
The first time someone told me their treatment for neuropathy involved filtering their blood, I'll admit I pictured something out of a science fiction novel. A machine that pulls your blood out, separates the parts, takes some away, and gives the rest back? It sounded extreme.
The truth is more reassuring once you understand it. Plasma exchange — also called plasmapheresis or therapeutic plasma exchange — has been used safely for decades. For specific kinds of neuropathy where the immune system is attacking the nerves, it can be life-changing, and in some cases life-saving. It's not a treatment for the burning, tingling neuropathy that most readers of this site are dealing with. It's the right tool for a much narrower, but very serious, set of conditions.
This article walks through what plasma exchange actually is, when it's the right treatment, when it isn't, what the procedure feels like, and what the research shows about how well it works.
What Is Plasma Exchange?
Your blood is made of two main parts: cells (red cells, white cells, platelets) and a liquid called plasma that carries them. The plasma is mostly water, but it contains proteins, hormones, antibodies, and many other molecules that circulate throughout your body.
Key Takeaway
Plasma exchange physically removes harmful antibodies and immune molecules from the bloodstream. It's first-line treatment for Guillain-Barré syndrome and CIDP — but it does nothing for diabetic, chemotherapy-induced, or idiopathic neuropathies.
In certain neuropathies, the immune system goes haywire and produces antibodies that attack the body's own peripheral nerves. These autoantibodies — along with related inflammatory molecules — float in the plasma. Plasma exchange is, very literally, a way to remove them.
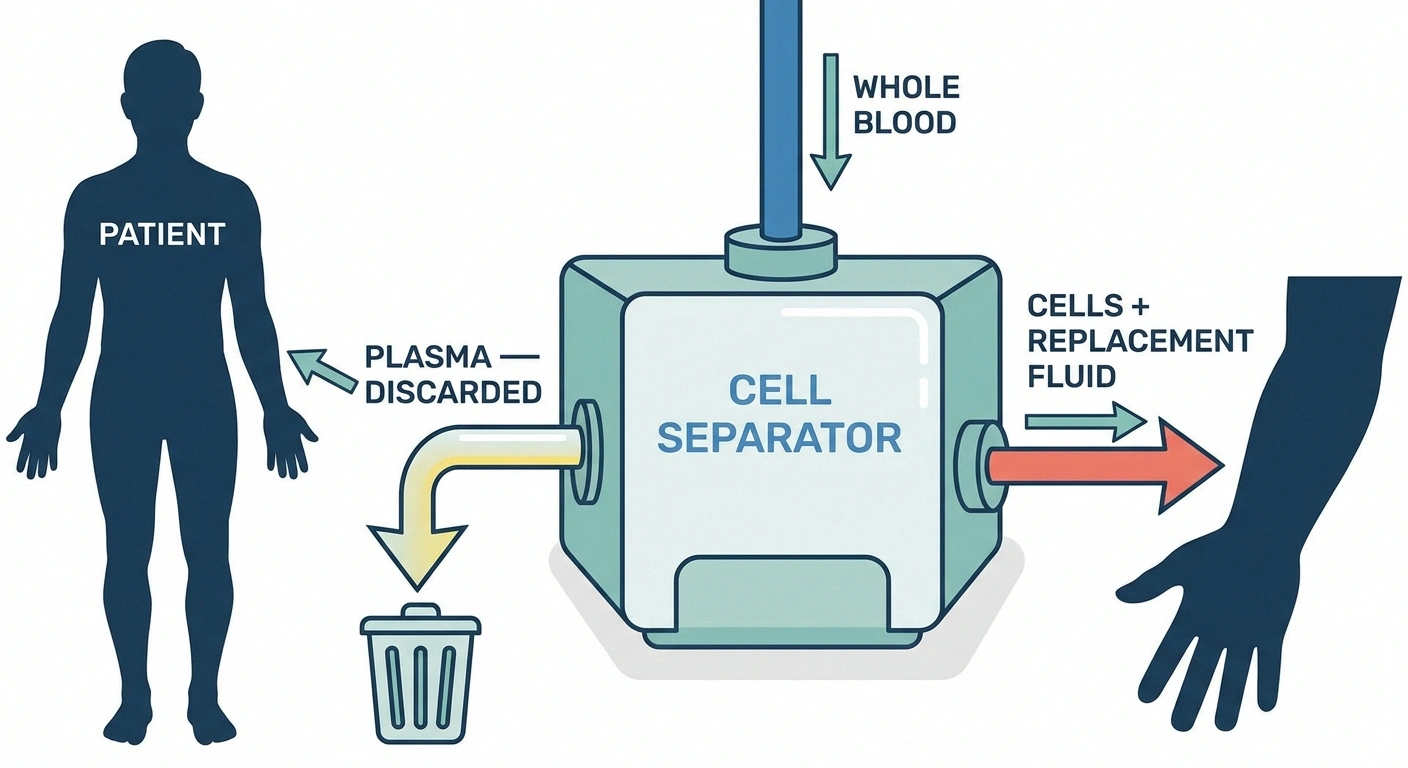
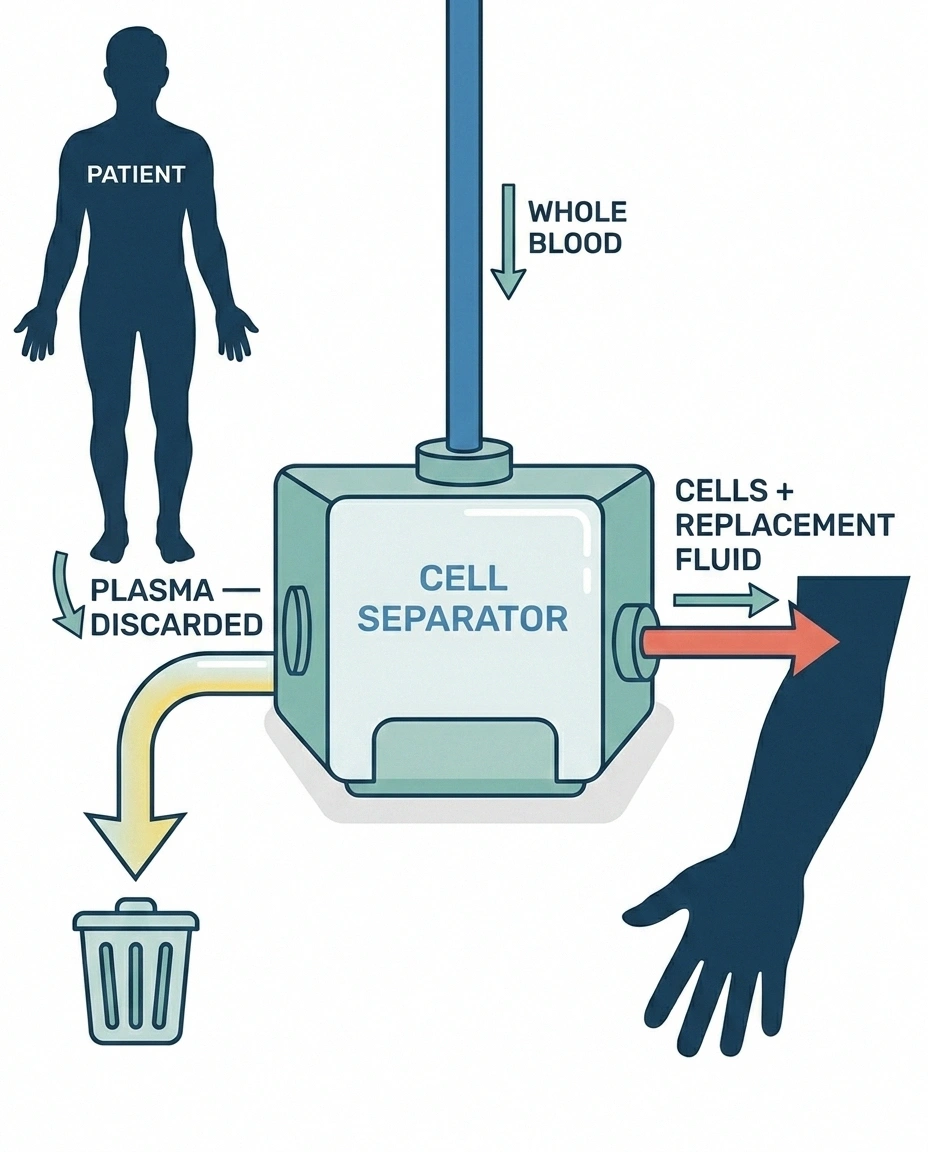
Here's what happens during a session:
- Blood is drawn from one access point — either a large peripheral IV or, more commonly for repeated sessions, a central venous catheter.
- A specialized machine called a cell separator spins the blood and separates plasma from cells, similar in principle to a blood-bank apheresis machine.
- The plasma is discarded.
- A replacement fluid — usually a 5% albumin solution, sometimes fresh frozen plasma — is mixed with the patient's own cells.
- The reconstituted blood is returned through a second access point.
One session typically removes 1 to 1.5 “plasma volumes” — meaning roughly the entire volume of plasma in your body — and takes 2 to 4 hours. The standard course is 5 sessions over 10 to 14 days, usually scheduled every other day. The whole experience is closer to dialysis than to surgery: you're awake, comfortable, and often reading or watching TV during the procedure.
Why Removing Plasma Helps Some Neuropathies
The therapeutic logic of plasma exchange depends entirely on the kind of neuropathy you have. Most cases of peripheral neuropathy — diabetic, alcoholic, idiopathic, vitamin-related, chemotherapy-induced — are not driven by circulating autoantibodies in the bloodstream. For those conditions, plasma exchange would do nothing useful.
What Plasma Exchange Removes
Autoantibodies
Antibodies the immune system has mistakenly produced against the body's own nerves.
Immune complexes
Antibody-antigen pairs that deposit in tissue and cause damage.
Complement proteins
Immune-system amplifiers that drive inflammation.
Inflammatory cytokines
Signaling molecules that direct immune attack on nerves.
Paraproteins
Abnormal antibodies from blood-cell disorders that damage nerves.
But a specific group of neuropathies are driven by circulating immune factors. In these conditions, plasma exchange does something dramatic: it physically removes the harmful agents from the body within hours, allowing nerve function to begin recovering as the immune attack pauses.
The classes of harmful factors that plasma exchange removes include:
- Autoantibodies — antibodies the immune system has mistakenly produced against the body's own nerves
- Immune complexes — antibody-antigen pairs that can deposit in tissue and cause damage
- Complement proteins — part of the immune system that amplifies inflammation
- Inflammatory cytokines — signaling molecules that drive immune attack
- Paraproteins — abnormal antibodies produced by certain blood-cell disorders
The effect is rapid. Patients with severe immune-mediated neuropathy can begin showing strength improvement within days of starting plasma exchange, compared to weeks for other treatments. The downside is that plasma exchange doesn't fix the underlying immune dysregulation — your immune system, left alone, will keep producing the antibodies. So plasma exchange is usually paired with other immunotherapies and may need to be repeated over months or years for chronic conditions.
When Plasma Exchange Is the Right Treatment
The American Society for Apheresis (ASFA) maintains a respected set of guidelines that grade conditions by how well plasma exchange works for them. The categories range from I (clear first-line therapy) to IV (not recommended). For neuropathies, the strongest indications are:
🔎 Research Says
Multiple Cochrane systematic reviews have established that plasma exchange and IVIG have equivalent efficacy in Guillain-Barré syndrome. Neither is clearly superior on average. Both work best when started within 7 days of symptom onset — early treatment cuts ventilation duration and improves long-term recovery.
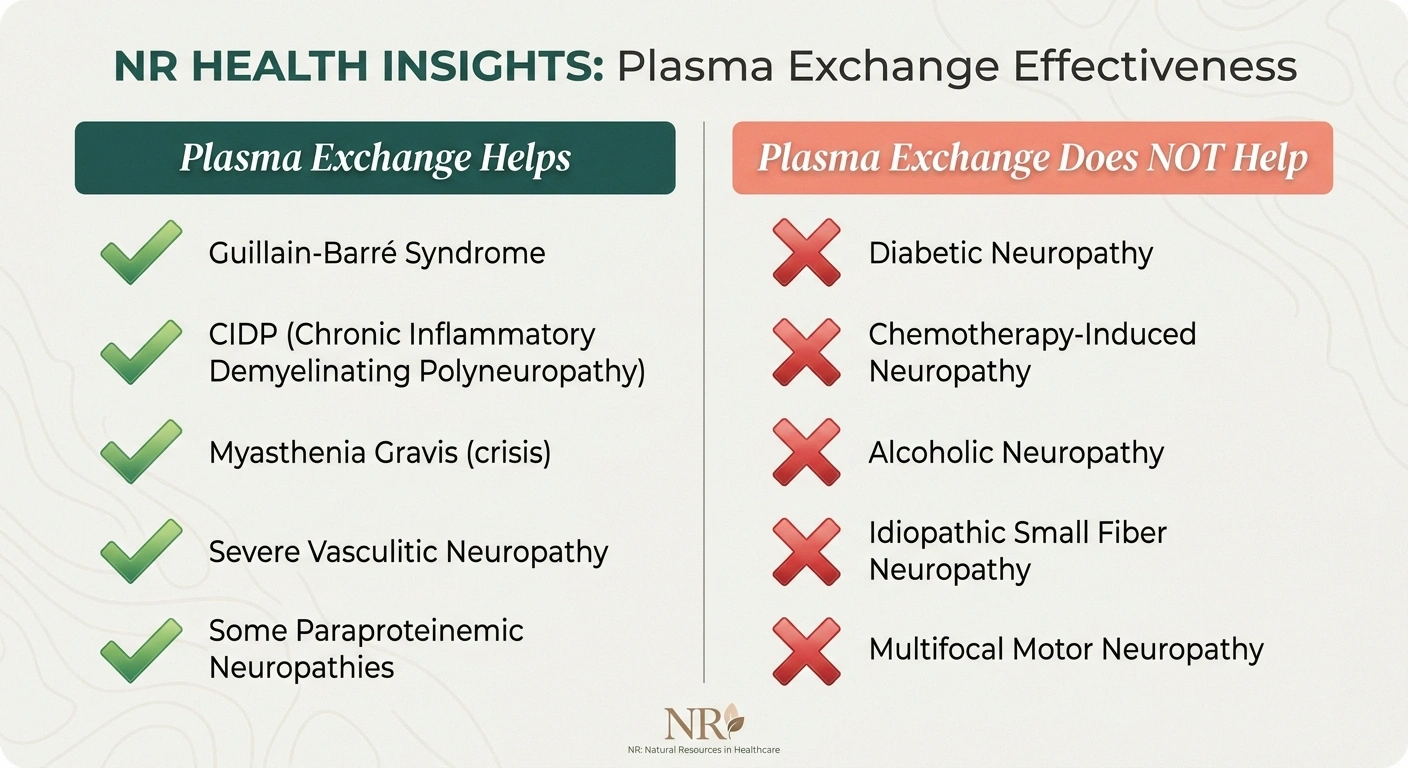
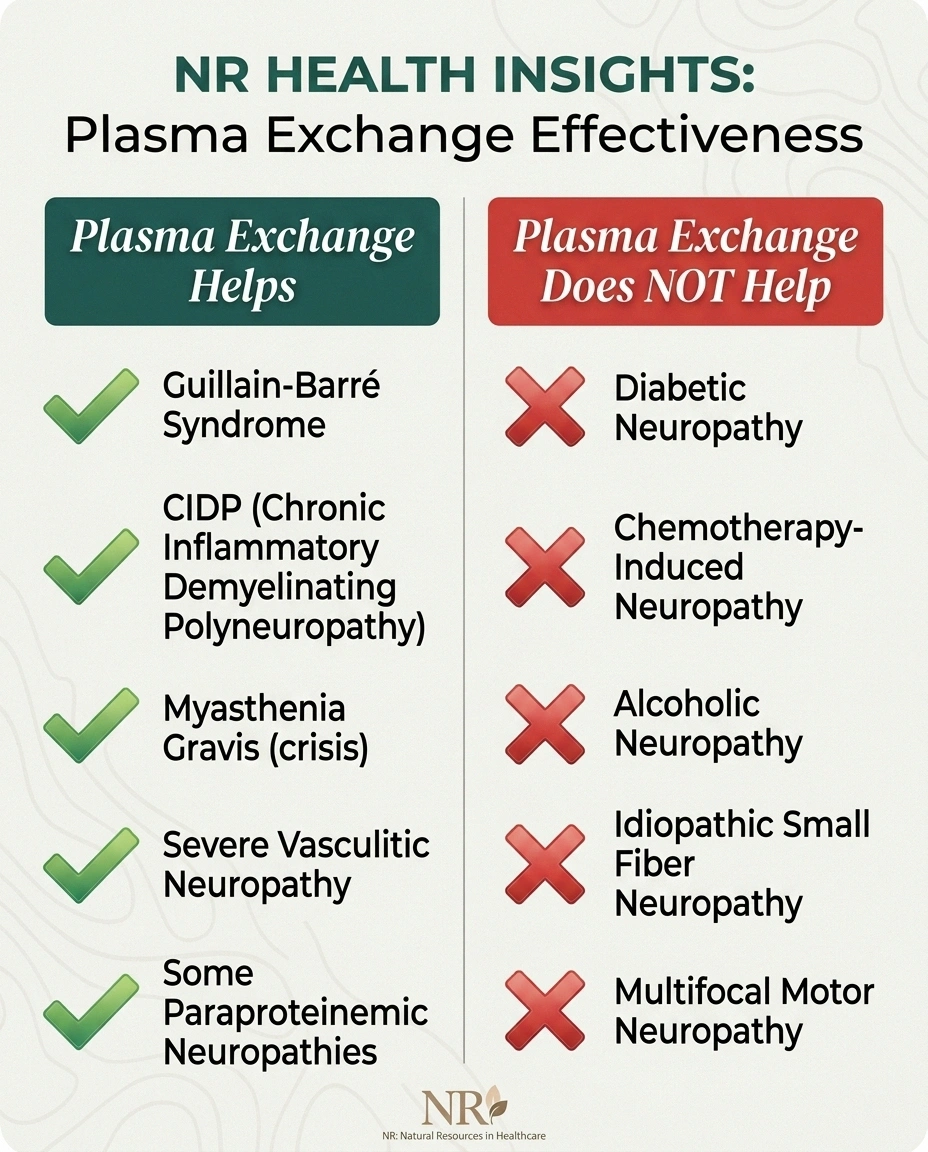
Guillain-Barré Syndrome (GBS) — ASFA Category I. GBS is an acute autoimmune attack on the peripheral nerves, often triggered by a recent infection. It causes rapidly progressive weakness, sometimes leading to paralysis and respiratory failure within days. Plasma exchange and IVIG are the two established first-line treatments — and according to multiple Cochrane systematic reviews, they have equivalent efficacy. The choice between them depends on availability, vascular access, patient factors, and physician experience. Both work best when started within 7 days of symptom onset, and ideally within the first 2 weeks. Studies show plasma exchange reduces the duration of mechanical ventilation, accelerates motor recovery, and improves long-term outcomes when given early.
Chronic Inflammatory Demyelinating Polyradiculoneuropathy (CIDP) — ASFA Category I. CIDP is the chronic cousin of GBS — a slow-motion autoimmune attack on the peripheral nerves that causes progressive weakness and sensory loss. Plasma exchange is one of three first-line treatments (alongside IVIG and corticosteroids). It's particularly useful during acute deterioration, but some patients also use it as long-term maintenance therapy with sessions every few weeks. Research has shown that serum from CIDP patients can transfer disease features in laboratory models, which provides direct evidence that circulating factors drive the disease — and explains why removing those factors works.
Myasthenia Gravis (related — neuromuscular junction). While myasthenia gravis affects the connection between nerve and muscle rather than the nerve itself, it's worth mentioning here because patients often see neurologists who manage both conditions. Plasma exchange is ASFA Category I for myasthenic crisis (acute respiratory deterioration) and is widely used.
Vasculitic neuropathy caused by autoimmune blood vessel inflammation, in severe cases.
Some paraproteinemic neuropathies — particularly those associated with IgM monoclonal gammopathies, including anti-MAG neuropathy in selected cases. The evidence here is more mixed, and plasma exchange is typically combined with other treatments.
Notably, plasma exchange is not recommended for multifocal motor neuropathy (MMN). In MMN, plasma exchange has actually been associated with worsening in some patients. IVIG is the treatment of choice for that condition.
And it's not used for the much more common neuropathy types — diabetic peripheral neuropathy, chemotherapy-induced neuropathy, alcoholic neuropathy, idiopathic small-fiber neuropathy. These conditions don't respond to plasma exchange because they're not driven by circulating immune factors that can be filtered out.
What the Research Shows
The research base for plasma exchange in immune-mediated neuropathy is decades old and well-established for the indications above. A few highlights worth knowing:
For Guillain-Barré syndrome, a Cochrane systematic review covering six randomized trials concluded that plasma exchange significantly reduces disability at four weeks and improves recovery at one year compared to supportive care alone. The benefit is largest when treatment is started within the first week of symptoms.
Multiple head-to-head studies comparing plasma exchange to IVIG in GBS have shown equivalent efficacy — neither treatment is clearly superior on average. This means the choice between them is often pragmatic: IVIG is easier to administer (peripheral IV vs. central line), but plasma exchange may have faster onset of action and avoids the rare but real thrombotic risk of high-dose IVIG.
For CIDP, plasma exchange has been demonstrated effective in randomized controlled trials going back to the 1980s. The evidence base is solid enough that ASFA classifies it as a Category I first-line indication. Long-term data shows that some patients respond better to plasma exchange than to IVIG, and vice versa, which is why a treatment trial of one and then the other is sometimes used to find the right approach for an individual patient.
One area of recent debate is the practice of combining IVIG followed by plasma exchange in GBS. A 2025 review in Frontiers in Neurology argued that this sequence may actually be counterproductive — the plasma exchange after IVIG can remove much of the just-infused immunoglobulin, reducing its therapeutic effect. The current recommendation is generally to choose one approach and stick with it rather than layering them.
What the Procedure Feels Like

If you or a family member is facing plasma exchange, knowing what to expect helps. Here's the practical experience:
A Plasma Exchange Session — Step by Step
Vascular access established
Two large peripheral IVs or a tunneled central catheter.
Blood drawn into cell separator
A specialized machine spins blood and separates cells from plasma.
Plasma is discarded
All circulating antibodies, complement, and cytokines go with it.
Replacement fluid mixed with cells
Usually a 5% albumin solution; occasionally fresh frozen plasma.
Reconstituted blood returned
2-4 hours total. Standard course: 5 sessions every other day for 10-14 days.
Before the first session. You'll have an evaluation including blood work to check for clotting issues, calcium and magnesium levels, and overall medical fitness. Vascular access is established — for a short course, this might be a large-bore peripheral IV in each arm. For longer courses, a tunneled central venous catheter may be placed in the chest, which sounds intimidating but is a routine procedure done under local anesthesia.
During the session. You'll be in a chair or bed, often in an apheresis suite that looks similar to a dialysis unit. You'll have IV lines in both arms (or a central line) and a blood pressure cuff that takes readings frequently. The cell separator machine sits next to you. Many people watch TV, read, or nap during the 2-4 hour session. You're not asleep or sedated.
What you'll feel. The most common sensation is tingling around the mouth and in the fingers, caused by the citrate anticoagulant lowering your blood calcium temporarily. The nursing team treats this with calcium tablets or IV calcium when it occurs. Some people feel cold (the blood being returned is at room temperature), so warm blankets are standard. A small percentage experience a drop in blood pressure that's quickly managed.
After the session. Most people feel tired and may have mild flu-like fatigue for the rest of the day. Plenty of fluids and rest help. You'll have follow-up labs to check electrolytes and clotting factors.
Across the course. Improvement in muscle strength and function typically begins within a few days of starting and often continues for weeks after the course is complete. Some patients begin to see clear functional improvement by the third or fourth session.
Risks and Side Effects

Plasma exchange has a generally good safety profile when performed in experienced apheresis centers, but there are real risks worth knowing:
Not for All Neuropathies
Plasma exchange is not a treatment for diabetic, alcoholic, chemotherapy-induced, or idiopathic neuropathy. It only helps neuropathies driven by circulating immune factors — and it can actually worsen multifocal motor neuropathy. Diagnosis-specific guidance is essential.
- Hypotension from volume shifts during the procedure — usually managed with fluids and slowing the rate
- Citrate toxicity causing tingling, perioral numbness, and low calcium — managed with calcium supplementation
- Allergic reactions to the replacement fluid (more common with fresh frozen plasma than albumin)
- Infection risk from the central venous catheter — meticulous line care is essential
- Bleeding tendency due to transient depletion of clotting factors removed in plasma — usually mild and self-resolving
- Reduced infection-fighting antibodies for several weeks, increasing susceptibility to infections during that window
- Electrolyte disturbances — low calcium, low magnesium, sometimes low potassium
Serious adverse events are uncommon. Major complication rates in modern apheresis centers are well under 5%, and life-threatening complications under 1%.
Plasma Exchange vs. IVIG: How to Think About the Choice
For the indications where both work — GBS and CIDP especially — patients and families often want to understand why one might be chosen over the other. Here's how that conversation usually goes with a neurologist:
Plasma Exchange vs. IVIG — Quick Comparison
Efficacy
Equivalent in GBS and CIDP per Cochrane review and ASFA guidelines.
Onset of action
PE often faster (days). IVIG typically slightly slower.
Vascular access
PE: large IVs or central line. IVIG: peripheral IV is fine.
Outpatient ease
IVIG: home infusion programs widely available. PE: typically infusion-center based.
Specific cautions
PE: bleeding, central line infection. IVIG: thrombosis, IgA deficiency, volume load.
Plasma exchange tends to be preferred when:
- The patient has had thrombotic complications with IVIG before, or has high baseline thrombotic risk
- IgA deficiency is present (some IVIG products are contraindicated)
- Heart failure or kidney disease makes the volume load of IVIG difficult to manage
- Faster onset of action is felt to be important
- The patient hasn't responded adequately to IVIG
IVIG tends to be preferred when:
- Vascular access is difficult or central line placement is undesirable
- The treatment center doesn't have apheresis available
- The patient has bleeding risk or coagulopathy
- Long-term outpatient maintenance is the goal (home IVIG infusion programs are well-established)
- Multifocal motor neuropathy is the diagnosis
For most patients with GBS or CIDP, both options are reasonable, and the choice often comes down to local availability, individual factors, and physician preference. Some patients try one and switch to the other if the first doesn't work well — both are part of the modern toolkit, not competing approaches.
Living Through a Course of Plasma Exchange

For people who go through plasma exchange — particularly for an acute condition like GBS — the experience can feel like a complete disruption to daily life followed by a slow climb back. Here are a few things I've heard from people in my support group who have been through it:
The emotional toll is real. Being acutely ill, often hospitalized, with weakness severe enough that this aggressive treatment is needed, is frightening. Anxiety and depression during and after a course of plasma exchange are common. Speaking with the medical team about emotional support, social work, or counseling resources is reasonable.
Recovery is gradual, not instant. Even when plasma exchange is working, full recovery from severe Guillain-Barré can take months to over a year. Physical therapy is essential during this period to rebuild strength and prevent contractures.
Infection precautions matter for several weeks. Because plasma exchange temporarily lowers your circulating antibody levels, you'll be more susceptible to infections during the recovery period. Hand hygiene, avoiding sick contacts, and being alert for fever are important.
Follow-up monitoring is ongoing. For chronic conditions like CIDP, ongoing monitoring of disease activity and decisions about maintenance therapy continue indefinitely. The neurologist becomes a long-term partner.
Support groups help. Both GBS and CIDP have well-organized patient support communities. Connecting with others who have been through what you're going through is one of the most powerful resources available.
The Right Tool for the Right Job
Plasma exchange is sometimes described in medical writing as a “physical immunotherapy” — it doesn't suppress the immune system the way drugs do; it removes the immune system's harmful products from circulation. For the immune-mediated neuropathies, that physical removal is genuinely transformative. People who would have been permanently disabled or worse without it routinely make near-complete recoveries.
5 sessions
in 10-14 days — the typical course for acute immune-mediated neuropathy
Each session removes 1-1.5 plasma volumes. Strength improvement often begins by session 2 or 3. Recovery continues for weeks to months after the course is complete.
For the much larger group of people with peripheral neuropathy from diabetes, chemotherapy, alcohol, vitamin deficiencies, or unknown causes, plasma exchange is not the answer. The mechanism doesn't apply, and the procedure carries real risks without commensurate benefit.
If you're being evaluated for plasma exchange, it means your medical team has identified — or strongly suspects — an immune-mediated process driving your nerve damage. That's actually a hopeful diagnosis, because immune-mediated neuropathies often respond well to treatment when the cause is correctly identified. The diagnostic workup that gets you to that point — including specialized testing like nerve conduction studies, lumbar puncture for protein analysis, and antibody panels — is part of why precise neurological care matters.
Plasma exchange is not a treatment to seek out for general nerve discomfort. It's a treatment for a specific kind of disease, given by specific kinds of medical teams, in specific settings. When it's the right answer, it's a remarkable answer.
Frequently Asked Questions
What is plasmapheresis used for?
In neurology, plasmapheresis is used primarily for immune-mediated neuropathies and related conditions including Guillain-Barré syndrome, chronic inflammatory demyelinating polyradiculoneuropathy (CIDP), myasthenia gravis crisis, and certain vasculitic and paraproteinemic neuropathies. It is also used for many non-neurological conditions including some kidney diseases, blood disorders, and severe autoimmune conditions.
How long does a plasma exchange session take?
A single plasma exchange session typically takes 2 to 4 hours from start to finish. The standard course for an acute neurological condition is 5 sessions performed every other day over 10 to 14 days. Some chronic conditions require maintenance sessions every few weeks indefinitely.
Is plasma exchange the same as dialysis?
No, but they share some similarities in setup. Dialysis filters waste products from blood for people with kidney failure. Plasma exchange separates and removes plasma containing pathogenic antibodies and immune complexes, replacing it with a substitute fluid. The machines, vascular access requirements, and patient experience are similar but the medical purpose is different.
How much does plasma exchange cost?
In the United States, a single plasma exchange session typically costs between 5,000 and 10,000 dollars when including facility, equipment, replacement fluid, and professional fees. A full course of 5 sessions can cost 25,000 to 50,000 dollars. Insurance coverage is generally available for ASFA Category I indications including Guillain-Barré syndrome and CIDP, but pre-authorization is often required.
Can plasma exchange cure neuropathy?
For acute immune-mediated neuropathies like Guillain-Barré syndrome, plasma exchange combined with supportive care can lead to near-complete recovery in many patients. For chronic conditions like CIDP, plasma exchange controls the disease but does not cure it — ongoing maintenance therapy is usually required. Plasma exchange does not cure or even help non-immune neuropathies including diabetic, alcoholic, or chemotherapy-induced neuropathy.
What are the side effects of plasmapheresis?
Common side effects include perioral and finger tingling from the citrate anticoagulant, mild hypotension, fatigue, feeling cold during the procedure, and temporary low calcium or magnesium levels. Less common but more serious risks include central line infections, allergic reactions to replacement fluid, and increased infection susceptibility for several weeks due to lowered antibody levels. Major complication rates in experienced centers are below 5%.
How quickly does plasma exchange work?
Plasma exchange has one of the fastest onsets of any neuropathy treatment. Improvement in muscle strength and function often begins within days of starting, sometimes after just 2 or 3 sessions. Maximum benefit typically develops over the course of treatment and continues for several weeks afterward. The rapid onset is one of the main advantages of plasma exchange over other immunotherapies.
Is plasma exchange better than IVIG for Guillain-Barré?
Multiple randomized trials and Cochrane systematic reviews have shown plasma exchange and IVIG to have equivalent efficacy in Guillain-Barré syndrome. Neither is clearly superior on average. The choice between them depends on availability, vascular access considerations, patient-specific risk factors, and physician experience. Both should be started early — within 7 days of symptom onset whenever possible.


