If you've been through a nerve conduction study or had a detailed conversation with a neurologist about your neuropathy, you may have heard words like “axonal” or “demyelinating” — and felt like you'd wandered into a foreign language course without the textbook.
I remember that feeling well. My first neurologist handed me a report with terms I couldn't pronounce, let alone explain to my husband when I got home. It took me months of research to understand that these weren't just technical labels — they described fundamentally different types of nerve damage, with different causes, different prognoses, and sometimes different treatment approaches.
Today I want to give you the clear explanation I wish I'd had earlier. Understanding whether your neuropathy is axonal, demyelinating, or both is genuinely useful knowledge — it helps you ask better questions and understand why your doctors are recommending what they're recommending.
A Quick Anatomy Lesson: The Parts of a Nerve
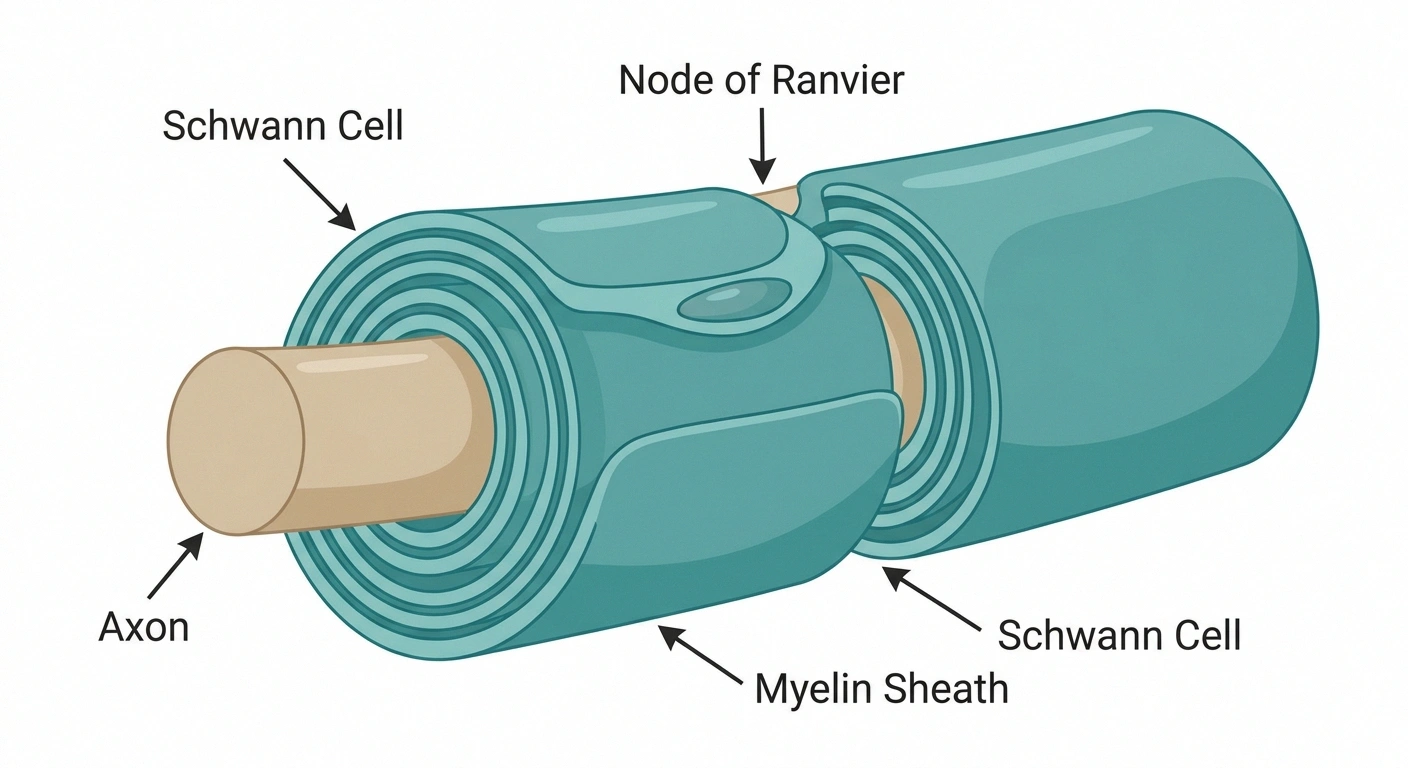
To understand the difference, you need to picture what a peripheral nerve actually looks like. Think of a single nerve fiber like an electrical cable. It has two key parts:
Key Concept
Axon = the wire. Myelin = the insulation.
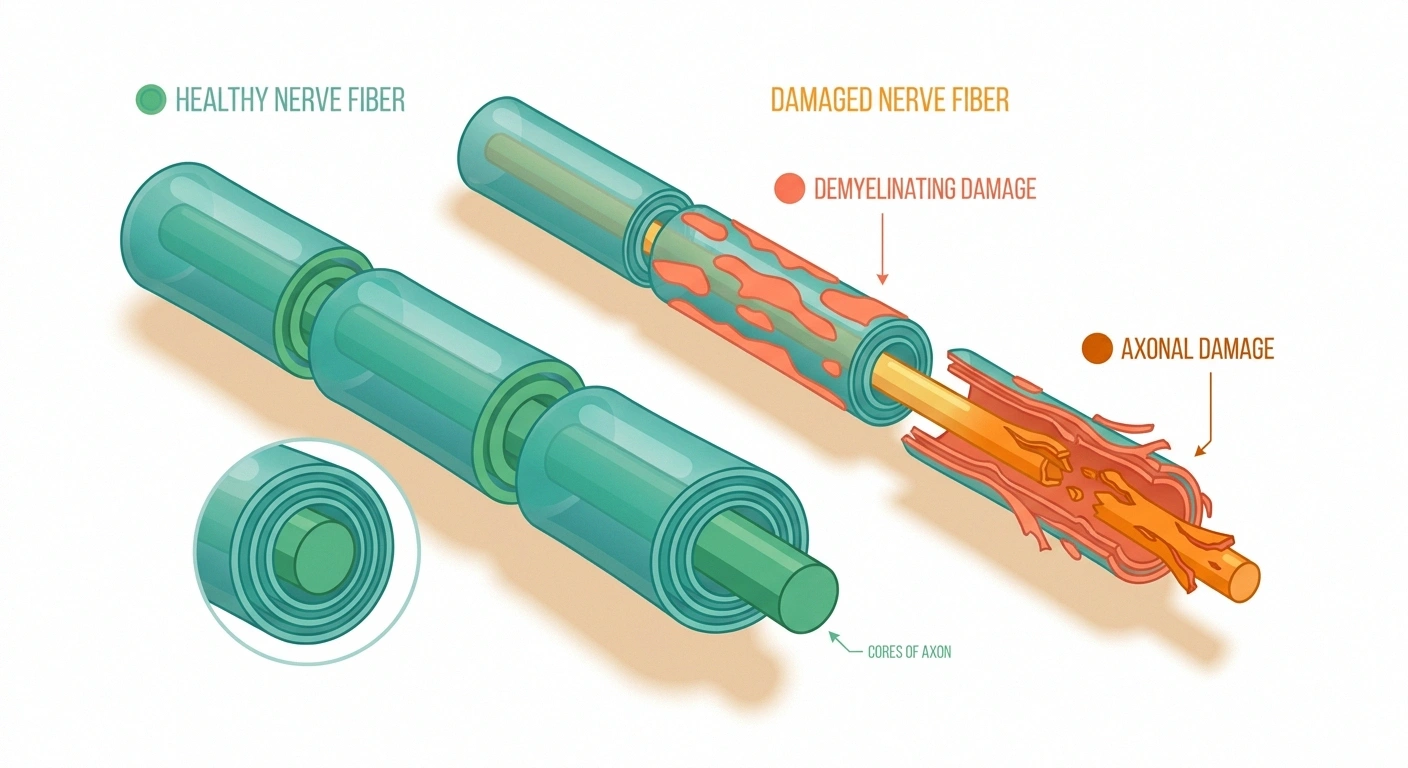
Axonal neuropathy damages the wire itself. Demyelinating neuropathy strips the insulation. Both disrupt the electrical signals your nerves send — but through different mechanisms with different implications for treatment and recovery.
The axon is the actual wire — the long fiber that carries electrical signals from point A to point B. It's the core of the nerve fiber, and it's what does the actual work of transmitting sensation and motor commands.
The myelin sheath is the insulation wrapped around the axon. It's made from specialized cells that spiral around the axon in layers, creating a protective coating. But myelin does more than just protect — it dramatically speeds up signal transmission through a process called saltatory conduction. Without it, nerve signals travel much more slowly.
Both of these components can be damaged in neuropathy. When the axon itself is attacked, that's axonal neuropathy. When the myelin sheath is the target, that's demyelinating neuropathy. And sometimes — in a scenario that's particularly complex — both happen at once. Understanding this difference is at the heart of understanding your own peripheral neuropathy.
Axonal Neuropathy: When the Wire Gets Damaged
Axonal neuropathy is the more common of the two types. In fact, the most prevalent form of neuropathy in the world — diabetic peripheral neuropathy — is primarily an axonal process. The axons themselves are gradually damaged or destroyed, while the myelin sheath may initially remain intact.
Common causes of axonal neuropathy include:
- Diabetes and prediabetes — the most common cause worldwide. High blood sugar generates oxidative stress that damages axons over time.
- Alcohol toxicity — chronic heavy drinking directly damages peripheral axons.
- Chemotherapy — certain chemotherapy drugs are neurotoxic to axons (see chemotherapy-induced neuropathy).
- Nutritional deficiencies — particularly B12 deficiency, which is essential for axon maintenance.
- Kidney disease (uremia) — toxin buildup can damage axons.
- Lyme disease — the Borrelia bacteria can trigger axonal damage.
- Hereditary forms — Charcot-Marie-Tooth type 2 and related conditions (see our article on hereditary neuropathy).
What axonal neuropathy feels like: Symptoms are typically length-dependent — meaning they start in the feet (the longest nerve fibers) and work their way up the legs over time. Sensory symptoms include numbness, tingling, burning, or loss of vibration and temperature sense. Motor involvement (weakness) occurs in more severe cases.
Demyelinating Neuropathy: When the Insulation Is Attacked
Demyelinating neuropathy occurs when the myelin sheath is damaged, stripped away, or fails to form properly. When myelin is lost, nerve signals slow dramatically and can become erratic. The axon itself may survive for a period — but if demyelination is severe or prolonged, secondary axonal damage eventually follows.
Common causes of demyelinating neuropathy include:
- Autoimmune attack — the immune system mistakenly targets myelin proteins. This is the mechanism in CIDP (chronic inflammatory demyelinating polyneuropathy) and the AIDP form of Guillain-Barré syndrome.
- POEMS syndrome — a rare plasma cell disorder associated with demyelinating neuropathy.
- Hereditary forms — Charcot-Marie-Tooth type 1 (the demyelinating subtype) involves mutations affecting myelin proteins.
- HIV infection — can trigger both inflammatory demyelination and direct axonal damage.
- Certain medications — a small number of drugs have been associated with demyelinating neuropathy.
What demyelinating neuropathy feels like: Symptoms may be less strictly length-dependent than axonal forms. Slowing of conduction can cause weakness, loss of reflexes, difficulty with coordination, and sensory changes throughout the limbs. In acute cases like GBS, progression can be rapid.
How Doctors Tell the Difference: EMG and Nerve Conduction Studies

This is where the EMG and nerve conduction study becomes your diagnostic map. These tests directly measure how your nerve fibers are functioning — and the patterns they reveal can tell a trained neurologist which type of damage is present.
What the EMG Shows
Axonal Pattern
- Reduced signal amplitude
- Near-normal speed
- Fibrillations on needle EMG
- Denervation in muscle
Demyelinating Pattern
- Markedly slowed speed
- Prolonged latencies
- Absent/prolonged F-waves
- No fibrillations (pure)
In axonal neuropathy, the NCS typically shows:
- Reduced amplitude of nerve signals (the “height” of the waveform is lower because fewer axons are conducting)
- Relatively normal conduction velocity (the signals that do travel are moving at a normal speed)
- On EMG: fibrillations and positive sharp waves (signs of denervation — the muscle is no longer receiving input from its nerve)
In demyelinating neuropathy, the NCS typically shows:
- Markedly slowed conduction velocity (signals are taking much longer to travel because the myelin insulation is gone)
- Prolonged distal motor latency (extra time for the signal to reach the muscle)
- Prolonged or absent F-waves (late responses that reflect conduction through proximal nerve segments)
- Temporal dispersion or conduction block (signals becoming dispersed or failing entirely at specific nerve segments)
- On EMG: reduced recruitment but typically NO fibrillations in pure demyelinating (the axons are still alive)
The distinction matters clinically because it guides the diagnostic search. A demyelinating pattern in an adult without obvious cause should trigger a workup for autoimmune conditions. An axonal pattern in a middle-aged patient with type 2 diabetes is almost certainly diabetic neuropathy until proven otherwise.
Can You Have Both? Mixed Neuropathy Explained
Yes — and this is more common than many patients realize. Mixed axonal-demyelinating neuropathy refers to a pattern where both types of damage are present simultaneously.
One important mechanism for this: when demyelinating neuropathy goes untreated, the axons underneath eventually begin to suffer from the chronic loss of myelin support. What started as a purely demyelinating condition accumulates axonal damage over time. This is why the prognosis for demyelinating neuropathy worsens significantly when axon loss is also present on NCS.
Mixed patterns can also occur in conditions like vasculitic neuropathy, certain hereditary neuropathies, and in advanced CIDP. Your neurologist may describe your NCS report as showing “predominantly axonal” or “predominantly demyelinating” with features of both.
Prognosis: Which Type Recovers Better?
This is the question people ask most urgently — and the honest answer requires some nuance.
Critical Timing Point
Untreated demyelinating neuropathy becomes axonal over time.
The prognosis for demyelinating neuropathy — including CIDP — depends heavily on how much axonal damage has accumulated before treatment begins. The longer immune-mediated demyelination goes unchecked, the more axons are lost beneath the damaged myelin, and recovery potential drops significantly.
Demyelinating neuropathy has better recovery potential, but with an important condition: it needs to be caught and treated before significant secondary axonal damage accumulates. The myelin sheath can regenerate. Schwann cells (the myelin-producing cells in the peripheral nervous system) can repair and rebuild damaged myelin sheaths, sometimes with near-complete recovery of function.
This is why conditions like GBS, which is a rapid-onset autoimmune demyelinating neuropathy, can produce near-complete recovery in many patients when treated promptly — even though the acute presentation can be terrifying.
CIDP, the chronic form, typically requires ongoing treatment to prevent relapse and axonal damage accumulation. With appropriate management (IVIG, plasmapheresis, or corticosteroids), many CIDP patients can maintain stable or improved function.
Axonal neuropathy has slower, less complete recovery. Peripheral axons can regrow, but only at approximately 1 millimeter per day — an excruciatingly slow process. For someone with axonal damage that extends from the spinal cord to the foot, complete regeneration is unlikely. The most realistic treatment goal is often stopping progression and optimizing function, rather than reversal.
There's an important nuance here: the degree of axonal injury in a demyelinating neuropathy is the strongest predictor of long-term outcome. A patient with CIDP who has preserved axon amplitudes on NCS will generally recover better than one with the same demyelinating pattern but significantly reduced CMAP amplitudes (indicating that axons are also being lost).
Treatment: Does the Type Change What's Prescribed?

Yes — and significantly so for autoimmune demyelinating neuropathy.
Treatment Approach by Type
Autoimmune Demyelinating (CIDP, GBS)
Disease-modifying: IVIG, plasmapheresis, corticosteroids — target the immune attack on myelin
Axonal Neuropathy (Diabetic, Toxic, etc.)
Remove the cause + symptomatic management (gabapentin, duloxetine, physical therapy). No equivalent disease-modifying therapy for most types.
Autoimmune demyelinating neuropathy (CIDP, GBS): These conditions respond to immune-modulating treatments that most axonal neuropathies don't respond to at all. IVIG, plasma exchange (plasmapheresis), and corticosteroids can halt or reverse the autoimmune attack on myelin. These aren't just symptomatic treatments — they're disease-modifying interventions that address the underlying process. The fact that something is being done about the cause is what allows recovery to occur.
Axonal neuropathy: For most acquired axonal neuropathies, there's no equivalent disease-modifying treatment. The primary approach is to:
- Identify and treat the underlying cause (control blood sugar in diabetic neuropathy, stop the offending medication, address nutritional deficiencies)
- Manage symptoms with appropriate medications (gabapentin, duloxetine, tricyclic antidepressants, topical agents)
- Protect function with physical therapy and fall prevention strategies
Both types may use similar symptomatic pain management medications — the distinction in treatment approach applies mainly to disease-modifying interventions. If you're trying to understand your treatment options, our complete guide to types of neuropathy provides a broader framework for navigating these conversations with your doctor.
Small Fiber Neuropathy: How Does It Fit In?

You may have heard about small fiber neuropathy and wondered how it fits into the axonal/demyelinating framework. Small fiber neuropathy primarily affects the smallest unmyelinated (C-fiber) and thinly myelinated (A-delta) nerve fibers, which are responsible for pain, temperature sensation, and autonomic function.
Axon Regeneration Rate
~1 mm
per day
For someone with axonal damage extending from the spine to the foot (roughly 1 meter), complete regeneration would theoretically require nearly 3 years — and is rarely complete in practice. This is why stopping progression early matters more than recovery timelines.
Because these fibers are unmyelinated or only lightly myelinated, they're largely invisible on standard nerve conduction studies (which primarily test larger myelinated fibers). Small fiber neuropathy requires different diagnostic testing — typically a skin punch biopsy to count intraepidermal nerve fiber density. It's considered an axonal process affecting small fibers specifically, with symptoms that often feel different from classic large-fiber neuropathy.
Questions to Ask Your Neurologist

Armed with this understanding, here are some questions worth bringing to your next appointment:
- Does my NCS/EMG show an axonal pattern, demyelinating pattern, or mixed?
- If there's a demyelinating pattern, has an autoimmune cause been ruled out?
- How much axonal loss is present, and what does that mean for recovery potential?
- Is my condition progressive, stable, or showing signs of improvement?
- Are there disease-modifying treatments appropriate for my specific type?
If you're preparing for a neurology appointment, our guide on how to prepare for your neurology appointment has a fuller list of questions and strategies for making the most of that visit.
The Bottom Line
The distinction between axonal and demyelinating neuropathy isn't just medical jargon — it's a meaningful difference in mechanism, prognosis, and treatment approach. Axonal neuropathy (the more common type, including most diabetic neuropathy) involves damage to the nerve fiber itself, with limited recovery potential and management focused on stopping the cause. Demyelinating neuropathy involves damage to the insulating myelin sheath, often autoimmune in origin, with better recovery potential when caught and treated early.
Understanding which type you're dealing with — or whether you have a mixed picture — helps you make sense of your test results, understand your prognosis more clearly, and participate more actively in decisions about your care. That understanding is one of the most valuable things you can carry into every conversation with your medical team.
FAQ: Demyelinating vs Axonal Neuropathy
What is the main difference between axonal and demyelinating neuropathy?
Axonal neuropathy involves damage to the axon, which is the nerve fiber that carries electrical signals. Demyelinating neuropathy involves damage to the myelin sheath, the protective insulating coating around the axon. Axonal damage reduces the number of functioning nerve fibers. Demyelinating damage slows signal conduction dramatically. Both types affect how nerves function, but through different mechanisms with different treatment implications.
Which type of neuropathy is worse?
Neither is universally worse, but they have different outlooks. Demyelinating neuropathy often has better recovery potential because myelin can regenerate — but only if treated before secondary axonal loss occurs. Axonal neuropathy tends to recover more slowly and incompletely because axon regeneration is very slow. The degree of axonal loss is the strongest predictor of long-term outcome in both types.
Can demyelinating neuropathy become axonal?
Yes. This is one of the most important reasons to treat demyelinating neuropathy promptly. When demyelinating damage is severe or prolonged, the axons beneath the damaged myelin eventually begin to suffer. What starts as a purely demyelinating condition can accumulate axonal damage over time, worsening prognosis. This is particularly relevant in CIDP, where delayed treatment can lead to irreversible axonal loss.
Is diabetic neuropathy axonal or demyelinating?
Diabetic peripheral neuropathy is predominantly axonal. High blood sugar generates oxidative stress that directly damages peripheral axons. While some degree of segmental demyelination can occur in advanced diabetic neuropathy, the primary process is axonal degeneration. This is reflected on nerve conduction studies, which typically show reduced nerve amplitudes with relatively preserved conduction velocities in diabetic neuropathy.
How does an EMG tell the difference between axonal and demyelinating neuropathy?
On nerve conduction studies, demyelinating neuropathy shows markedly slowed conduction velocities, prolonged distal latencies, and prolonged or absent F-waves. Axonal neuropathy shows reduced amplitudes with near-normal velocities. On the needle EMG portion, axonal damage produces fibrillations and positive sharp waves in muscles, indicating the muscle has lost its nerve input. Pure demyelinating neuropathy typically does not produce these denervation findings.
What conditions cause demyelinating neuropathy?
The most common causes include autoimmune conditions (CIDP and GBS are the most prevalent), hereditary forms (Charcot-Marie-Tooth type 1 and related inherited demyelinating neuropathies), POEMS syndrome, and HIV-associated neuropathy. Some medications have also been associated with demyelinating neuropathy as a rare adverse effect.
Can you recover from demyelinating neuropathy?
Recovery is possible and often good, particularly when treatment begins before significant secondary axonal loss occurs. In Guillain-Barre syndrome, most patients achieve significant recovery with appropriate treatment. CIDP patients can often maintain stable or improving function with ongoing treatment. The degree of axonal involvement at the time of treatment initiation is the most important factor influencing outcome.
What is mixed axonal-demyelinating neuropathy?
Mixed neuropathy shows features of both axonal and demyelinating damage on electrodiagnostic testing. This can occur when a demyelinating neuropathy has progressed to the point of secondary axonal damage, in conditions that independently cause both types (such as vasculitic neuropathy), or in hereditary neuropathies with complex patterns. The presence of axonal loss in a primarily demyelinating neuropathy generally worsens the prognosis compared to pure demyelinating damage.