
Browse all our types and causes of neuropathy guides for more articles like this one.
Pregnancy changes your body in ways no one fully prepares you for — the swollen feet, the back pain, the exhaustion. But when my reader Sarah wrote to me about the numbness and tingling that started in her hands during her third trimester, she was frightened. Her OB reassured her it was “probably carpal tunnel,” but Sarah wanted to understand what was happening to her nerves and whether it would affect her baby. If you're pregnant and experiencing strange nerve symptoms, this guide is for you.
Peripheral neuropathies during pregnancy are more common than most women realize. While they're rarely dangerous to mother or baby, they can be deeply uncomfortable and anxiety-inducing — especially when you're already navigating the physical demands of growing a new life. Let's talk about what causes nerve problems during pregnancy, which types are most common, and what you can do about them.
Why Pregnancy Affects Your Nerves
Your body undergoes profound changes during pregnancy, and several of these can directly affect nerve function. Understanding these mechanisms helps explain why nerve symptoms develop and — importantly — why most resolve after delivery.
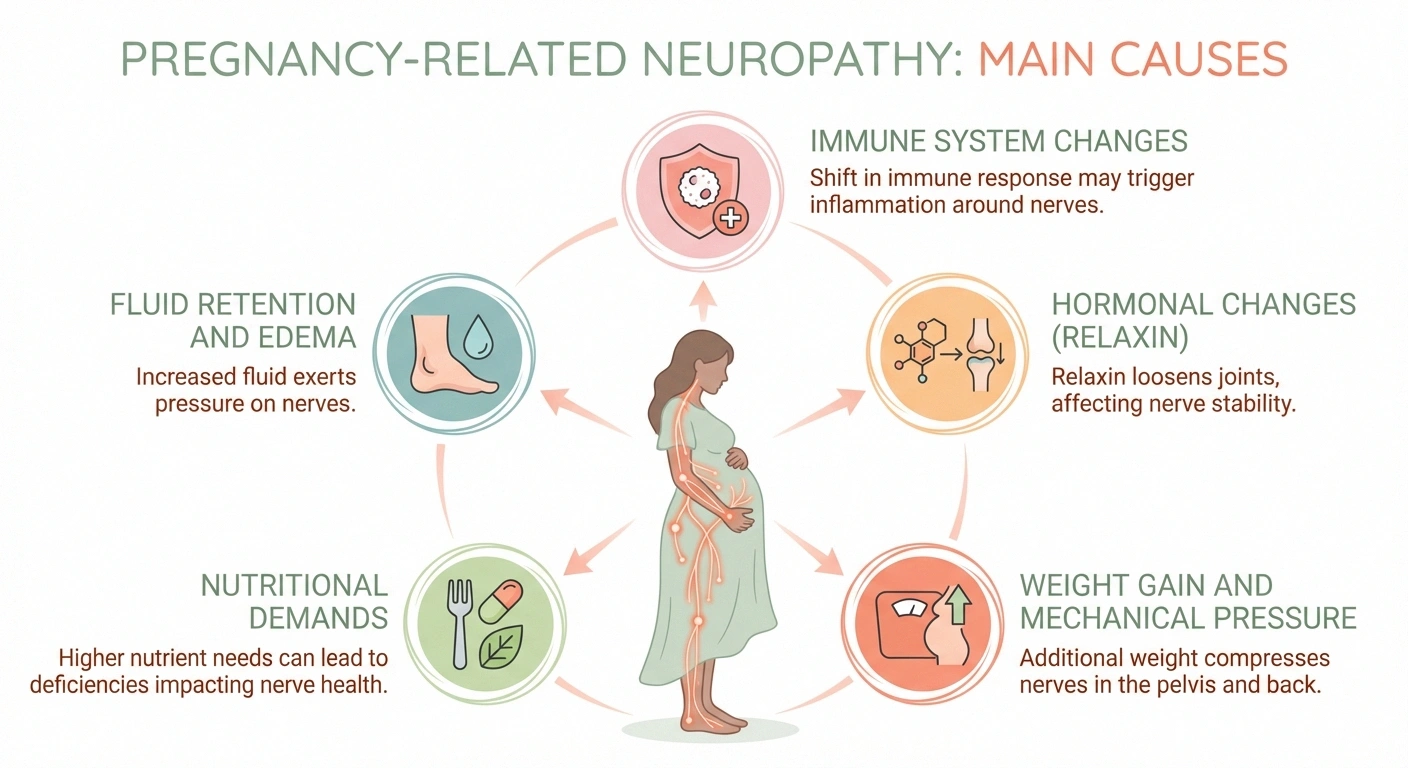
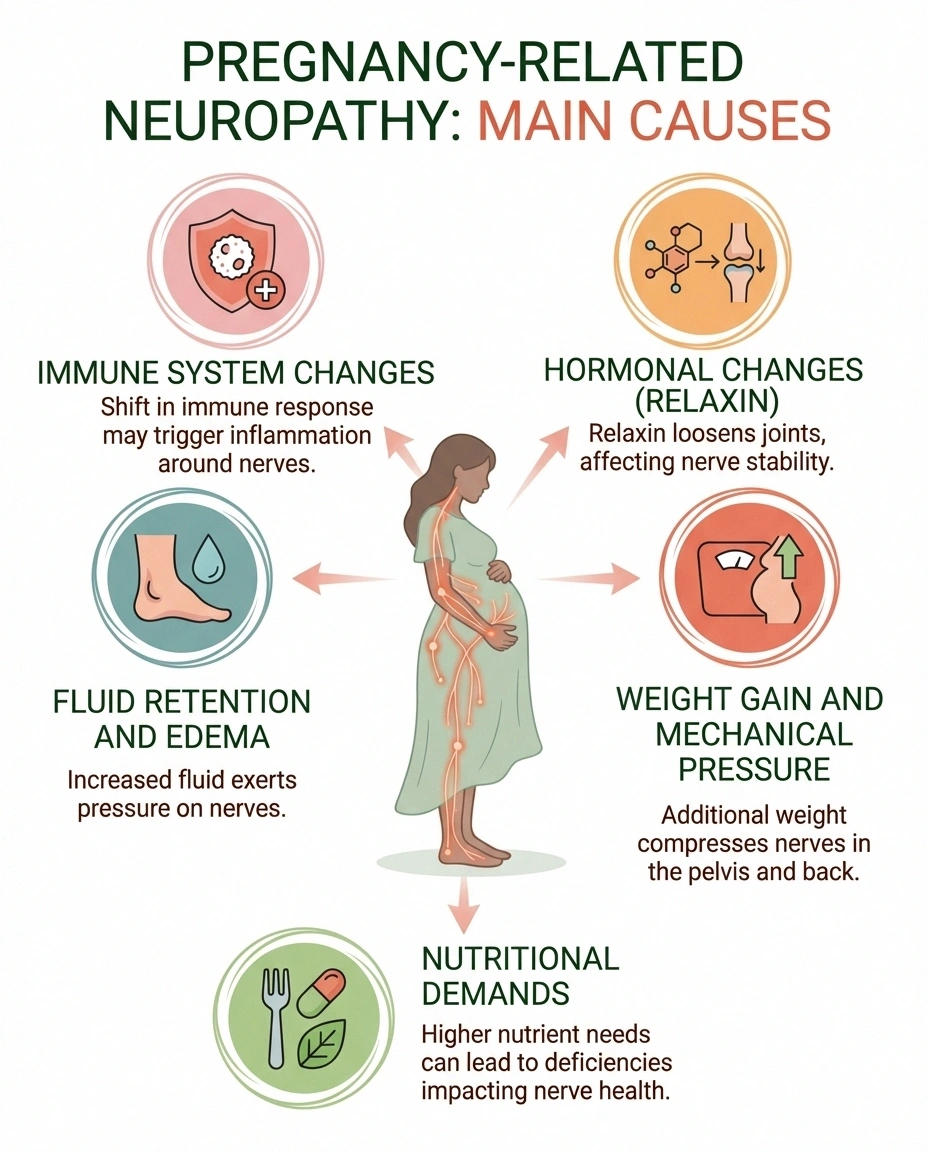
Fluid retention and edema. During pregnancy, your blood volume increases by roughly forty to fifty percent. This extra fluid can cause tissue swelling throughout your body, and when that swelling occurs in tight anatomical spaces — like the carpal tunnel in your wrist or the tarsal tunnel in your ankle — nearby nerves get compressed. This is the single most common cause of pregnancy-related neuropathy.
Hormonal changes. Pregnancy hormones, particularly relaxin, loosen ligaments and connective tissue to prepare your body for delivery. But these same changes can alter the structure of the spaces where nerves travel, potentially creating compression. Hormonal shifts also affect how your body processes fluids, contributing to the edema mentioned above.
Weight gain and mechanical pressure. As your uterus grows, it can press directly on nerves in your pelvis and lower back. The additional weight you carry changes your center of gravity and posture, which can stretch or compress nerves — particularly in the lumbar spine and lower extremities.
Nutritional demands. Growing a baby requires enormous nutritional resources. Vitamin deficiencies — especially B12, folate, and iron — can develop or worsen during pregnancy, and these deficiencies are known to affect nerve function. According to a comprehensive review in Continuum: Lifelong Learning in Neurology, clinicians should always consider nutritional causes when evaluating neuropathy in pregnancy.
Immune system changes. Pregnancy modulates your immune system in complex ways, and these shifts can occasionally trigger inflammatory responses that affect nerves — a factor in conditions like Bell's palsy and Guillain-Barré syndrome, which occur more frequently during pregnancy and the postpartum period.
Carpal Tunnel Syndrome: The Most Common Culprit
If there's one pregnancy neuropathy that stands above the rest in terms of frequency, it's carpal tunnel syndrome (CTS). Estimates of pregnancy-related CTS vary widely — from about one percent to as high as sixty percent of pregnant women — depending on how studies define and diagnose the condition. The most reliable figure, based on prospective studies using electrodiagnostic confirmation, is approximately seventeen percent.
What it feels like: Achy wrist and hand pain, tingling or numbness in the thumb, index, and middle fingers (the median nerve distribution), symptoms that are worse at night, and a feeling of stiffness or clumsiness in the hands. Many women describe waking up at night and needing to “shake out” their hands to relieve the symptoms.
When it starts: Most pregnancy-related CTS develops in the third trimester, when fluid retention peaks. However, some women develop symptoms earlier, particularly with twins or when significant weight gain occurs early.
The good news: Pregnancy-related CTS is typically milder than non-pregnancy CTS and usually resolves after delivery. According to a three-year longitudinal study published in Muscle & Nerve, approximately fifty percent of patients improved within one year, and sixty to seventy percent improved within three years.
The caveat: That same study challenged the previous belief that seventy-five percent of cases resolve within the first month postpartum. Among women not treated surgically, fifty percent still had some symptoms at three years. Women with earlier symptom onset and greater pregnancy-related weight gain were more likely to have persistent symptoms.
Managing it during pregnancy:
- Wrist splints — Wearing neutral-position wrist splints, especially at night, is the first-line recommendation. They prevent the wrist from flexing during sleep, which compresses the median nerve.
- Activity modification — Avoid repetitive hand and wrist movements when possible. Take frequent breaks from typing, cooking, and other hand-intensive tasks.
- Elevation and ice — Elevating your hands and applying cold packs may reduce swelling in the carpal tunnel.
- Corticosteroid injection — If symptoms are severe and don't respond to conservative measures, a steroid injection into the carpal tunnel can provide relief. This is generally considered safe during pregnancy when the benefit outweighs the risk.
Surgery for carpal tunnel syndrome can almost always wait until after delivery. The exception is if you develop actual muscle weakness in the thumb — a sign of significant nerve damage that may warrant earlier intervention.
Bell's Palsy During Pregnancy
Bell's palsy — sudden weakness or paralysis on one side of the face — is two to four times more common during the third trimester and early postpartum period compared to non-pregnant women of the same age. While frightening, it's important to know that most cases resolve well.

Recognizing Bell's palsy: Sudden onset of one-sided facial weakness that affects both the upper and lower face (including the forehead and eyelid), difficulty closing the eye on the affected side, reduced blinking, drooping of the mouth, possible pain behind the ear, and sometimes changes in taste. If only the lower face is affected and the forehead can still move normally, this may indicate a stroke rather than Bell's palsy — which requires emergency evaluation.
Treatment in pregnancy: In non-pregnant patients, a short course of corticosteroids (like prednisone) is standard treatment and has been shown to improve outcomes. During pregnancy, the use of steroids is less well-studied, and the decision should be made with your obstetric team, weighing the potential benefits against risks. Eye care — using artificial tears and taping the eye closed at night — is essential to protect the cornea when the eye can't close completely.
Prognosis: Most women with pregnancy-related Bell's palsy recover fully, though it may take several months. The overall prognosis is similar to Bell's palsy in the general population, where about seventy percent of patients achieve complete recovery.
Lower Extremity Neuropathies: When Your Legs Are Affected
Several distinct nerve problems can affect your legs during pregnancy and delivery:
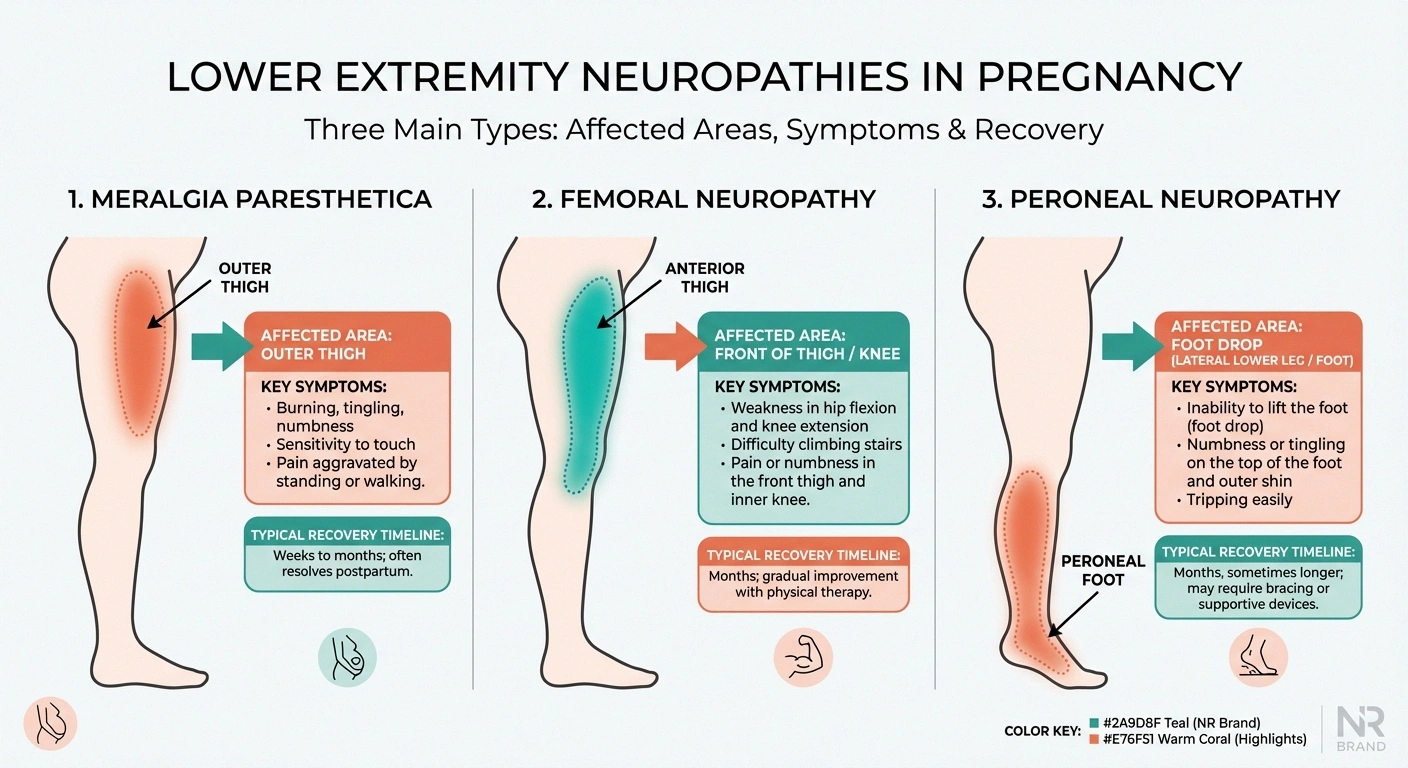
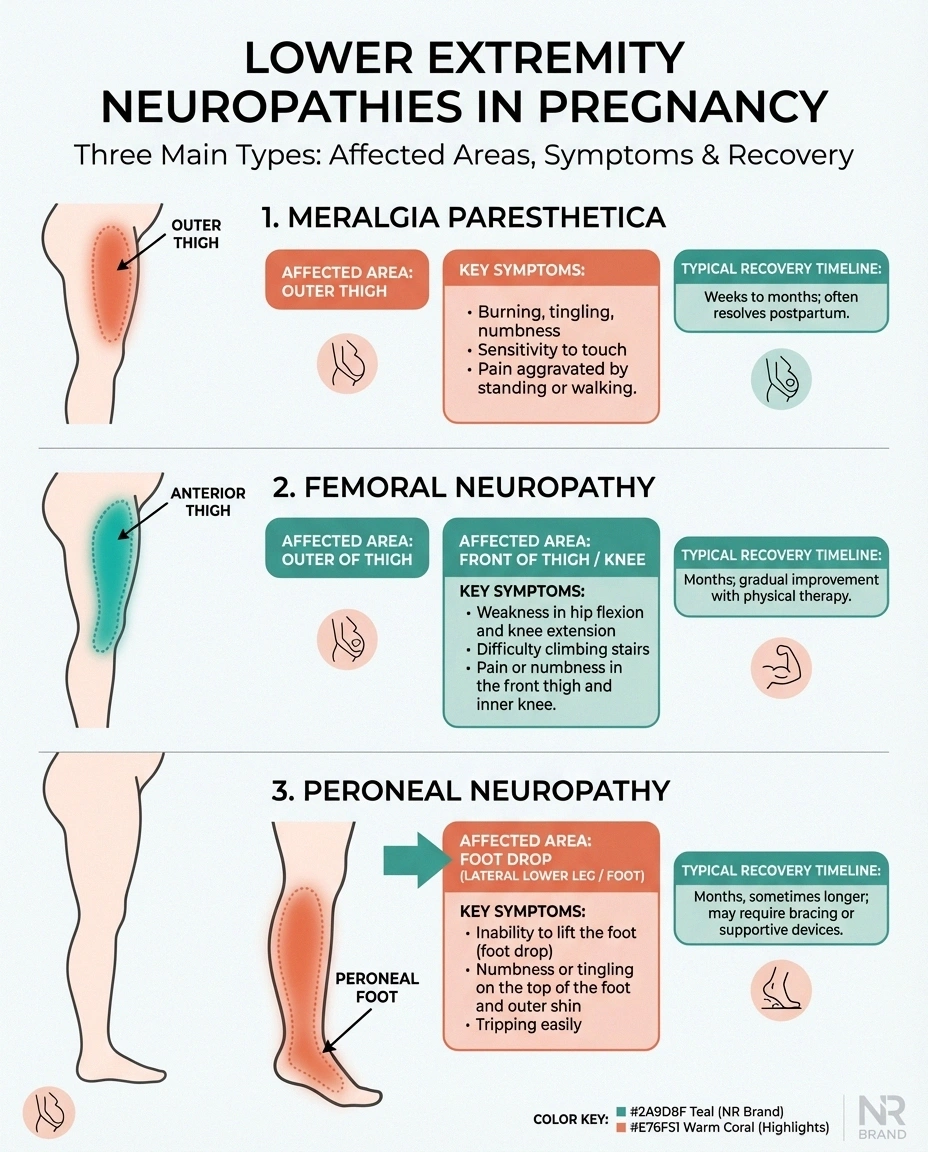
Meralgia Paresthetica (Lateral Femoral Cutaneous Nerve)
This is the second most common entrapment neuropathy in pregnancy after carpal tunnel syndrome. The lateral femoral cutaneous nerve passes under the inguinal ligament near the hip, and pregnancy's combination of weight gain, postural changes, and ligament laxity can compress it.
Symptoms: Burning, tingling, or numbness on the outer thigh. It's a purely sensory nerve, so there's no muscle weakness. Many women describe it as a patch of their thigh that feels “sunburned” or “numb and tingly at the same time.”
Treatment: This is primarily a waiting game. Meralgia paresthetica almost always resolves after delivery once the mechanical compression is relieved. Wearing loose clothing around the waist, avoiding prolonged standing, and gentle stretching may provide some relief in the meantime.
Femoral Neuropathy
The femoral nerve can be compressed during labor and delivery, particularly during prolonged pushing or when the hips are held in deep flexion for extended periods. Retractors used during cesarean section can also affect this nerve.
Symptoms: Weakness in knee extension (difficulty straightening the leg), reduced knee reflex, and numbness over the front of the thigh and inner leg.
Recovery: Most labor-related femoral neuropathies recover within three to six months, though physical therapy may be needed to maintain strength and prevent falls during recovery.
Peroneal Neuropathy
Compression of the peroneal nerve at the fibular head (just below the outer knee) can occur during labor if the legs are positioned in stirrups or held in certain positions for extended periods.
Symptoms: Foot drop — difficulty lifting the front part of your foot — and numbness over the top of the foot and outer lower leg.
Recovery: Attention to positioning during labor can help prevent this. Recovery usually occurs within weeks to months, though an ankle-foot orthosis may be needed temporarily to prevent tripping.
Lumbosacral Plexopathy: The Pelvic Nerve Bundle
The lumbosacral plexus — a network of nerves in the pelvis — can be compressed by the baby's head during labor. This is more common with larger babies, prolonged labor, and in women with a smaller pelvis.
Symptoms: Pain, weakness, and numbness in one or both legs, often developing during or shortly after delivery. The pattern depends on which part of the plexus is affected — it may mimic femoral neuropathy, peroneal neuropathy, or present with multiple nerve involvement.
This is different from epidural complications. It's important to distinguish lumbosacral plexopathy from complications of epidural or spinal anesthesia. While both can cause leg weakness after delivery, they have different causes, treatments, and prognoses. EMG and nerve conduction studies — which are safe postpartum — can help distinguish between these.
Recovery: Most cases improve significantly within months, though recovery can be gradual. Physical therapy, balance training, and supportive care are the mainstays of treatment.
Pre-Existing Neuropathy and Pregnancy
If you already have neuropathy before becoming pregnant, planning ahead is essential. Several conditions require special attention:

Action: Meticulous blood sugar management; coordinate with endocrinologist and OB
Action: Genetic counseling; physical therapy for balance; fall prevention planning
Action: IVIG generally considered safest treatment option during pregnancy
neuropathy in diabetics — Women with pre-existing diabetic neuropathy need meticulous blood sugar management throughout pregnancy. Autonomic neuropathy (affecting the autonomic nervous system) can be particularly challenging during pregnancy, as it may cause blood pressure instability, gastroparesis (delayed stomach emptying that worsens nausea), and altered heart rate responses. Close collaboration between your neurologist, endocrinologist, and OB team is critical.
Charcot-Marie-Tooth disease (CMT) — This inherited neuropathy doesn't prevent pregnancy, but it does require special planning. Women with CMT may experience worsening of symptoms during pregnancy, particularly increased weakness and balance difficulties. Genetic counseling about the risk of passing CMT to your child should be part of pregnancy planning.
Chronic inflammatory demyelinating polyneuropathy (CIDP) — This autoimmune neuropathy may flare during pregnancy, particularly in the third trimester and postpartum period. Treatment decisions become complex, as some immunosuppressive medications used for CIDP are not safe during pregnancy. Intravenous immunoglobulin (IVIG) is generally considered the safest option during pregnancy.
If you have any pre-existing nerve condition, I strongly encourage you to discuss pregnancy planning with both your neurologist and your OB/GYN before conceiving. Adjusting medications, optimizing nutrition, and establishing a monitoring plan beforehand can prevent many complications.
Gestational Diabetes and Nerve Risk
Gestational diabetes — diabetes that develops during pregnancy — affects six to nine percent of pregnancies. While it's a well-known risk factor for diabetes-related complications, its relationship with neuropathy during pregnancy is more nuanced.
The short answer: gestational diabetes alone is unlikely to cause significant neuropathy during the pregnancy itself. Diabetic neuropathy typically develops after years of chronic high blood sugar, not months. However, gestational diabetes does increase some risks worth knowing about:
- It may make existing subclinical nerve damage worse
- It increases the risk of having a larger baby, which raises the risk of delivery-related nerve compression
- It signals a higher lifetime risk of developing type 2 diabetes — and with it, diabetic neuropathy — later in life
- High blood sugar levels may impair the body's ability to heal from any nerve injury that does occur
Managing your blood sugar carefully during pregnancy protects both your immediate nerve health and your long-term risk. Talk to your healthcare team about monitoring and management strategies.
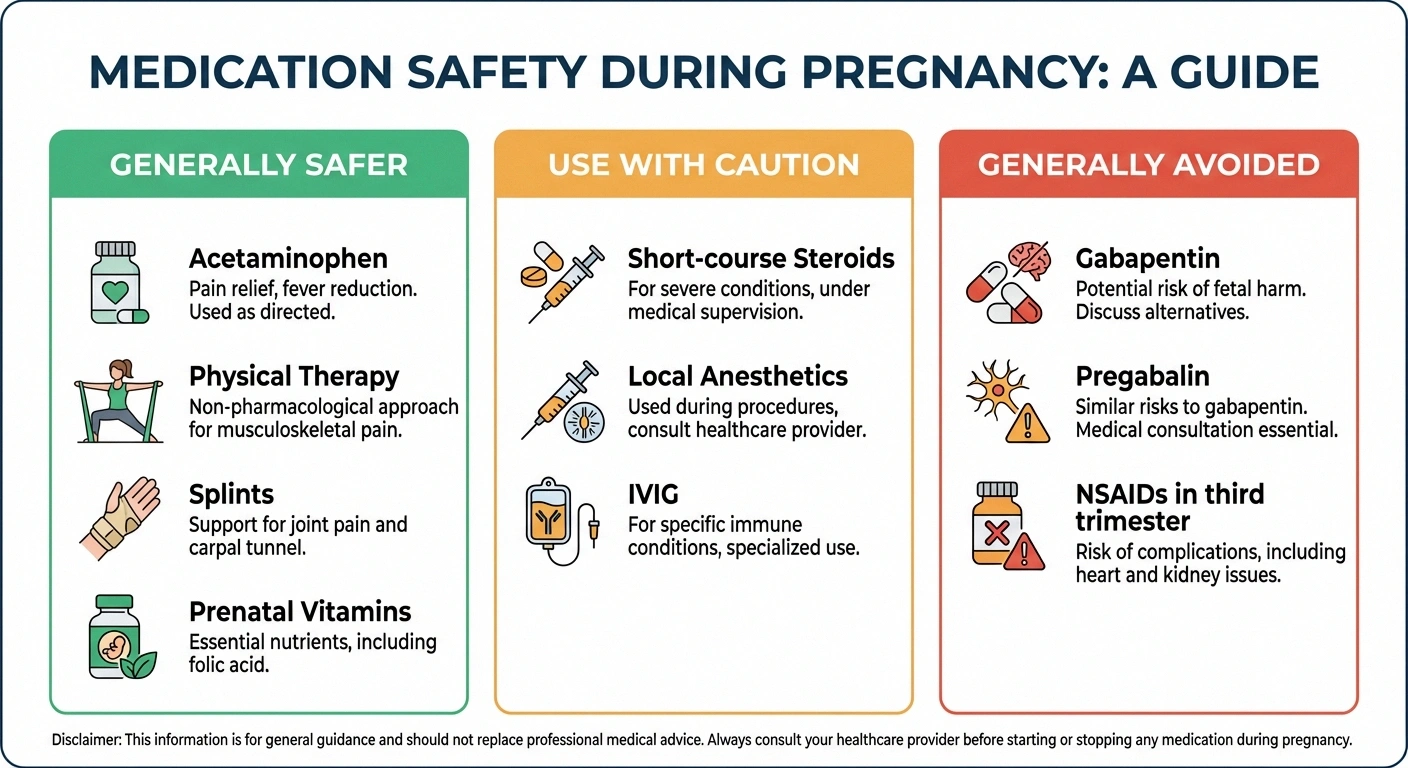
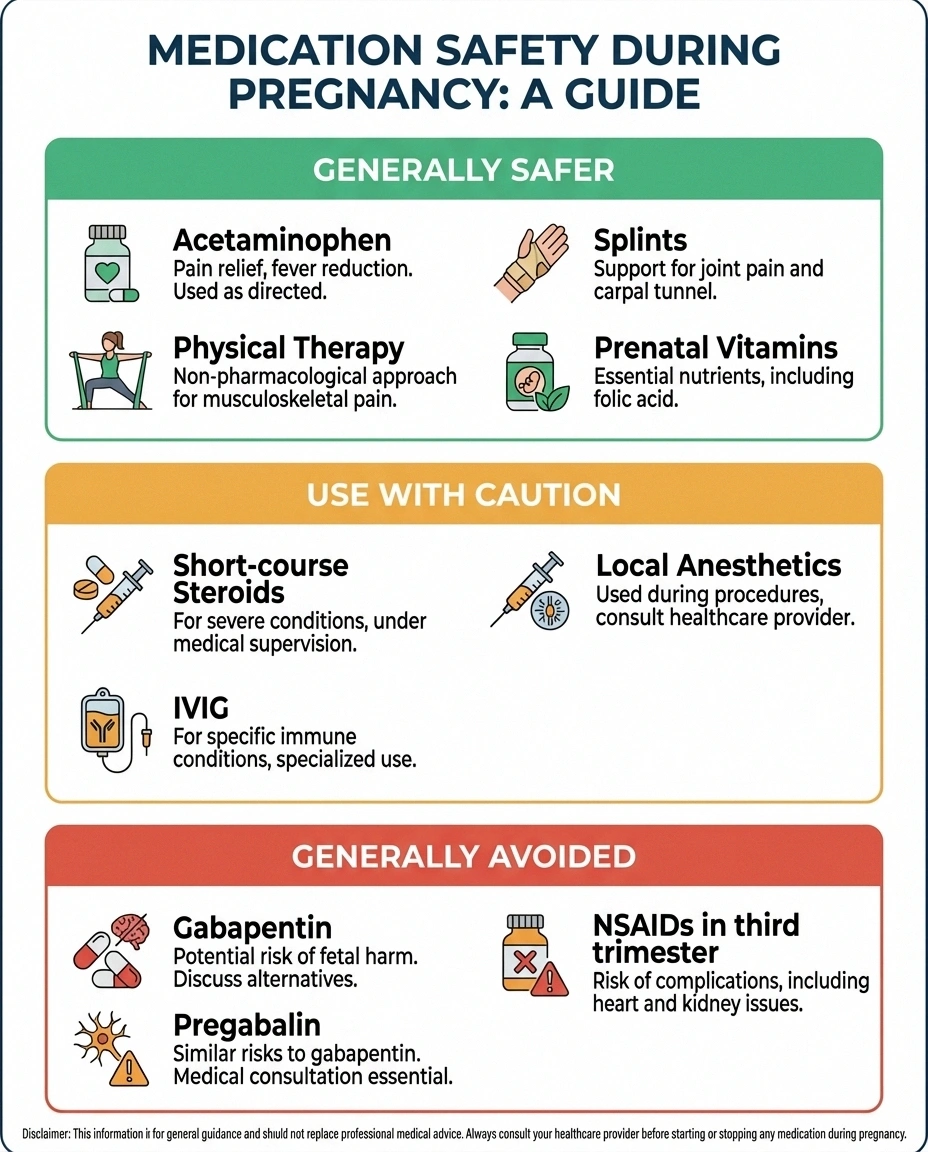
Medication Safety: Treating Nerve Pain During Pregnancy
One of the most challenging aspects of neuropathy during pregnancy is the limited treatment options. Many medications commonly used for nerve pain — including gabapentin, pregabalin, and duloxetine — have potential risks during pregnancy.
• Physical therapy
• Wrist splints & supports
• Topical treatments (discuss first)
• Prenatal vitamins with B vitamins
• Local anesthetic injections
• IVIG (for autoimmune cases)
• Most nerve pain antidepressants
• NSAIDs (third trimester)
• Opioids (except short-term)
Here's a general framework, though every situation is different and these decisions should always be made with your healthcare provider:
Generally considered safer during pregnancy:
- Acetaminophen (Tylenol) for mild pain
- Physical therapy and gentle exercise
- Wrist splints, supportive footwear, and positioning aids
- Topical treatments (used sparingly and discussed with your doctor)
- Prenatal vitamins with adequate B vitamins
Use with caution (risk-benefit discussion needed):
- Short-course corticosteroids (for severe Bell's palsy or CTS)
- Local anesthetic injections (for specific nerve blocks)
- IVIG (for autoimmune neuropathies)
Generally avoided during pregnancy:
- Gabapentin and pregabalin (limited safety data, potential fetal risks)
- Most antidepressants used for nerve pain (some may be continued if already prescribed — discuss with your doctor)
- NSAIDs in the third trimester
- Opioids (except in carefully managed short-term situations)
If you were taking neuropathy medications before becoming pregnant, do not stop them abruptly — some require gradual tapering to avoid withdrawal effects. Work with your prescribing doctor and OB to create a safe plan.
Nutrition for Nerve Health During Pregnancy
Good nutrition serves double duty during pregnancy — supporting your baby's development while protecting your nerve health. Pay special attention to these nutrients:

Vitamin B12 — Essential for myelin production (the protective coating around your nerves). B12 deficiency causes neuropathy and is more common in pregnancy, especially in women who follow vegetarian or vegan diets. Your prenatal vitamin should contain B12, but if you're deficient, supplementation or injections may be needed.
Folate — Critical for neural tube development in your baby and for nerve function in general. Most prenatal vitamins provide adequate folate, but women with MTHFR variants may need methylfolate instead of folic acid.
Iron — Iron deficiency anemia is common in pregnancy and can contribute to nerve dysfunction. Your OB should be monitoring your iron levels regularly.
Magnesium — Plays a role in nerve signaling and muscle function. Many pregnant women are mildly deficient, and supplementation (often magnesium glycinate, which is gentler on the stomach) may help with nerve symptoms, muscle cramps, and sleep.
Vitamin D — Increasingly recognized for its role in nerve health. Deficiency is common and worth testing for, especially if you have limited sun exposure.
A well-balanced neuropathy-supportive diet rich in leafy greens, lean proteins, whole grains, and healthy fats provides the foundation. Your prenatal vitamin fills in the gaps, but food should be your primary source of these nutrients.
Postpartum Neuropathy: When Symptoms Start After Delivery
Not all pregnancy-related neuropathies appear during pregnancy itself. Several nerve conditions commonly develop in the postpartum period:
Delivery-related nerve injuries — As discussed above, femoral, peroneal, and lumbosacral plexus injuries may become apparent only after delivery. If you notice new leg weakness, numbness, or difficulty walking in the hours and days after giving birth, report these symptoms to your medical team.
Postpartum carpal tunnel syndrome — CTS can develop or worsen postpartum, often related to the hand positioning demands of breastfeeding and constantly holding a newborn. Ergonomic adjustments to your nursing position and continued wrist splint use can help.
Postpartum Bell's palsy — The risk of Bell's palsy remains elevated in the early postpartum weeks. If you develop sudden facial weakness after delivery, seek medical evaluation promptly.
Neuralgic amyotrophy (Parsonage-Turner syndrome) — This rare but important condition involves sudden severe pain in the shoulder followed by weakness in the arm. It can be triggered by the immune shifts of pregnancy and delivery. The pain is often intense enough to require urgent medical attention.
The reassuring fact: the overall prognosis for recovery from pregnancy-related and postpartum neuropathies is very good. Most women recover fully, though some may need several months of patience and, in certain cases, physical therapy to regain full function.
When to Call Your Doctor
While most nerve symptoms during pregnancy are benign, certain situations warrant prompt medical evaluation:
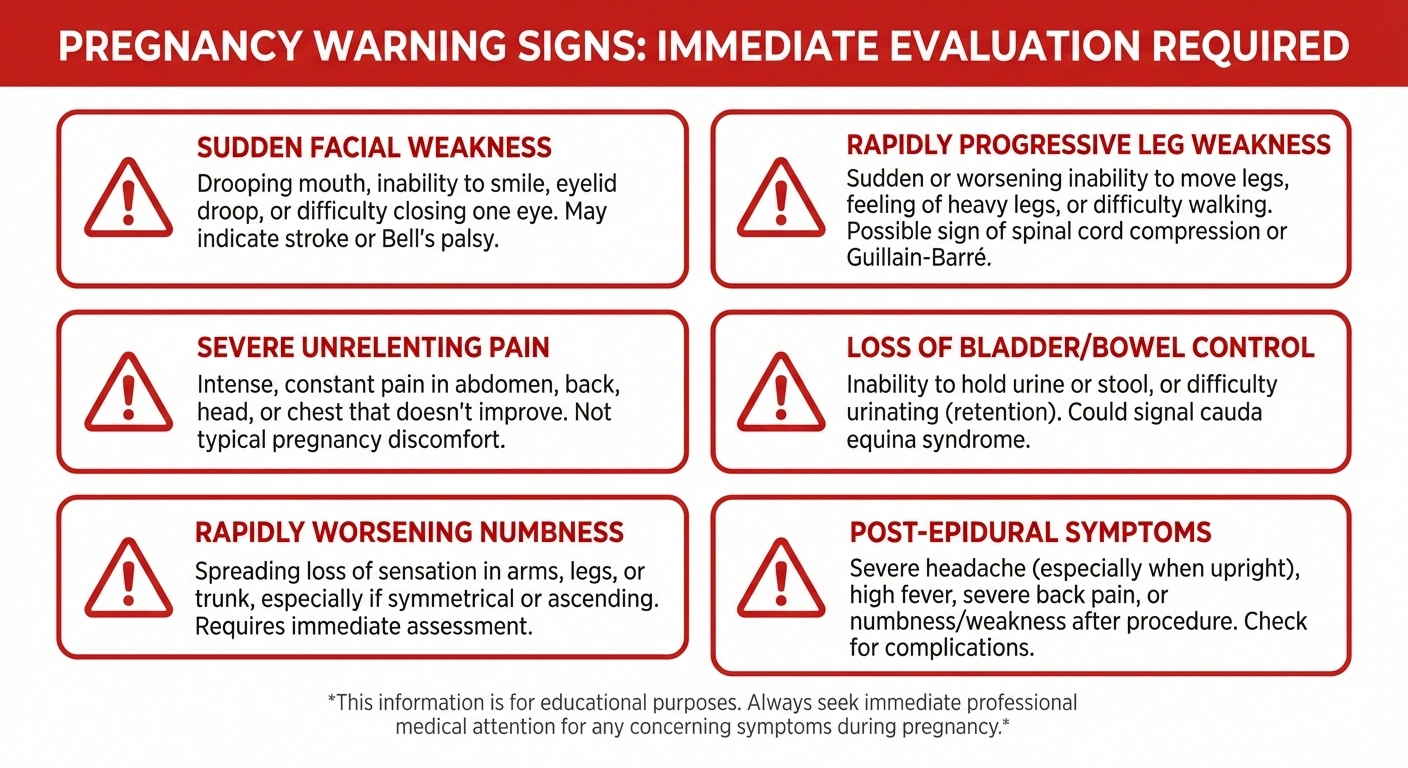
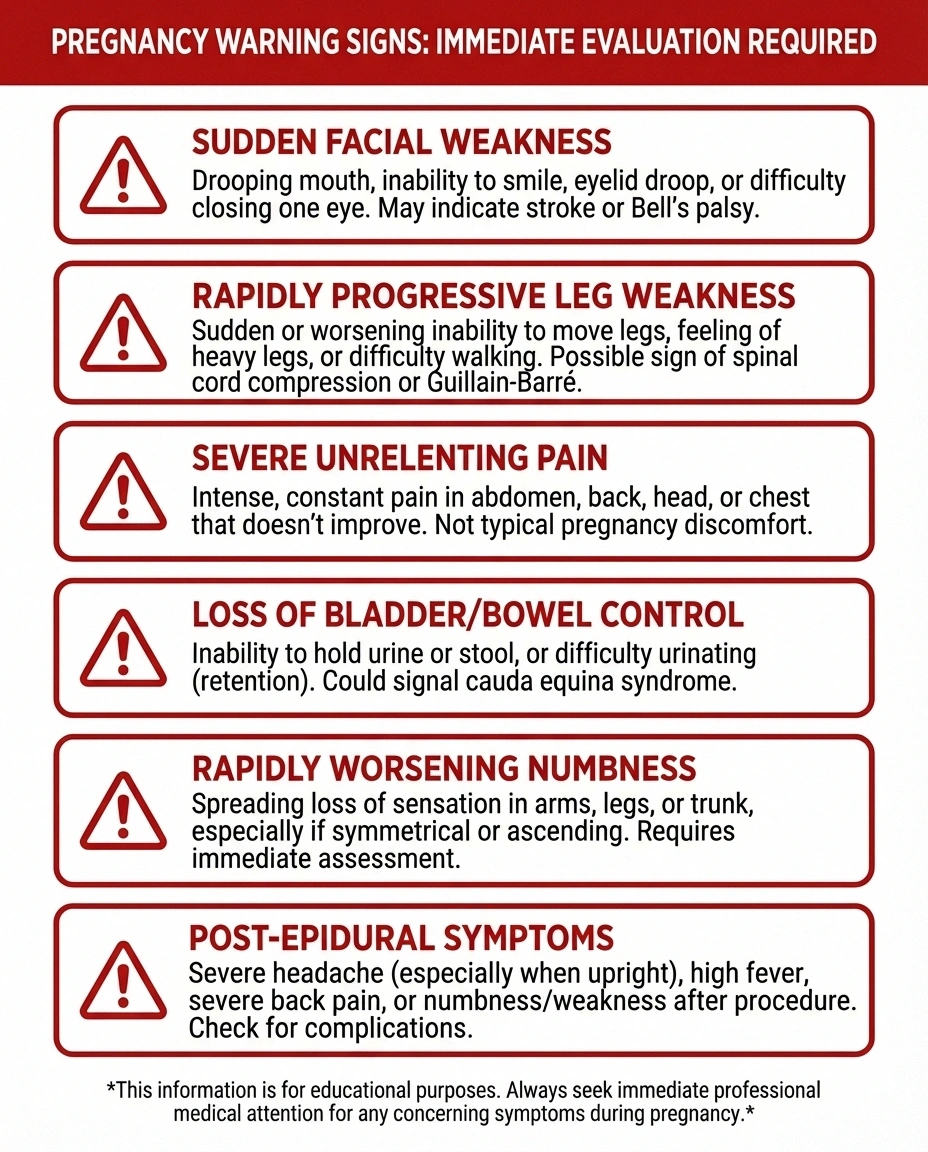
- Sudden weakness in your face, arm, or leg — This could indicate Bell's palsy, but it could also be a stroke. Seek emergency evaluation.
- Rapidly progressive weakness in both legs — Could indicate Guillain-Barré syndrome, which requires urgent treatment.
- Loss of bladder or bowel control — May indicate cauda equina syndrome, a medical emergency.
- Severe, unrelenting pain — Particularly in the shoulder (possible neuralgic amyotrophy) or leg (possible plexopathy).
- Numbness or weakness that is worsening rapidly — Rather than stable symptoms, progressive worsening needs evaluation.
- Symptoms that develop after epidural or spinal anesthesia — While usually temporary, these deserve assessment to rule out rare complications.
Trust your instincts. If something feels wrong, it's always better to have it checked and be reassured than to wait and wonder.
Frequently Asked Questions
Can pregnancy cause permanent nerve damage?
Permanent nerve damage from pregnancy is uncommon but can occur, particularly with severe delivery-related nerve compression or in cases where an underlying condition like diabetes contributes. The vast majority of pregnancy-related neuropathies resolve within months of delivery, especially carpal tunnel syndrome and meralgia paresthetica.
Will carpal tunnel syndrome come back in future pregnancies?
If you developed carpal tunnel syndrome during one pregnancy, there is a higher chance of recurrence in subsequent pregnancies. The fluid retention and hormonal changes that trigger it tend to repeat. However, knowing what to expect allows you to start wearing wrist splints early and manage symptoms proactively.
Is it safe to have an EMG or nerve conduction study during pregnancy?
Yes. EMG and nerve conduction studies are safe during pregnancy. They use very small electrical stimuli and fine needles that pose no risk to the developing baby. These tests can be helpful for diagnosing the specific nerve problem and guiding treatment decisions.
Can breastfeeding medications affect neuropathy?
Many neuropathy medications pass into breast milk. Gabapentin, pregabalin, and most antidepressants used for nerve pain are present in breast milk in varying amounts. The decision to take these while breastfeeding should weigh the mother's need for pain management against potential infant exposure. Discuss this with both your neurologist and pediatrician.
Does neuropathy during pregnancy affect the baby?
In most cases, maternal neuropathy does not directly affect the baby. The nerve symptoms affect the mother's peripheral nerves, not the baby's developing nervous system. The main concerns are indirect — neuropathy medications that may have fetal effects, and autonomic neuropathy that could affect blood pressure stability during pregnancy and delivery.
Should I see a neurologist during pregnancy for nerve symptoms?
A neurologist referral is recommended if symptoms are severe, progressive, don't fit a typical pattern like carpal tunnel syndrome, or if you have a pre-existing neurological condition. Many OB/GYN practices will refer you when symptoms persist beyond what's expected for normal pregnancy-related changes.
Taking Care of Your Nerves While Growing a Baby
Dealing with nerve symptoms during pregnancy adds an extra layer of challenge to an already demanding time. But here's what I want you to hold onto: the overwhelming majority of pregnancy-related neuropathies are temporary. Your body is doing extraordinary work right now, and the changes causing your nerve symptoms are part of that process.
Focus on what you can control — good nutrition, gentle movement, proper support devices like wrist splints, and open communication with your healthcare team. If your symptoms are manageable, know that they're very likely to improve after delivery. If they're not manageable, there are safe treatment options even during pregnancy.
And if you're planning a future pregnancy with an existing neuropathy condition, take the time to work with your medical team beforehand. A little preparation goes a long way toward a smoother experience for both you and your baby.
You're stronger than your nerves give you credit for right now. This, too, will pass.


