Neuropathy Types Explained: A Complete Guide
The phrase “types of neuropathy” sounds simple until you start looking it up. Then suddenly you are seeing peripheral, autonomic, focal, proximal, sensory, motor, small fiber, diabetic, idiopathic, hereditary, mononeuropathy, polyneuropathy — and it feels like everyone is using a different map.
Here is the cleanest way to understand it: neuropathy can be classified in more than one way at the same time. A person can have diabetic peripheral neuropathy that is mostly sensory and follows a length-dependent pattern. None of those labels cancel each other out. They describe different parts of the same picture.
How Doctors Classify Neuropathy
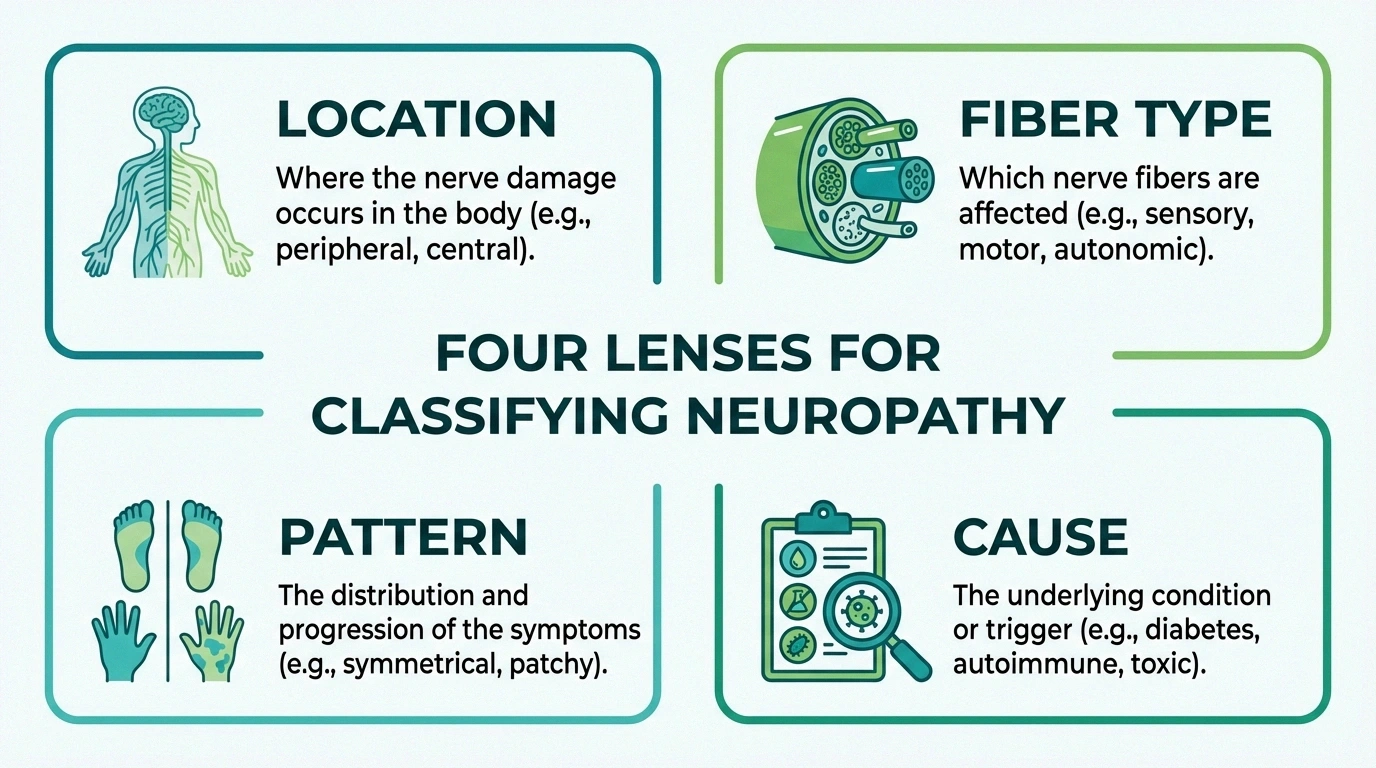
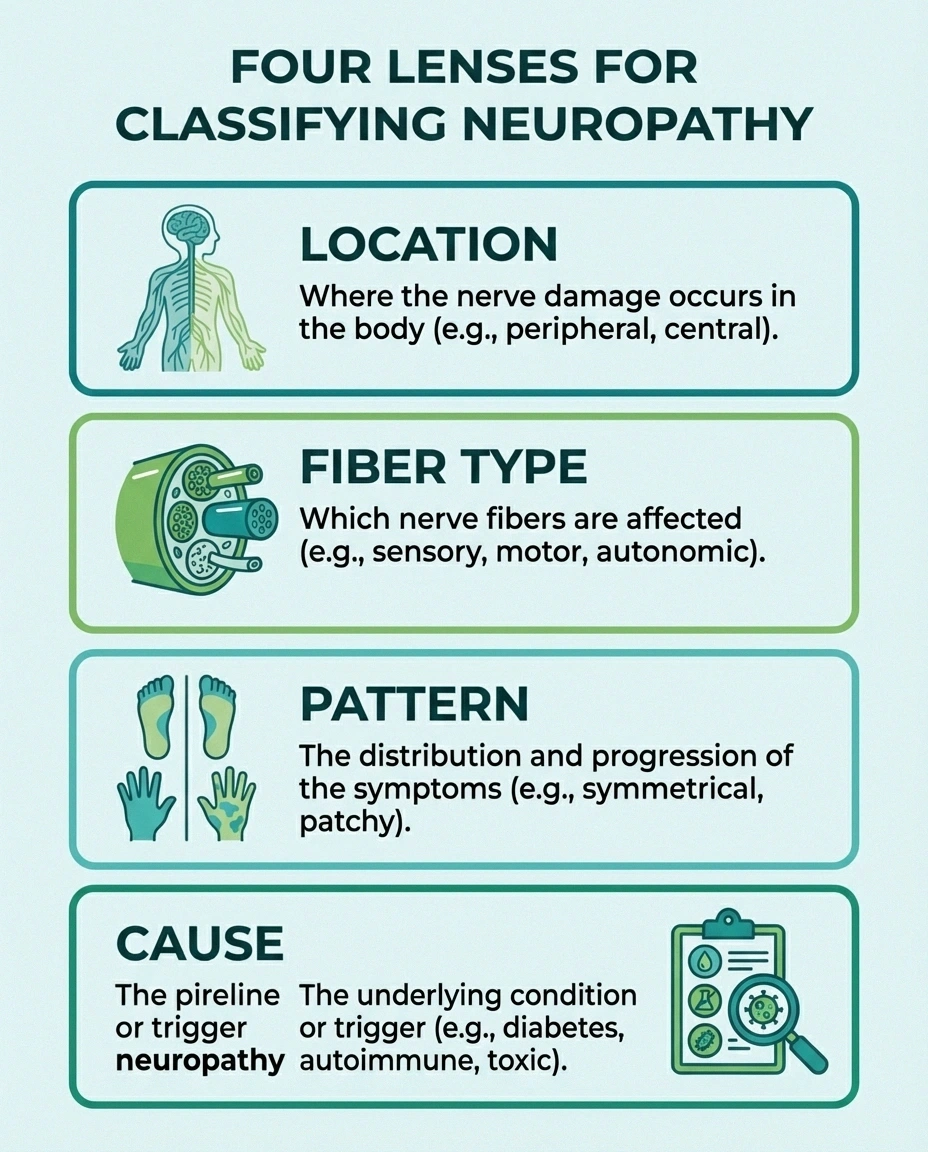
Most neuropathy diagnoses are sorted using four big lenses:
Location, fiber type, pattern, and cause — that is the fastest way to untangle a neuropathy label
- Where the nerve problem is located — peripheral, focal, proximal, cranial, autonomic
- What kind of nerve fibers are affected — sensory, motor, autonomic, or mixed
- How the pattern behaves — one nerve, many nerves, length-dependent, sudden, progressive, symmetric, asymmetric
- What is causing it — diabetes, toxins, autoimmune disease, chemotherapy, vitamin deficiency, heredity, compression, and more
That is the leverage point. When you understand which lens a doctor is using, the diagnosis stops sounding contradictory and starts sounding structured.
The Four Broad Patterns People Hear About Most
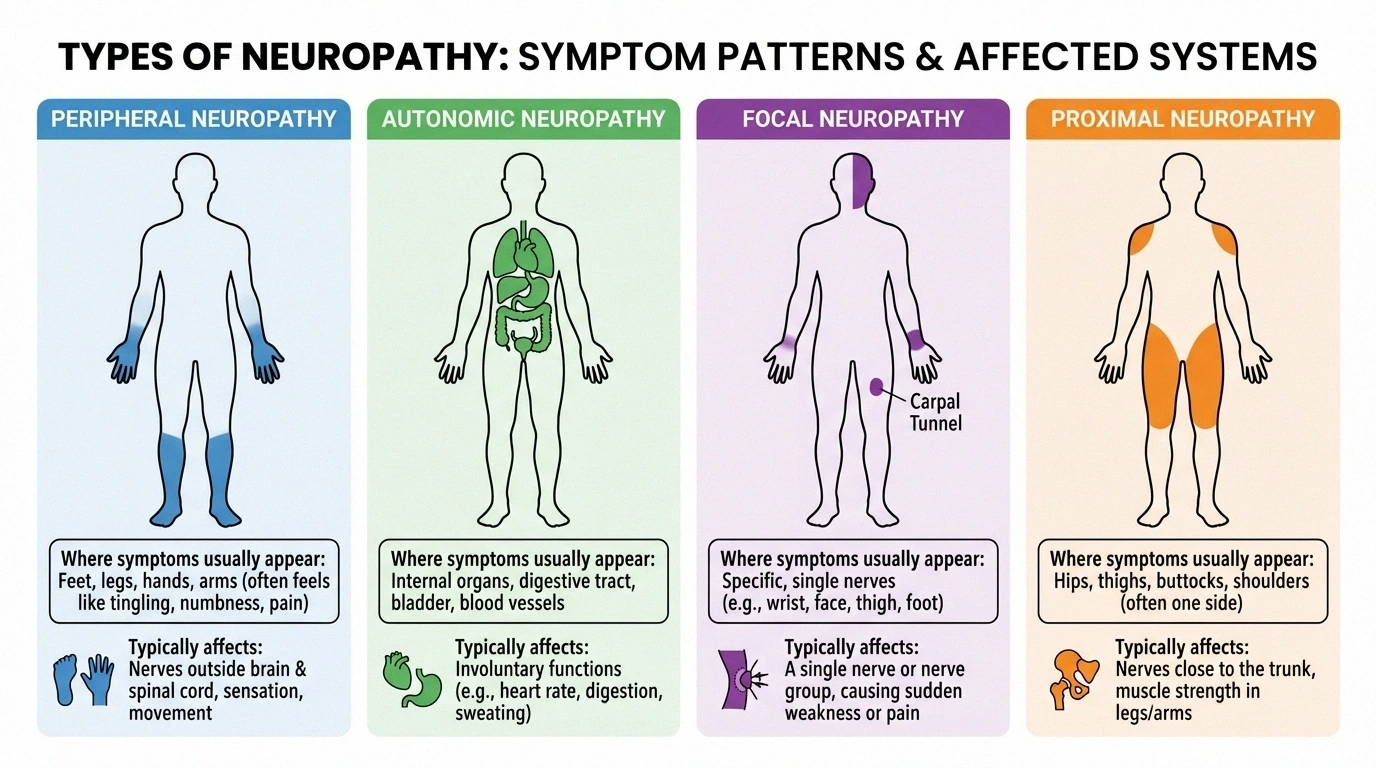
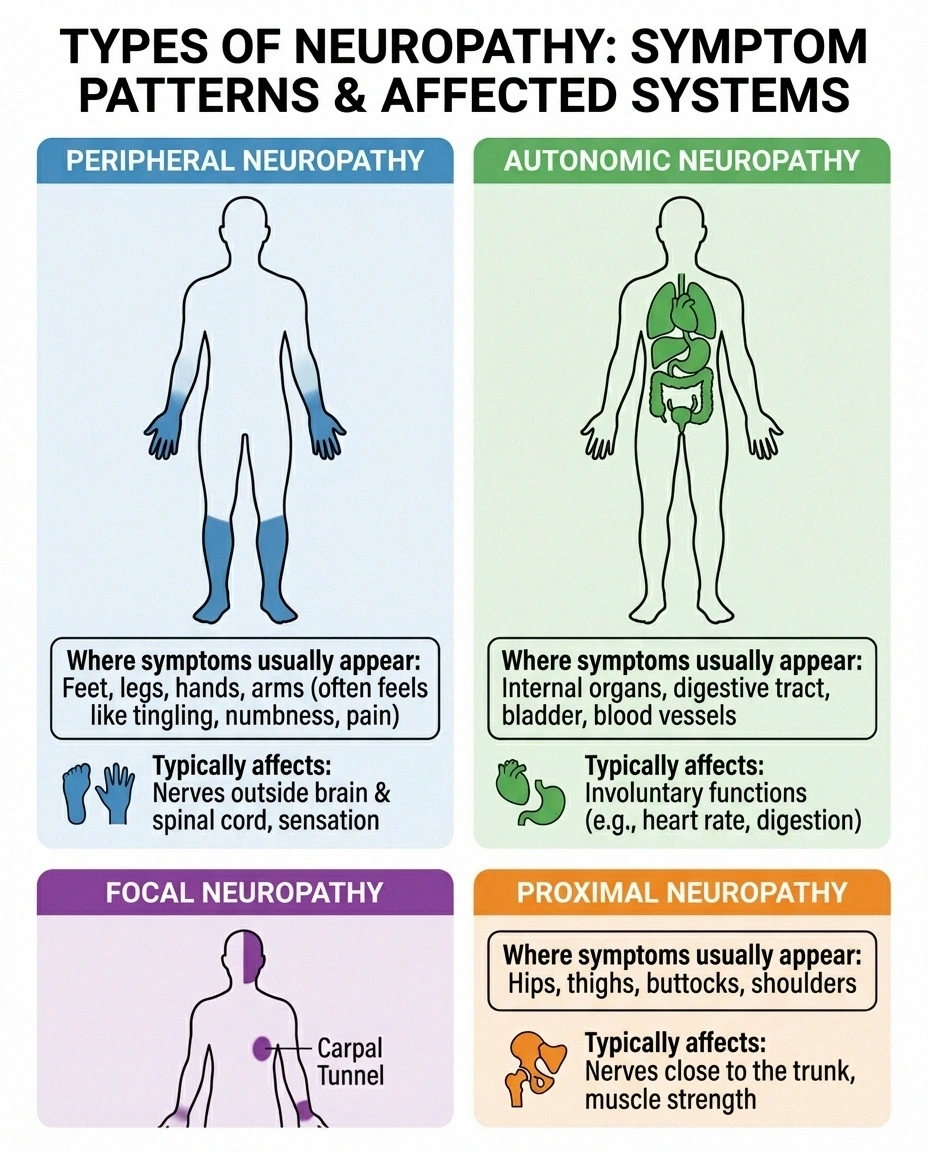
When people search “types of neuropathy,” they are usually landing on the classic four-part framework below. It is not the only useful framework, but it is the one most consumer-facing articles start with.
Peripheral
Usually starts in feet or hands. Often length-dependent.
Autonomic
Affects blood pressure, digestion, sweating, bladder, and sexual function.
Focal
One nerve or one tight area. More localized symptoms.
Proximal
Often starts in hips, buttocks, or thighs with pain and weakness.
Peripheral Neuropathy
This is the broad umbrella most people mean when they say “neuropathy.” It refers to damage in the peripheral nerves outside the brain and spinal cord. Symptoms often begin in the feet and hands because the longest nerves are affected first. That is why burning, numbness, tingling, or “invisible socks” sensations usually start distally.
Autonomic Neuropathy
Autonomic neuropathy affects the nerves that control automatic body functions: blood pressure, digestion, bladder function, sweating, sexual function, and heart rate. The symptoms can feel less obviously “nerve-like,” which is why this type is often missed or minimized at first.
Focal Neuropathy
Focal neuropathy means a single nerve or a small group of nerves is affected. Think compression injuries, carpal tunnel, cranial nerve involvement, or a sudden band of pain from a more targeted nerve problem. Symptoms are more localized and may show up abruptly rather than following the classic stocking-glove pattern.
Proximal Neuropathy
Proximal neuropathy usually involves the hips, buttocks, or thighs rather than the feet first. It often causes severe pain followed by weakness. In diabetic patients it is sometimes discussed as diabetic amyotrophy. It is less common than distal sensory neuropathy and can feel like a completely different disease when it shows up.
Sensory, Motor, and Autonomic Fiber Involvement
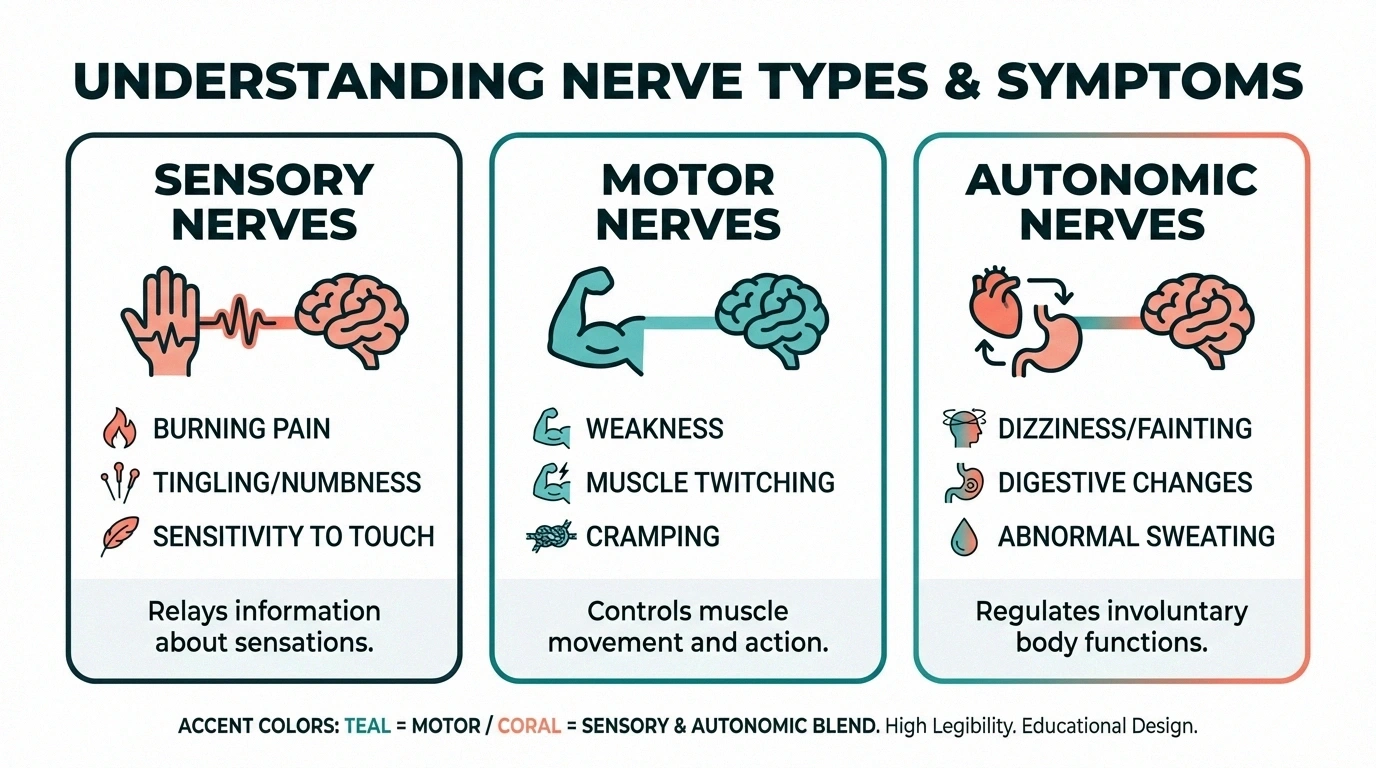
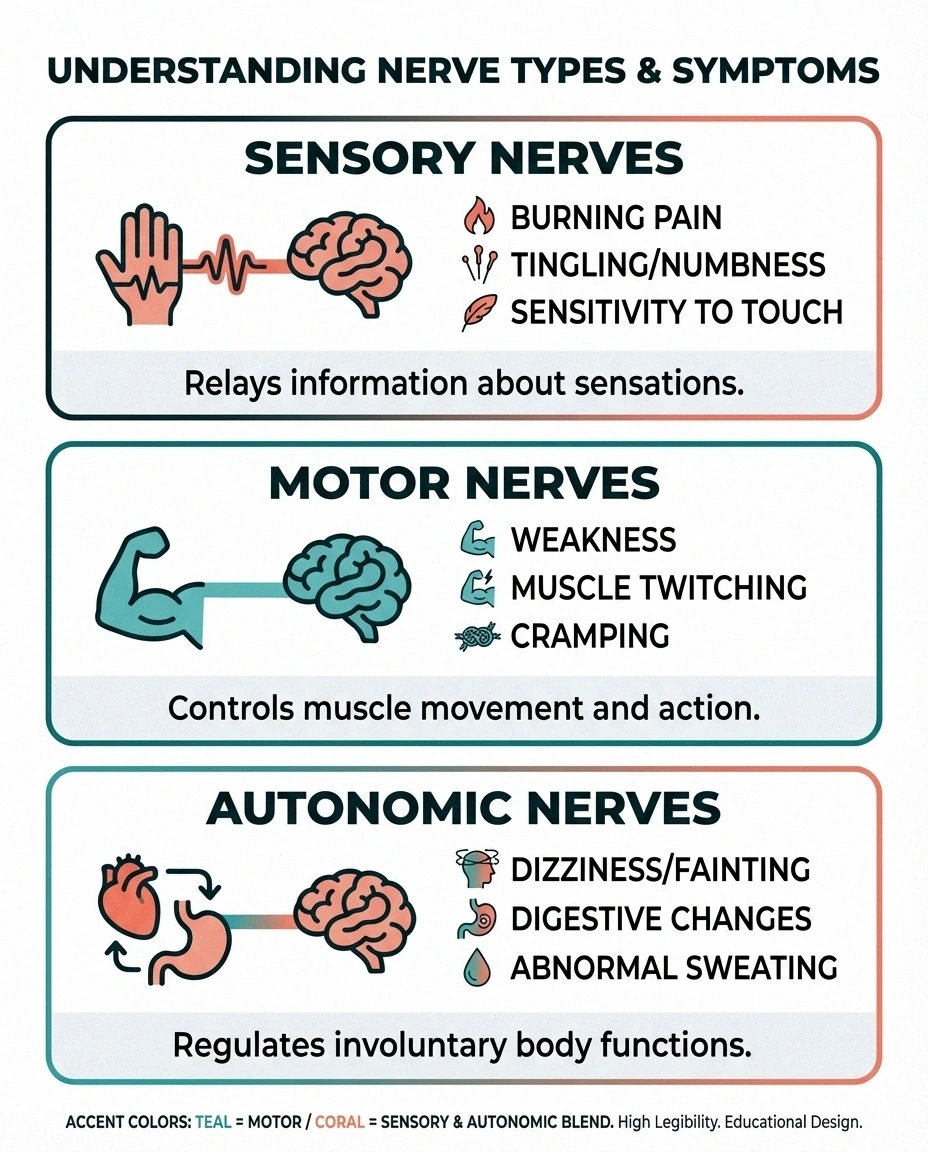
Another way to classify neuropathy is by the kind of nerve fibers involved. This system matters because it predicts symptoms.
Symptom Clues by Fiber Type
Sensory: burning, tingling, numbness, pain from touch
Motor: weakness, cramps, muscle wasting, foot drop
Autonomic: dizziness, sweating changes, bladder or digestive symptoms
- Sensory neuropathy causes numbness, tingling, burning, cold sensitivity, altered touch, or severe pain from light contact. This is where classic nerve pain descriptions live.
- Motor neuropathy causes weakness, cramping, muscle wasting, twitching, foot drop, or reduced coordination.
- Autonomic neuropathy causes dizziness on standing, bowel changes, sweating changes, bladder symptoms, temperature regulation problems, or sexual dysfunction.
- Mixed neuropathy is common. Many people do not fit neatly into one bucket.
NINDS also emphasizes that many neuropathies are length-dependent. That means the farthest nerve endings — usually in the feet — are hit first. But not all neuropathies behave that way. Some start around the torso, move unpredictably, or attack one nerve at a time.
Common Named Neuropathy Types You May See on a Diagnosis List

This is where people get confused, because many “types” are actually specific causes or subtypes rather than broad categories. Some common examples include:
- Small fiber neuropathy — often heavy on burning pain, temperature sensitivity, and autonomic overlap
- Diabetic neuropathy — common cause category that can include several patterns
- Idiopathic neuropathy — how neuropathy progresses and spreads with no clear cause found despite workup
- Toxic neuropathy — linked to alcohol, chemotherapy, or other toxic exposures
- Hereditary neuropathy / Charcot-Marie-Tooth — inherited nerve disorders
- Ulnar neuropathy — focal compression or injury to the ulnar nerve
- Chemotherapy-induced neuropathy — acquired neuropathy after cancer treatment
ADA also highlights examples such as cranial neuropathy, compression mononeuropathy, femoral neuropathy, thoracic or lumbar radiculopathy patterns, unilateral foot drop, and Charcot joint. The point is not to memorize every subtype. The point is to realize that “type” can refer to structure, cause, or pattern depending on context.
Why the Cause Matters as Much as the Type
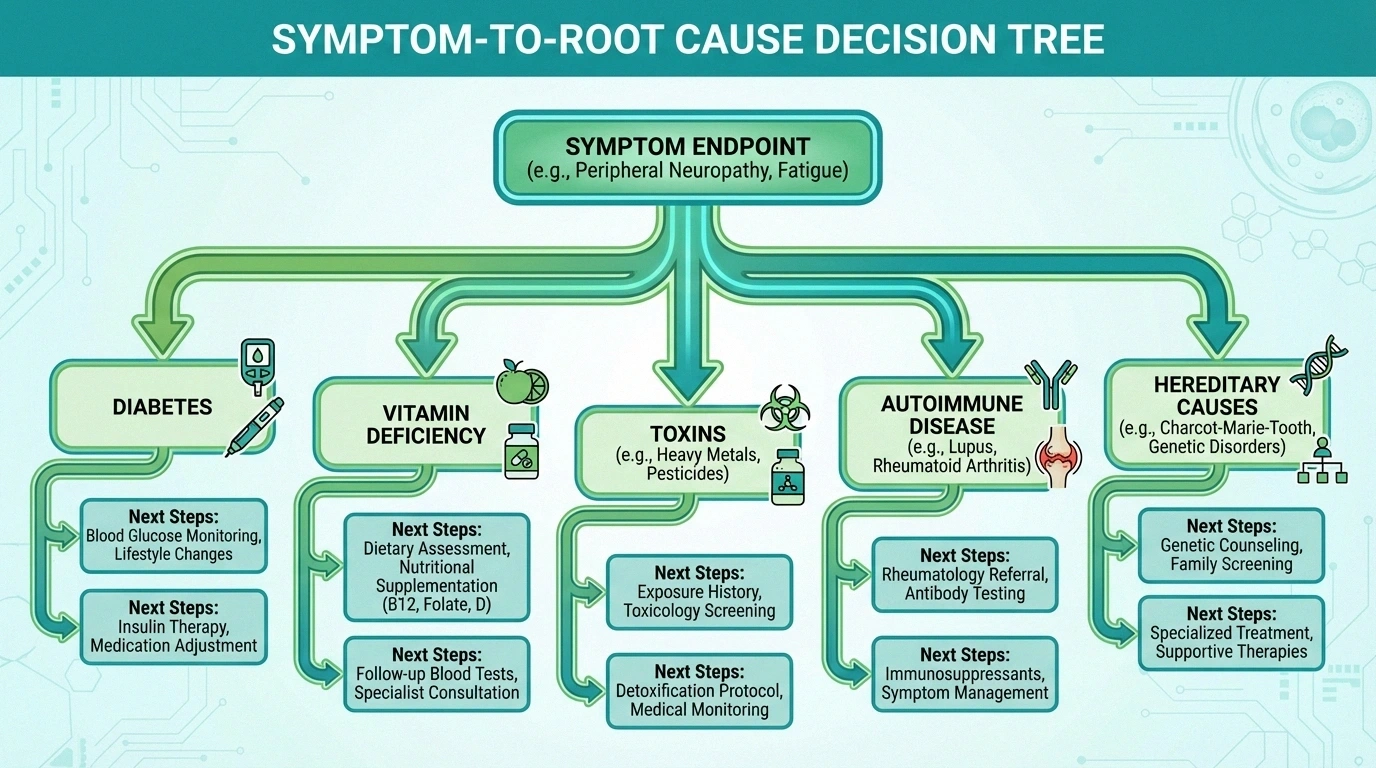
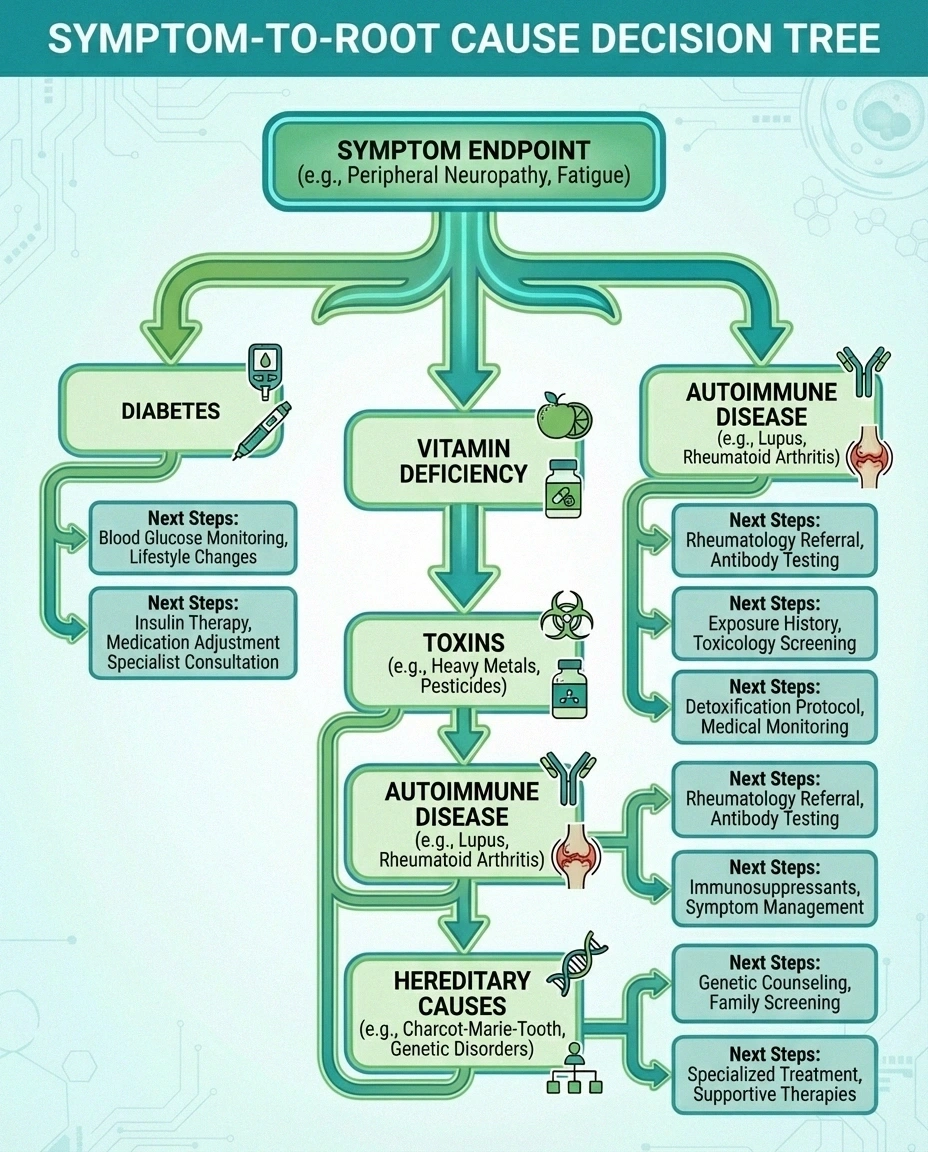
Two people can both have peripheral neuropathy and still need completely different next steps. One may need tighter diabetes control. Another needs a vitamin deficiency corrected. Another needs a medication review because the drug causing the problem is still on board. Another may need autoimmune evaluation.
Important
“Peripheral neuropathy” is often a starting label, not the finish line. The cause and pattern still matter because they change treatment and urgency.
That is why a good diagnosis is not just a label like “peripheral neuropathy.” It should keep moving until the bigger questions are answered:
- Which nerves are affected?
- How is the pattern behaving?
- What is the most likely cause?
- Is the problem stable, progressive, reversible, or urgent?
If your current label feels vague, it may simply mean the workup is incomplete — not that the condition is impossible to understand.
How Diagnosis Usually Happens

Diagnosis usually starts with the symptom story and neurologic exam. From there, testing may include blood work, EMG and nerve conduction studies, medication review, and sometimes more specialized tests such as skin biopsy for suspected small fiber neuropathy or autonomic testing when dizziness, sweating, or digestive symptoms dominate.
The right test depends on the pattern. A focal compression problem does not need the same workup as a widespread progressive neuropathy. The fastest way to get traction is to match the testing strategy to the pattern instead of ordering everything blindly.
Frequently Asked Questions
What are the four main types of neuropathy?
The classic consumer-facing framework is peripheral, autonomic, focal, and proximal neuropathy. But that is only one way neuropathy is classified.
Is small fiber neuropathy different from peripheral neuropathy?
Small fiber neuropathy is a subtype of peripheral neuropathy. It describes which fibers are affected rather than replacing the broader peripheral category.
What is the difference between mononeuropathy and polyneuropathy?
Mononeuropathy affects one nerve or one limited nerve area. Polyneuropathy affects many nerves, often in a more symmetric pattern that begins in the feet and moves upward.
Can one person have more than one neuropathy type?
Yes. A person may have a peripheral neuropathy that is mainly sensory, caused by diabetes, and worse in a length-dependent pattern. Those labels can all describe the same case.
Why does my diagnosis still feel vague?
Sometimes the broad category is clear before the exact cause is. That often means the workup is still in progress, not that nothing useful can be learned.
The Bottom Line
The word “type” is doing too much work in most neuropathy conversations. Sometimes it means location. Sometimes it means fiber involved. Sometimes it means cause. Sometimes it means pattern.
Once you separate those layers, the whole subject gets a lot less confusing — and your diagnosis starts sounding like a system instead of a contradiction.
This article is for educational purposes only and does not constitute medical advice. Consult a qualified healthcare provider for diagnosis and treatment decisions.