The day my own EMG report came back, I sat at the kitchen table with a manila envelope, a half-cold cup of coffee, and a printout that may as well have been written in a foreign language. Phrases like “reduced CMAP amplitude,” “prolonged distal latency,” and “abnormal spontaneous activity in the tibialis anterior” stared up at me. I knew the test had something to do with my neuropathy. I had no idea whether the words on that page were good news, bad news, or the same news I already had.
If you are sitting at your own kitchen table right now with your own report, this article is for you. I am not a doctor and I cannot interpret your specific numbers. What I can do, after years of being a patient and helping other patients in our community navigate exactly this moment, is walk you through the layout of a typical EMG and nerve conduction study report so the words stop being noise. By the end, you will know what each section is measuring, what the numbers mean in plain language, and which questions to bring to your neurologist when you sit down to discuss it. The interpretation is your neurologist's job. Reading the report intelligently and asking better questions is yours.
What an EMG and a Nerve Conduction Study Actually Measure
Most people walk out of the test thinking they had “an EMG.” In almost every case, you actually had two tests done back to back: a nerve conduction study (NCS) and an electromyography (EMG). They look at different things and the report combines both, which is part of why the document is so confusing on first read.
Your report is two tests in one. The nerve conduction study measures the electrical signal traveling through your nerve fibers. The needle EMG listens to what your muscles are doing in response. Read together, they tell your neurologist whether the nerve is damaged and whether the muscle has started to suffer because of it.
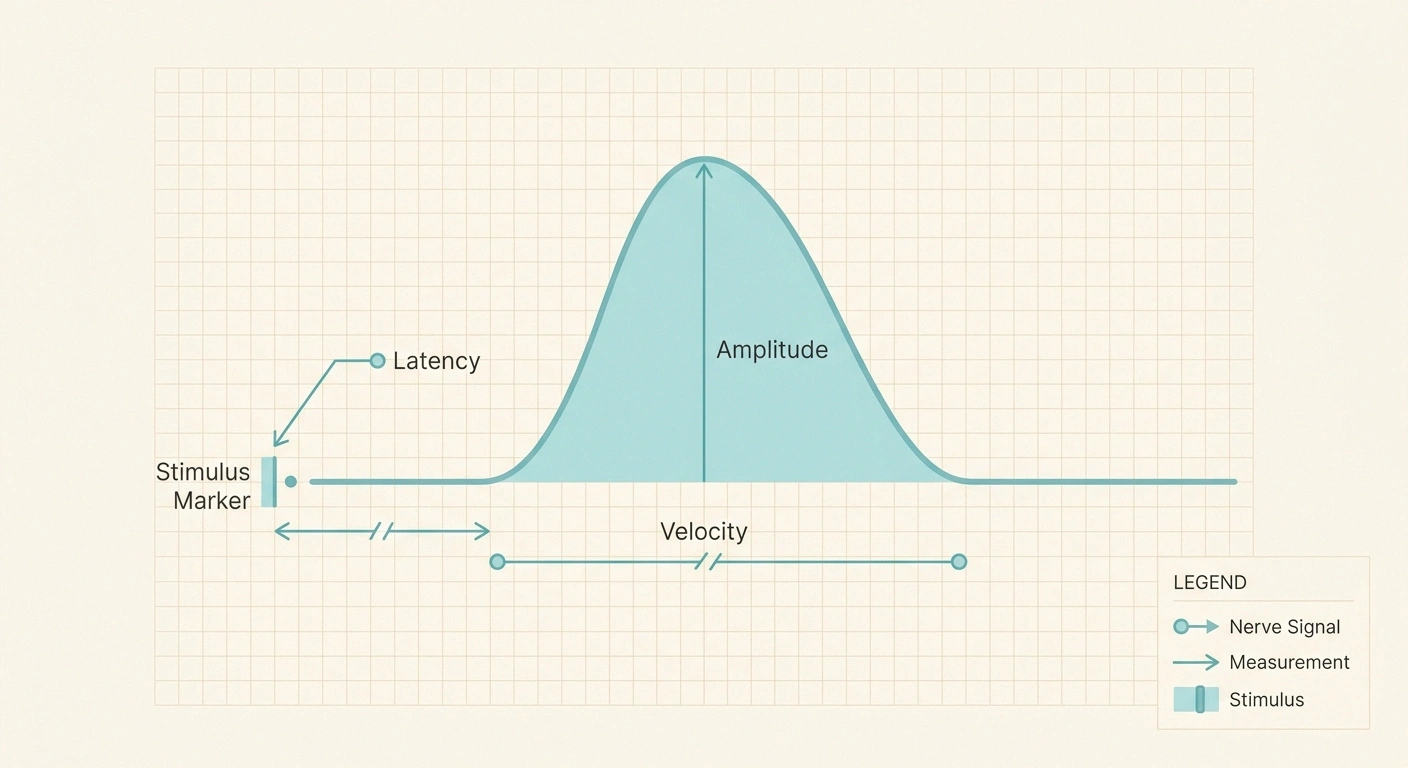
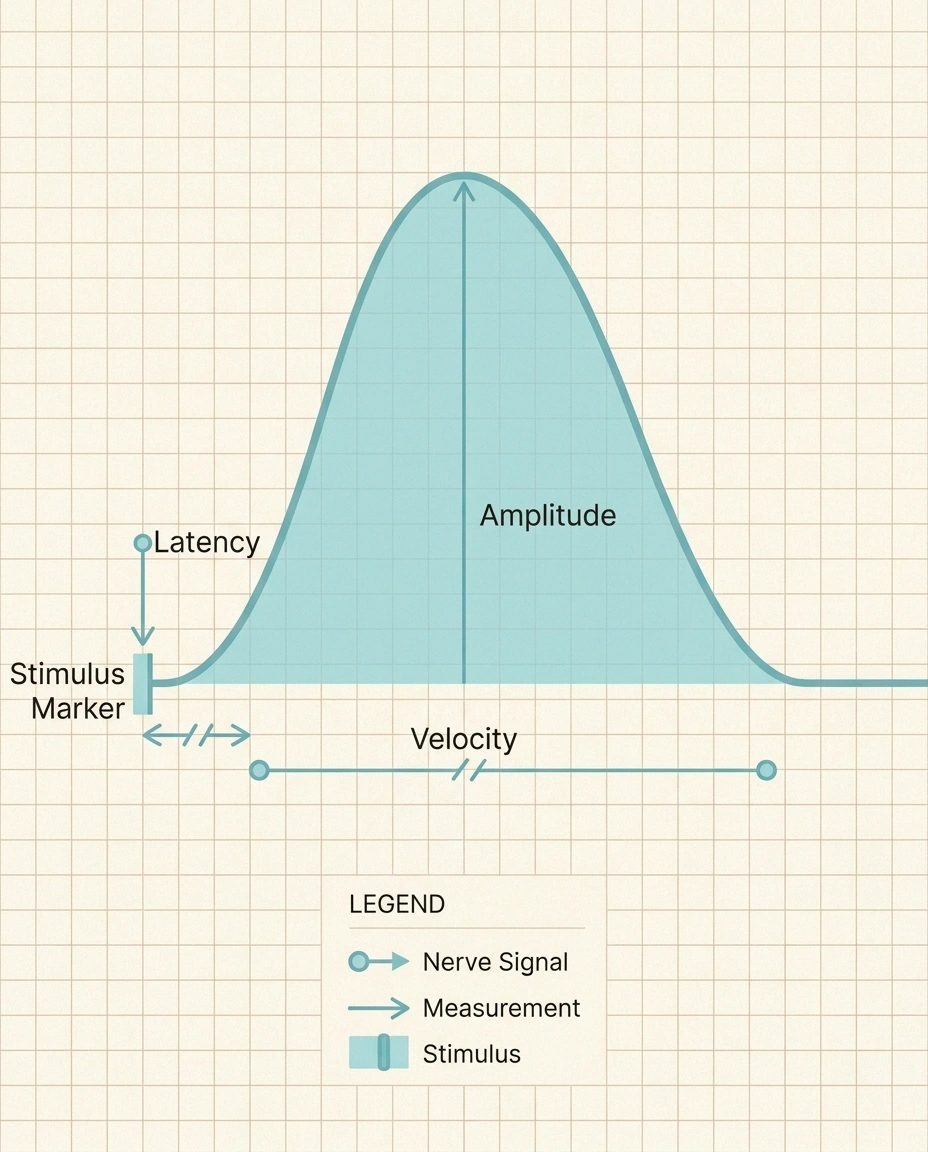
A nerve conduction study sends a small electrical pulse along a nerve and measures how fast and how strongly the signal travels. Stickers go on your skin, a stimulator clicks at one spot, and a recorder picks up the response further down the limb. The output is a set of numbers describing the wave: how fast it moved, how tall it was, and how long it took to start. According to the National Library of Medicine's MedlinePlus guide to EMG and NCS, the two are routinely run together because each one fills in a piece the other cannot see.
An electromyography study uses a thin needle electrode placed directly into a muscle. The neurologist listens and watches the electrical chatter of the muscle while it is at rest and while you contract it. The report describes what was heard: was the muscle quiet at rest as it should be, or was there spontaneous noise that should not be there? When you contracted, did the motor units fire in a normal pattern?
The reason both are done together is straightforward. The nerve conduction study tells your neurologist what is happening inside the nerve fibers themselves. The needle EMG tells them what is happening in the muscle that the nerve is supposed to be controlling. Put together, they answer two questions: is the nerve damaged, and if so, has the muscle started to suffer because of it? If you want a deeper map of the full diagnostic workup, our guide on tests your doctor may order for neuropathy covers where EMG and NCS sit in the larger picture.
The Anatomy of an EMG/NCS Report
Every report I have ever seen, and every report described in the AANEM standards for reporting, follows roughly the same four-part skeleton. Once you can find each section on the page, the rest gets a lot easier.
- NCV (Nerve Conduction Velocity)
- How fast the signal travels through the nerve, in meters per second.
- Amplitude
- How tall the recorded wave is. A measure of how many fibers are working.
- Distal Latency
- Time in milliseconds from stimulus to first response near the muscle.
- F-Wave
- A late signal that travels up the nerve and back; tests the full length.
- H-Reflex
- An electrical reflex measured in the calf; evaluates the reflex arc.
- Fibrillation Potential
- Single muscle fiber firing on its own; sign the nerve supply is lost.
- MUAP
- Motor unit action potential; the wave a working motor unit produces.
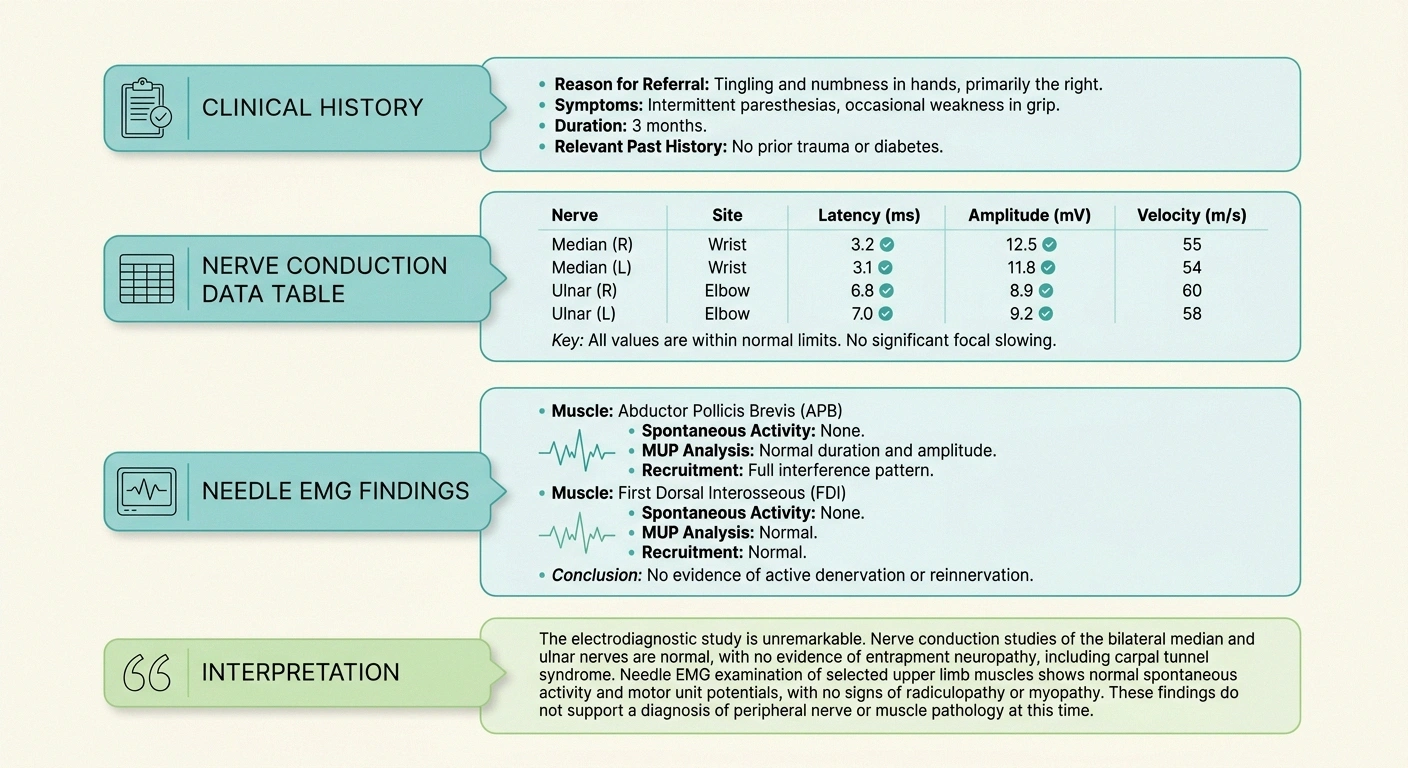
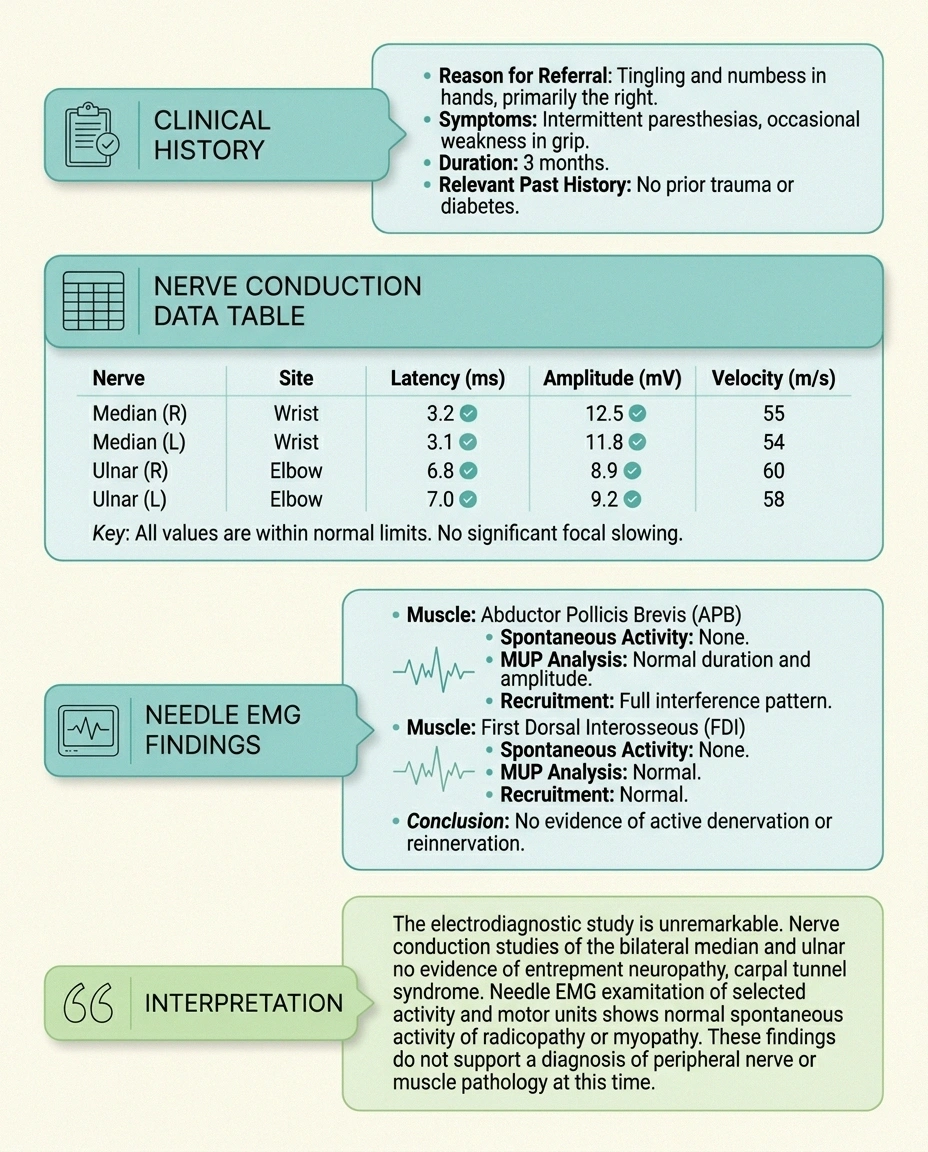
The first section is the clinical history. It contains your name, the date, the referring physician, and a short summary of why you were sent for testing. This part is not interpretation; it is context.
The second section is a table of nerve conduction data. This is usually the most intimidating block because it is wall-to-wall numbers. Each row is one nerve that was studied (median, ulnar, peroneal, tibial, sural, and so on). The columns show distal latency in milliseconds, amplitude in millivolts or microvolts, and conduction velocity in meters per second. Some reports also include F-wave latency and H-reflex latency rows.
The third section is the needle EMG findings. This is descriptive rather than tabular. It lists each muscle the neurologist sampled and what was observed at rest and during voluntary contraction. Words like “fibrillation potentials,” “positive sharp waves,” “polyphasic motor units,” and “reduced recruitment” live here.
The fourth and most important section is the interpretation. If you are short on time, read this last paragraph first. This is where the neurologist who performed the test pulls everything together into a clinical impression: “findings consistent with a length-dependent, primarily axonal, sensorimotor polyneuropathy” or something similar. The numbers above support this sentence; this sentence is what your treating neurologist will be working from.
Reading the Nerve Conduction Numbers
Three numbers do most of the work in the NCS table: amplitude, latency, and conduction velocity. Each one tells you something different about the nerve, and together they paint a picture of whether the problem is the nerve fiber itself or the protective coating around it.
| Measurement | Typical Normal Range | What Abnormal Suggests |
|---|---|---|
| Upper limb NCV | ≥50 m/s | Demyelination if markedly slowed |
| Lower limb NCV | ≥40 m/s | Demyelination, sometimes mixed |
| Sural sensory amplitude | ≥6 µV | Axonal sensory loss |
| Upper limb sensory amp. | ≥12 µV | Axonal sensory loss |
| F-wave (upper limb) | 25–32 ms | Demyelination, proximal lesion |
| F-wave (lower limb) | 45–56 ms | Demyelination, proximal lesion |
Always compare to your specific lab's printed reference range. Values vary by age, height, and limb temperature.
Amplitude is the height of the electrical wave that gets recorded. Think of it as the size of the response. It is measured in millivolts (mV) for motor responses and microvolts (µV) for sensory responses. A reduced amplitude usually means there are fewer working nerve fibers carrying the signal. As a rough reference point, a normal sural sensory amplitude is typically 6 µV or greater and upper limb sensory amplitudes are usually 12 µV or greater, though every lab uses its own reference range and you should always look at the “normal” column on your report rather than memorize numbers.
Distal latency is the time in milliseconds between when the stimulator fires and when the response shows up at the recording electrode closest to the muscle. Prolonged latency means the signal took too long to start, which usually points to a problem at the end of the nerve closest to the muscle, often the result of damage to the myelin sheath. If you want to understand what myelin actually is and why it matters, our piece on the myelin sheath in neuropathy goes into the biology in plain language.
Conduction velocity is how fast the signal traveled along the nerve, measured in meters per second. Healthy peripheral nerves in the arms typically conduct at 50 m/s or faster; in the legs the threshold is generally 40 m/s or faster. When velocity drops well below the lab's lower limit of normal, the report is telling you the signal is moving sluggishly through the nerve, which is the hallmark of demyelination.
The AANEM-style report will also flag whether the nerve studied was motor (controls movement) or sensory (carries sensation). Some neuropathies hit one type more than the other, which is why the distinction between motor versus sensory neuropathy shows up so often in interpretation paragraphs.
F-Waves and H-Reflexes: The “Late Responses”
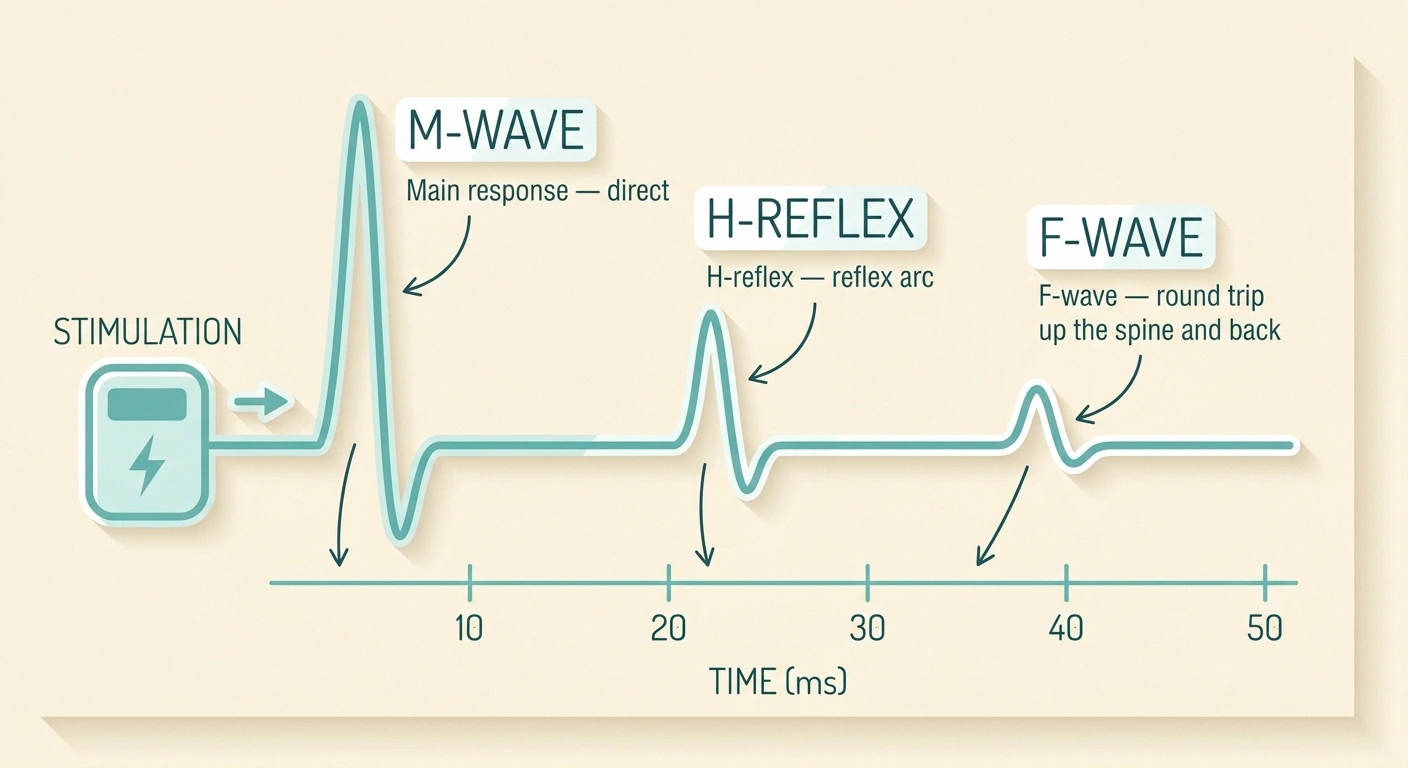
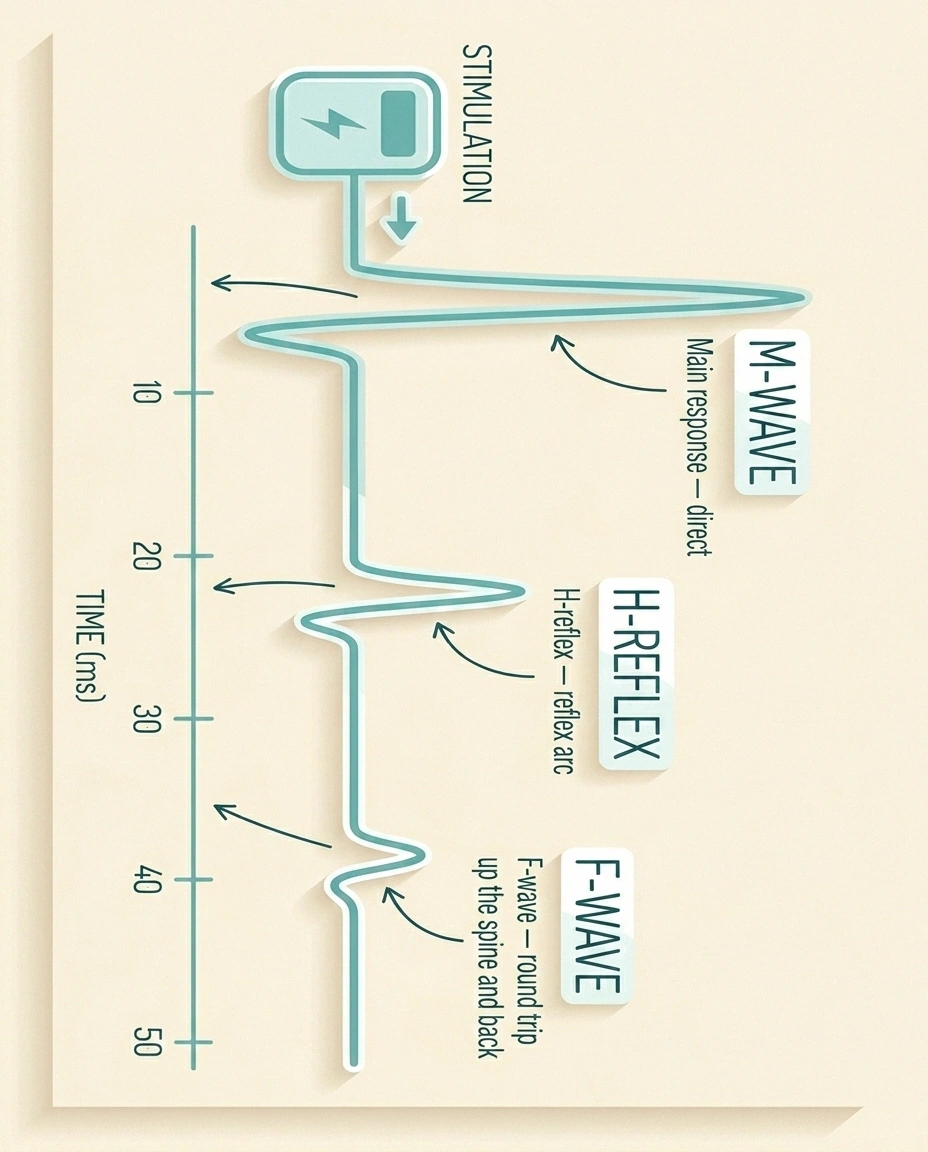
Many reports include two extra rows that confused me for years: F-wave latency and H-reflex latency. These are called “late responses” because they show up after the main wave on the recording.
An F-wave is a small signal that travels up the nerve toward the spinal cord and bounces back down. Because it covers the entire length of the nerve, it is excellent at picking up problems in the segments of the nerve that the standard NCS misses. Normal F-wave minimum latency is roughly 25–32 milliseconds in the upper extremities and about 45–56 milliseconds in the lower extremities, with side-to-side differences greater than one millisecond raising a flag. Prolonged F-wave latency is one of the earliest and most sensitive signs of demyelinating neuropathy, including CIDP and other inflammatory polyneuropathies.
An H-reflex is the electrical equivalent of the tap-the-knee reflex test, most commonly recorded in the calf. It evaluates the entire reflex arc, sensory nerve in and motor nerve out. A delayed or absent H-reflex on one side is often the first measurable sign of an S1 nerve root problem, and bilateral abnormality can support a diagnosis of polyneuropathy. Research summarized at PubMed Central on the F-wave index describes how these late responses become a useful early marker when standard parameters are still borderline normal.
Reading the Needle EMG Section

The needle EMG section reads more like a paragraph than a table. The neurologist describes each sampled muscle with phrases that follow a consistent grammar once you know what to look for.
The first half of each muscle entry covers what was happening at rest. A healthy muscle is electrically silent when relaxed. If the report mentions fibrillation potentials or positive sharp waves, the muscle was firing on its own. As described in the StatPearls reference on abnormal spontaneous EMG activity, fibrillations represent individual muscle fibers firing because they have lost their nerve supply. In neuropathy, this is the muscle telling you “the nerve I depend on is sick.”
Fasciculations are different. They are spontaneous discharges of an entire motor unit and they can occur in healthy people, particularly when fatigued or after caffeine. In isolation they are usually not alarming. In combination with widespread fibrillations and certain motor unit changes, they can suggest motor neuron disease, which is one reason your neurologist samples multiple muscles.
The second half of each muscle entry covers what happened when you contracted the muscle. The report will describe the motor unit action potentials, abbreviated MUAPs, in terms of size, duration, and shape. Large, long-duration, polyphasic motor units suggest reinnervation, where surviving nerve branches have grown to take over orphaned muscle fibers. Small, short-duration motor units point in a different direction, usually toward muscle disease.
Recruitment describes how motor units come online as you try harder. Reduced recruitment means few motor units are firing very fast, and it is a classic neurogenic finding consistent with a peripheral nerve problem. Early or rapid recruitment, where many units fire at low effort, is a myopathic pattern. For a deeper look at how length-dependent neuropathy distributes across muscles in the report, our guide to length-dependent neuropathy explains why the worst findings tend to cluster in the feet first.
Demyelinating Versus Axonal: The Pattern That Matters Most
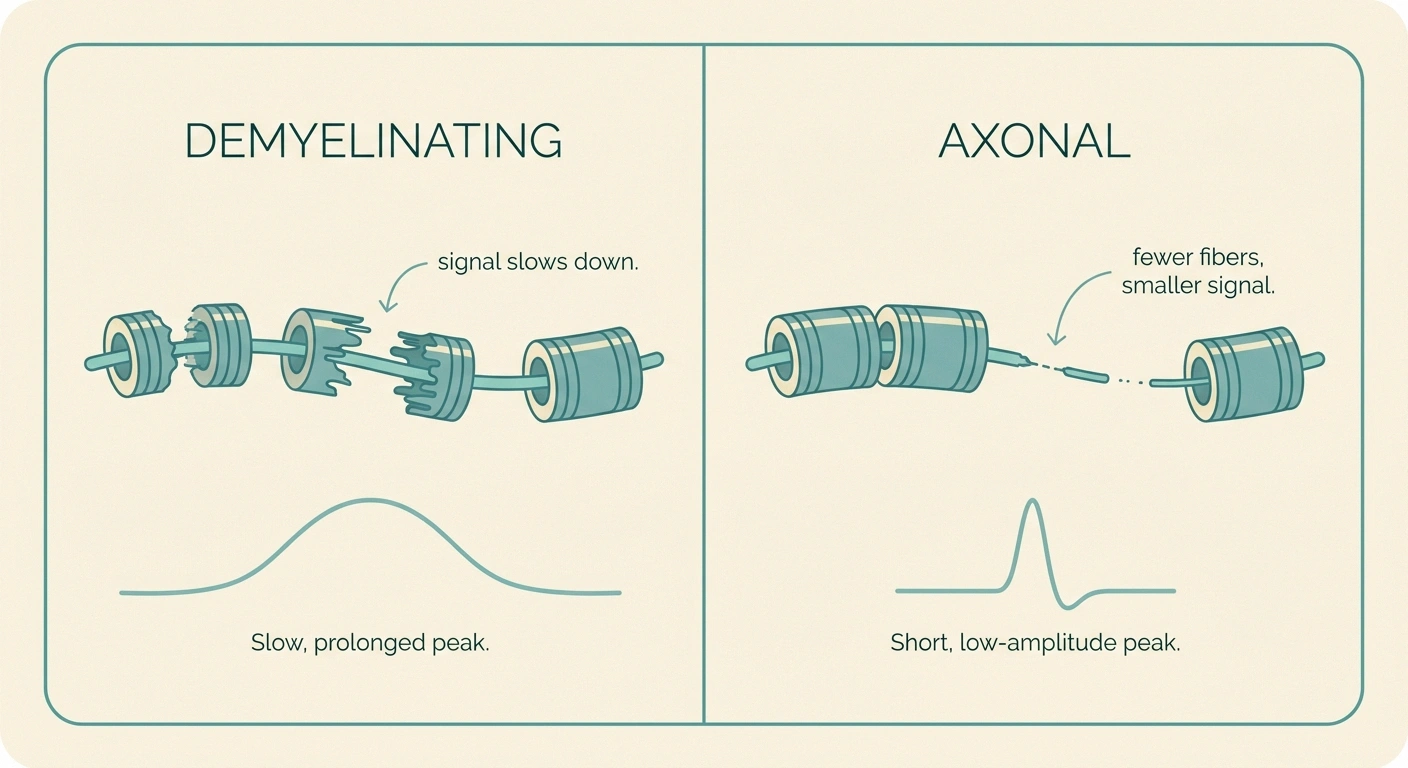
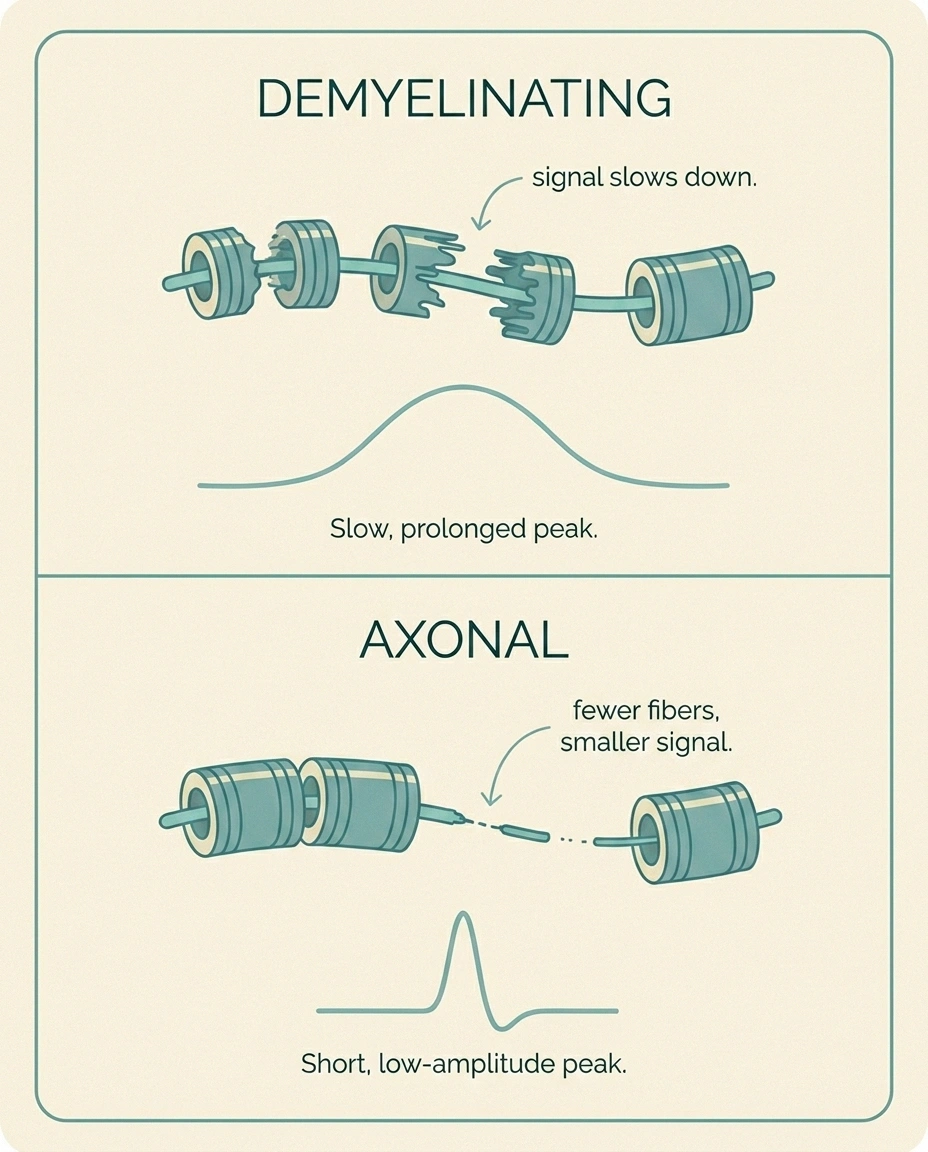
If there is one phrase that determines what your neurologist will do next, it is whether your report calls your neuropathy “demyelinating,” “axonal,” or “mixed.” This single distinction shapes the differential diagnosis, the treatment plan, and the urgency of follow-up. Our companion article on demyelinating versus axonal neuropathy goes deep into the biology; here is the short version of how the EMG/NCS report tells the two apart.
| Finding | Demyelinating | Axonal |
|---|---|---|
| Conduction velocity | Markedly slowed | Near normal |
| Amplitude | Often preserved early | Reduced |
| Distal latency | Prolonged | Near normal |
| F-wave latency | Prolonged | Near normal |
| Conduction block | May be present | Absent |
| Fibrillations on EMG | Few or none early | Common |
| Common causes | CIDP, GBS, hereditary | Diabetes, alcohol, chemo |
A demyelinating pattern shows up on the NCS as marked slowing of conduction velocity, prolonged distal latencies, prolonged F-wave latencies, and sometimes conduction block (a sudden drop in amplitude as the signal crosses a particular segment). On the needle EMG, demyelination by itself produces relatively few changes because the muscle fibers are still attached to their nerves; you may see only altered recruitment. The classic demyelinating pattern is most often seen in inherited neuropathies and in inflammatory neuropathies like CIDP and Guillain-Barré syndrome, where treatment can dramatically change the course.
An axonal pattern is the opposite picture. Conduction velocities are near normal or only mildly slowed, but amplitudes are reduced because the actual nerve fibers carrying the signal are dying off. On the needle EMG, axonal damage produces fibrillations at rest and large polyphasic motor units with reduced recruitment when you contract. The classic axonal pattern is what most people with diabetic, alcoholic, chemotherapy-induced, or idiopathic length-dependent polyneuropathy see on their report.
A mixed pattern shows features of both. Many chronic neuropathies start as one and develop the other over time, particularly demyelinating neuropathies where prolonged demyelination eventually causes secondary axonal loss. The interpretation paragraph will name which is the dominant feature.
A study published on PubMed Central documents that chronodispersion of F-wave latencies, the difference between maximal and minimal latency, is one of the most sensitive parameters for detecting demyelinating neuropathy, often catching abnormalities before standard nerve conduction velocity numbers cross the abnormal line. If your report includes F-wave studies, those rows can carry diagnostic weight beyond the headline conduction velocity.
What “Mild,” “Moderate,” and “Severe” Actually Mean
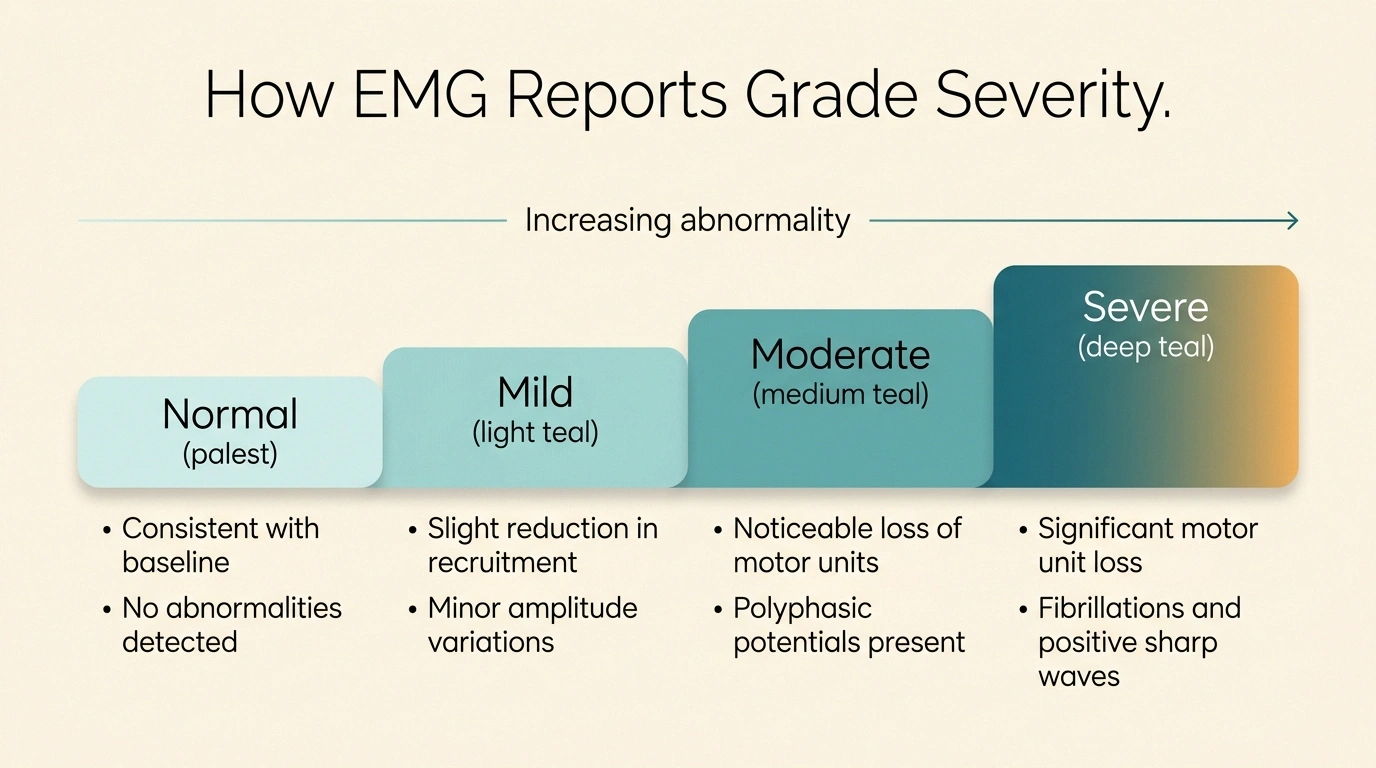
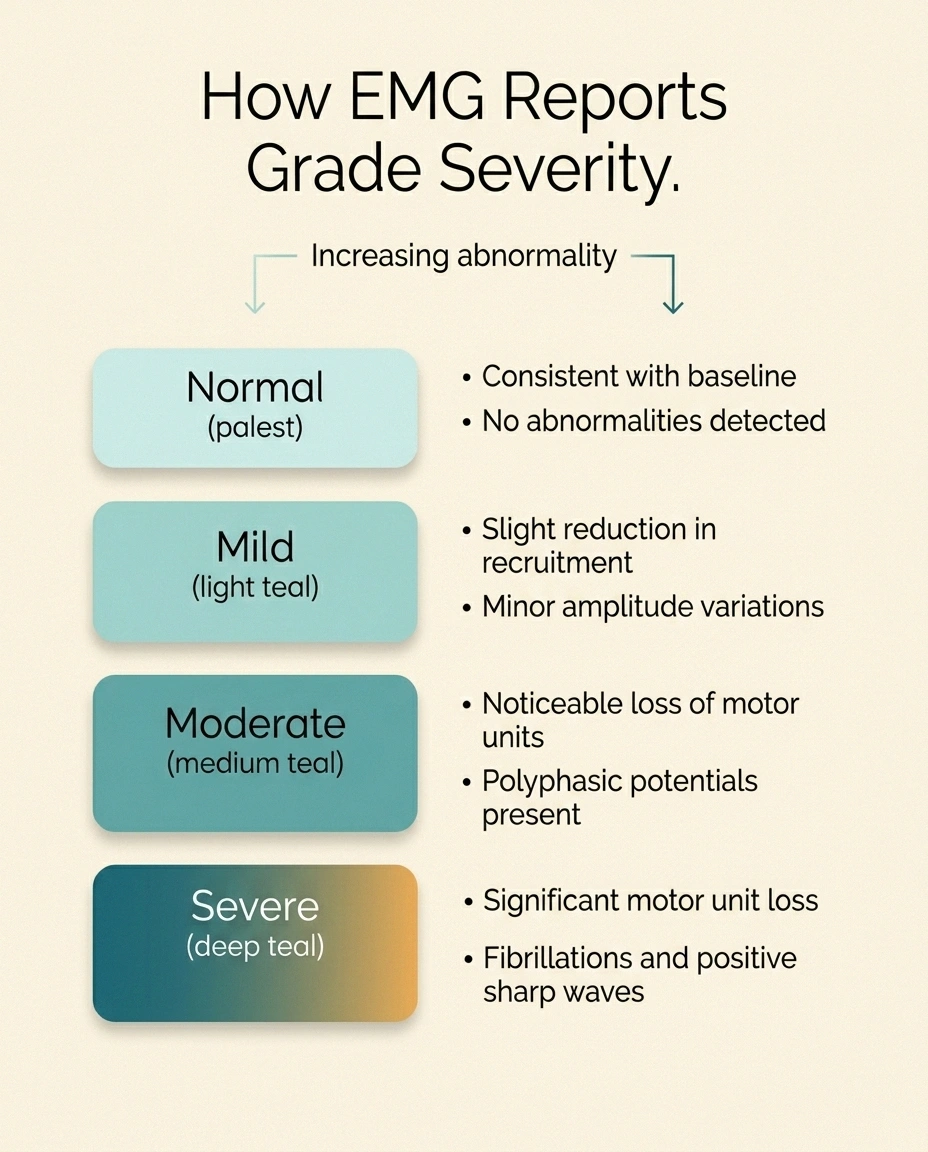
Most reports grade the abnormality somewhere on a four-step ladder: normal, mild, moderate, or severe. There is no universal cutoff, but in the laboratories I have seen, the words generally line up with how far the numbers fall outside the lab's reference range and how much of the limb is involved.
Mild generally means a small but real abnormality, often confined to the most distal part of the nerve. You may see slight slowing of conduction velocity, slightly reduced amplitude, or a few fibrillations in foot muscles only.
Moderate means abnormalities that are clearly outside the reference range, often involving more of the nerve and more muscles. Amplitudes may be reduced to half of normal or less; fibrillations may extend up the leg.
Severe means findings far outside the reference range, often including absent responses on some nerves and widespread denervation on the EMG. A nerve with “no response obtained” is one severity step beyond severe; the signal could not be recorded at all.
I want to gently note something here. A mild report does not always mean mild symptoms, and a normal report absolutely does not mean nothing is wrong. Which brings us to the most important warning in this whole article.
When the EMG Is Normal but Your Symptoms Are Not
This is the trap I want every patient to walk past. EMG and nerve conduction studies measure only the large, myelinated nerve fibers. They do not measure the small unmyelinated and thinly myelinated fibers that carry burning pain, temperature sensation, and most autonomic function. If your neuropathy is small fiber neuropathy, your EMG and NCS can be entirely normal.
A normal EMG and nerve conduction study does not rule out neuropathy. These tests measure only large, myelinated nerve fibers. If you have burning pain, temperature changes, or autonomic symptoms with a normal report, ask your neurologist about small fiber neuropathy testing — skin biopsy for intraepidermal nerve fiber density or quantitative sensory testing. Many patients are sent home with a normal EMG and a real, treatable small fiber neuropathy that was simply not measured.
Multiple peer-reviewed studies confirm this. The PubMed entry on quantitative sensory testing in small fiber neuropathy documents that NCS and EMG were normal in patients with clinically diagnosed small fiber neuropathy and that QST or skin biopsy was needed to make the diagnosis. If your report says “no electrodiagnostic evidence of large fiber neuropathy” but you are still living with burning, tingling, or temperature changes in your feet, ask your neurologist whether small fiber neuropathy needs to be evaluated separately. A normal EMG is not the end of the conversation; it is sometimes the start of a different one.
Questions to Bring to Your Follow-Up Appointment
The single most useful thing I do with my own report is sit down the night before my neurologist appointment, read the interpretation paragraph slowly, and write down questions. Here is the list I built for myself over time. Not all of these will apply to every report, but most will get you a more productive conversation. For more on getting the most out of these visits, our guide on how to talk to your doctor about neuropathy covers the broader skill of advocating for yourself in the exam room.
- Is the pattern in my report demyelinating, axonal, or mixed, and what does that mean for my diagnosis?
- Are my findings consistent with my symptoms, or is there a mismatch I should know about?
- Could small fiber neuropathy explain symptoms not captured by this test?
- What is the most likely cause of this pattern in my case?
- Are there blood tests, skin biopsy, or imaging I should have next?
- How severe is what you are seeing, and is it progressing?
- Should I see a neuromuscular subspecialist?
- When should I repeat this test to track progression?
- What treatment options are appropriate given this specific pattern?
Walk in with the report in hand, the questions written out, and a willingness to ask “can you say that in plain language?” if you do not understand the answer. A good neurologist welcomes the engagement. If your current one does not, our piece on choosing a neurologist for neuropathy covers how to find one who does.
What to Do If Your Results Are Inconclusive or Surprising

Sometimes the report does not deliver a clean answer. Common patterns I see in our community include: borderline numbers in the equivocal zone between normal and mild abnormality; a pattern that does not match the symptom story; or findings that point to something the referring doctor was not expecting.
Your EMG report is a starting point, not a verdict. Read the interpretation paragraph first. Compare your numbers to the lab's reference range. Look for the words demyelinating, axonal, or mixed. Bring your questions written down. And remember: a normal EMG does not rule out neuropathy if your symptoms are real. The interpretation is your neurologist's job. Asking better questions is yours.
If the numbers are borderline, ask whether repeating the test in six to twelve months would clarify the trajectory. Neuropathy is often a moving target, and a second study compared to the first can show progression that a single study cannot.
If the pattern does not match your symptoms, ask whether additional testing is warranted. Skin biopsy for small fiber neuropathy, autonomic testing, blood work for treatable causes (B12, glucose tolerance, thyroid, paraprotein, immune markers), genetic testing if inherited neuropathy is suspected, or imaging of the spine if a radiculopathy is hidden in the picture.
If the findings point somewhere unexpected, particularly toward an inflammatory or hereditary process, ask about referral to a neuromuscular subspecialist. Conditions like CIDP have time-sensitive treatment options that improve outcomes when caught early, and the difference between “saw a general neurologist” and “saw a neuromuscular specialist” is sometimes the difference between a working diagnosis and the right diagnosis.
I will close where I started. The day my own report came home, I did not understand a word of it. The next day, after a long morning with a printed copy and a notepad, I had a list of questions and the beginnings of a vocabulary. The week after that, I had a conversation with my neurologist that finally felt like a conversation. Your report is not a verdict written in a foreign language. It is a starting point. You hold it in your hands. The next move is yours.
Frequently Asked Questions
Can I read my own EMG report without a doctor?
You can read it for context and to prepare better questions, but you cannot interpret it. EMG and NCS results are pattern-based and require clinical correlation with your symptoms, your physical exam, and the lab's specific reference ranges. Your role is to understand the vocabulary so the conversation with your neurologist is more productive. The interpretation belongs to a trained electromyographer.
What does “abnormal spontaneous activity” mean on an EMG report?
It usually refers to fibrillation potentials and positive sharp waves, which are signs that muscle fibers are firing on their own because they have lost contact with their nerve. In the context of peripheral neuropathy, this typically points to axonal damage. The location and density of these findings help the neurologist judge severity and distribution.
Is a slow nerve conduction velocity always serious?
Not always. Mild slowing can be related to age, height, low limb temperature during the test, or a borderline finding that needs follow-up. Marked slowing, particularly when combined with prolonged latencies and conduction block, is more concerning and points to demyelination. The lab compares your numbers to its own reference ranges, and your neurologist interprets them in context.
Can my EMG be normal if I have neuropathy?
Yes. Standard EMG and NCS measure only large, myelinated fibers and miss small fiber neuropathy entirely. If you have burning pain, temperature changes, or autonomic symptoms with a normal EMG, ask your neurologist about skin biopsy for intraepidermal nerve fiber density or quantitative sensory testing. A normal EMG rules out large fiber neuropathy; it does not rule out neuropathy.
What is the difference between an axonal and a demyelinating pattern?
Axonal patterns show reduced amplitudes with relatively preserved conduction velocity, plus fibrillations and large motor units on needle EMG. Demyelinating patterns show marked slowing of conduction velocity, prolonged distal and F-wave latencies, and sometimes conduction block, with relatively preserved amplitudes early on. The distinction matters because demyelinating neuropathies often have specific, time-sensitive treatments.
What are F-waves and H-reflexes for?
Both are late responses that travel longer distances than standard nerve conduction signals. F-waves cover the full length of a motor nerve and are sensitive to demyelination, particularly proximal demyelination that standard testing can miss. H-reflexes evaluate the reflex arc and are useful for detecting S1 radiculopathy and supporting a diagnosis of polyneuropathy.
How accurate is an EMG for diagnosing neuropathy?
EMG and NCS are highly accurate for large fiber peripheral neuropathies, with strong sensitivity and specificity for axonal and demyelinating patterns. They are not accurate for small fiber neuropathy and they do not always pick up very early or very mild large fiber damage. The test is one piece of a clinical picture that also includes your history, exam, and bloodwork.
Should I ask for a copy of my EMG report?
Yes, always. Request a full copy including the data tables, the needle EMG findings, and the interpretation paragraph. Keep it with your medical records. If you ever change neurologists or need a second opinion, the original report is the most useful single document you can hand a new clinician.