
For a long time, I thought of my neuropathy as a “feet problem.” The numbness, the tingling, the burning at night — it all felt like it lived below the knees, separate from the rest of my body. Then a friend in my support group mentioned that her neurologist had ordered a heart rhythm test. I asked her why, and her answer surprised me: “Because the same nerves that aren't talking to my feet aren't talking to my heart, either.”
That single sentence changed how I understand neuropathy. The nerves that carry sensation from your toes are part of the same vast electrical network that tells your heart how fast to beat, your blood vessels when to constrict, and your blood pressure how to respond when you stand up. When that network is damaged, the consequences don't stay in your feet.
This article walks through what the research actually shows about the connection between neuropathy and heart disease — including a quieter, often-missed condition called cardiac autonomic neuropathy that may be the single most important reason to take peripheral nerve damage seriously as a whole-body issue.
The Nerves Behind Your Heartbeat
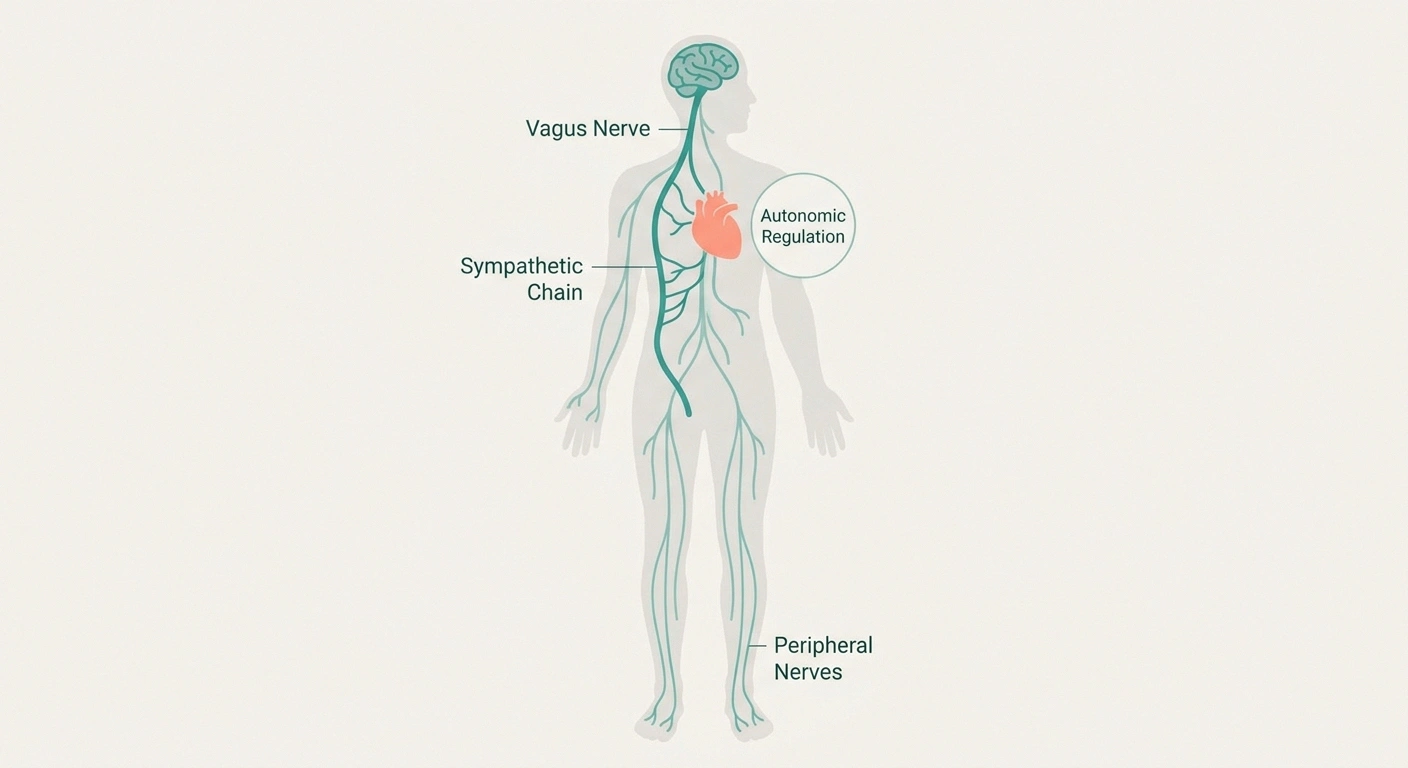
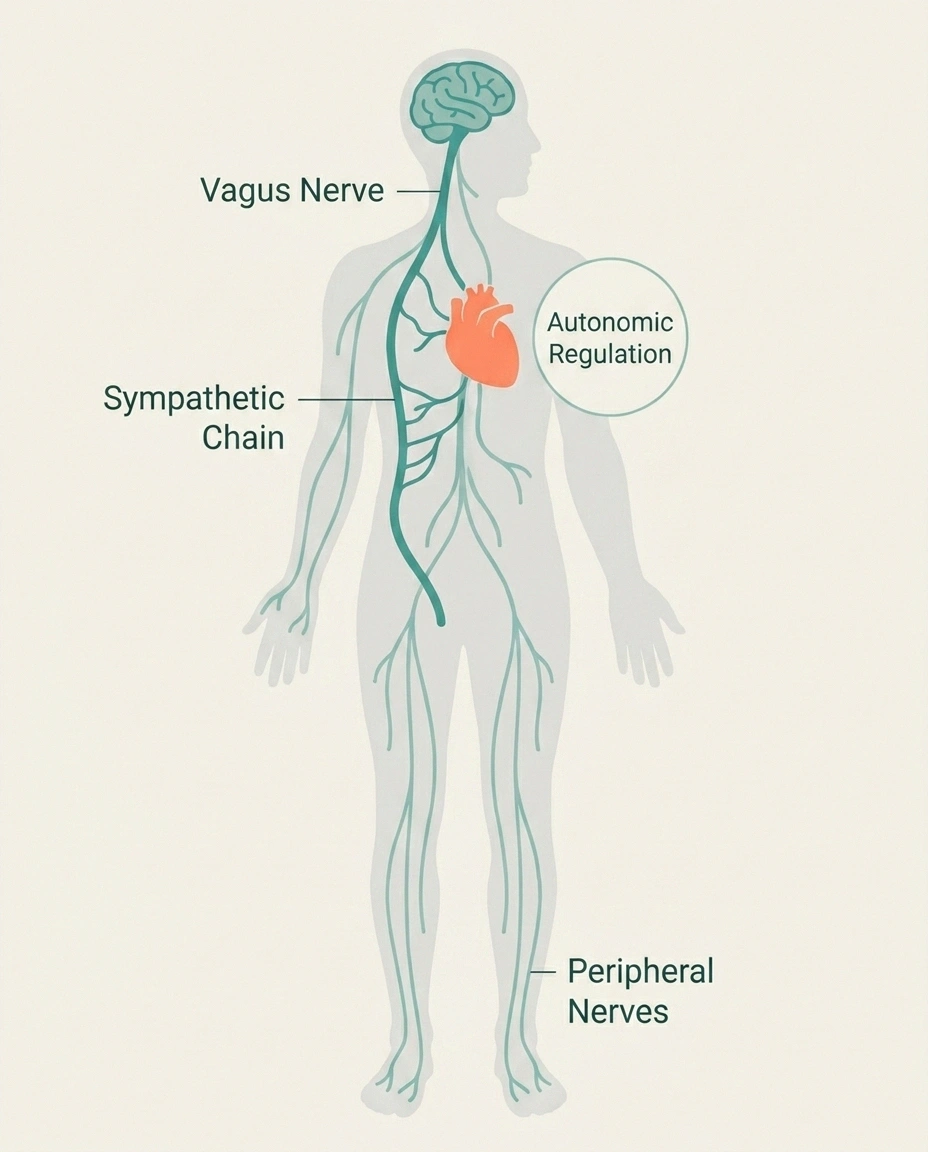
Most people associate “neuropathy” with damage to the sensory nerves — the ones that carry signals about pain, temperature, and touch from your skin to your brain. But the peripheral nervous system has another major branch called the autonomic nervous system, which runs the things you don't consciously control: heart rate, blood pressure, digestion, sweating, bladder function.
Key Takeaway
The autonomic nerves that control your heart rate and blood pressure are part of the same peripheral nervous system that runs to your feet. When peripheral neuropathy is present, autonomic damage to the heart — called cardiac autonomic neuropathy — often quietly accompanies it.
The autonomic system has two competing arms. The parasympathetic branch (working largely through the vagus nerve) slows your heart and lowers blood pressure. The sympathetic branch speeds your heart up and raises blood pressure when you need to act. In a healthy body, these two work in constant balance, adjusting your heart rate dozens of times every minute in response to breathing, posture, emotion, and activity.
When the autonomic nerves get damaged — by diabetes, chemotherapy, autoimmune disease, alcohol, or other causes — that balance breaks down. The condition is called cardiac autonomic neuropathy, often shortened to CAN. It's not as well-known as diabetic foot neuropathy, but it may be more dangerous.
What Cardiac Autonomic Neuropathy Actually Looks Like

CAN is sneaky. Unlike the burning, tingling, and stabbing pains of small fiber neuropathy, autonomic damage often produces symptoms that are easy to dismiss or misattribute. Many people walk around with significant CAN for years before anyone connects the dots.
Five Warning Signs of Cardiac Autonomic Neuropathy
1. Resting heart rate over 90-100 bpm
Vagal “brake” weakened — sympathetic accelerator runs unopposed.
2. Dizziness on standing (orthostatic hypotension)
Blood pressure does not adjust to postural changes.
3. Loss of heart rate variability
A healthy heart speeds up on inhale, slows on exhale. CAN flattens this.
4. Exercise intolerance
Heart rate doesn't ramp up properly — or recover normally afterward.
5. Silent myocardial ischemia
Heart attack without chest pain. Most dangerous sign — and most common in CAN.
The most common signs include:
- Resting tachycardia. A consistently fast heart rate at rest — typically above 90 to 100 beats per minute when you're sitting quietly. This happens because the parasympathetic vagal “brake” on the heart has been weakened by nerve damage, leaving the sympathetic accelerator unopposed.
- Orthostatic hypotension. Your blood pressure drops when you stand up. You feel dizzy, lightheaded, sometimes nearly faint. The autonomic nerves that should constrict your blood vessels and increase your heart rate during postural changes aren't responding fast enough.
- Loss of heart rate variability. A healthy heart doesn't beat at a metronomic, fixed rate — it speeds up slightly when you breathe in, slows when you breathe out. Loss of this normal variation is one of the earliest signs of CAN, often detectable before any symptoms appear.
- Exercise intolerance. Your heart can't ramp up appropriately for activity, so you fatigue quickly, feel breathless out of proportion to effort, or your heart rate doesn't recover normally after exercise.
- Silent myocardial ischemia. This is the most dangerous one. The pain signals from the heart muscle to the brain are dampened by autonomic damage, which means a heart attack can occur without chest pain. People with diabetes and CAN are particularly at risk for “silent” cardiac events.
If any of these sound familiar, especially the dizziness on standing or unexplained resting tachycardia, this is worth raising with your doctor — especially if you've already been diagnosed with peripheral neuropathy.
Why the Connection Exists: Shared Roots
The link between neuropathy and heart disease isn't coincidence. It runs much deeper than two separate conditions that happen to occur together. The relationship has at least three different layers:
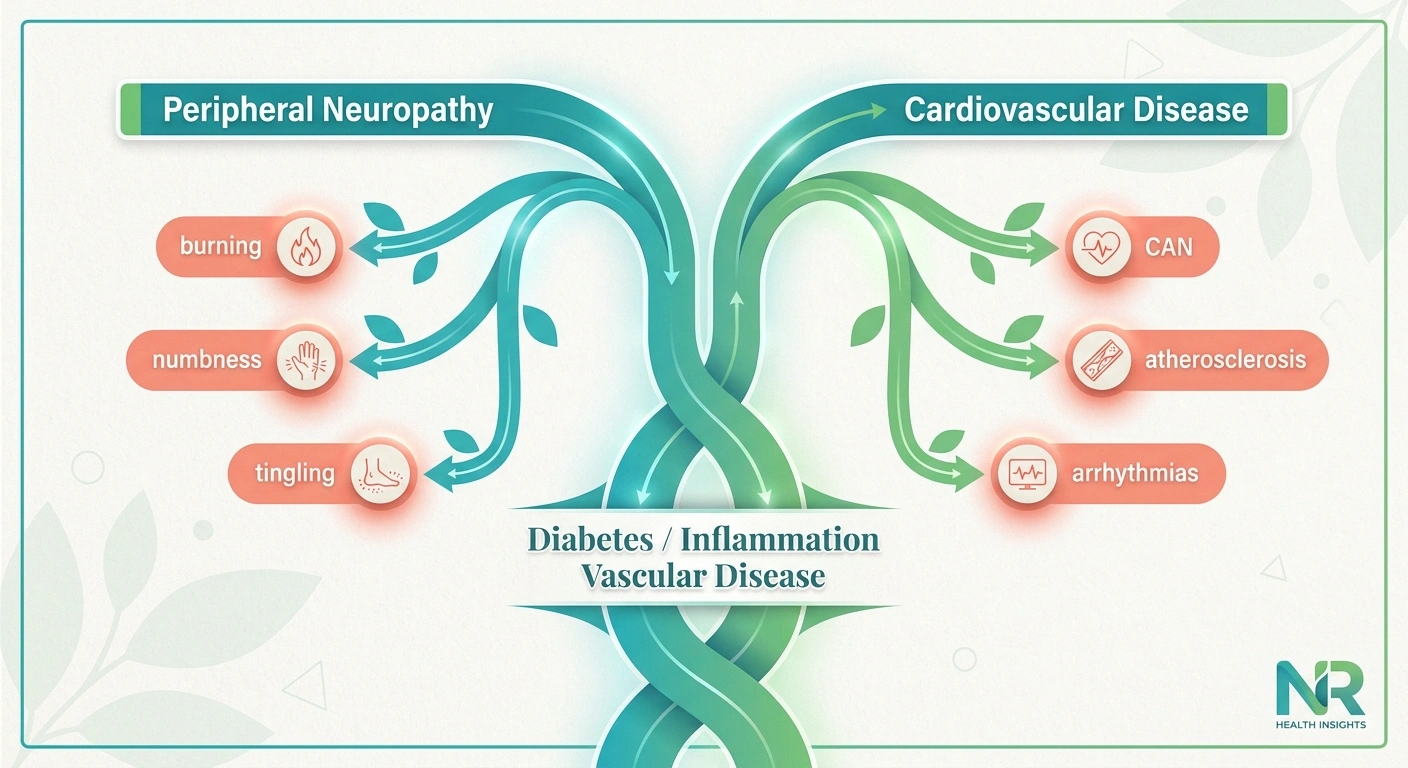
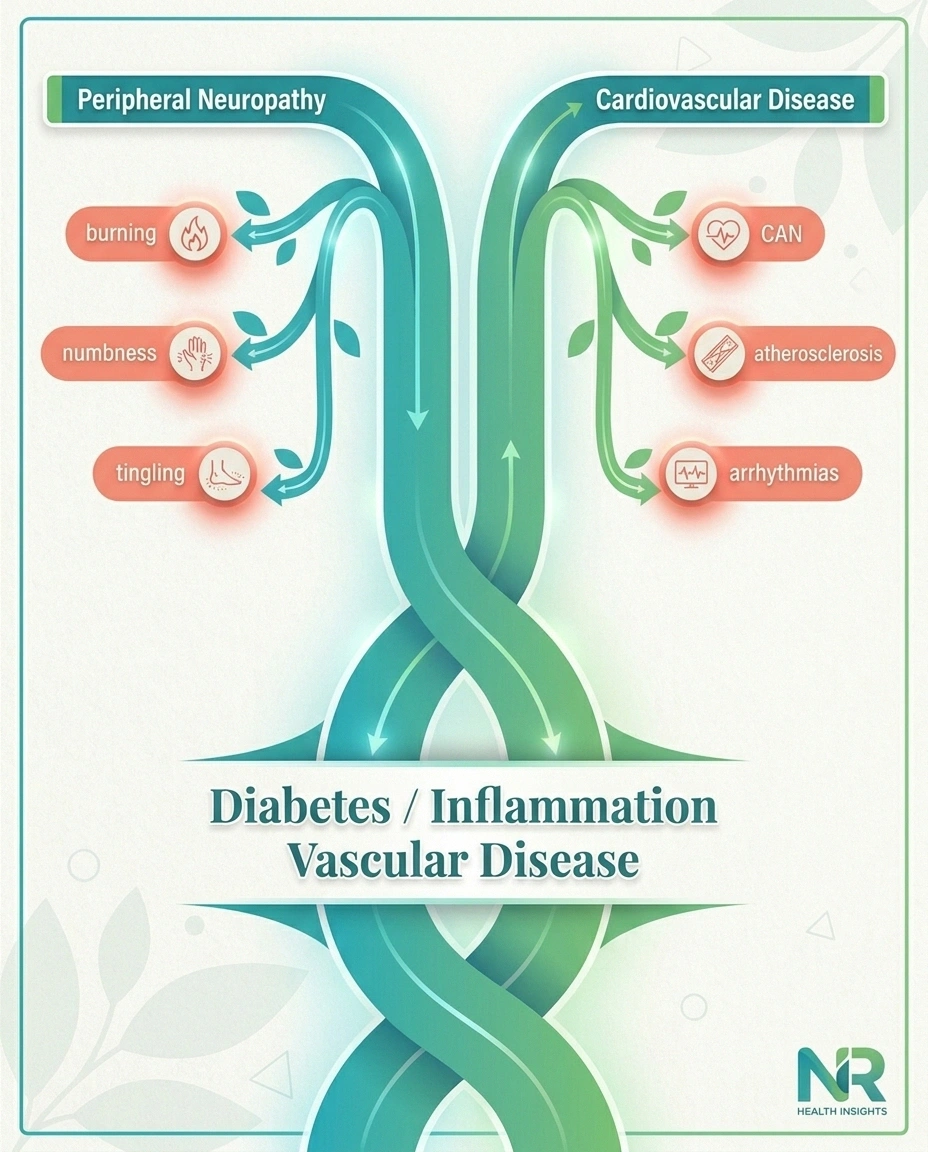
Layer 1: Direct autonomic damage to the heart. The nerves that regulate cardiovascular function are themselves peripheral nerves. The same processes that damage the sensory nerves in your feet — high blood sugar, microvascular disease, oxidative stress, inflammation — damage the autonomic nerves running to your heart and blood vessels. The damage isn't in two places by accident; it's in two branches of the same tree.
Layer 2: Shared upstream causes. Diabetes is the most obvious example. Long-term elevated blood glucose damages both peripheral nerves and blood vessels. The mechanisms include glycation of proteins, oxidative stress, inflammation, and microvascular changes. Diabetic neuropathy and atherosclerotic heart disease are essentially two outputs of the same underlying disease process. Hypertension, dyslipidemia, smoking, and obesity follow the same pattern — they injure both nerves and the cardiovascular system in parallel.
Layer 3: Systemic inflammation. A growing body of research points to chronic, low-grade inflammation as a shared driver of both peripheral neuropathy and cardiovascular disease. Markers like C-reactive protein, interleukin-6, and tumor necrosis factor-alpha are elevated in both conditions. The blood-nerve barrier and the endothelial lining of blood vessels are both vulnerable to inflammatory damage, and they often fail together.
This is why peripheral neuropathy has been called a “crystal ball” for cardiovascular disease in some clinical literature. When you see nerve damage, you're often looking at the visible tip of a much larger systemic problem.
The Mortality Numbers Matter
The research on CAN and mortality is sobering, and I think it's important to be honest about it rather than soft-pedal it. The point isn't to scare anyone — it's to make clear why this matters and why early detection changes outcomes.
🔎 Research Says
In a study of 3,250 patients with type 1 diabetes, cardiac autonomic neuropathy was the single strongest predictor of mortality — stronger than HbA1c, stronger than blood pressure, stronger than any other measured variable. CAN raises cardiovascular mortality risk two- to three-fold compared to people without autonomic damage.
One large study of 3,250 patients with type 1 diabetes found that cardiac autonomic neuropathy was the single strongest predictor of mortality over the follow-up period — stronger than HbA1c, stronger than blood pressure, stronger than any other measured variable. Other studies have shown two- to three-fold increases in cardiovascular mortality among patients with CAN compared to those without.
For people with type 2 diabetes, peripheral neuropathy itself — even without documented CAN — is an independent predictor of cardiovascular events. A 2025 cross-sectional study published in Scientific Reports found significantly higher rates of coronary artery disease, heart failure, and peripheral artery disease among T2D patients with peripheral neuropathy compared to those without it.
This doesn't mean a peripheral neuropathy diagnosis is a cardiac death sentence. The opposite, actually. It means peripheral neuropathy is a red flag that deserves a thorough cardiovascular workup — which can lead to early intervention, better risk-factor control, and dramatically better outcomes than waiting until something dramatic happens.
How CAN Is Diagnosed

The good news is that several simple, non-invasive tests can detect cardiac autonomic neuropathy long before it causes obvious symptoms. These are sometimes called the Ewing tests or cardiovascular autonomic reflex tests:
Warning
If your resting heart rate is consistently above 100 bpm, you feel dizzy on standing, or you experience unexplained breathlessness — do not wait. These can be signs of cardiac autonomic neuropathy. People with CAN are at higher risk of silent heart attacks. Discuss autonomic testing with your doctor.
- Heart rate response to deep breathing. You breathe deeply and slowly while your heart rate is monitored. A healthy heart speeds up on inhale, slows on exhale. Damaged autonomic nerves blunt this response.
- Valsalva maneuver. You exhale forcefully against a closed airway (like bearing down). The expected pattern of heart rate and blood pressure changes is well-defined; CAN flattens it.
- Heart rate response to standing. Going from lying to standing should produce a characteristic heart rate increase, then decrease. CAN dulls this.
- Blood pressure response to standing. A drop of more than 20 mmHg systolic or 10 mmHg diastolic on standing suggests autonomic dysfunction.
- 24-hour heart rate variability. A Holter monitor records every beat for a full day, allowing detailed analysis of how heart rate varies in response to normal life. Reduced variability is a sensitive marker of CAN.
If you have peripheral neuropathy and any concerning symptoms — frequent dizziness on standing, a resting heart rate consistently above 100, unexplained fatigue or exercise intolerance — ask your doctor whether autonomic testing is appropriate. The tests are inexpensive, widely available, and often covered by insurance when there's a clinical reason to order them.
Heart Disease as a Cause of Neuropathy (The Reverse Direction)
The connection runs both ways. Cardiovascular disease can also cause peripheral neuropathy through several mechanisms:
Peripheral artery disease (PAD) reduces blood flow to the legs and feet, which starves the nerves of oxygen and nutrients. The result is an ischemic neuropathy that often coexists with classic claudication symptoms. People with both PAD and diabetes are at especially high risk.
Heart failure with reduced cardiac output can compromise nerve perfusion throughout the body, contributing to neuropathic symptoms. Severe heart failure has been associated with both small fiber and large fiber neuropathy.
Statin medications, used widely for cardiovascular protection, are an under-recognized cause of peripheral neuropathy in some patients. The relationship is complicated and often debated, but for some people statin-induced neuropathy is a real and reversible phenomenon worth investigating if symptoms began after starting cholesterol medication.
Atrial fibrillation and other arrhythmias raise the risk of small embolic events that can damage nerves in the periphery, although this is a less common cause.
What This Means for Your Care

If you have peripheral neuropathy, the cardiovascular implications shift the calculus on several aspects of your medical care. Here's what's reasonable to discuss with your doctor:
A Practical Plan If You Have Neuropathy
Ask for a cardiovascular risk assessment
Lipids, glucose, ECG, blood pressure on standing and lying — go beyond the basic checkup.
Tighten control of underlying causes
Glucose, blood pressure, cholesterol — what protects nerves protects the heart.
Build a graded exercise routine
With CAN, perceived exertion is more reliable than heart rate targets. Go gradually.
Manage orthostatic symptoms
Rise slowly, hydrate, compression stockings, raise the head of the bed. Medications exist for severe cases.
Flag CAN before any surgery
Anesthesiologists need to know — perioperative cardiac risk is elevated with CAN.
A thorough cardiovascular risk assessment. This means more than a single blood pressure check. Cholesterol panel including LDL and HDL particle sizes when available, fasting glucose and HbA1c, ECG, possibly a stress test if you have risk factors, and an honest conversation about family history and lifestyle.
Tight control of underlying causes. If diabetes is driving your neuropathy, blood sugar control reduces the progression of both peripheral nerve damage and cardiac autonomic damage. The same is true for blood pressure and lipids. The interventions that protect your nerves protect your heart, and vice versa.
Smart exercise prescription. Exercise is one of the most important interventions for both neuropathy and cardiovascular health, but with CAN, a graded approach matters. Heart rate may not respond appropriately, so perceived exertion and pace become more reliable guides than target heart rate zones. Walking, swimming, and other low-impact aerobic activities are good choices, often best done with input from a physical therapist or exercise physiologist familiar with autonomic dysfunction.
Caution around anesthesia and surgery. If you ever face a surgical procedure, make sure your anesthesiologist knows about your neuropathy — and especially any signs of autonomic involvement. People with CAN are at higher risk of perioperative complications including blood pressure instability, arrhythmias, and silent cardiac events. Pre-operative cardiac evaluation is wise.
Managing orthostatic hypotension. If you get dizzy on standing, simple measures help: rising slowly, drinking adequate water, increasing salt intake (only with medical approval), wearing compression stockings, and elevating the head of the bed at night. Medications like midodrine and droxidopa exist for severe cases.
Living With Both — A Practical Mindset
I won't pretend learning that peripheral neuropathy may be a cardiovascular warning was an easy realization. There's grief in adding another layer to a chronic condition. But there's also empowerment.
13.5%
of adults over 40 have peripheral neuropathy
Each one is potentially carrying a quiet warning sign of cardiovascular disease. The same lifestyle changes — diet, movement, glycemic control — protect both nerves and heart.
The same lifestyle changes that protect your nerves protect your heart. Eating an anti-inflammatory diet high in vegetables, fish, nuts, and whole grains while reducing refined sugars and processed foods supports both. Moving your body daily — even gentle chair exercises if standing is hard — protects both. Sleeping well, managing stress, not smoking, moderating alcohol, maintaining a healthy weight — every one of these is a two-for-one investment.
The connection between neuropathy and heart disease isn't a reason to despair. It's a reason to take the whole-body view your symptoms have been quietly trying to tell you about all along. Your feet are not separate from your heart. They never were. And caring for one is, in the most literal sense, caring for the other.
Frequently Asked Questions
Can peripheral neuropathy cause heart problems?
Peripheral neuropathy itself does not directly cause heart disease, but the same underlying conditions that damage peripheral nerves — diabetes, vascular disease, inflammation — also damage cardiac autonomic nerves and the cardiovascular system. Cardiac autonomic neuropathy, a specific form of nerve damage affecting the heart, can cause arrhythmias, blood pressure instability, and increase the risk of silent heart attacks.
What is cardiac autonomic neuropathy?
Cardiac autonomic neuropathy is damage to the autonomic nerves that regulate heart rate, heart rhythm, and blood pressure. It is most common in diabetes but can occur with any condition that damages autonomic nerves. Signs include resting tachycardia, dizziness on standing, exercise intolerance, and reduced heart rate variability. It significantly raises the risk of cardiovascular events.
How is cardiac autonomic neuropathy diagnosed?
Diagnosis uses a battery of simple non-invasive tests including heart rate response to deep breathing, the Valsalva maneuver, heart rate response to standing, blood pressure response to standing, and 24-hour heart rate variability monitoring. These are sometimes called the Ewing tests. They are widely available and often covered by insurance when clinically indicated.
Does diabetic neuropathy increase heart attack risk?
Yes. Multiple studies show that diabetic peripheral neuropathy is an independent predictor of cardiovascular events, including heart attack. Cardiac autonomic neuropathy specifically is associated with two- to three-fold increases in cardiovascular mortality. The mechanism involves both shared underlying disease processes and direct damage to cardiac nerves.
Can heart medication cause neuropathy?
Yes, some cardiovascular medications can cause or contribute to peripheral neuropathy. Statin-induced neuropathy is the best-known example, although the relationship is debated. Amiodarone, used for arrhythmias, can also cause neuropathy. If neuropathy symptoms began shortly after starting a heart medication, it is worth discussing with your prescribing doctor.
What heart tests should someone with neuropathy ask about?
For someone with peripheral neuropathy, reasonable cardiovascular testing includes a standard ECG, heart rate variability testing, blood pressure measurement on standing and lying, and a comprehensive risk-factor assessment with lipid panel and HbA1c. If there are symptoms suggestive of autonomic dysfunction, more detailed autonomic testing is appropriate. A cardiologist consultation may be warranted in higher-risk cases.
Can lifestyle changes reverse cardiac autonomic neuropathy?
Early-stage cardiac autonomic neuropathy can be improved or stabilized with intensive lifestyle intervention, particularly in diabetes. Tight glycemic control, regular aerobic exercise, weight loss when appropriate, and blood pressure control have all been shown to improve heart rate variability and other measures of autonomic function. Advanced CAN is more difficult to reverse but can often be slowed.
Why does my heart rate feel high all the time with neuropathy?
A persistently elevated resting heart rate in someone with neuropathy may indicate cardiac autonomic neuropathy with loss of vagal parasympathetic tone. Without the normal parasympathetic brake, the sympathetic accelerator runs unopposed and resting heart rate climbs. This deserves medical evaluation, both to confirm the cause and to assess cardiovascular risk.


