
Peripheral Nerve Stimulation: An Emerging Treatment Option
When neuropathy medications stop providing enough relief — or when side effects make them hard to tolerate — many people feel stuck. You've tried gabapentin, maybe pregabalin, possibly duloxetine. You've explored natural remedies and TENS units. And yet the burning, tingling, and shooting pain persists. If this sounds familiar, peripheral nerve stimulation (PNS) may be worth learning about — it's a treatment that's been quietly gaining momentum as a powerful option for neuropathic pain that hasn't responded well to other approaches.
Unlike oral medications that affect your entire body, PNS targets specific nerves at the source of your pain. And unlike TENS units that stimulate through the skin surface, PNS places electrodes directly near or alongside the affected nerves — delivering more precise, more powerful relief. According to a 2024 narrative review in Pain and Therapy, PNS has shown “significant promise with minimal side effects” for various neuropathic pain conditions.
Browse all our treatments and therapies guides for more articles like this one.
What Is Peripheral Nerve Stimulation?
Peripheral nerve stimulation is a neuromodulation technique that uses mild electrical impulses to interrupt or modify pain signals traveling along damaged nerves. A thin electrode (sometimes called a “lead”) is placed near a specific peripheral nerve, and a small external or implanted device delivers precisely calibrated electrical pulses to that nerve.

of the global population lives with neuropathic pain — and less than half respond adequately to first-line medications
The concept isn't brand new — the first peripheral nerve stimulators were developed in the mid-1960s, according to the International Neuromodulation Society. But for decades, the technology was limited by bulky hardware, difficult surgical implantation, and a lack of randomized clinical trials. What's changed is the technology itself. Modern PNS systems are minimally invasive, often temporary, and backed by growing clinical evidence. Some of today's devices can be placed with just local anesthesia in an outpatient setting — no general surgery required.
How Does PNS Work to Reduce Pain?
To understand how PNS helps neuropathy pain, it helps to understand what's happening in your nervous system when you feel that burning, tingling, or shooting sensation.
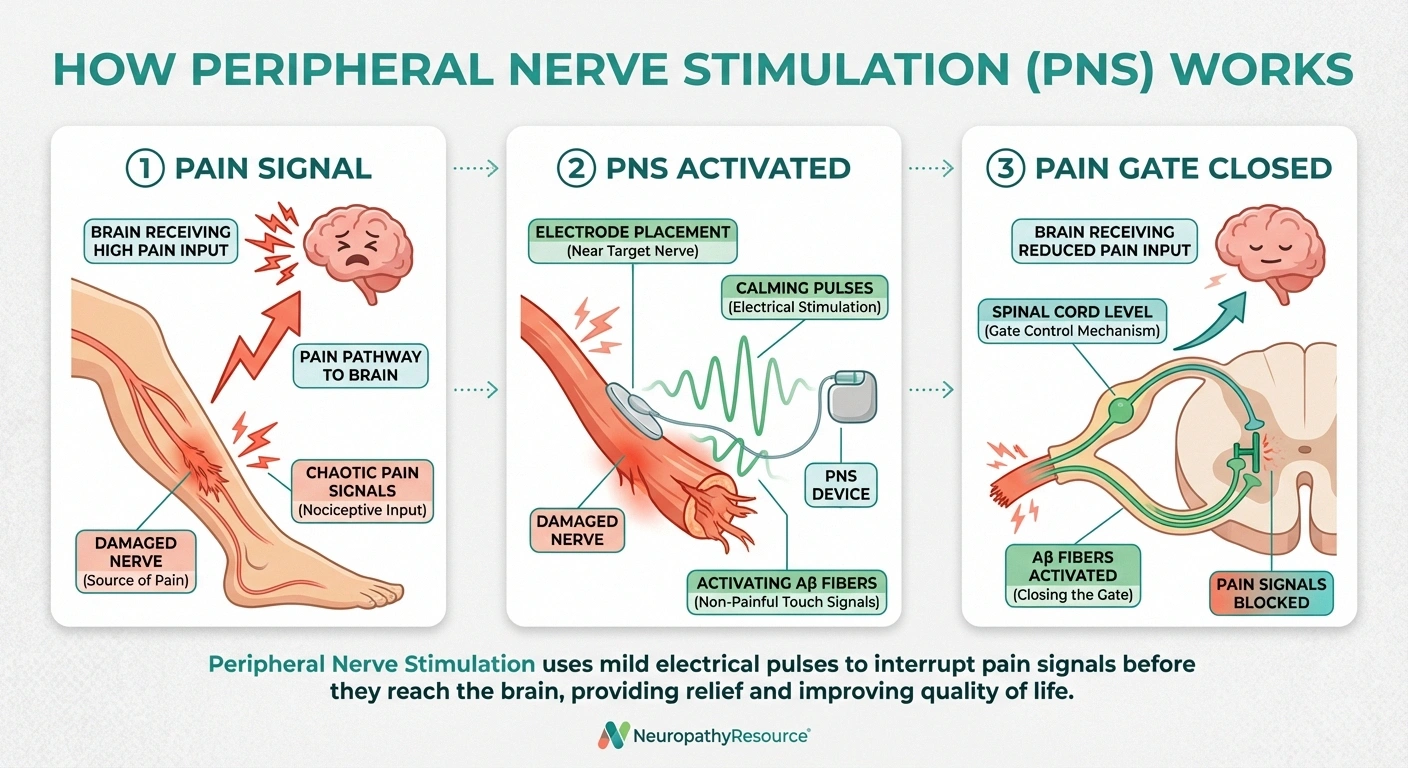
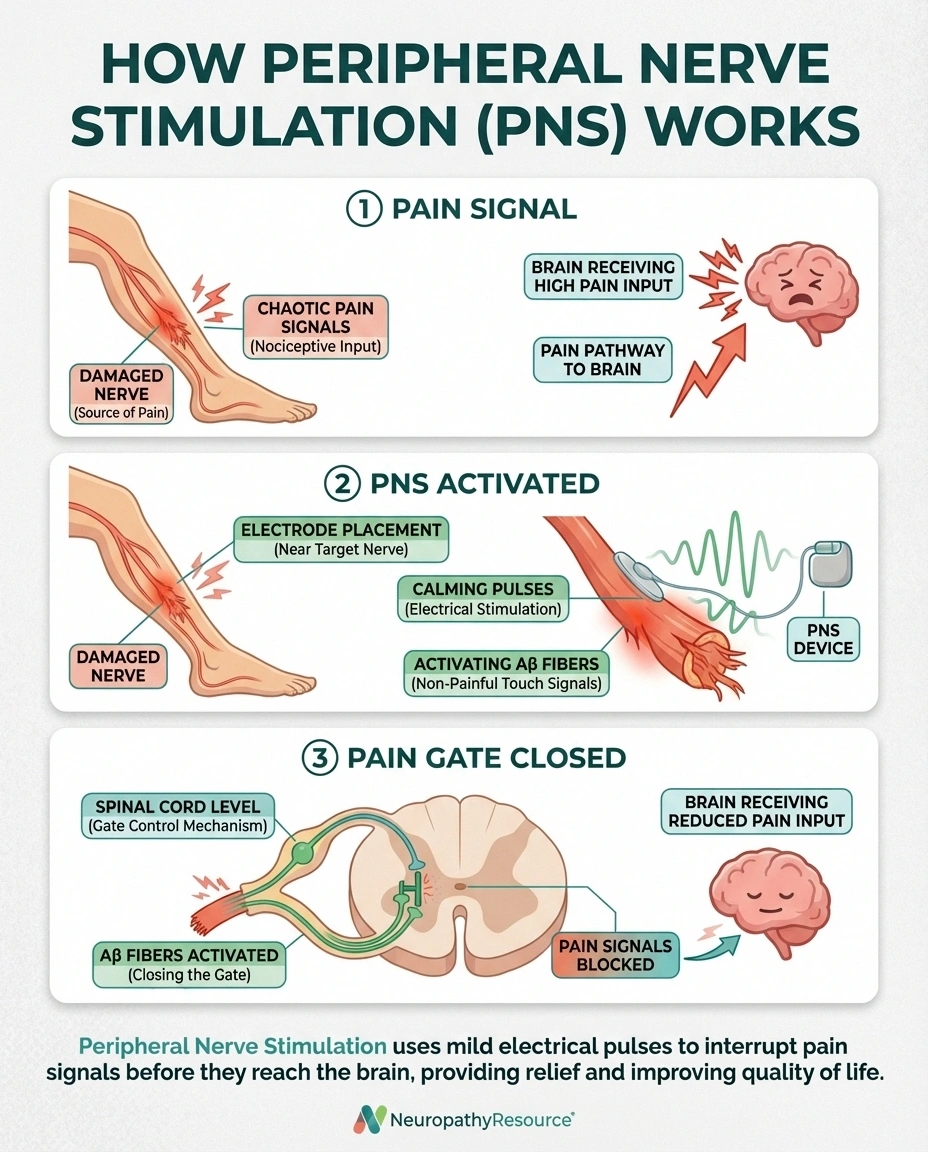
In neuropathy, damaged nerve fibers send abnormal electrical signals to your brain. These signals get interpreted as pain, even when nothing is actually causing physical harm. The pain is real — it's being generated by the nerves themselves — but the source is nerve dysfunction, not tissue damage.
PNS works through several mechanisms. The primary one is called the “gate control theory” of pain. When the PNS device sends mild electrical pulses to a nerve, it activates the large, non-pain-sensing nerve fibers (called Aβ fibers). These activated fibers essentially “close the gate” on pain signals from smaller nerve fibers, blocking or reducing the pain messages that reach your brain.
But that's not all PNS does. Research suggests that peripheral nerve stimulation also modulates neurotransmitter levels in the spinal cord and brain, changes how the brain processes pain signals over time, may promote nerve healing through improved blood flow to stimulated areas, and can reduce local inflammation around damaged nerves. Some emerging data even suggests that PNS may create lasting changes in how your nervous system processes pain, meaning that benefits can continue even after the stimulation device is removed.
PNS vs. TENS: What's the Difference?
If you've tried a TENS unit (transcutaneous electrical nerve stimulation), you might wonder how PNS is different. While both use electrical stimulation for pain relief, they work in fundamentally different ways:
📋 TENS Units
✓ Non-invasive, over-the-counter
✓ Self-applied at home
✗ Stimulates through skin surface
✗ Signal diffuses through tissue
✗ Effects typically temporary
⚡ Peripheral Nerve Stimulation
✓ Electrode placed directly at nerve
✓ Precise, calibrated stimulation
✓ Effects can last months to years
✗ Requires medical procedure
✗ Prescription/specialist only
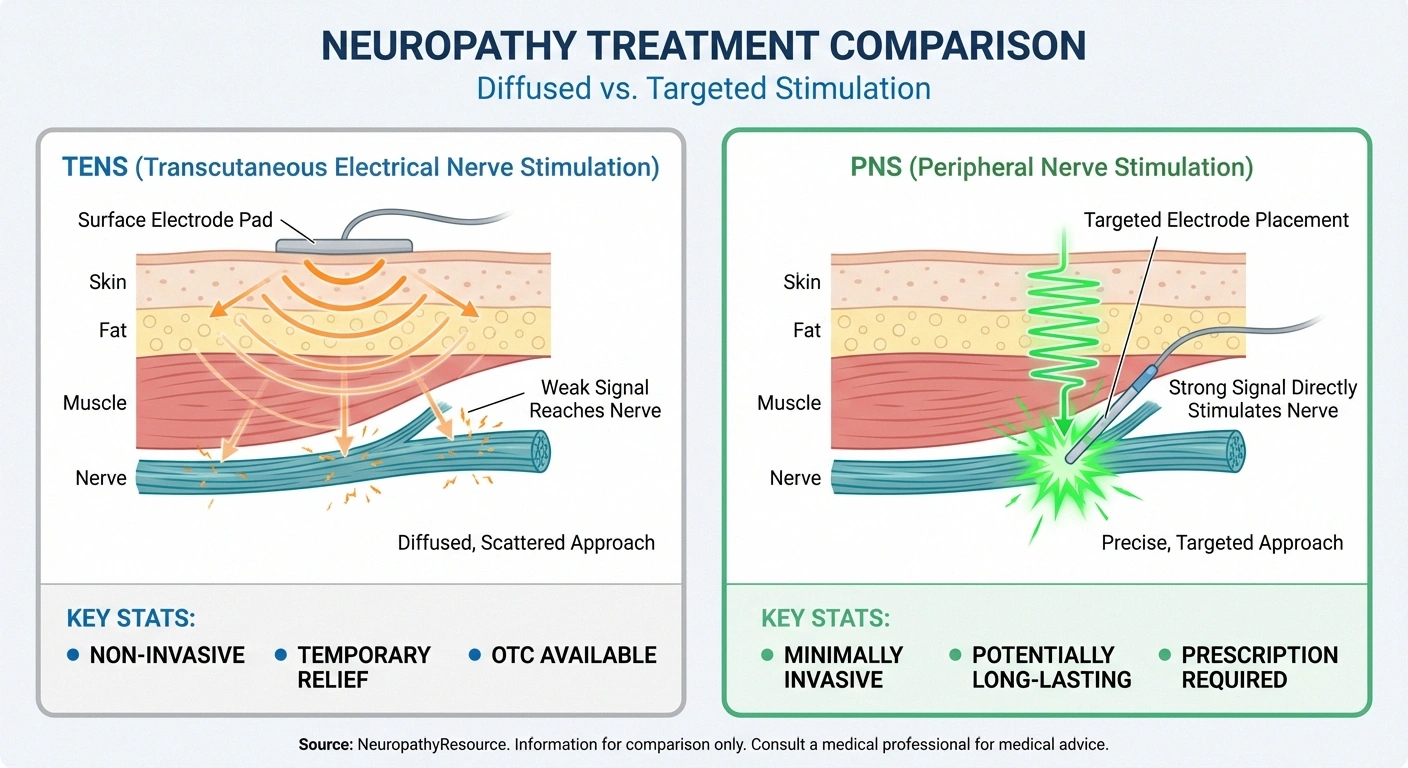
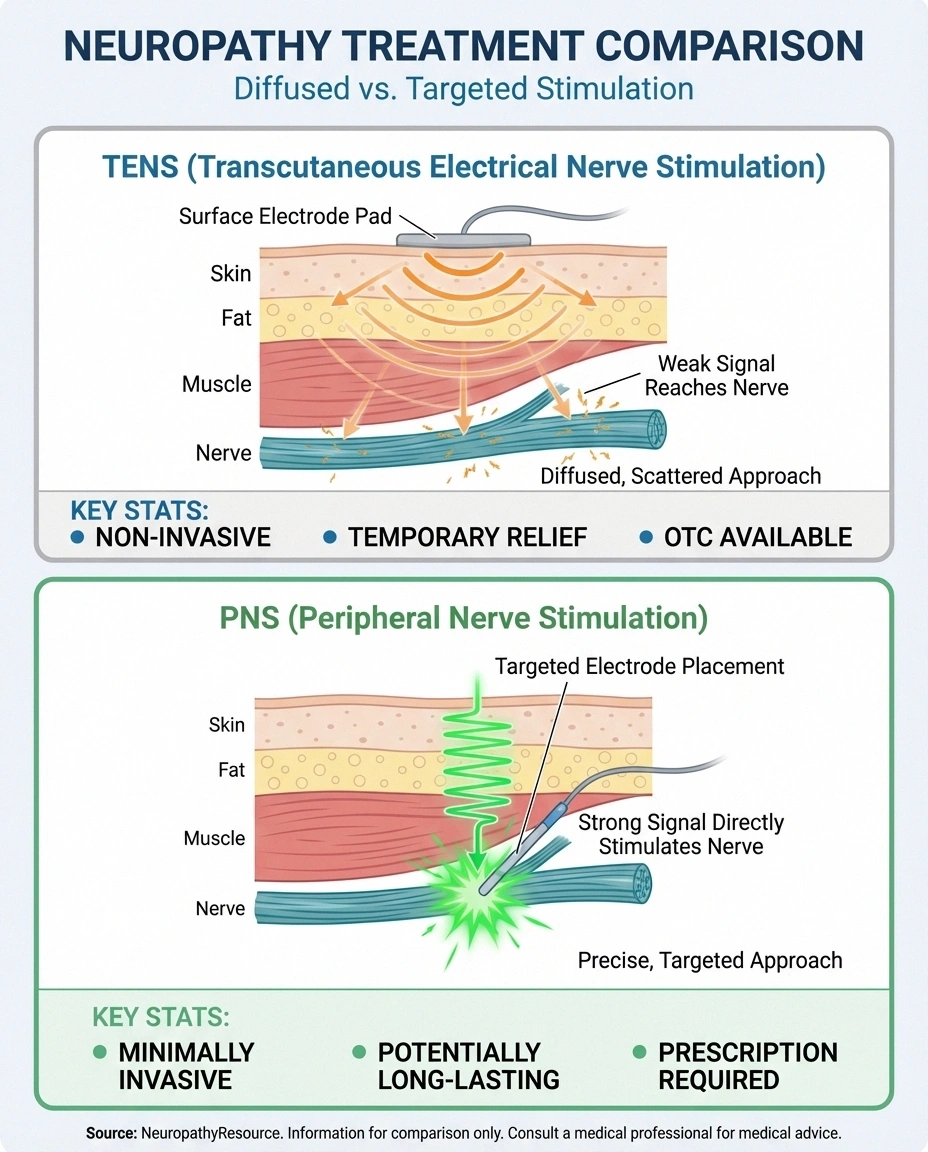
TENS sends electrical signals through the skin surface using sticky pad electrodes. The current has to pass through skin, fat, and muscle tissue to reach nerves, which means it's diffused and less targeted. TENS is non-invasive and widely available over the counter, making it an accessible first-line option. But its effects tend to be temporary — most people need to use TENS regularly to maintain relief, and it may not penetrate deeply enough to affect the nerves most responsible for neuropathic pain.
PNS places electrodes directly adjacent to the target nerve, delivering stimulation with much greater precision and intensity. Because the electrical current doesn't have to travel through layers of tissue, it can be calibrated more precisely for each patient. PNS requires a medical procedure for placement, but it offers more potent and often longer-lasting relief. Some patients experience pain reduction that persists for months or even years after a temporary PNS device is removed.
Think of it this way: TENS is like shouting through a closed window hoping the person inside can hear you. PNS is like speaking directly into their ear. Both can communicate the message, but one is significantly more effective for complex or severe pain.
PNS vs. Spinal Cord Stimulation: Understanding the Options
Spinal cord stimulation (SCS) is another neuromodulation technique that some neuropathy patients may encounter. While both PNS and SCS use electrical stimulation to manage pain, there are important differences.
SCS places electrodes in the epidural space near the spinal cord, modulating pain signals at a central level. It can cover large body areas and has been used for decades for conditions like failed back surgery syndrome and complex regional pain syndrome. However, SCS is a more invasive procedure, carries higher infection risks, and requires electrode placement near the spinal cord.
PNS offers several advantages over SCS according to the medical literature: lower infection rates due to less invasive placement, the ability to target specific nerves rather than broad spinal cord regions, easier trial periods with temporary devices, reversibility — many PNS systems can be removed without lasting effects, and lower overall complication rates.
For people with neuropathic pain that follows a specific nerve distribution — like pain isolated to one foot, one hand, or a specific nerve pathway — PNS may offer more targeted relief than SCS. Your pain management specialist can help determine which approach best fits your specific situation.
What Conditions Can PNS Treat?
PNS has been studied and used for a growing list of neuropathic pain conditions. According to StatPearls, current indications include:
Diabetic peripheral neuropathy. One of the most promising applications. Patients with diabetic neuropathy who haven't found adequate relief from medications may benefit from PNS targeting the tibial, peroneal, or sural nerves in the legs.
Post-surgical neuropathy. Nerve damage from surgery — including post-operative neuropathy — can be targeted with PNS when the specific injured nerve can be identified.
Trigeminal neuralgia. PNS has shown effectiveness for trigeminal neuralgia, targeting the specific branches of the trigeminal nerve causing facial pain.
Post-herpetic neuralgia. The nerve pain that persists after shingles can be treated with PNS, particularly when it follows a specific nerve pathway.
Complex regional pain syndrome (CRPS). PNS is increasingly used for CRPS, particularly when the pain is localized to a specific limb or region.
Ulnar, median, and radial neuropathy. Pain and dysfunction from ulnar neuropathy or neuropathy in the hands can be targeted with PNS near the affected nerve.
Occipital neuralgia. Severe headache pain from occipital nerve irritation responds well to PNS in many patients.
Phantom limb pain. Research has shown that PNS can even help with phantom limb sensations after amputation, with some participants able to perceive tactile feedback through stimulation.
What to Expect During a PNS Procedure
If you and your doctor decide that PNS is worth trying, here's what the process typically looks like:

The PNS Journey: 3 Stages
Evaluation
Detailed pain history, diagnostic nerve testing (EMG/NCS), review of previous treatments. Your specialist identifies the target nerve(s).
Trial Period (5–60 days)
Temporary lead placed under local anesthesia with ultrasound guidance. Outpatient, 30–60 minutes. You test the device with a handheld remote to fine-tune settings.
Decision: Continue or Remove
If trial works: continue with lasting relief after removal, or upgrade to permanent implant. If not: lead is simply removed — no lasting harm — and you explore other options.
The Evaluation
Before any device placement, your pain management specialist or peripheral nerve surgeon will conduct a thorough evaluation. This usually includes a detailed history of your pain — when it started, where exactly you feel it, what makes it better or worse. You may undergo diagnostic testing like an EMG or nerve conduction study to pinpoint which nerves are involved. Your doctor will also review what treatments you've already tried, as PNS is typically recommended after other approaches haven't provided adequate relief.
The Trial Period
One of the great advantages of modern PNS is the ability to do a trial first. A temporary lead is placed near the target nerve using ultrasound or X-ray guidance, usually under local anesthesia. According to Duke Health, the lead can be as thin as a sewing thread or spaghetti noodle. The procedure is typically done in an outpatient setting and takes about thirty to sixty minutes.
During the trial (which usually lasts five to sixty days depending on the device), you'll wear a small external transmitter and battery. You can use a handheld remote to adjust the stimulation settings — finding the right frequency and intensity for your pain. This trial period lets you experience PNS before committing to a longer-term solution.
Permanent or Extended Placement
If the trial provides meaningful pain relief, you and your doctor may decide to move to a longer-term PNS system. Some patients find that the temporary device provides lasting relief that continues even after removal — sometimes for months or years. Others benefit from a fully implanted system like the Bioventus StimRouter, which is placed under the skin and intended for long-term use.
The implantation procedure is more involved than the trial but still typically performed under local or light sedation in an outpatient setting. Recovery is usually brief, with most patients returning to normal activities within a few days.
Current PNS Devices and Systems
Several PNS systems are currently available, each with different strengths. While the field is evolving rapidly, here are the main categories:
Temporary percutaneous systems (like SPRINT). These are designed for short-term use — typically sixty days. A thin lead is placed through the skin near the target nerve, connected to a small wearable transmitter. After the treatment period, the lead is simply removed in a clinic visit. The SPRINT system has shown pain relief lasting up to two years or more after the sixty-day treatment period in some patients. The main limitation is that the device can't be submerged in water during the treatment period.
Permanent implantable systems (like StimRouter). These are fully implanted under the skin for long-term use. They can be submerged, don't need to be removed after a set period, and provide ongoing stimulation as needed. An external transmitter and battery power the device wirelessly. These are ideal for patients who need continuous or long-term stimulation.
Ultrasound-guided open-coil systems. Newer devices use open-coil lead designs that can be placed under ultrasound guidance alone (without fluoroscopy or X-ray), making the procedure simpler and more accessible. These systems are part of the growing trend toward less invasive, office-based PNS placement.
Does PNS Actually Work? What the Research Shows
The evidence for PNS has grown substantially in recent years, though researchers acknowledge that more large-scale randomized controlled trials are still needed. Here's what the current evidence tells us:
Research Says
A multicenter randomized controlled trial found that percutaneous PNS significantly reduced chronic neuropathic pain vs. placebo, with benefits persisting beyond the stimulation period. Multiple studies report pain reduction of 50% or more in a significant proportion of patients. Side effects are minimal — mostly insertion-site discomfort and occasional lead migration.
A multicenter randomized controlled trial published in Regional Anesthesia and Pain Medicine found that percutaneous PNS significantly reduced chronic neuropathic pain compared to placebo stimulation, with benefits persisting well beyond the stimulation period. Multiple studies have shown pain reduction of fifty percent or more in a significant proportion of patients. The 2024 narrative review in Pain and Therapy concluded that PNS is “a promising treatment modality” warranting additional high-quality trials, while noting its demonstrated effectiveness across multiple neuropathic pain conditions.
Side effects tend to be minimal. The most common complications include discomfort at the insertion site, lead migration (the electrode shifting from its ideal position), and occasional skin irritation near the external transmitter. Serious complications like infection are rare but possible, as with any procedure that breaks the skin.
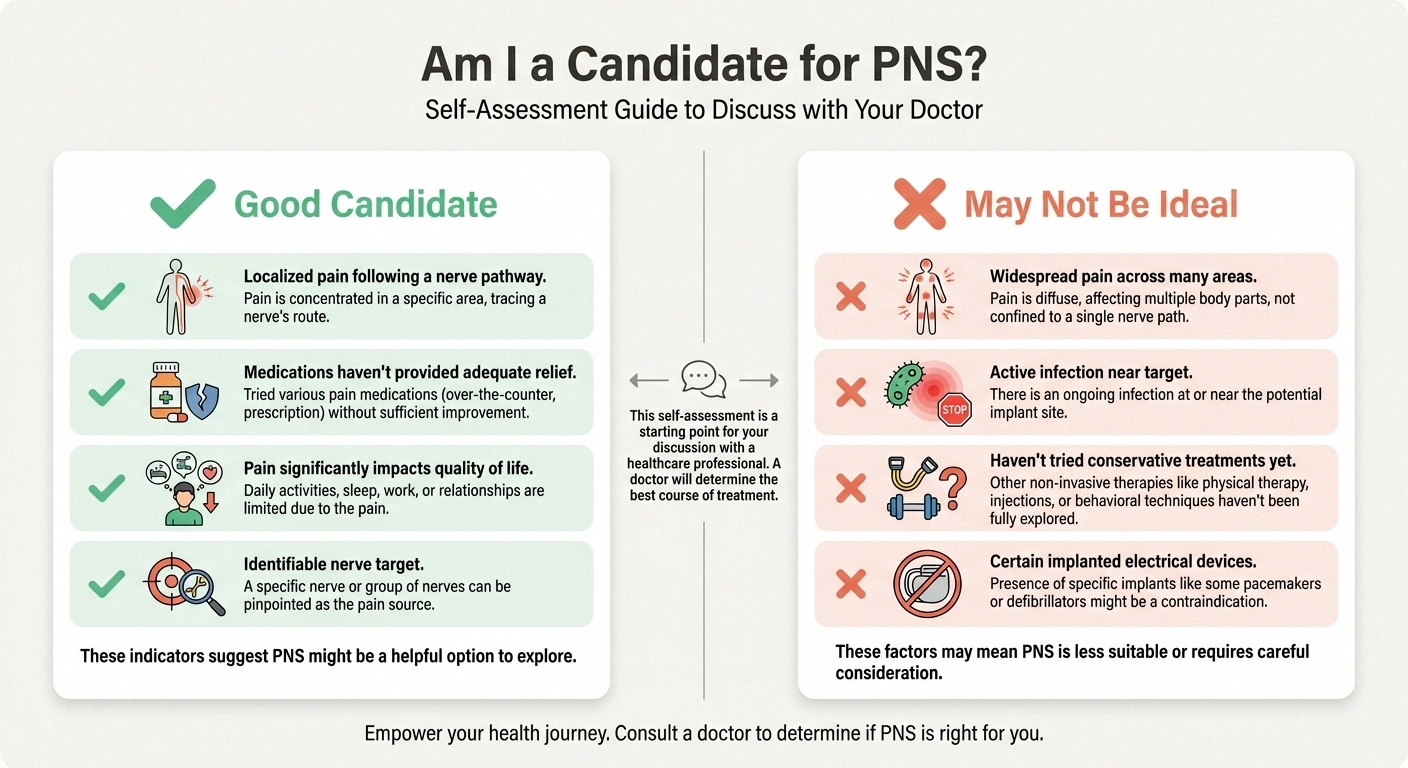
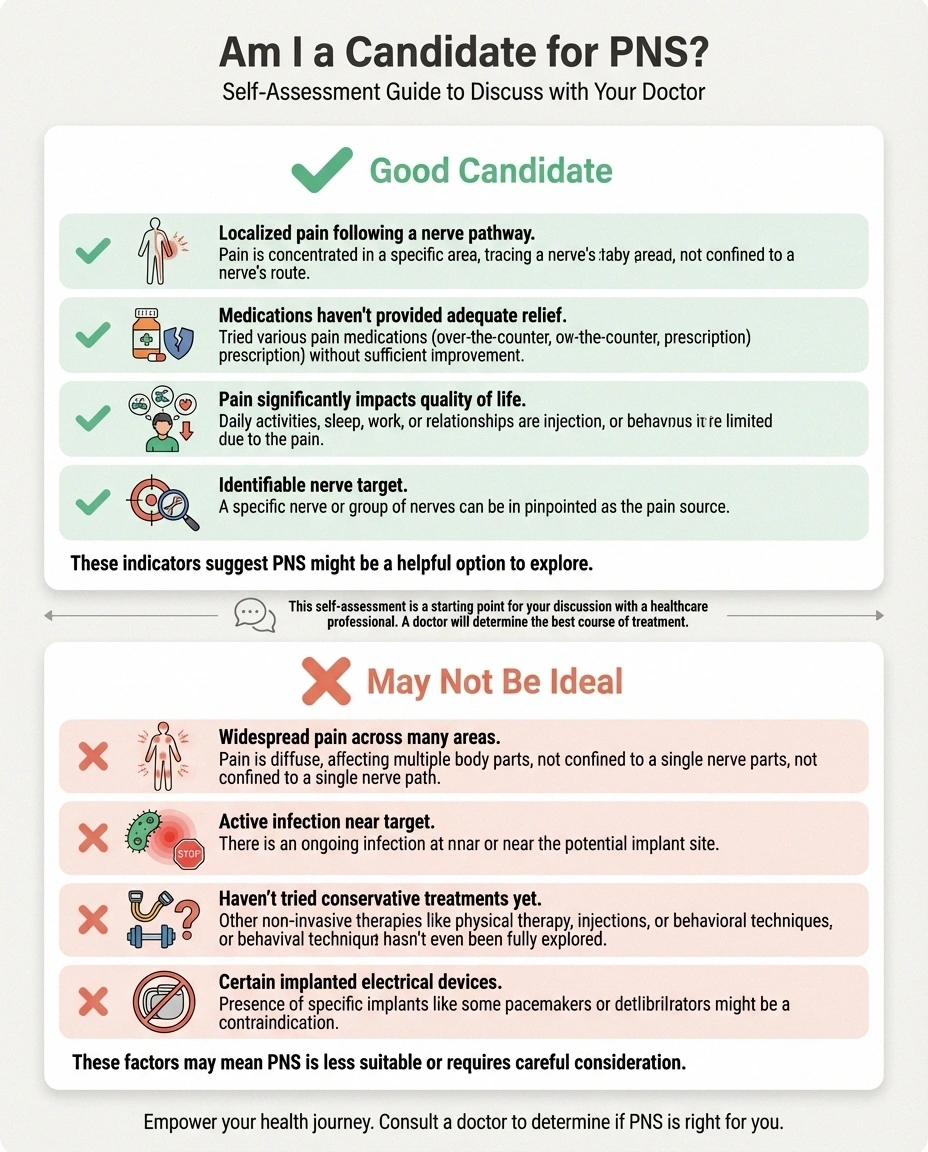
Is PNS Right for You?
According to Dr. Neill Li, a peripheral nerve surgeon at Duke Health, PNS is ideal for “any type of chronic pain that is isolated and has an identifiable nerve target.” You may be a good candidate for PNS if:
Talk to Your Doctor
PNS is a medical procedure that requires specialist evaluation. Don't pursue PNS without first trying more conservative treatments (medications, physical therapy, lifestyle changes). Always discuss with a pain management specialist or peripheral nerve surgeon who can properly assess whether PNS is appropriate for your specific condition.
Your neuropathic pain is localized to a specific area or follows a known nerve pathway. You've tried medications like gabapentin, pregabalin, or duloxetine without adequate relief, or you can't tolerate their side effects. Your pain significantly impacts your quality of life, sleep, mobility, or mental health. Your doctor can identify the specific nerve or nerves causing your pain. You're willing to undergo a minimally invasive procedure.
PNS may not be the best option if your pain is widespread and affects many areas simultaneously (like generalized small fiber neuropathy throughout both legs and feet), if you have a bleeding disorder or active infection near the target area, if you have a pacemaker or other implanted electrical device (though some newer PNS systems may be compatible), or if you haven't yet tried more conservative treatments.
How to Talk to Your Doctor About PNS
If you're interested in exploring PNS, here's how to have a productive conversation with your healthcare provider:

Come prepared. Bring a list of every treatment you've tried for your neuropathy, including medications, dosages, and why you stopped them (didn't work, side effects, etc.). This helps your doctor see that you've exhausted other options. Our guide on how to talk to your doctor about neuropathy has additional tips for productive appointments.
Describe your pain precisely. PNS works best for localized pain with an identifiable nerve target. Be specific about where you feel pain — “my left foot, especially along the outside edge and the bottom three toes” is much more helpful than “my feet hurt.” Note when the pain is worst and what triggers flare-ups.
Ask the right questions. Am I a candidate for peripheral nerve stimulation? Would a trial period be appropriate before committing to an implant? Which nerves do you think are causing my pain, and could PNS target them? What are the realistic expectations for pain reduction — not elimination, but improvement? What happens if the trial doesn't work? What's the recovery time? Will insurance cover the procedure?
Get the right referral. Not every pain doctor offers PNS. You may need a referral to a pain management specialist, peripheral nerve surgeon, or neuromodulation center. Academic medical centers and university hospitals are often at the forefront of PNS technology.
Cost and Insurance Coverage
Cost is understandably a concern for many patients considering PNS. Here's what you should know:
Many insurance plans now cover PNS for approved indications, particularly when you've documented that other treatments have failed. Medicare covers PNS for certain conditions, though coverage policies can vary by region. Prior authorization is almost always required, and your doctor's office typically handles this process. Out-of-pocket costs vary widely — the trial period is generally less expensive than permanent implantation, and some device manufacturers offer patient assistance programs.
The best first step is to ask your pain specialist's office about insurance verification before scheduling any procedures. They can submit a pre-authorization request and give you a clearer picture of your potential costs.
Combining PNS With Other Neuropathy Treatments
PNS doesn't have to be an either-or choice. Many patients use PNS alongside other treatments for comprehensive pain management:
Key Takeaway
PNS works best as part of a comprehensive pain management plan — not a standalone solution. Many patients combine PNS with reduced medication dosages, physical therapy, exercise, and topical treatments for the best overall results. The goal is enough pain reduction to improve function, sleep, and quality of life.
PT for nerve pain combined with PNS can improve mobility and strength while the stimulator manages pain. Some patients continue taking reduced doses of neuropathy medications, using PNS to bridge the gap to adequate relief. Topical treatments like capsaicin cream can complement PNS for surface-level nerve pain. Exercise programs may be easier to maintain when PNS reduces the pain that previously limited activity.
The goal of integrating PNS into your treatment plan isn't necessarily to replace everything else — it's to improve your overall pain management enough that you can function better, sleep better, and live more fully.
The Future of Peripheral Nerve Stimulation
PNS technology is evolving rapidly. Several developments are on the horizon that could make this treatment even more accessible and effective:
Wireless and miniaturized devices. Next-generation PNS systems are becoming smaller, wireless, and battery-free — powered by external radiofrequency transmitters. This could eliminate the need for implanted batteries and reduce device-related complications.
Closed-loop stimulation. Current PNS devices deliver constant stimulation at preset parameters. Future systems may use sensors to detect nerve activity in real time and adjust stimulation automatically — responding to your pain as it happens, like a thermostat that adjusts when the temperature changes.
Broader clinical evidence. More randomized controlled trials are underway for specific conditions like diabetic neuropathy, chemotherapy-induced neuropathy, and idiopathic neuropathy. As this evidence base grows, insurance coverage and clinical guidelines are likely to expand.
More accessible placement. As ultrasound-guided techniques improve, PNS placement may become available in more clinics and practices, reducing the need to travel to specialized academic centers.
Frequently Asked Questions
Does PNS hurt when it's turned on?
Modern PNS devices use high-frequency stimulation that most patients cannot feel at all. Unlike older devices that produced a noticeable tingling sensation, current technology works below the sensory threshold. You may feel mild tingling during initial calibration, but during normal use, the stimulation should be imperceptible while still providing pain relief.
Can I go through airport security with a PNS device?
Temporary PNS systems (like SPRINT) include a small external component that should be visible to security. You'll receive a patient identification card from the manufacturer. Let security personnel know about your device before going through screening. For permanent implants, the device is MRI-conditional in many cases, but always check with your doctor before any imaging procedures.
How long do the batteries last in a PNS device?
For temporary systems, the external battery is rechargeable and lasts throughout the treatment period (typically sixty days). For permanent implants like the StimRouter, the external transmitter uses replaceable batteries that typically last several weeks per set. The implanted components themselves don't contain batteries — they're powered wirelessly by the external transmitter.
Can PNS help with neuropathy in both feet?
PNS can potentially be used bilaterally (on both sides), but this requires separate electrode placements for each target nerve. Whether bilateral treatment is appropriate depends on your specific condition, the nerves involved, and your pain specialist's assessment. Some patients start with one side and add the other later if the initial trial is successful.
What happens if PNS doesn't work for me?
If the trial period doesn't provide meaningful relief, the temporary lead is simply removed and you can explore other options. There's no lasting harm from an unsuccessful trial. Your doctor may recommend alternative approaches like spinal cord stimulation, different medication combinations, or other interventional techniques. The trial-first approach is one of PNS's key advantages — you don't have to commit to a permanent device without knowing whether it will help.
Is PNS the same as a “nerve block”?
No, they're quite different. A nerve block uses injected medication (typically a local anesthetic, sometimes with a steroid) to temporarily numb a nerve. The relief from a nerve block usually lasts hours to weeks. PNS uses electrical stimulation rather than medication, and its effects can last much longer — potentially months or years. However, nerve blocks can be useful diagnostically — if a nerve block at a specific location relieves your pain, it helps confirm which nerve should be targeted with PNS.
Taking the Next Step
Peripheral nerve stimulation isn't a miracle cure, and it's not right for everyone. But for people living with chronic neuropathic pain that hasn't responded adequately to medications and other treatments, it represents a genuine option worth exploring — one backed by growing evidence and improving technology.
The field is moving fast. Devices are getting smaller, procedures are becoming less invasive, and the evidence base is expanding. If you've been told to “just learn to live with” your neuropathy pain, PNS may be worth a conversation with your pain management doctor.
Start by understanding your options, asking informed questions, and finding a specialist who has experience with modern PNS technology. Your nerves may not be able to heal themselves, but with the right tools, their pain signals can be managed — and your quality of life can improve significantly.


