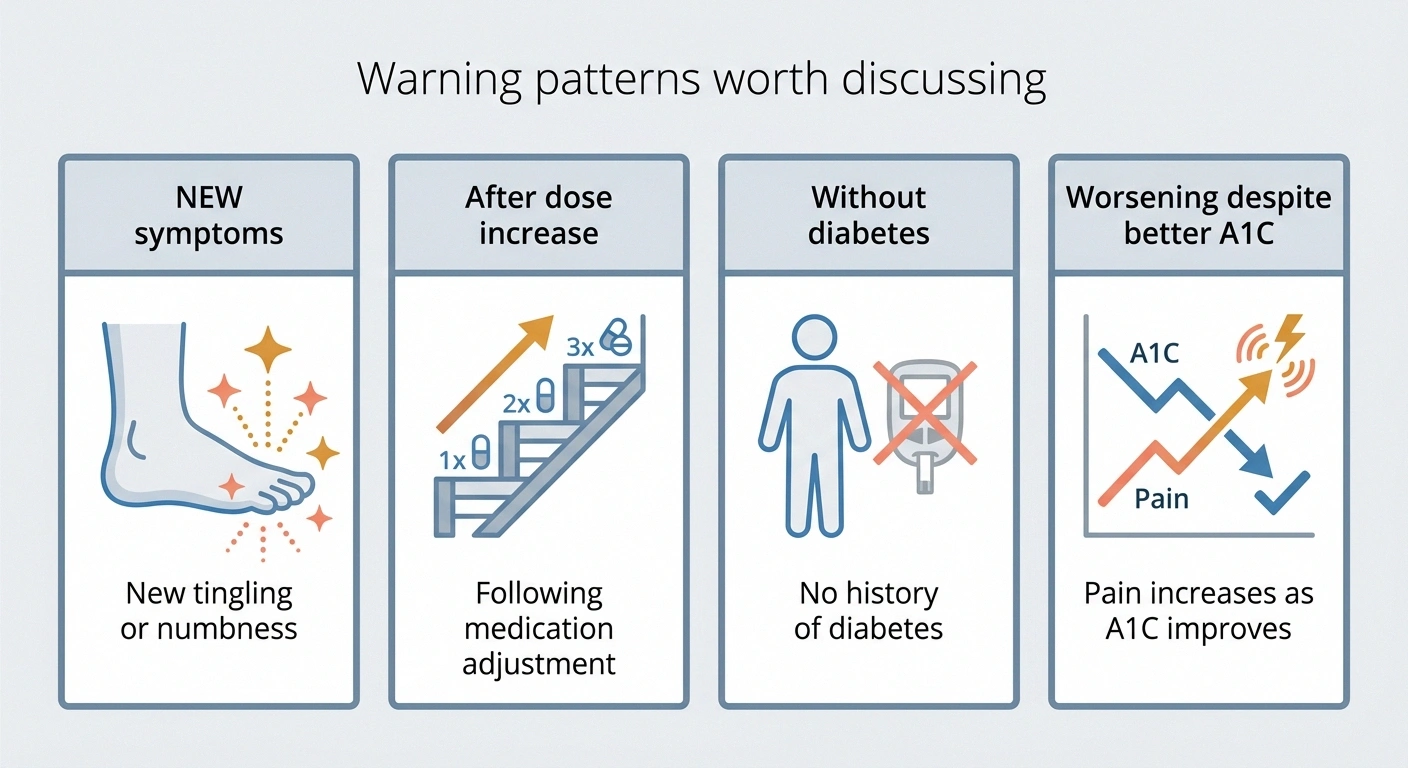
Pattern suggesting adverse drug effect (a concern to discuss):
- Symptoms are new — you didn't have neuropathy before starting tirzepatide.
- Symptoms began or worsened sharply after a dose increase, particularly to 10 mg or 15 mg.
- You don't have diabetes (you're on Zepbound for weight loss only) — so a diabetic-neuropathy explanation doesn't fit your situation.
- Symptoms are worsening despite stable or improving metabolic markers.
- Symptoms include features suggestive of acute drug effect — sudden onset, allodynia, or rapid progression.
A mixed picture is possible too — someone with pre-existing diabetic neuropathy whose symptoms briefly worsened during a rapid A1C drop (treatment-induced neuropathy of diabetes), then plateaued or improved as metabolic control stabilized. That's actually a well-documented pattern in the medical literature, separate from any drug-specific concern.
What to Do — Step by Step
Whether you're worried about neuropathy as a side effect or hoping tirzepatide will help an existing case, here's a sensible action sequence.
1. Don't stop tirzepatide on your own. Abrupt discontinuation can cause blood sugar to rebound rapidly, which has its own risks. If you're considering stopping, do it with your prescriber's input.
2. Document the timeline carefully. When did symptoms start? Did they begin or worsen after a dose change? How have they evolved? A simple symptom journal tracking severity, location, and timing — alongside your tirzepatide dose history — gives your doctor far better information to work with than memory.
3. Get a baseline neurological assessment. If symptoms are concerning, ask for a referral to neurology. A clinical exam plus standard tests can help distinguish between drug-related, diabetes-related, and other causes. For the framework of what tests get ordered, see neuropathy diagnosis: tests your doctor may order.
4. Discuss alternatives if a drug-related cause is likely. If your endocrinologist or PCP concludes the symptoms are likely drug-related, the conversation usually focuses on:
- Dose reduction — sometimes returning to a lower dose resolves symptoms while preserving meaningful benefit.
- Slower titration — staying at each dose longer before increasing.
- Switching to a single GLP-1 like semaglutide, which has not produced the same neuropathy signal.
- Discontinuation — with a clear plan for what comes next for blood sugar and weight management.
None of those choices is one-size-fits-all. The right answer depends on how severe symptoms are, how much benefit you're getting from the drug, your overall metabolic picture, and your treatment alternatives.
5. Report adverse events. If you believe tirzepatide caused or worsened your neuropathy, you can report it directly to the FDA's MedWatch program. Real-world adverse-event reports inform how the medical community understands rare side effects. Your report matters more than you might think.
How Tirzepatide Compares to Other Diabetes Drugs in This Specific Context
If you have type 2 diabetes and you're choosing between tirzepatide and other classes — or considering switching — neuropathy is one of several factors, not the only one. A quick contextual scan:
- Metformin — first-line for type 2 diabetes, generally well-tolerated, but long-term use is associated with B12 deficiency, which can itself cause neuropathy. See our piece on metformin and the B12 deficiency connection.
- Semaglutide (Ozempic/Wegovy) — GLP-1 only. Strong A1C and weight benefits, somewhat smaller than tirzepatide. No documented neuropathy signal at the rates reported for tirzepatide. Our piece on Ozempic and neuropathy goes deeper.
- Insulin — direct glycemic control, no neuropathy signal as a drug effect, but rapid initiation can occasionally trigger treatment-induced neuropathy of diabetes (TIND) the same way any rapid A1C drop can.
- SGLT-2 inhibitors (jardiance, farxiga) — modest A1C effect, modest weight loss, cardiovascular and kidney benefits. No notable neuropathy signal.
The drug-class choice for diabetes is bigger than neuropathy alone, and your endocrinologist or primary care doctor is the right partner for that conversation. What's worth carrying into the visit is that tirzepatide specifically has produced a small but real signal that no other class has, and that's something to weigh — not panic over, but weigh.
Realistic Expectations
If you're hoping tirzepatide will fix your existing diabetic neuropathy, lower expectations. Even with dramatic metabolic improvement, nerve recovery is slow and incomplete. Damaged axons regrow at roughly 1 millimeter per day under ideal conditions — so improvement from the foot to the lower leg can take months, and full reversal at advanced stages is uncommon. What's realistic is slowed progression and, for some patients, partial symptom improvement over many months.
If you're worried about tirzepatide causing neuropathy, the rare-but-real frequency means most patients will not develop the side effect. But “most” doesn't mean “you.” Knowing the warning signs — new tingling, sharp progression with dose increases, symptoms in someone without diabetes — lets you catch a problem early when it's most likely to be reversible.
The cleanest mental model: tirzepatide is a powerful drug doing powerful things to your metabolism. Powerful drugs deserve careful monitoring. Whether your nerve story turns out to be a good one or a concerning one depends on factors you can partially influence (titration speed, dose, monitoring) and factors you can't (your individual biology). Knowing both possibilities exist and watching for both is what informed patient-hood looks like.
Bringing This to Your Doctor

If you're going into an appointment to discuss tirzepatide and nerve symptoms, here are questions that move the conversation forward:
- “Based on the timing and pattern of my symptoms, do you think this is more likely tirzepatide-related, diabetes-related, or treatment-induced neuropathy of diabetes from rapid blood-sugar improvement?”
- “Are there tests we can do to help distinguish?”
- “What's your threshold for adjusting my dose or switching me to a GLP-1-only drug like semaglutide?”
- “If we keep me on tirzepatide, what should I watch for that would change your recommendation?”
Our guide on how to talk to your doctor about neuropathy pain has more on getting the most from these conversations.
Frequently Asked Questions
Does Mounjaro cause neuropathy?
Peripheral neuropathy has been reported as a rare adverse event for tirzepatide (Mounjaro and Zepbound) at frequencies below 1% in post-marketing surveillance and case-report literature. It is not a common side effect, but the signal is real. New nerve symptoms after starting tirzepatide — particularly after dose increases to 10 mg or 15 mg — warrant a conversation with your prescriber.
Can tirzepatide reverse my diabetic neuropathy?
Tirzepatide is not FDA-approved as a neuropathy treatment, and no pivotal clinical trial has tested neuropathy progression as a primary endpoint. However, because tirzepatide dramatically improves A1C and produces significant weight loss — both of which are major drivers of nerve damage in type 2 diabetes — it is biologically plausible that successful tirzepatide therapy could slow diabetic neuropathy progression and produce partial symptom improvement over many months. Complete reversal is uncommon, especially at advanced stages of nerve damage.
Should I stop Mounjaro if I get tingling in my feet?
Do not stop tirzepatide on your own without your prescriber's input. Abrupt discontinuation can cause rapid blood-sugar rebound. Document the timing and pattern of symptoms carefully, then bring the information to your endocrinologist or primary care doctor. They will help determine whether the symptoms are likely drug-related, metabolic, or another cause, and discuss whether dose reduction, slower titration, switching drugs, or stopping is the best path.
Will losing weight on Zepbound help my nerve pain?
Excess body weight is an independent risk factor for peripheral neuropathy, separate from diabetes. Substantial weight loss — including through tirzepatide-induced weight reduction — can plausibly reduce neuropathy progression and, in some patients, produce partial symptom improvement. The mechanism likely involves reduced inflammation, improved insulin sensitivity, and reduced mechanical strain. Improvement is generally gradual and often partial rather than complete.
What dose of tirzepatide is most likely to cause nerve side effects?
Patient reports and case-series literature suggest that new or worsening nerve symptoms most commonly occur during titration to the higher doses, particularly 10 mg and 15 mg. Lower doses (2.5 mg, 5 mg) have produced fewer such reports. This pattern is consistent across the available data, though not all patients at higher doses experience nerve symptoms.
Is the neuropathy permanent if I stop tirzepatide?
Most case reports describe partial improvement after discontinuation, though some patients have persistent residual symptoms. Outcomes appear to depend on how long symptoms were present before stopping the drug and how severe they became. Earlier recognition and earlier discontinuation tend to be associated with more complete recovery. Long-term outcome data for tirzepatide-related neuropathy is still limited because the drug is relatively new.
How is tirzepatide different from semaglutide for neuropathy risk?
Tirzepatide activates both the GLP-1 and GIP receptors. Semaglutide activates only the GLP-1 receptor. The neuropathy signal that has emerged for tirzepatide has not appeared at the same frequency for semaglutide. Why this difference exists is not yet understood. Possible explanations include the additional GIP receptor activation, dose-related effects, or other pharmacologic differences. For patients concerned about the neuropathy signal specifically, semaglutide may be discussed with the prescriber as an alternative GLP-1 option.
Can people without diabetes develop neuropathy from Zepbound?
Yes, this has been reported. Cases of new peripheral neuropathy in non-diabetic patients taking Zepbound for weight management have appeared in case reports and patient communities. This pattern is particularly concerning because the usual explanations (diabetic neuropathy from poor control, treatment-induced neuropathy of diabetes from rapid A1C drops) do not apply. New nerve symptoms in a non-diabetic patient on Zepbound warrant prompt evaluation by your prescribing clinician and possible neurology referral.