Cebranopadol is the drug I've been getting the most questions about lately, and there are good reasons for that. The headline news — that Tris Pharma's Phase 3 trials in acute postoperative pain produced results that, in post-hoc analysis, beat oxycodone — broke through in a way most drug news doesn't. Patients in the neuropathy community immediately wanted to know two things: would it work for chronic nerve pain, and could they get it.
The honest answer to both questions is “it's complicated, but there's real reason for cautious interest.” Cebranopadol is not approved for any condition yet. The Phase 3 program that recently succeeded was for acute pain, not chronic neuropathy. But the earlier Phase 2 data in diabetic neuropathic pain was genuinely promising, the mechanism is unlike anything currently approved for nerve pain, and the FDA submission is moving forward. Let me walk you through what we actually know — what the science is, what the data shows, and what realistic patient access looks like over the next several years.
What Cebranopadol Is and Why It's Different
Cebranopadol is an investigational oral pain medication developed by Tris Pharma. It's classified as a “first-in-class dual NMR agonist” — a mouthful that translates to: it activates two different receptors in your pain pathways at the same time, and that combination doesn't match any drug currently on the market.
The two receptors are the µ-opioid peptide (MOP) receptor — the receptor that morphine, oxycodone, hydrocodone, and every other classical opioid engages — and the nociceptin/orphanin FQ peptide (NOP) receptor — a receptor in the same broad family but with a very different physiologic role.
Engaging MOP produces powerful pain relief. It also produces the things we don't want from opioids: euphoria that drives misuse, respiratory depression that makes overdoses deadly, tolerance that requires escalating doses, and physical dependence. Cebranopadol's design idea is that simultaneous NOP activation modulates the MOP response — preserving the analgesia while damping down the abuse-liability and respiratory-risk pieces.
That's the theory. The Phase 3 data so far supports it for acute pain. Whether it holds up across the years of chronic use that neuropathy treatment requires is still being studied.
The Dual NOP/MOP Mechanism in Plain Language
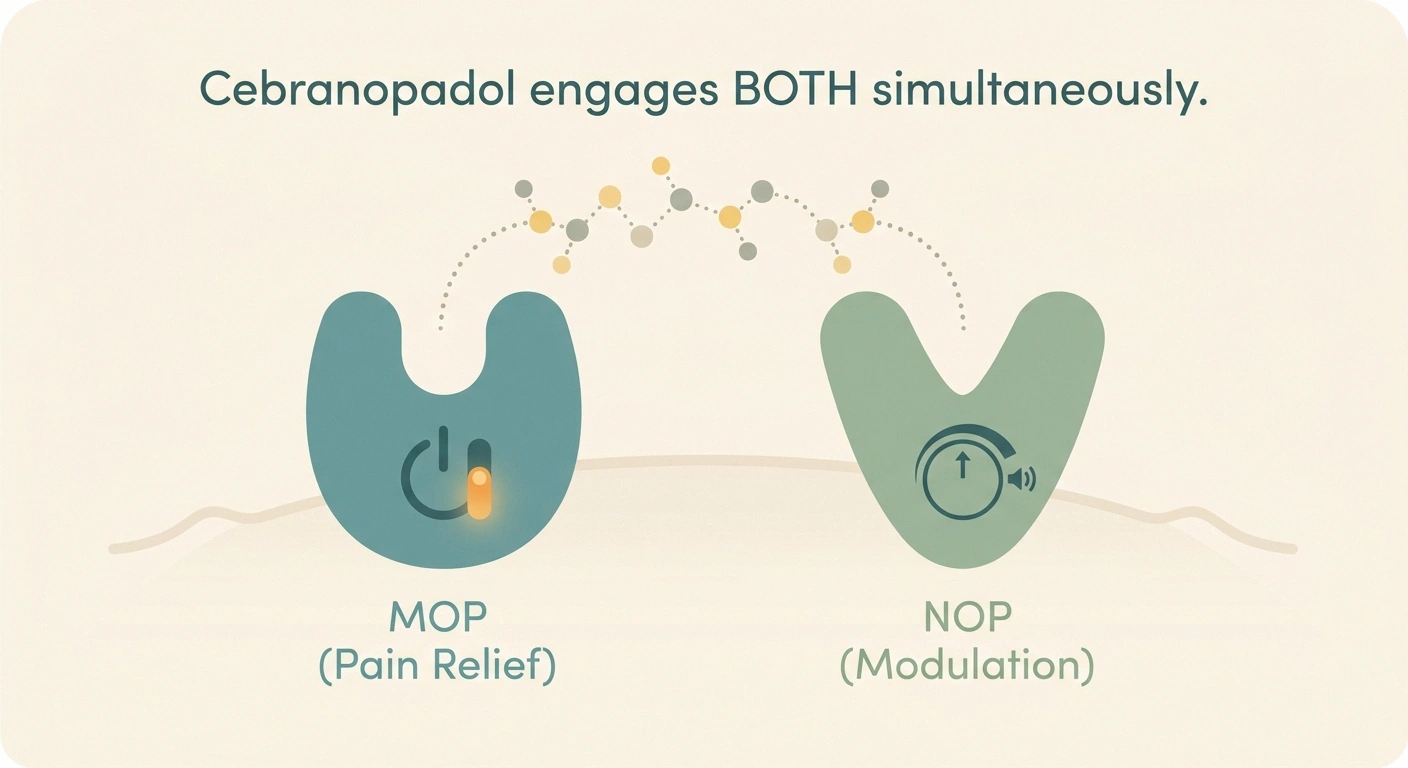
If you picture your pain signaling as a household alarm system, MOP is the system's main “off” switch. Hit it hard with a classical opioid and the alarms quiet down — but you also get all the side effects of fully disabling the alarm. NOP is more like a volume knob on the alarm itself; turning it down dampens the noise without flipping the master switch.
Cebranopadol engages both at once. The pain relief comes from the MOP component. The “softer” character of that relief — the apparent reduction in euphoric “high” that classical opioids produce — appears to come from the simultaneous NOP signaling pulling the response in a different direction.
In preclinical animal studies, this combination produced strong analgesia in models of acute pain, chronic neuropathic pain (including chemotherapy-induced models), and inflammatory pain — with measurably less of the reward-pathway activation that drives addiction in animal models.
The clinical reality is more nuanced than the theory. Cebranopadol is not a “non-opioid” drug. It IS engaging the opioid receptor. The question is whether the addition of NOP engagement meaningfully changes the abuse-liability profile in humans over months and years of use. We won't have a firm answer to that until post-marketing surveillance after FDA approval.
What the ALLEVIATE Phase 3 Trials Showed

The Phase 3 program that recently completed is called ALLEVIATE, and it tested cebranopadol in two acute postoperative pain models.
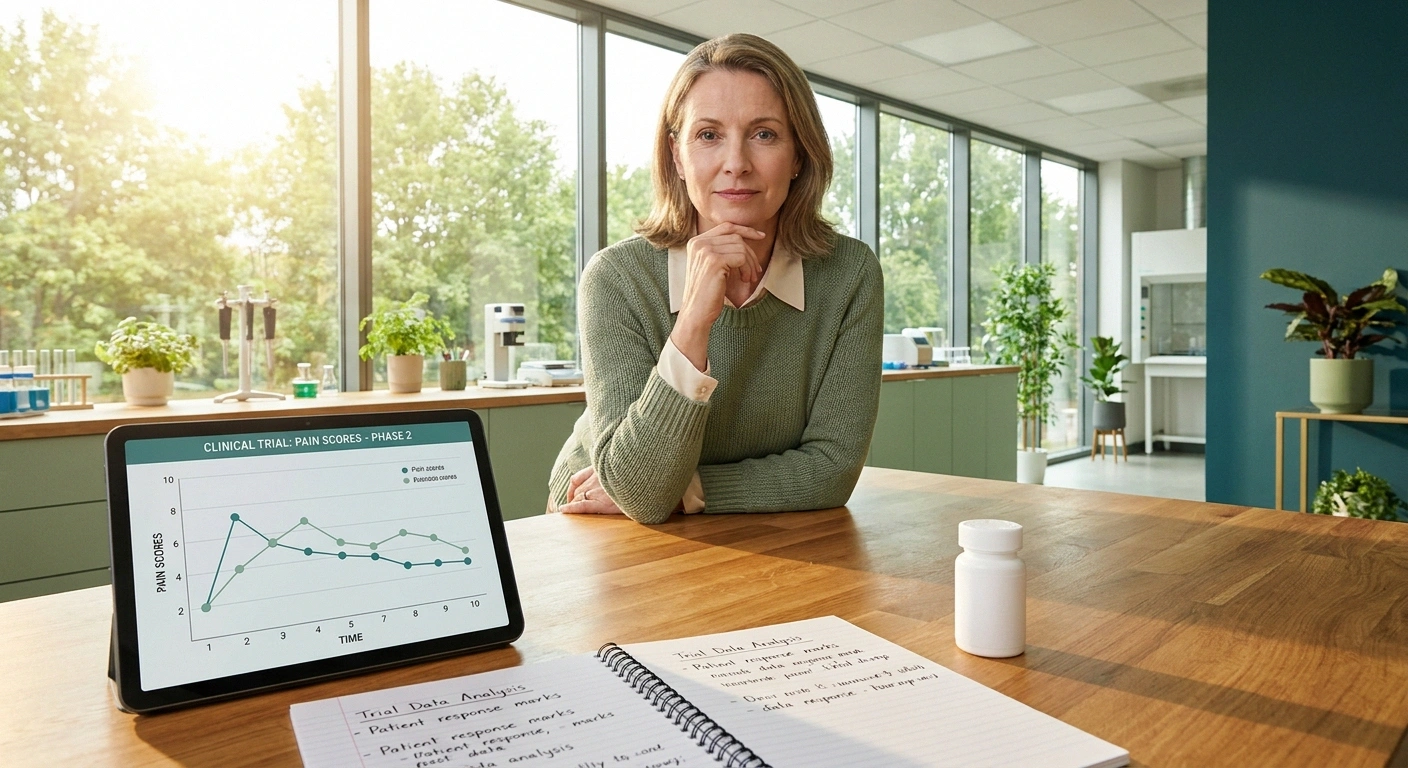
ALLEVIATE-1 (ClinicalTrials.gov NCT06545097) studied patients after abdominoplasty surgery. The primary endpoint was the area under the curve of the Pain Numeric Rating Scale from 4 through 48 hours after surgery — basically a measure of total pain experienced over a critical post-op window. Cebranopadol met that endpoint with statistically significant reduction compared to placebo, with what Tris Pharma described as a favorable safety profile.
ALLEVIATE-2 (NCT06423703) studied patients after bunionectomy — a foot surgery. Same primary endpoint structure, this time from 2 through 48 hours after dosing. Cebranopadol met its primary endpoint. In a post-hoc analysis (meaning an analysis specified after the data came in, not in advance), cebranopadol showed greater analgesic efficacy than the active comparator, oxycodone IR 10 mg — which is a standard mid-strength postoperative opioid.
“Greater than oxycodone in a post-hoc analysis” is genuinely notable, but worth flagging two caveats. Post-hoc analyses are exploratory, not confirmatory; the FDA gives them less weight than pre-specified analyses. And acute postoperative efficacy doesn't automatically translate to chronic nerve-pain efficacy — those are different conditions with different signaling biology.
Following these results, Tris Pharma announced plans to submit an FDA New Drug Application (NDA) for acute pain. That's the regulatory step before approval consideration.
What the Earlier Diabetic Neuropathy Data Showed
Here's where the neuropathy story gets relevant. Cebranopadol has been in clinical development for years — over 32 trials involving more than 2,200 participants across acute pain, chronic pain, and diabetic neuropathic pain indications. The DPN-specific data is from earlier Phase 2 studies.
Those Phase 2 studies in painful diabetic peripheral neuropathy showed positive efficacy signals — meaningful pain reduction in patients on cebranopadol compared with placebo — with a generally favorable safety profile. The trials were not large enough to be definitive, but they were positive enough to justify continued development.
Preclinical research published in journals like Pain and Inflammopharmacology has also shown that cebranopadol is effective in mouse models of chemotherapy-induced peripheral neuropathic pain, which is a different population of nerve-pain patients where current treatment options are particularly limited.
The pattern that emerges: the drug appears to work across a broad range of pain types, not just acute pain. Whether the magnitude of effect in chronic neuropathy will be large enough to justify dedicated approval, and how it will compare on a daily-use basis to existing options like duloxetine or pregabalin, are still open questions.
Where Cebranopadol Sits vs Today's Options
To make sense of where cebranopadol would fit in the chronic neuropathy toolbox, it helps to look at what's currently available.
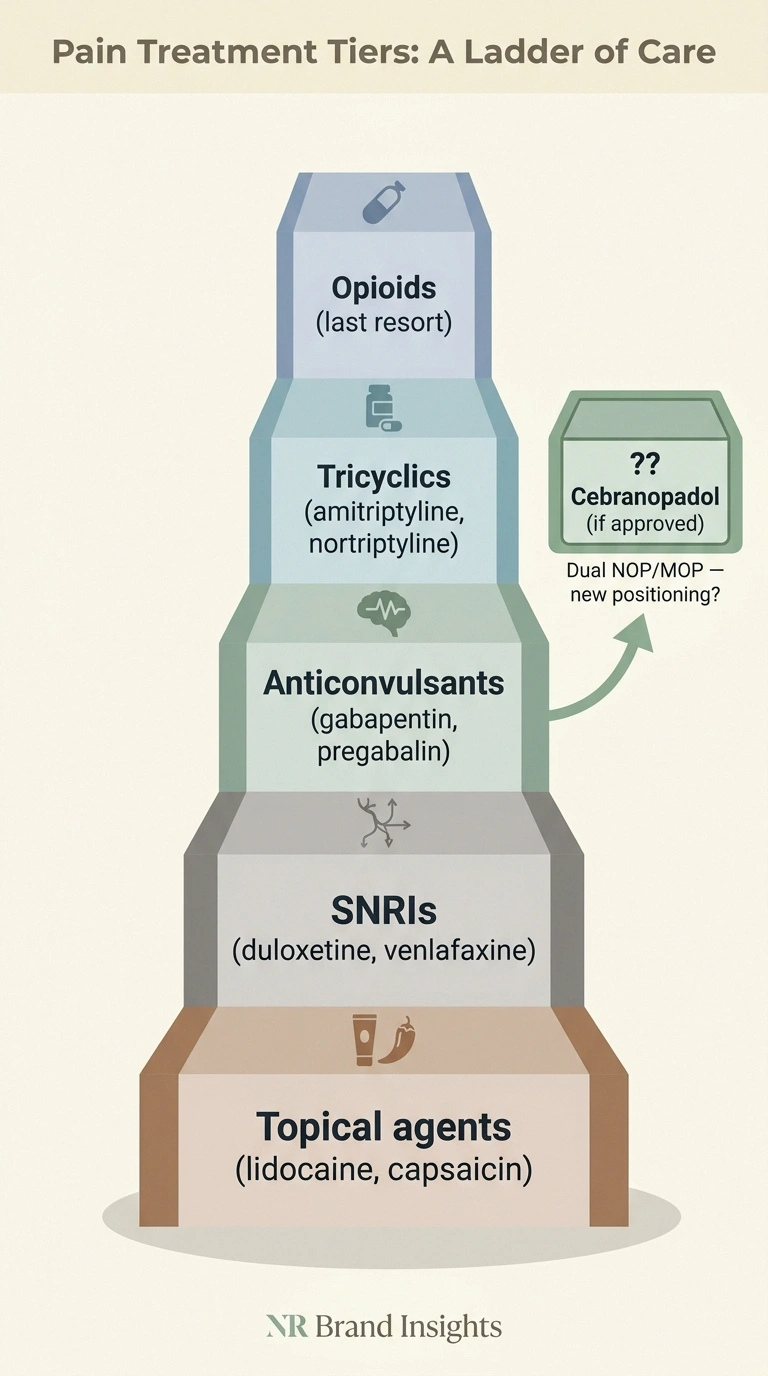
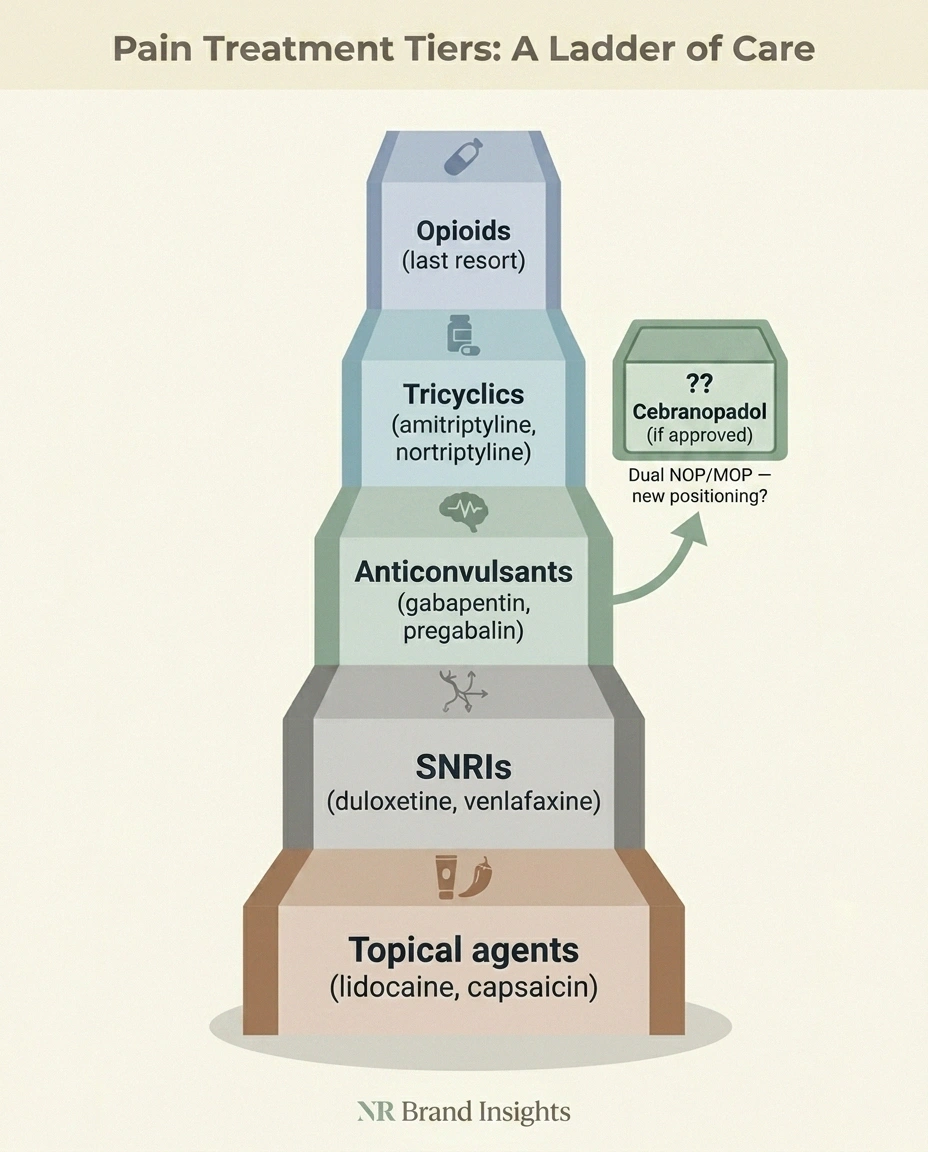
For peripheral neuropathic pain, the typical treatment ladder starts with anticonvulsants — gabapentin or pregabalin — or SNRIs like duloxetine and venlafaxine. Tricyclic antidepressants like amitriptyline and nortriptyline are also commonly used. Topical agents — lidocaine patches, capsaicin cream — can help for localized pain.
When all of these fail or aren't tolerated, the conversation about opioids enters. Opioid use for chronic neuropathic pain is controversial and increasingly restricted. The reality is that for some patients, especially those with severe and unresponsive symptoms, opioids remain the only thing that provides function. But the risks — physical dependence, tolerance, overdose risk, restrictive prescribing rules — make them a last resort.
If cebranopadol's clinical profile holds up, it could sit in a new spot: a drug that engages the opioid system enough to provide potent pain relief, but with a substantially reduced abuse-liability profile that makes long-term chronic use more feasible. That would be genuinely novel positioning.
It would NOT replace gabapentin or duloxetine as first-line, almost certainly. Those are inexpensive generics with decades of clinical experience. Cebranopadol, as a brand-new drug, will arrive expensive, prior-authorization-laden, and reserved for patients who have failed standard options.
The Realistic Timeline
This is the section that matters most for anyone considering whether to wait, plan around, or pivot toward cebranopadol. Here's the realistic timeline.
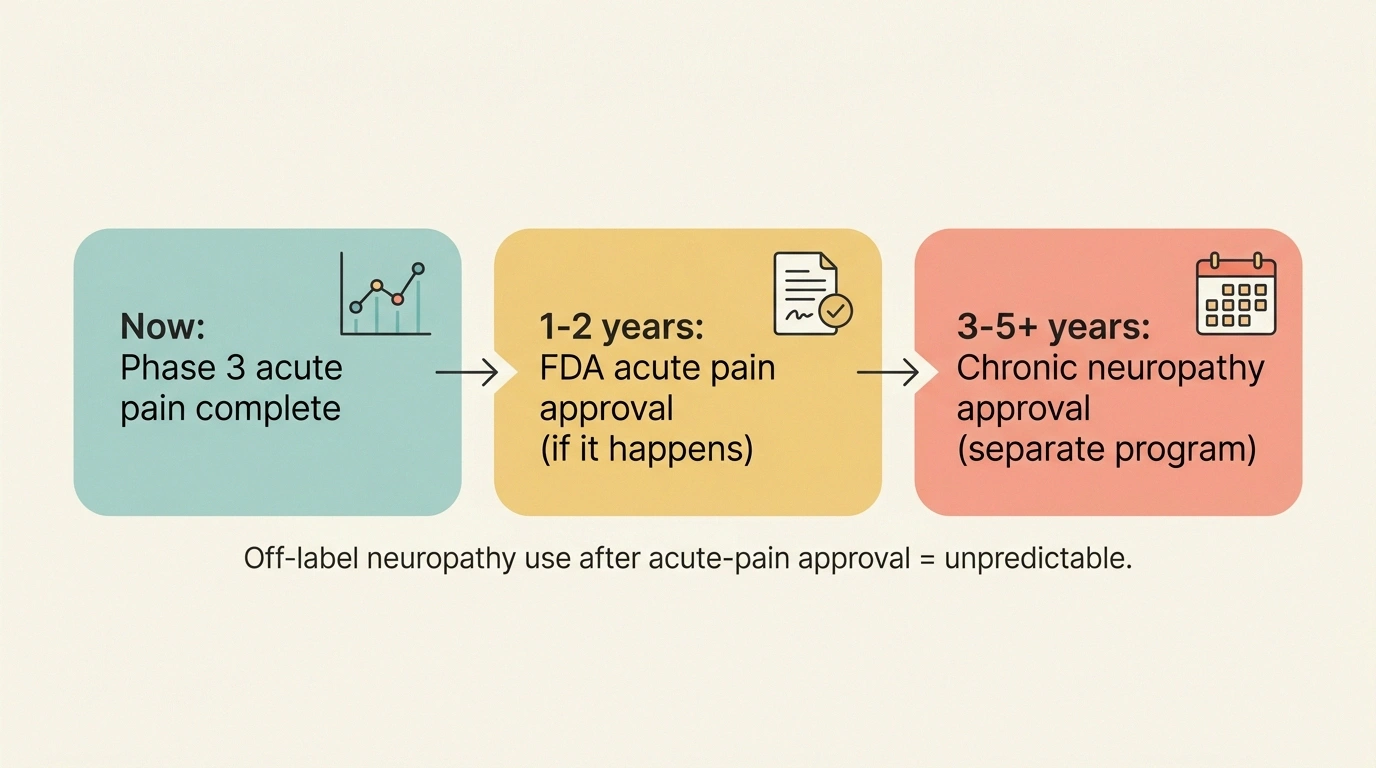
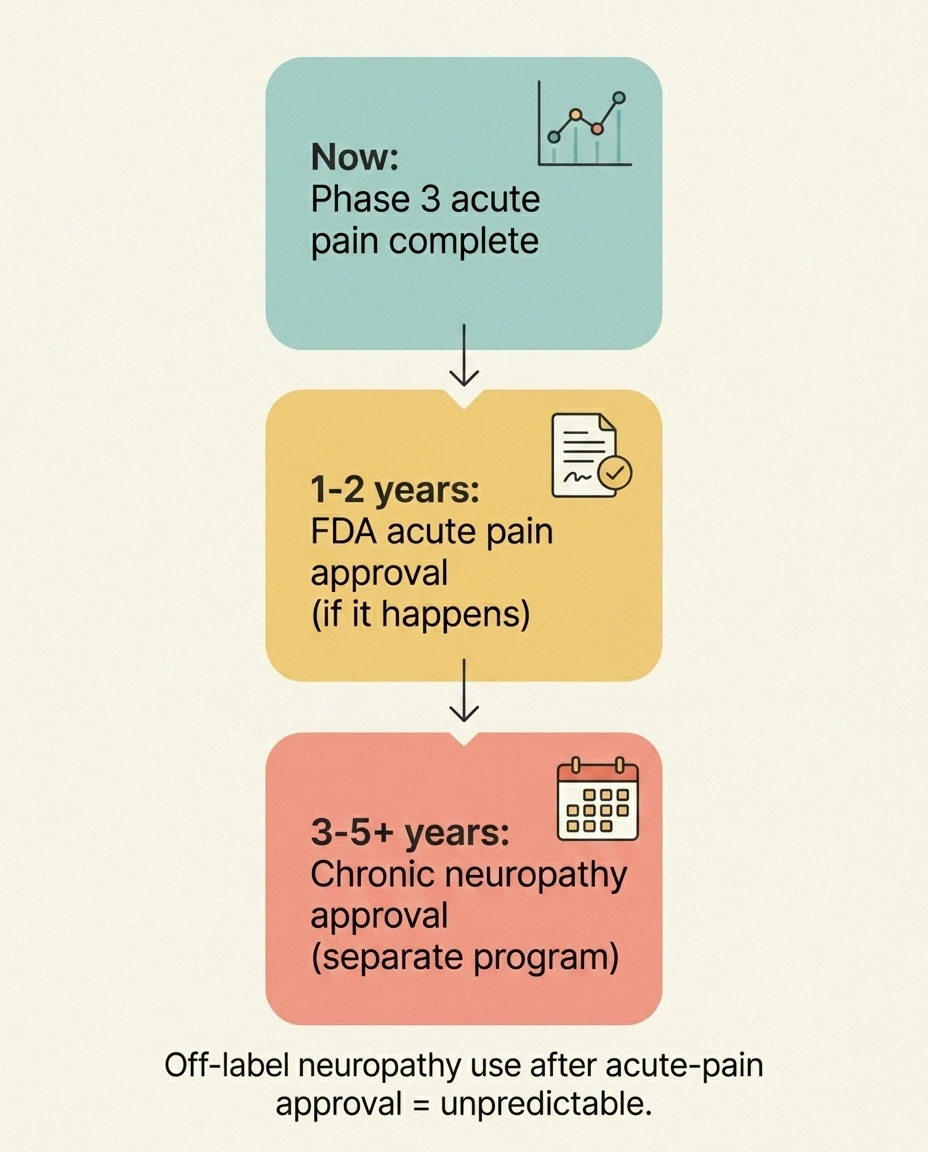
For acute pain: FDA submission is planned now. NDA review typically takes 10 months for standard review or 6 months for priority review. If priority review is granted and approval lands, cebranopadol could be available in pharmacies for acute postoperative pain in 2026 or 2027. That doesn't directly help chronic neuropathy patients, but it does mean the drug exists and doctors can theoretically prescribe it off-label.
For chronic neuropathic pain: A dedicated approval would require a separate Phase 3 program testing cebranopadol over weeks or months in patients with established neuropathy. Whether and when Tris Pharma initiates such a program depends on commercial strategy and trial design. Realistic earliest neuropathy-specific approval: 2028-2030.
For off-label use after acute-pain approval: This is the wild card. Once a drug is approved for any indication, doctors can legally prescribe it off-label for other conditions. Off-label use for neuropathic pain happens routinely with many drugs. Whether cebranopadol becomes a commonly off-label-prescribed neuropathy drug after acute-pain approval depends on physician comfort, insurance coverage, and the drug's positioning by the company.
Insurance coverage for off-label use of a new brand-name drug is unpredictable. Some plans cover it freely with prior authorization documenting failed alternatives. Some refuse. This will be a case-by-case fight if patients pursue it early.
The Side Effect Picture
In the published Phase 3 acute-pain data, the most common adverse events with cebranopadol were nausea, vomiting, dizziness, and headache — a profile broadly similar to other centrally-acting analgesics. Critically for the abuse-liability question, the trials specifically tracked indicators of euphoria and reinforcing effects; the early data suggests these are reduced compared with classical opioids.
What we don't yet have is long-term chronic-use data. Tolerance development, dependence over months of daily dosing, withdrawal characteristics, drug interactions across the full pharmacopeia — these come into focus through post-marketing experience after approval. Patients who become early adopters of any new drug are, in essence, contributing to that body of evidence.
For chronic neuropathy patients, the side effect profile will need to be acceptable across years, not just days. That's a different bar than acute-pain trials test.
What to Discuss With Your Doctor

If you're paying attention to cebranopadol because your current neuropathy treatments aren't working, here are the practical conversations to have.
- Have I given my current medications a fair trial at therapeutic doses?
- Have I seen a pain specialist or neurologist for a second opinion?
- Am I addressing the underlying cause (glucose control, etc.)?
- Could a current clinical trial enrollment be the right move?
First — and this matters more than the drug pipeline — make sure you've gone through the standard options thoughtfully. Many patients land on a sub-therapeutic dose of gabapentin and conclude “gabapentin doesn't work,” when the issue is that they never got titrated up. Same with duloxetine and pregabalin. A meaningful trial of a current option includes adequate dose escalation, sufficient duration (often 4-8 weeks), and good adherence. If you haven't been through that, the next drug — including cebranopadol if it arrives — isn't likely to be different.
Second, if you've tried multiple standard options and still have inadequate relief, ask your doctor about clinical trial enrollment. Cebranopadol may not have an active neuropathy-specific trial enrolling right now, but other late-stage candidates do. Search ClinicalTrials.gov by your condition and your geographic area, and bring options to your doctor.
Third, ask about referral to a pain specialist or pain clinic if you haven't been seen by one. Pain medicine physicians have access to specialized treatments — nerve blocks, spinal cord stimulation, dorsal root ganglion stimulation, ketamine infusion — that primary care doesn't typically offer. These can fill the gap while drug development continues.
Fourth, follow the news but don't reorganize your life around an unapproved drug. The realistic 2026-2027 question is: “What can I do now to improve my situation?” That's a question with concrete answers — better glucose control if you're diabetic, evidence-based supplements, physical therapy, mental-health support for the chronic-pain dimension, and optimization of current medications.
Where Cebranopadol Fits in the Bigger Picture
The broader story is that there's more nerve-pain drug development happening right now than at any point in the last twenty years. Cebranopadol is one of multiple novel candidates in late-stage trials — alongside pilavapadin, VX-993, and others.
For patients, this means the medicine cabinet is genuinely going to look different in three to five years. Not every candidate will succeed. But the diversity of mechanisms in late-stage testing — selective sodium-channel blockade, AAK1 inhibition, dual NOP/MOP engagement, gene therapy — means at least some of these are likely to clear the FDA bar.
For our complete map of the late-stage pipeline, see our 2026 neuropathy drug pipeline guide. For broader context on emerging treatments beyond drugs, see our coverage of new neuropathy treatments in 2026.
The thing I want you to leave with is this: cebranopadol is a real candidate worth watching, the science is interesting, and the Phase 3 data so far is encouraging. AND patient access remains years away, the chronic neuropathy indication specifically is going to take longer than the acute pain indication, and your treatment plan today should be built around what's available today. Hold both of those at once. That's how to follow drug development without letting it distort your present care.
Frequently Asked Questions
Is cebranopadol approved by the FDA?
No. As of 2026, cebranopadol is investigational. Tris Pharma is preparing an FDA New Drug Application based on the Phase 3 ALLEVIATE results for acute postoperative pain. Approval, if it happens, would be specifically for acute pain initially — not chronic neuropathy.
Will cebranopadol be approved for neuropathy specifically?
A dedicated neuropathy approval would require a separate Phase 3 program. Whether and when that happens depends on Tris Pharma's commercial strategy. The realistic earliest timeline for a chronic neuropathy approval is 2028-2030.
Is cebranopadol an opioid?
It engages the µ-opioid receptor, so functionally yes — it works through the opioid system. What makes it different from classical opioids is the simultaneous engagement of the NOP receptor, which appears to reduce (not eliminate) the abuse-liability and respiratory-depression risk seen with traditional opioids. It is not classified as a non-opioid drug.
Could my doctor prescribe cebranopadol off-label for neuropathy if it gets approved for acute pain?
Once a drug is FDA-approved for any condition, off-label prescribing is legal at the physician's discretion. Whether it would happen depends on clinical judgment, insurance coverage (which is often restrictive for off-label use of new brand-name drugs), and physician comfort with a new mechanism.
How does cebranopadol compare to gabapentin or duloxetine?
Gabapentin and duloxetine work through entirely different mechanisms (α2δ calcium channel binding and serotonin/norepinephrine reuptake inhibition, respectively). They're inexpensive generics with decades of clinical experience. Cebranopadol, as a brand-new opioid-receptor-engaging drug, would arrive expensive and reserved for patients who have failed standard options. Direct head-to-head trials in neuropathy haven't been conducted.
What were the side effects in the trials?
The most common adverse events with cebranopadol in the acute-pain Phase 3 trials were nausea, vomiting, dizziness, and headache — a profile broadly similar to other centrally-acting analgesics. Long-term chronic-use data is more limited.
Is there a clinical trial of cebranopadol for neuropathy I can join?
Check ClinicalTrials.gov for current cebranopadol trials. The published Phase 2 trials in diabetic neuropathy completed years ago; whether a new Phase 3 program in neuropathy is recruiting depends on Tris Pharma's plans. Other late-stage neuropathy drug trials (for pilavapadin, VX-993, and others) may be relevant alternatives.
Should I wait for cebranopadol before trying current neuropathy treatments?
No. The realistic neuropathy-specific approval timeline is at least three years away, possibly longer. Untreated chronic neuropathy can progress and impact quality of life significantly. Work with your doctor on currently available options and stay informed about what's emerging.
How can I follow cebranopadol news?
Tris Pharma posts trial updates through press releases and its investor relations page. NeurologyLive, Patient Care Online, and similar industry-focused outlets cover late-stage drug news. This site publishes updates as significant readouts occur.


